

Abstract
The aim of this study was to assess the level of availability of HIV prevention strategies in secondary schools in Kabarole district, Uganda in order to inform the design of interventions to strengthen HIV Prevention and psychosocial support. Quantitative and qualitative research methods were used in eight secondary schools in Kabarole district to establish available HIV prevention and psychosocial support services. Questionnaires were administered to 355 students 12-24 years old. In addition, 20 Key Informant interviews were held with education service providers. Quantitative data was analyzed using Epi-data and qualitative data were analyzed by thematic content analysis. Seven of the eight schools had at least one HIV prevention strategy. Two teachers in each of the five schools had been trained in HIV prevention. No school had a nurse trained in HIV prevention, care and support. Education service providers had limited knowledge of HIV prevention support and care of students living with HIV. We found out that students had knowledge on how one can acquire HIV. HIV prevention services reported by students in schools included: talks from teachers and guests (19%), drama with HIV prevention related messages (16%), peer education clubs (15%), workshops and seminars on HIV (8%), sensitization about HIV/AIDS (7%), guidance and counseling (6%), talking compounds- (5%), abstinence talks (6%), keeping students busy in sports (4%), straight talk (4%). Sixty three percent reported receiving HIV reading materials from various sources. Preventing HIV infection among students in schools is still demanding with limited interventions for students. Efforts to support school interventions should focus on including HIV Prevention in the school curriculum, working with peer educators as well as education service providers who spend much of the time with the students while at school.
Key words: HIV, secondary schools, Uganda
Introduction
Approximately forty percent of the 2.6 million HIV infections that occurred in 2009 were among youth aged 15-24 years.1 Multiple factors make young people particularly vulnerable to HIV/AIDS including lack of knowledge, poorly developed life skills, lack of parental mentoring, early sexual debut, sexual coercion and unlimited access to health facilities.2 Most youth in sub Saharan Africa initiate sexual activity while they are still of school age whether or not they are still in school,3 some of what young people learn in school affects their lifelong norms, attitudes and behaviors.4
School-based HIV programs have great potential for HIV prevention education.5 For purposes of this paper, these are interventions aimed at HIV prevention that are targeting students in schools. School based programs was one of the several strategies Stover and colleagues (2002) viewed as a necessary step for decreasing HIV infection rates and protect the general population from further infection.6 Schools provide an established venue for intervention and their location is known and is sustained within the community. In addition, schools have established mechanisms for introduction of new programs and accessing students. With school-based programs, the size of the target population is known and can ably guide program design and implementation. Services in school-based settings can be of high quality, and are provided in a private, confidential and competent manner in an environment all students are familiar with. Ethier and colleagues provide more evidence on the effectiveness of school-based interventions as a critical access point for HIV preventive services to adolescents.7
School based programs can also be effective in improving young people’s knowledge of HIV/AIDS and reducing risky sexual behavior.8 As adolescents gain more accurate knowledge about sex and HIV/AIDS, they develop more rational reasoning for engaging in sexual activities and are more likely to abstain from sexual intercourse.9 Findings from an adolescent intervention on HIV/AIDS prevention through peer support implemented in secondary schools in South Africa indicated that peer education can contribute to a delayed onset of sexual activity and can therefore contribute to the prevention of HIV/AIDS among adolescents.10 A similar project to empower youth in schools to fight against HIV/AIDS in Uganda indicated a change in sexual behavior among pupils and this was noted to be primarily a consequence of information, education and communication activities aimed at increasing their knowledge about HIV/AIDS.11 Evaluation of this project indicated a reduction in self reported sexual activity of pupils due to fear of disease and pregnancy. The proportion of boys who viewed abstinence as good increased from 62% in 1994 to 89% in 2001 while that of girls increased from 65% in 1994 to 91% in 2001. As reported by Coates and colleagues (2008), behavioral strategies need to be more sophisticated, combined and scaled up. Similarly, behavioral strategies must be taken important with behavioral HIV prevention needs integrated with biomedical and structural approaches, and treatment for HIV Prevention.12 Al-Iryani and colleagues (2011) note that there is existing research evaluating the efficacy of peer education for HIV prevention in schools from countries with concentrated or generalized HIV epidemics.13 It is however important to note, that such programs in Uganda have largely been implemented in primary schools with very little documented about similar programs in secondary schools. We set out to establish what interventions on HIV prevention and psychosocial support for adolescents were available in secondary schools in Kabarole district, Uganda.
Materials and Methods
Study site
We conducted a quantitative and qualitative study among education service providers and students in 8 purposively selected secondary schools in Kabarole district, Uganda. The district is located in the western part of Uganda, some 320 km southwest of Kampala. Kabarole has a total area of 1844.25 km2 of which 137,802 is covered by forests. By March 2010, the district had an estimated population size of 403,100 people. The district is the most urbanized in the region with the highest HIV prevalence of 11.3%. It is also home to a tribe with the highest HIV prevalence rate in the country with 14.8%. In addition, the district has an estimated 163,998 persons living with HIV/AIDS and only 25,637 (16%) of them in care.14
Study population
A total of 375 participants were involved in the study including district officials in the health and education departments, students, teachers, school nurses and matrons. There were 355 students from 8 schools. They were 12-24 years in all classes of senior one-senior six. The 20 district officials, teachers, school nurses and matrons from the eight schools participated in the key informant interviews. Both students and education service providers were purposively selected. Students were selected considering representativeness of all classes and sexes as well as ability to express themselves. Education service providers were selected depending on the role they play in schools in relation to HIV and students counseling.
Data collection methods
A self-administered questionnaire composed of both closed- and open-ended questions was the main study instrument for students. The questionnaire addressed sociodemographic characteristics, knowledge of how HIV can be acquired and prevented, HIV prevention interventions in the schools, sources of information on HIV prevention, challenges faced by HIV positive students in the schools and how they are supported, what could be done to reduce HIV infection in secondary schools and nature of support to HIV positive adolescents administered. Key informant interview guides included questions on available HIV prevention interventions in schools, nature of services provided by school administration, school teachers, nurses and matrons who interact with students, HIV related trainings undertaken by education service providers in the schools. The student’s questionnaire was self administered while key informant interviews were held with education service providers.
Data analysis
Quantitative data was coded, entered into epi-database, analyzed and exported to SPSS, summarized and presented in proportions. The qualitative data were manually analyzed using themes.
Ethical considerations
Ethical approval was sought from the Makerere University School of Public health higher degrees, research and ethics committee. Further clearance was obtained from the Uganda National Council of Science and Technology. Written consent was sought from the ministry of education, district education and health officers, head teachers and students prior to completing the questionnaire. Assent was also sought from students that were under the consenting age. Names of students who completed the questionnaires were not written for confidentiality.
Results
Background characteristics of the study participants
A total of 355 students and 20 education service providers and selected district officials were consulted. Of the students 47% (167) were female and 53% (188) were males. Students from single sex schools were 21% while 79% were from mixed schools. Day scholars were 48% with 52% in boarding school. The age of respondents varied with 31% between 12-15 years, 59% having 16-19 years while only 10% were above 20 years. We found out that majority of the respondents (70%) come from rural areas and only 30% from the town. The highest percentage (72%) of the students interviewed lived with biological parents, 11% with older siblings and relatives, 10% with grandparents, 5% guardians other than relatives and only 2% lived alone. Respondents for the in-depth interviews included: district officials specifically district education officer and inspector of schools, district community development officer, and district health officer. Education service providers included: teachers from all schools, 4 school nurses and 5 school matrons. All teachers interviewed were in charge of HIV education and awareness creation in schools as well as senior woman and man teachers. A summary of the characteristics of the students who completed questionnaires is presented in Table 1.
Table 1.
Social demographic characteristics of respondents.
| Characteristics, class | Frequency (%) |
|---|---|
| Gender | |
| Female | 167(47) |
| Male | 188(53) |
| Status of school | |
| Mixed | 280(79) |
| Single sex | 75(21) |
| Educational status of respondents | |
| Day | 171(48) |
| Boarding | 184(52) |
| Age | |
| 12-15 | 105(31) |
| 16-19 | 202(59) |
| 20-24 | 35(10) |
| Class of respondent | |
| S1-S2 | 136(38) |
| S3-S4 | 118(33) |
| S5-S6 | 100(28) |
| Residential status | |
| Urban/town | 106(30) |
| Rural/village | 245(70) |
| Household head | |
| Biological parent | 251(72) |
| Older sibling | 37(11) |
| Grand parent | 35(10) |
| Other guardian | 19(5) |
| Self | 7(2) |
Knowledge about HIV/AIDS prevention, attitude and practice among education service providers
We found out that in all schools that participated in the baseline, education service providers had limited knowledge on HIV prevention and handling of students living with HIV. Each of the schools had at least a teacher that had been trained in HIV/AIDS. Teachers’ acknowledged having limited knowledge of handling students that disclosed their HIV status. In one of the schools, they admitted having failed to deal with two students who disclosed their HIV status as noted: Two of our students disclosed their HIV status and wanted support to enable them take their medication. We were so scared and held a meeting to discuss how best we can go about it, we felt HIV was more real than we had assumed but handed them over to a fellow student who had training in nursing for support in adherence.
School nurses and matrons lacked HIV related trainings with one nurse having been sensitized in HIV/AIDS. Another school had attended a Reproductive health related training prior to working with the school.
Knowledge about HIV/AIDS, attitude and practice among adolescents
In all schools, students knew how one can acquire HIV with the following being reported; having unprotected sex with an infected person (37%), sharing sharp instruments (27%), mother to child transmission (20%), blood transfusion (10%), kissing an infected person (3%), accidents (2%) and using unsterilized instruments (1%) (Figure 1).
Figure 1.
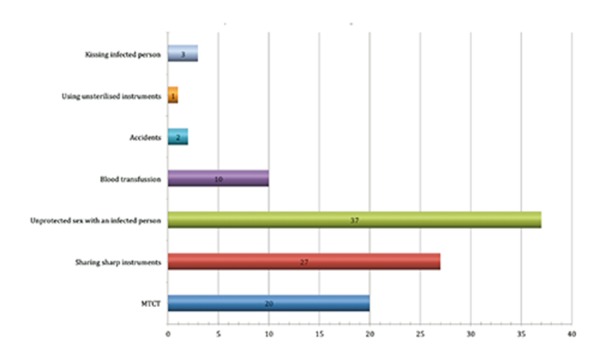
Ways in which one can acquire HIV.
Knowledge on HIV prevalence among fellow students
We found out that 30% of students acknowledged knowing that some of the fellow students had HIV. The number of students in day school reporting this was higher at 33% compared to 27% in boarding schools. The number of 16-19 who reported this was higher at 36% compared to 27% among 20-24 and 21% among 12-15 year olds. Students reported knowing this through various sources including: physical appearance (29%), nature of medication they take (23%), rumors (12%), frequent illness (12%), and from teachers (12%). Only 6% of the students had seen the HIV testing cards of the infected students while 6% had been disclosed to by the HIV infected colleagues (Figure 2). HIV infected students were reported to be having several problems including: frequent illness (25%), discrimination and stigma by fellow students (17%), being worried all the time (16%) and self stigma (13%) as well as poor feeding.
Figure 2.
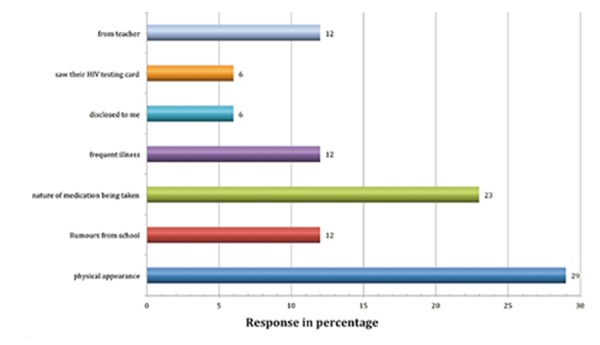
Source of information on HIV status of colleagues at school.
HIV status disclosure in secondary schools
Disclosure by the students was still limited with four of the eight schools having had 2-5 students disclosing their HIV status to the head teacher, school nurse or senior teacher. We found out that head teachers had been disclosed to more than teachers, school nurse and matron. It was reported that parents and guardians disclose their children’s HIV status compared to the students. One of the schools had an organization that supported children infected and affected by HIV. Management of the organization disclosed the status of all its students and members to the school authorities since the students had to regularly go for treatment and check up.
Discussions with the head teachers revealed that while adolescents found it easier to disclose to head teachers, parents found it easier to disclose to school matrons and nurses. Head teachers reported that students prefer disclosing to them because they can easily get permission for clinic appointments. Both matrons and nurses reported that parents easily disclosed to them the children’s HIV status because they are closer to their children outside class and can support them in adherence unlike head teachers as observed. Parents disclose because they want us as school matrons and nurses to keep an eye on their children and ensure they take their medication.
HIV prevention activities available in the schools
The students reported having various forms of interventions offering HIV prevention in secondary schools in Kabarole district. These include talks from teachers and guests (19%), drama with HIV prevention related messages (16%), peer education clubs (15%), workshops and seminars on HIV (8%), sensitization about HIV/AIDS (7%), guidance and counseling reported by 6%, talking compounds/compounds with message boards (5%), abstinence talks (6%), keeping students busy in sports (4%), straight talk (4%), among others.
We found out that the Presidential Initiative on AIDS Strategy Communication to Youth was the lead trainer of teachers and had held a three days training for two teachers inclusive of the head teacher in 2009. The trained teachers were Trainers of Trainers expected to pass on the knowledge and skills to other teachers and students after each lesson. Straight Talk, which advocates for safer sex, including abstinence, non penetrative sex and condom use was in five schools.
It was reported that five of the schools had peer-to-peer program that trains students to be peer educators. One training had been conducted for peer educators in 2009. Three schools were benefiting from interventions from Kabarole Youth Alliance a program that creates awareness on HIV/AIDS and does HIV testing among youths in Kabarole district. One of the schools benefited from the Teen star program that mainly teaches about sexuality. The program targets senior three students (15-17 years) for a period of 1 year. The senior woman teacher was trained and provided with a syllabus to guide program implementation. During the one-year of implementing the program, students meet once a week to cover a given topic until the syllabus will be completed.
Information education and communication materials in schools
Seven of the schools received information, education and communication (IEC) materials on HIV prevention topics together with questions and answers on experiences of adolescents received from all over the country. Music dance and drama (MDD) clubs were also reported as sources of information used in schools. Four of the schools reported having MDD groups that present in and outside their school. Sixty three percent of students reported having received IEC materials in their respective schools.
Various schools store IEC materials differently as reported by students including; library (51%), talking compounds (16%), notice board (11%), kept by the career/senior teacher (5%), stored in head teachers’ office (5%), given out to students (4%), bursars office (2%), school lab (2%) and in classes (3%). We found out that utilization of materials differed among the students with 19% of students reporting daily usage, 21% during their free time, 13% reported twice or three times a week, 10% read once a term,9% accessed them weekly while 8% accessed them every time they walked past signposts on their school compound.
Discussion
Our study was aimed at assessing HIV prevention interventions in secondary schools in Kabarole. Our findings that peer educators play a major role in HIV prevention awareness in secondary schools are in line with Speizer and colleagues (2003) who noted that peer educators play a major role in the success of interventions involving behaviour change15 and Williams and colleagues (2010) who observed that in order to ensure success of the HIV interventions, those providing the intervention must be a member of the target population and of the surrounding community.16 Bok and Morales (1997) also assert that interventions led by peers are more effective than those led by adults since peers are more apt to impact group norms and individual intentions to change behavior. Peer educators have also demonstrated that they can present material in a way that addresses the relevance of HIV prevention to young people’s lives.17 Despite the existence of some interventions for HIV prevention in schools, formal sex education that has been proven to be effective in reducing adolescent’s involvement in risky sexual behaviors as noted by Mueller and colleagues was not reported.18
Secondary students in both day and boarding schools spend most of their time in schools. As confirmed in a previous study conducted in Mbarara, Uganda, while there, they turn to education service providers who include teachers, school nurses and matrons for information on health related issues.19 Our study findings are contrary to this study findings because education service providers have not had much training in HIV prevention and thus have limited information on HIV that they can share with students. They are also contrary to a previous study by Vegnani and colleagues (2002) in which the importance of support and participation by school heads and teachers for the existence of a sound school based policy that supports HIV interventions.20
Information, education and communication materials distributed to schools can only have an impact on increasing students’ knowledge on HIV/AIDS if well accessed and utilized by the target group or beneficiaries.21 Although students acknowledged getting IEC materials in HIV prevention distributed to their schools, they are not widely accessed by all students in schools. Even where they can be accessed, utilization is limited due to the poor reading culture, storage and limiting school programs. Sometimes IEC materials are stored in the library, here students may easily miss out on them especially if they are used to going to the library for only borrowing books or serious reading in preparation for exams. This is mainly attributed to the poor reading culture in Uganda whereby both adults and children find it difficult to read and can only read under serious circumstances such as when expecting exams. Where IEC material are kept in staff room and head teacher’s offices, students do not easily access them for fear of entering offices. Where they are distributed and students take them home, a few of them get access and others miss out. Frequency of reading IEC material differed depending on the school, storage and students interest. While in some schools adolescents read the paper privately, it was revealed that in other schools, it was read privately first, then shared with colleagues in guided discussions.
Despite the students knowledge that having unprotected sex with an HIV infected person is one of the ways through which HIV is spread, many adolescents in school are still having unprotected sex. These findings are similar to those of studies conducted in Trinidad and Tobago22 South Africa23 and Tanzania24 which all indicate that adolescents in school are still predisposed to sexually transmitted diseases and HIV due to being sexually active and engaged in unprotected sex.25 This is also in agreement with a similar study that indicated that 80% of young people still have insufficient understanding of how to avoid HIV.26
Conclusions
Preventing HIV infection among students in schools is still demanding given that there are limited interventions for students yet sexual risk behavior is influenced by social interactions and peer pressure which are common in schools. Efforts to support school interventions must focus on including HIV prevention in the school curriculum, working with peer educators as well as education service providers who spend much of the time with the students while at school.
Acknowledgements
This research and the development of this article was supported in part by Makerere University School of Public Health/Centers for Disease Control (CDC) Fellowship Program, Makerere University School of Public Health and Baylor College of Medicine Children’s Foundation Uganda through cooperative agreement Number 5U2GPS000942 from Centers for Disease Control and Prevention (CDC). The authors give special thanks to the Ministry of education, Kabarole district local government, all the schools that participated in the study and all respondents. We would also like to thank the data management team.
References
- 1.World Health Organization. 2009 AIDS Epidemic Update, UNAIDS, Geneva, Switzerland; 2009. [Google Scholar]
- 2.United Nations Population Fund. HIV Interventions for Most-at-risk young people. Global Guidance Brief. UNFPA: New York, USA; 2008. [Google Scholar]
- 3.Kaaya S, Flitcher A, Mbwambo J, et al. A review of studies of sexual behavior of school students in sub-Saharan Africa. Scand J Public Health 2002;30:148-60. [DOI] [PubMed] [Google Scholar]
- 4.Sue M, Mavedzenge N, Doyle AM, Ross DA. HIV prevention in young people in Sub Saharan Africa; a systematic review. J Adolescent Health 2011;49:568-86. [DOI] [PubMed] [Google Scholar]
- 5.Napierala Mavedzenge SM, Doyle AM, Ross DA. HIV prevention in young people in sub-Saharan Africa: a systematic review. J Adolesc Health 2011;49:568-86. [DOI] [PubMed] [Google Scholar]
- 6.Gallant M, Maticka-Tyndale E. Schoolbased HIV prevention programmes for African youth. Soc Sci Med 2004;58:1337-51. [DOI] [PubMed] [Google Scholar]
- 7.Juszczak L, Ammerman A. Reaching adolescent males through school based health centres. J Adolesc Health 2011;48:538-9. [DOI] [PubMed] [Google Scholar]
- 8.Youth Development. HIV/AIDS Prevention among Youth: what works? Available from: http://siteresources.worldbank.org/INTCY/Resources/395766-1186420121500/YDNii1HIVAIDS.pdf [Google Scholar]
- 9.Shuey DA, Babishangire BB, Omiat S, Bagarukayo H. Increased sexual abstinence among in school adolescents as a result of school health education in Soroti district Uganda. Health Educ Res 1999;14:411-9. [DOI] [PubMed] [Google Scholar]
- 10.Visser MJ. HIV/AIDS Prevention through peer education and support in secondary schools in South Africa. SAHARA J 2007;4:678-94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ngatia P, Omiat S. Empowering youth to fight HIV/AIDS: encouraging sexual abstinence - the Soroti School Health and HIV/AIDS Prevention Project in Uganda: African Medical and Research Foundation (AMREF); 2004. [Google Scholar]
- 12.Coates TJ, Richter L, Caceres C. Behavioural strategies to reduce HIV transmission: how to make them work better. Lancet 2008;372:669-84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Al-Iryani B, Basaleem H, Al-Sakkaf K, et al. Evaluation of a school-based HIV prevention intervention among Yemeni adolescents. BMC Public Health 2011;11:279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Health Communication Partnership - Uganda. Quarterly Progress Report. 2010. Jan 1 -Mar 31. Available from: https://www.k4health.org/sites/default/files/2009-10%20Q2%20HCP%20Report%20Jan%20to%20March.pdf [Google Scholar]
- 15.Speizer IS, Magnani RJ, Colvin C. The effectiveness of adolescent reproductive health intervention in developing countries; a review of the evidence. J Adolesc Health 2003;33:324-84. [DOI] [PubMed] [Google Scholar]
- 16.Williams JK, Wyatt GE, Wingood G. The Four Cs of HIV Prevention with African Americans: crisis, condoms, culture and community. Curr HIV/AIDS Rep 2010;7: 185-93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Bok M, Morales J. Effective HIV prevention interventions for adolescents and young adults: a theoretical approach. J HIV/AIDS Prev Ed Adolesc Child 1997;1:9-35. [Google Scholar]
- 18.Mueller TE, Gavin LE, Kulkarni A. The association between sex education and Youth’s engagement in sexual intercourse, age at first intercourse and birth control use at first sex. J Adolesc Health 2008;42:89-96. [DOI] [PubMed] [Google Scholar]
- 19.Ybarra ML. Health information seeking among Mbarara adolescents; results from the Uganda Media and you survey. J Health Ed 2007;23:249-58. [DOI] [PubMed] [Google Scholar]
- 20.Johnson B, Vergnani T, Chopra M. The challenges of introducing HIV/AIDS education into primary schools in South Africa. Proceedings of the XIV International AIDS Conference, 2002 Jul 7-12, Barcelona, Spain. [Google Scholar]
- 21.Ngatia PM, Omiat S. Empowering youth to fight HIV/AIDS: encouraging sexual abstinence. The Soroti School Health and HIV/AIDS Prevention Project in Uganda. 2004. [Google Scholar]
- 22.Voisin DR, Dillon-Remy M. Psychocultural factors associated with HIV infection among Trinidad and Tobago adolescents. J HIV/AIDS Prev Ed Adolesc Child 2002;4:65-82. [Google Scholar]
- 23.Campbell C, Foulis CA. Peer education, gender and the development of critical consciousness, participatory HIV prevention by South African youths. Soc Sci Med 2002;55:331-45. [DOI] [PubMed] [Google Scholar]
- 24.Bearinger LH, Sieving RE, Ferguson J, Sharma V. Global perspectives on the sexual and reproductive health of adolescents: patterns, prevention, and potential. Lancet 2007;369:1220-31. [DOI] [PubMed] [Google Scholar]
- 25.Campbell C, Foulis CA. Creating contacts that support youths-led HIV prevention in schools. Soc Trans 2002;33:339-56. [Google Scholar]
- 26.WHO Technical Report series #938. Preventing HIV/AIDS in young people. A systematic Review of the evidence from Developing Countries. UNAIDS Interagency Task Team on Young People. UNAIDS/UNFPA/UNICEF/WHO: Geneva, Switzerland; 2006. [Google Scholar]