

Abstract
Nitrous oxide is a gas that is odorless, colorless, and has a sweet taste at room temperature. Nitrous oxide has several uses, including in surgery and dentistry (referred to as “laughing gas”), in automotive racing, and in aerosol spray propellants. The aerosol spray propellants that typically use nitrous oxide are whipped cream canisters and cooking sprays. Unfortunately, these over-the-counter household items are a source of nitrous oxide that can be used for recreational use. The most popular is the use of industrial-grade canisters having the slang term “whippets.” The nitrous oxide can be extracted by pushing the nozzle down slightly to the side and catching the released gas with a balloon. The contents of the balloon can then be directly inhaled, giving an instant feeling of euphoria. This is not a benign means to achieve a euphoric state but can cause severe nitrous oxide–induced B12 deficiency, which is presented in this case report.
An estimated 800,000 young adults abuse inhalants every year (1), and almost 11% of high school seniors report using inhalants at least once in their lifetime (2). Heavy inhalant abuse can result in a variety of side effects, including cardiac arrhythmias, hypoxia, metabolic acidosis, and neurologic deficits. Of all inhalants, nitrous oxide is particularly toxic due to its conversion of the active monovalent form of vitamin B12 to its inactive bivalent form (3). We present a case of subacute combined degeneration of the spinal cord due to nitrous oxide–induced vitamin B12 deficiency.
CASE DESCRIPTION
A 22-year-old man with a history of polysubstance abuse and asthma presented with a 1-month history of worsening hand numbness and difficulty with fine motor movements, followed by intermittent numbness in both feet and significant gait ataxia. He admitted to daily nitrous oxide abuse for months prior, reportedly inhaling over 30 whipped cream chargers every day. Neurologic exam was remarkable for decreased vibratory sensation in bilateral lower extremities, absence of distal proprioception, hyperreflexia, impaired coordination, rapid alternating movements, truncal ataxia, and a positive Romberg test. Serologic workup illustrated a mild anemia with a hemoglobin of 11.7 g/dL and mean corpuscular volume of 98 fL. His vitamin B12 level was at the low end of normal at 222 pg/mL; however, his homocysteine and methylmalonic acid levels were elevated at 16.3 μmol/L and 1.56 μmol/L, respectively. Magnetic resonance imaging (MRI) of the spine illustrated abnormal T2 hyperintensity of the dorsal columns of C1 to T5, consistent with extensive subacute combined degeneration (Figure). B12 supplementation was started along with cessation of nitrous oxide use, resulting in significant clinical improvement. The patient was not tested for other causes of B12 deficiency, such as atrophic gastritis, given his excessive use of nitrous oxide and improvement after discontinuation of nitrous oxide.
Figure.
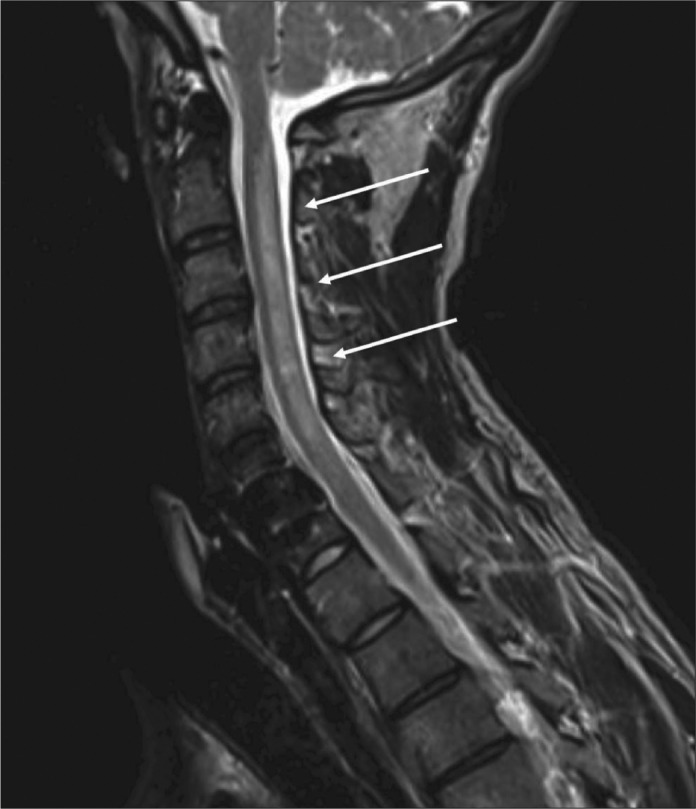
MRI of the cervical spine illustrating a long segment of T2 hyperintensity involving the dorsal column of virtually the entire cervical spinal cord consistent with a diagnosis of subacute combined degeneration.
DISCUSSION
Although our patient's vitamin B12 level was at the low end of normal, his clinical presentation, elevated levels of homocysteine and methylmalonic acid, and MRI findings are consistent with a diagnosis of nitrous oxide–induced vitamin B12 deficiency. Unfortunately, the accessibility and low cost of whipped cream chargers have made nitrous oxide inhalation, or “whippets,” increasingly popular among teenagers and adults alike. While significant toxicities rarely occur with occasional inhalation, heavy nitrous oxide abuse can result in significant polyneuropathy and ataxia (5), as seen in our patient. Provider recognition and early identification of nitrous oxide–induced vitamin B12 deficiency is essential, as neurologic deficits are often reversible with aggressive vitamin B12 supplementation and nitrous oxide cessation (4).
References
- 1.Results from the 2007 National Survey on Drug Use and Health: National Findings (DHHS Publication No. SMA 08-4343) Rockville, MD: Substance Abuse and Mental Health Services Administration, 2008; Substance Abuse and Mental Health Services Administration Office of Applied Studies. [Google Scholar]
- 2.Eaton DK, Kann L, Kinchen S, Shanklin S, Flint KH, Harris WA, Lowry R, McManus T, Chyen D, Whittle L, Lim C, Wechster H. Centers for Disease Control and Prevention. Youth risk behavior surveillance—United States 2011. MMWR Surveill Summ. 2012;61(4):1–162. [PubMed] [Google Scholar]
- 3.Kaufman B, Sutin KM, Wahlander S, Miller SM. Goldfrank's Toxicologic Emergencies 6th ed. Stamford, CT: Appleton & Lange, 1998; Anesthetics and neuromuscular blocking agents. In Goldfrank LR Flomenbaum NE Lewin NA Howland MA Nelson LS Hoffman RS eds. [Google Scholar]
- 4.Vishnubhakat SM, Beresford HR. Reversible myeloneuropathy of nitrous oxide abuse: serial electrophysiological studies. Muscle Nerve. 1991;14(1):22–26. doi: 10.1002/mus.880140105. [DOI] [PubMed] [Google Scholar]
- 5.Cheng HM, Park JH, Hernstadt D. Subacute combined degeneration of the spinal cord following recreational nitrous oxide use. BMJ Case Rep. 2013:bcr2012008509. doi: 10.1136/bcr-2012-008509. [DOI] [PMC free article] [PubMed] [Google Scholar]