

Summary
Background
Robert’s uterus is a very rare müllerian duct anomaly which is characterised by septate uterus with obstruction of a one-sided cavity and formation of hematometra. Therefore, patients present with cyclical abdominal pain during menstruation along with normal menstrual flow.
Case Report
We present magnetic resonance imaging (MRI) findings in a case of Robert’s uterus in a young woman.
Conclusions
Robert’s uterus is a very rare anomaly which can be very well characterized by magnetic resonance imaging (MRI). MRI can also show any associated hematometra and endometriomas complicating this condition and aid in the institution of appropriate management in such cases.
MeSH Keywords: Adnexa Uteri, Magnetic Resonance Imaging, Mullerian Ducts
Background
Robert’s uterus is a variant of septate uterus and is an extremely rare anomaly, which was first described in 1970 [1]. It is characterized by asymmetrical septum with obstruction of one of the uterine cavities. The other cavity communicates normally with the single cervix, which is responsible for cyclical menstrual flow. Since the obstructed cavity has functional endometrium, its secretions become retained with every menstruation and therefore it presents with cyclical pain [2,3]. We report MRI findings in a young women with Robert’s uterus who presented with cyclical menstrual pain and dysmenorrhoea.
Case Report
A 15-year-old female patient (menarche one year earlier) presented with severe dysmenorrhoea with normal menstrual flow. On the abdominal examination, fullness and tenderness was seen in the left flank. There was no history of tuberculosis or any urinary complaints. Ultrasound revealed a septate uterus with heterogeneous collection in the left uterine cavity. There was a left-sided, complex cystic lesion with haematosalpinx. Both kidneys were normally visualized. MRI was performed in a 1.5T system (Achieva, Philips Medical Systems, The Netherlands), which showed a septate uterus with normal outer fundal contour of the uterus. The left-sided cavity was obstructed with associated hematometra. There was also left haematosalpinx and endometriomas in the left ovary with loculated, hemorrhagic fluid in the lower peritoneal cavity. The right-sided uterine cavity was seen to communicate with the single cervical canal (Figures 1, 2). The patient underwent exploratory laparotomy with excision of the left-sided uterine cavity and of the left adnexal endometriotic lesions. The postoperative course was uneventful with relief of dysmenorrhoea.
Figure 1.
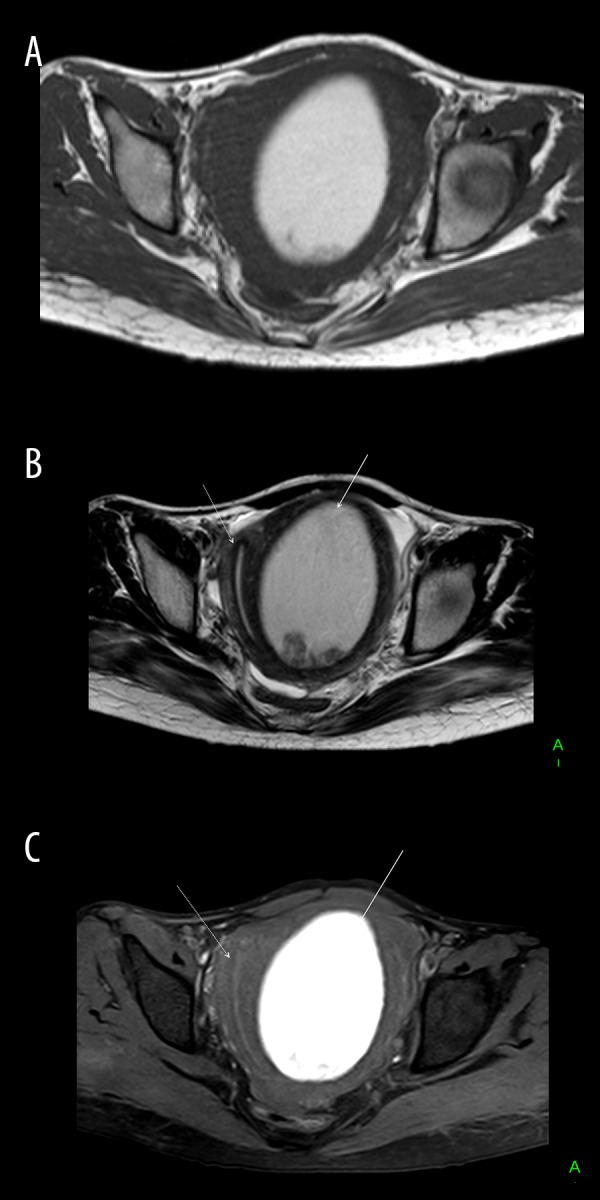
Axial T1W (A), T2W (B) and T1W fat-saturated (C) images showing a septate uterus with normal uterine contour and normal right-sided cavity (dotted white arrows in B and C) as well as the obstructed left-sided cavity with hematometra appearing hyperintense on T1W and T1W fat-saturated images with a shading effect on T2W images (white arrows in B and C).
Figure 2.

Coronal T2W images (A–C) showing single cervix (white arrow in A) connecting with the right-sided uterine cavity of a septate uterus (white and dotted white arrows in B). Also seen is the left haematosalpinx (white arrows in C and D) and lobulated, hemorrhagic fluid in the lower peritoneal cavity (dotted black arrows in C).
Discussion
Since its first description in 1970, Robert’s uterus has not been well characterised in the literature compared to other müllerian duct anomalies presenting with cyclical abdominal pain such as the unicornuate uterus with functional endometrium and obstructed hemivagina with ipsilateral renal anomaly syndrome (OHVIRA) [4,5]. There are very few reports of Robert’s uterus in the literature [2,3,6]. The mean age at diagnosis is more than 20 years, unlike our patient who presented at an age of 15 years [6]. Robert’s uterus results from a variation of septate uterus when the inferior part of the septum turns obliquely causing obstruction of one of the uterine cavities. The obstructed cavity with functioning endometrium releases cyclical secretions which can extend into the fallopian tube and the adnexal region with formation of haematosalpinx and endometriomas. Therefore, the classical presentation is with cyclical abdominal pain and dysmenorrhoea [2,3,6].
Ultrasound is helpful in visualising hematometra and associated adnexal endometriomas. With the advent of the 3-dimensional ultrasound, the outer contour of the uterus can be assessed, which can help in the diagnosis as the outer uterine contour is normal in this condition. However, there are still limitations of sonography in differentiating between different subtypes of müllerian duct anomalies. MRI is the modality of choice for a full visualisation of the extent of the anomaly and any associated complications. It provides exquisite anatomical detail and direct visualisation of the uterine contour, especially on coronal images [3,7]. MRI also provides valuable information regarding the contents of uterine and adnexal collections. Chronic blood products typically appear bright on T1W and T1W fat-suppressed images with a shading effect on T2W images. T1W fat-sat images are very sensitive in detecting small endometriomas [8].
The management of Robert’s uterus is not fully established, because it is reported sparsely in the literature, mainly as case reports. Open as well as minimally invasive treatments have been described [2,3,9]. The goals of treatment are drainage of the hematometra, prevention of its recurrence and drainage/excision of adnexal endometriomas. Recurrence of hematometra can be prevented by a complete excision of the obstructed cavity with preservation of the normal cavity or by ablation of the functional endometrium in the obstructed uterine cavity or by a unification of both uterine cavities by incising the septum [2,6,9,10]. In cases with associated adnexal endometriomas and associated adhesions, open laparotomy may be a better approach as adequate clearance of adnexal endometriomas can be done using open surgery. Incision of the septum has been described in both hysteroscopic and laparoscopic approaches with good outcomes. This can postpone the irreversible procedures and also keeps more possibilities for improving the uterine cavity for a better reproductive outcome later on [11,12].
Conclusions
In conclusion, Rober’s uterus is a very rare müllerian duct anomaly, which can be very well evaluated with MRI. It is important to consider this diagnosis in young patients with dysmenorrhoea with normal menstrual flow. Early diagnosis is important, as minimally invasive procedures may be more effective if detected before the formation of adnexal endometriomas.
Footnotes
Conflicting of interest
None.
References
- 1.Robert H. [Asymmetrical bifidities with unilateral menstrual retention (apropos of l2 cases)]. Chirurgie. 1970;96(11):796–99. [in French] [PubMed] [Google Scholar]
- 2.Capito C, Sarnacki S. Menstrual retention in a Robert’s uterus. J Pediatr Adolesc Gynecol. 2009;22(5):e104–6. doi: 10.1016/j.jpag.2008.03.004. [DOI] [PubMed] [Google Scholar]
- 3.Maddukuri SB, Karegowda LH, Prakashini K, Kantipudi S. Robert’s uterus: A rare congenital müllerian duct anomaly causing haematometra. BMJ Case Rep. 2014;2014 doi: 10.1136/bcr-2014-204489. pii: bcr2014204489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Silva PD, Welch HD. Laparoscopic removal of a symptomatic rudimentary uterine horn in a perimenarchal adolescent. JSLS. 2002;6(4):377–79. [PMC free article] [PubMed] [Google Scholar]
- 5.Mittal K, Gupta S, Mittal P, et al. Uterus didelphys with obstructed hemivagina and ipsilateral renal anomaly syndrome: A rare cause of cyclic abdominal pain in a young female. Int J Adv Med Health Res. 2016;3:28–30. [Google Scholar]
- 6.Gupta N, Mittal S, Dadhwal V, Misra R. A unique congenital mullerian anomaly: Robert’s uterus. Arch Gynecol Obstet. 2007;276(6):641–43. doi: 10.1007/s00404-007-0389-2. [DOI] [PubMed] [Google Scholar]
- 7.Behr SC, Courtier JL, Qayyum A. Imaging of müllerian duct anomalies. Radiographics. 2012;32(6):E233–50. doi: 10.1148/rg.326125515. [DOI] [PubMed] [Google Scholar]
- 8.Siegelman ES, Oliver ER. MR imaging of endometriosis: Ten imaging pearls. Radiographics. 2012;32(6):1675–91. doi: 10.1148/rg.326125518. [DOI] [PubMed] [Google Scholar]
- 9.Perino A, Chianchiano N, Simonaro C, Cittadini E. Endoscopic management of a case of ‘complete septate uterus with unilateral haematometra’. Hum Reprod. 1995;10(8):2171–73. doi: 10.1093/oxfordjournals.humrep.a136256. [DOI] [PubMed] [Google Scholar]
- 10.Channawar S, Chamariya S, Chauhan AR, Mayadeo NM. Robert’s Uterus. JPGO. 2014;1(2) Available from: http://www.jpgo.org/2014/02/roberts-uterus.html. [Google Scholar]
- 11.Li J, Yu W, Wang M, Feng LM. Hysteroscopic treatment of Robert’s uterus with laparoscopy. J Obstet Gynaecol Res. 2015;41(9):1491–94. doi: 10.1111/jog.12735. [DOI] [PubMed] [Google Scholar]
- 12.Ludwin A, Ludwin I, Martins WP. Robert’s septate uterus: Modern imaging techniques and ultrasound-guided hysteroscopic treatment without laparoscopy/laparotomy. Ultrasound Obstet Gynecol. 2016 doi: 10.1002/uog.15976. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]