

Abstract
Metastatic cardiac malignancies are significantly more common than primary cardiac tumors. Primary lung cancers often invade the heart locally and they can also spread to the heart via the blood, lymphatic system or both; in contrast, an extension to the left atrium from the pulmonary vein is very rare. Here, we report a case of a 79-year-old man with an acute neurological syndrome, in which an integrated multimodality imaging approach has allowed to discovery a lung cancer with cerebral embolism and intracavitary heart dissemination through the left superior pulmonary vein.
Keywords: Acute neurological syndrome, cerebral embolism, left atrial mass, lung cancer
INTRODUCTION
By the term cardiac metastases, we define distant spread of a tumor to any of the structures composing the heart and also tumors affecting the heart cavities or producing actual intracavitary neoplastic thrombi.[1] Any malignant neoplasm, in particularly melanoma, and lung and breast carcinoma can spread to the heart through four alternative paths: by direct extension, through the bloodstream, through the lymphatic system and by intracavitary diffusion through either the inferior vena cava or the pulmonary veins.[2]
We report a case of an elderly man with a lung cancer discovered after a metastatic diffusion to heart and brain.
CASE REPORT
A 79-year-old male presented to the emergency department with a confusional state characterized by clouded consciousness, disorientation in time and space, difficulty in speech and gait and mouth deviation to the right. He also showed dysarthria, right hemiparesis, hemi-hypoesthesia and Babinski sign, bilateral grasping-sign and a positive Epstein sign. He was a former heavy smoker, hypertensive and diabetic patient with a previous history of ischemic cardiomyopathy and prior vascular and cardiac surgery due to aneurysm of the abdominal aorta and myocardial infarction, respectively. A reduced breath sound on the right hemi-thorax was found at the chest examination while cardiac objectivity was unremarkable.
The electrocardiogram showed sinus rhythm with a heart rate of 65 beats/m,‘ some premature ventricular complex and left atrial enlargement. Chest X-ray revealed two nodular opacities on the right lung, the largest of which of 2.0 cm.
Owing to the neurological status, patient was immediately submitted to a noncontrast-enhanced computed tomography (CT) head scan demonstrating a large, but nonspecific cerebral edema in the right frontal, temporal and parietal lobe and then, referred to the Neurological Department of our institution.
A brain magnetic resonance imaging (MRI), a chest CT scan and a transthoracic echocardiogram (TTE) were quickly scheduled. This last identified a large, round-shaped mass, in the left atrium (LA), mobile during the cardiac cycle suspected to arise from left superior pulmonary vein. However, this approach failed to provide a full characterization of the lesion, comprehensive of size, morphology and spatial relationships with surrounding structures. Therefore, patient was immediately submitted to transesophageal echocardiogram (TEE). Through this examination we were able to:
Confirm that the mass came from the left superior pulmonary vein [Figure 1],
Evaluate its size (linear dimensions = 3.5 × 3.6 cm with a largest planimetric area of about 10 cm2) and morphology (inhomogeneous texture for the presence of anechogenic areas in the context of a hyperechogenic tissue [Figure 1] and
Rule out any hemodynamic consequence into the left cavities by color Doppler flow analysis.
Figure 1.
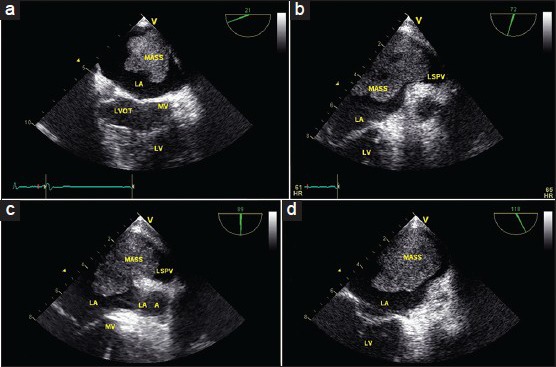
Multiplanar transesophageal echocardiogram shows the mass (a) coming from the left superior pulmonary vein (b and c) and prolapsing into the left atrium (d)
On the 2nd day, after admission, the prearranged brain MRI showed one heterogeneous, hypointense lesion, at the frontal right lobe, with perilesional vasogenic edema and partial compression of right lateral ventricle. Furthermore, an area of altered signal with “finger-like” appearance in the right cerebellar hemisphere, compatible with neoplastic edema was also identified [Figure 2a and b].
Figure 2.
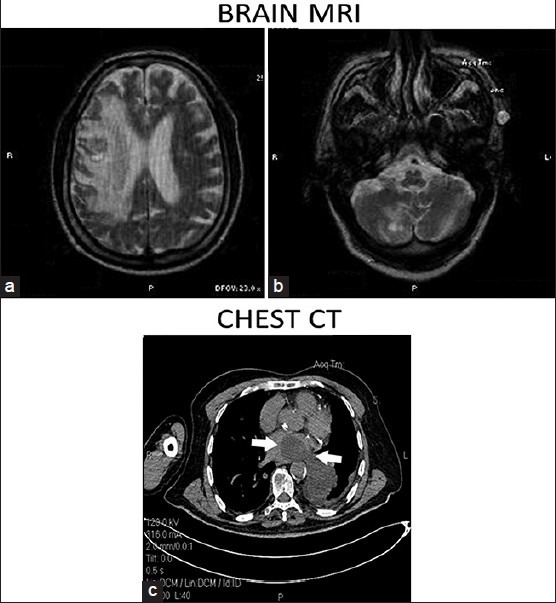
(a and b) Brain magnetic resonance imaging T2-weighted axial images (for explanations, please see the text). (c) Axial unenhanced computed tomography scan shows a left inferior pulmonary lobe solid mass that infiltrates left pulmonary veins and left atrium (white arrows)
Due to the above-mentioned imaging findings from cerebral and cardiac evaluation and in relation to the presence of nodular opacities on chest X-ray, a metastatic lung cancer was suspected. Accordingly, patient underwent chest CT scan showing a solid mass in the left inferior pulmonary lobe, infiltrating the left pulmonary veins and left atrium [Figure 2c]. Focal thickening of adjacent pleura was also seen and on parenchymal window, a pulmonary mass with maximum axial diameter of 57 mm was identified. Therefore, a starting diagnosis of lung cancer with brain metastases and intracavitary heart dissemination through the left superior pulmonary vein was made. However, to achieve a definitive diagnosis from histology, patient was scheduled for a biopsy of pulmonary lesions but, unfortunately, he suddenly died before we can conclude the diagnostic procedures.
DISCUSSION
The heart can be metastasized by any malignant neoplasm able to spread to distant sites, in particularly melanoma, lung tumors, breast carcinoma and linfoma.[1] Although primary cardiac tumors are extremely uncommon, secondary tumors are more frequent.
Lung tumors are the leading metastatic cancers that spread to the heart through direct invasion, and rarely extend into the chambers of the left side of the heart via pulmonary veins. Neoplastic thrombi can also be produced in the LA, after tumor embolism through the venous circulation of the lungs, mostly in patients with lung carcinoma. Large thrombi can even involve the mitral valve, and more commonly facilitate distant metastases.[1]
Although, extension from the pulmonary veins into the LA is rare, this circumstance has been reported in limited case reports.[2,3]
In lung carcinomas, rate of metastasis depends on the particular histotype. Adenocarcinoma spread to the heart in 26% of cases, squamous cell carcinoma in 23.4%, and undifferentiated carcinoma in 21.2%. Intra-pulmonary veins and intra-atrial masses can induce widespread emboli and circulatory impairment via outflow obstruction. In fact, sudden severe complications, including cerebral infarction, peripheral arterial occlusion and syncopal attacks have been reported in patients with this type of extension.[4]
Multimodality imaging approach should be used for the assessment of cardiac masses. Echocardiography, the first-choice modality, provides essential information with regard mass size, location, mobility, anatomical relationships, hemodynamic consequences and response to the treatment.[5] Especially, TEE adds important information, and it should always be considered when the transthoracic images are inappropriate, and in all the cases in which embolic sources are researched.
Particularly, echocardiography is helpful for LA masses differential diagnosis, including primary or secondary cardiac tumors,[6] infective endocarditis (IE)[7] and thrombi.[8,9,10] Despite, IE may be excluded on the basis of medical history and clinical data, echocardiography is anyway an important tool providing unique diagnostic elements. In general, infective vegetation presents as an oscillating mass attached to a valvular structure, with a motion independent to that of the valve, however it may also present as non oscillating masses with atypical location.[7] TEE enhances the sensitivity of TTE to about 85-90% for the diagnosis of vegetations, while more than 90% specificity has been reported for both TTE and TEE.[8] None of clinical and echocardiographic features in this case was suggestive of IE.
More challenging is the distinction between myxoma and non-myxomatous neoplasms. On echocardiography, myxomas appear as mobile masses attached to the endocardial surface through a stalk, usually arising from the interatrial septum in the region of fossa ovalis. They also have inhomogenous echogenecity and are highly mobile. However, 25% of myxomas may originate away from the atrial septum. In this case, the observed origin of the LA mass from pulmonary vein, by TEE, effectively allowed excluding a myxoma. However, in case the stalk is not clearly visible on echo, the diagnosis cannot be made by echocardiography and requires further imaging techniques, like MRI or CT.[9]
Fundamental is also the differential diagnosis with an atrial thrombus. Unlike myxoma, the thrombus usually lies on the wall of LA through a large base of implantation and can involve any segment, more often the LA appendage in patients with atrial fibrillation (AF). In some cases, LA thrombi may present with a stalk. A diagnosis of thrombus should be highly suspected if an LA mass is associated with AF, dilated LA, mitral stenosis, low ejection fraction, prosthetic mitral valves or spontaneous atrial contrast echoes.[10] None of these conditions was present in our case.
Through standard echocardiography, difficult remains the distinction between primary and secondary cardiac neoplasms. Nevertheless, as a general rule, nonseptal origin and pulmonary vein extension of the tumor strongly indicate the possibility of a secondary tumor.
Briefly, TTE and TEE have been fundamental tools for differential diagnosis in this case. However, it remains unclear whether the cerebral embolism presenting as an acute neurological syndrome was due to metastasis of the presumed primary lung cancer via bloodstream or to embolization of the LA mass.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Bussani R, De-Giorgio F, Abbate A, Silvestri F. Cardiac metastases. J Clin Pathol. 2007;60:27–34. doi: 10.1136/jcp.2005.035105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Dogan A, Icli A, Arslan A, Varol E, Ozaydin M. Metastatic atrial sarcoma extending from the lung into the left atrium via a pulmonary vein. Exp Clin Cardiol. 2012;17:77–8. [PMC free article] [PubMed] [Google Scholar]
- 3.Vojacek J, Burkert J, Pafko P, Mates M, Spatenka J, Pavel P. Extension of pulmonary adenocarcinoma into the left atrium. Asian Cardiovasc Thorac Ann. 2006;14:e99–e101. doi: 10.1177/021849230601400530. [DOI] [PubMed] [Google Scholar]
- 4.Collins NJ, Barlow MA, Woodford PA, Hayes PC. Intracardiac extension of metastatic pulmonary leiomyosarcoma. Heart Lung Circ. 2005;14:121–2. doi: 10.1016/j.hlc.2005.03.003. [DOI] [PubMed] [Google Scholar]
- 5.Ekmektzoglou KA, Samelis GF, Xanthos T. Heart and tumors: Location, metastasis, clinical manifestations, diagnostic approaches and therapeutic considerations. J Cardiovasc Med (Hagerstown) 2008;9:769–77. doi: 10.2459/JCM.0b013e3282f88e49. [DOI] [PubMed] [Google Scholar]
- 6.Pugliatti P, Donato R, Grimaldi P, Nunnari F, de Gregorio C, Zito C, et al. Extrinsic pulmonary stenosis in primary mediastinal B-cellular lymphoma. J Clin Ultrasound. 2014 doi: 10.1002/jcu.22133. [DOI] [PubMed] [Google Scholar]
- 7.Habib G, Badano L, Tribouilloy C, Vilacosta I, Zamorano JL, Galderisi M, et al. Recommendations for the practice of echocardiography in infective endocarditis. Eur J Echocardiogr. 2010;11:202–19. doi: 10.1093/ejechocard/jeq004. [DOI] [PubMed] [Google Scholar]
- 8.Zito C, Carerj S, Di Bella G, Spinelli F, Cavallari V, Coglitore S, et al. An unusual right heart mass. Cardiovasc Pathol. 2009;18:61–3. doi: 10.1016/j.carpath.2007.12.005. [DOI] [PubMed] [Google Scholar]
- 9.Scheffel H, Baumueller S, Stolzmann P, Leschka S, Plass A, Alkadhi H, et al. Atrial myxomas and thrombi: Comparison of imaging features on CT. AJR Am J Roentgenol. 2009;192:639–45. doi: 10.2214/AJR.08.1694. [DOI] [PubMed] [Google Scholar]
- 10.Diaconu CC. Left atrial thrombus: A case report. J Med Life. 2011;4:417–8. [PMC free article] [PubMed] [Google Scholar]