

Abstract
Takotsubo cardiomyopathy (TC) is characterized by transient systolic dysfunction of the apical and middle segments of the left ventricle, accompanied by electrocardiographic abnormalities and mild elevation of cardiac biomarker levels in the absence of obstructive coronary artery disease. The following case is of a woman suffering from chronic emotional stress with a very early recurrence. An acute trigger event was not detectable in both cases. It is possible to suppose that, in predisposed subjects, chronic stress by increasing sympathetic activity may be considered not only a trigger for TC, but also a negative prognostic factor for early recurrence.
Keywords: Takotsubo cardiomyopathy, chronic stress, myocardial infarction
INTRODUCTION
Takotsubo cardiomyopathy (TC) is a cardiomyopathy characterized by typical wall motion abnormalities of the left ventricle whose most frequently resembles the “takotsubo” used by Japanese for catching octopuses. It mimics an acute coronary syndrome, but the coronary angiography typically reveals the absence of an obstructive atherosclerotic disease and the echocardiographic segmental wall abnormalities typically occur beyond the territory of perfusion of a coronary single vessel.[1] The causes are still unclear and the syndrome may be thought as a neurogenic disorder due to an acute physical and emotional stress with excessive sympathetic activity and abnormal catecholamine release.[2] TC is currently considered a quite benign condition, with a complete recovery in few days or weeks. However, the recurrence, once thought to be rare, has been increasingly reported worldwide. In a recently published review of literature, it has been evidenced in a significant heterogeneity among studies with an annual recurrence of roughly 1.5%. Cumulative incidence of recurrent events increased from 1.2% in the first six months to nearly 5% in six years. Unfortunately, the relatively small number of recurrences has still now precluded the identification of predictors of outcome. Interestingly, medical therapy (ACE-I and ARB rather than b-blockers) discontinuation may have an impact in the risk of recurrence.[3] Both precocious (one year)[4] and very late (about 10 years) repeated episodes have been previously described[5] with the possibility of variable patterns of left ventricular region involvement.[6,7]
CASE REPORT
A 61-year-old woman was referred to our department for acute chest pain. She was a smoker with positive family history for cardiovascular disease. She reported chronic stress related to the handicap of her daughter and frequent family quarrels. Upon admission, she was symptomatic for typical chest pain. Clinical examination was unremarkable. The admission electrocardiogram showed negative T-waves in V4-V6 leads [Figure 1], and markers of myocardial necrosis were mildly elevated (maximum I troponin: 1.5 ng/dl). Transthoracic echocardiogram revealed apical and mid-segment akinesis with hyperkinesia of basal segments and a moderately impaired systolic function (ejection fraction 45%) [Figure 2]. We suspected Takotsubo cardiomyopathy. The patient underwent coronary angiography that revealed a non-significant stenosis of the anterior descending artery. The left ventriculogram confirmed our suspicion [Figure 3]. Before discharge, we assessed diffuse negative T-waves on electrocardiogram and normalization of segmental kinesis on transthoracic echocardiogram. After the discharge, the patient discontinued medical therapy with β-blockers, ACE inhibitors and mineral receptor antagonist, for symptomatic hypotension. Two months later, she suffered acute chest pain again. Transthoracic echocardiogram showed a typical apical ballooning pattern [Figure 2], maximum troponin I was 0.11 ng/dl. Given the previous medical history and recent detection of non-significant coronary lesions, coronary angiography was not repeated, and the patient was conservatively treated and her hospital course was uncomplicated. Her pre-discharge transthoracic echocardiogram showed normalization of segmental kinesis. The patient is in good health and is followed-up in our institution.
Figure 1.
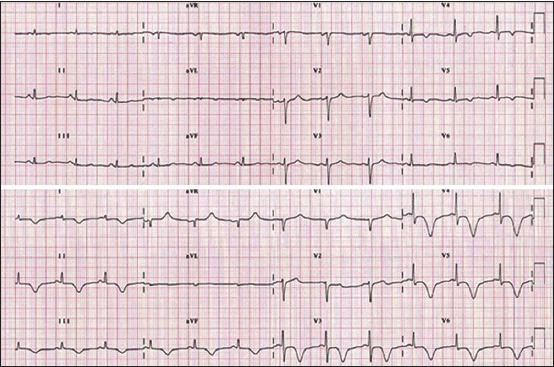
Electrocardiogram registered upon admission (upper panel) and before discharge (lower panel)
Figure 2.
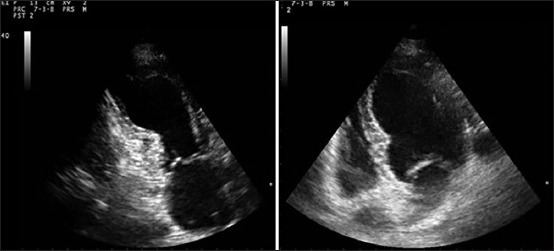
Transthoracic echocardiogram recorded during the second in-hospital admission and showing apical akinesis, with basal segments hyperkinesis (left systolic frame, right diastolic frame)
Figure 3.
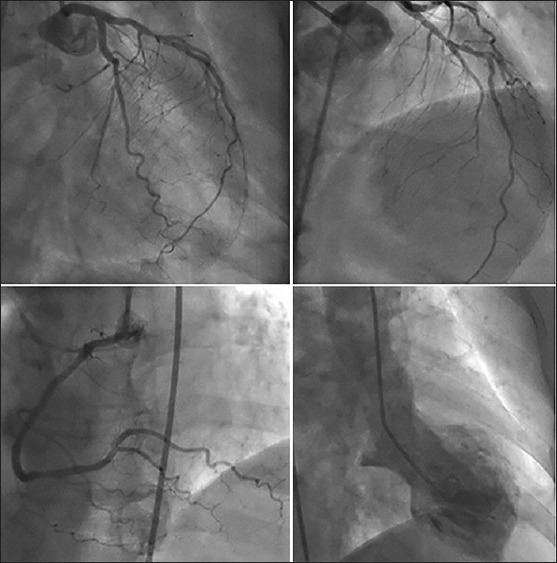
Coronary angiography showing non-significant atherosclerotic lesions and ventriculography showing apical ballooning of the left ventricle
CONCLUSIONS
The reaction to psychological stress is well-characterized but its link with cardiovascular disease risk is less established. Epidemiological data show that chronic stress predicts the occurrence of coronary artery disease; in addition, short-term emotional stress can act as a trigger of cardiac events in people with advanced atherosclerosis.[8] An acute emotional or physical stress is typical of TC, even if not always detectable. The influence of chronic stress and psychiatric illness in the pathogenesis of TC is far less studied. In some studies, high-anxiety trait is a common finding but it is not significantly more frequent than in control patients with myocardial infarction. Moreover, a high-anxiety trait seems to be neither associated with a worse outcome nor a predictor of TC.[9] In other studies, a psychiatric disorder in TC was detectable in up to 50% of cases.[10] Patients with TC and chronic stress may have a higher catecholamine response to minor stressful situations and decreased inhibition of catecholamine with longer cardiac stimulation. We report an unusual case of TC in a woman suffering from chronic emotional stress with a very early (one month) recurrence. An acute, physical or emotional, trigger event was not detectable in both cases. It is possible to suppose that, in predisposed subjects, chronic stress by increasing sympathetic activity may be considered not only a trigger for TC, but also a negative prognostic factor for early recurrence. Future studies may demonstrate an increased prevalence of psychiatric disorders or chronic stress in patients with TC and, on the other hand, a high prevalence of TC in patients with psychiatric diseases.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Novo S, Akashi Y, Arbustini E, Assennato P, Azzarelli S, Barbaro G, et al. Takotsubo cardiomyopathy: A consensus document. G Ital Cardiol (Rome) 2008;9:785–97. [PubMed] [Google Scholar]
- 2.Maroules CD, Linz NA, Boswell GE. Recurrent Takotsubo cardiomyopathy. J Cardiovasc Comput Tomogr. 2009;3:187–9. doi: 10.1016/j.jcct.2009.03.001. [DOI] [PubMed] [Google Scholar]
- 3.Singh K, Carson K, Usmani Z, Sawheney G, Shah R, Horovitz J. Systematic review and meta analysis of incidence and correlates of recurrence of takotsubo cardiomyopathy. Int J Cardiol. 2014;174:696–701. doi: 10.1016/j.ijcard.2014.04.221. [DOI] [PubMed] [Google Scholar]
- 4.Cemin R, Oberhollenzer R. Annual recurrence of acute left ventricular apical ballooning. Int J Cardiol. 2007;119:237–8. doi: 10.1016/j.ijcard.2006.07.119. [DOI] [PubMed] [Google Scholar]
- 5.Cerrito M, Caragliano A, Zema D, Zito C, Oreto G. Very late recurrence of Takotsubo syndrome. Ann Noninvasive Electrocardiol. 2012;17:58–60. doi: 10.1111/j.1542-474X.2011.00481.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Xu B, Williams PD, Brown M, Macisaac A. Takotsubo cardiomyopathy: Does recurrence tend to occur in a previously unaffected ventricular wall region? Circulation. 2014;129:e339–40. doi: 10.1161/CIRCULATIONAHA.113.007015. [DOI] [PubMed] [Google Scholar]
- 7.Singh K, Parsaik A, Singh B. Recurrent takotsubo cardiomyopathy: Variable pattern of ventricular involvement. Herz. 2013 doi: 10.1007/s00059-013-3896-x. [DOI] [PubMed] [Google Scholar]
- 8.Steptoe A, Kivimäki M. Stress and cardiovascular disease. Nat Rev Cardiol. 2012;9:360–70. doi: 10.1038/nrcardio.2012.45. [DOI] [PubMed] [Google Scholar]
- 9.Del Pace S, Parodi G, Bellandi B, Zampini L, Venditti L, Ardito M, et al. Tuscany Registry of Tako-tsubo Cardiomyopathy. Anxiety trait in patients with stress-induced cardiomyopathy: A case-control study. Clin Res Cardiol. 2011;100:523–9. doi: 10.1007/s00392-010-0276-x. [DOI] [PubMed] [Google Scholar]
- 10.Nguyen SB, Cevik C, Otahbachi M, Kumar A, Jenkins LA, Nugent K. Do comorbid psychiatric disorders contribute to the pathogenesis of tako-tsubo syndrome. A review of pathogenesis? Congest Heart Fail. 2009;15:31–4. doi: 10.1111/j.1751-7133.2008.00046.x. [DOI] [PubMed] [Google Scholar]