

Abstract
Background:
Acne is a very common skin disease in which scars are seen in 95% of the patients. Although numerous treatments have been recommended, researchers are still searching for a single modality to treat the complication due to its variety in shape and depth. We compared the effects of fractional carbon dioxide (CO2) laser alone and in combination with subcision in the treatment of atrophic acne scars.
Materials and Methods:
This clinical trial study was performed in Skin Diseases and Leishmaniasis Research Center (Isfahan, Iran) during 2011–2012. Eligible patients with atrophic acne scars were treated with fractional CO2 laser alone (five sessions with 3-week interval) on the right side of the face and fractional CO2 laser plus subcision (one session using both with four sessions of fractional CO2 laser, with 3-week interval) on the left side. The subjects were visited 1, 2, and 6 months after the treatment. Patient satisfaction rate was analyzed using SPSS 20 software.
Results:
The average of recovery rate was 54.7% using the combination method and 43.0% using laser alone (P < 0.001). The mean patient satisfaction was significantly higher with the combination method than laser alone (6.6 ± 1.2 vs. 5.2 ± 1.8; P < 0.001). Bruising was only seen with the combination method and lasted for 1 week in 57.0% and for 2 weeks in 43.0%. Erythema was seen in both methods. Postinflammatory pigmentation and hyperpigmentation were associated with combination method. No persistent side effects were seen after 6 months.
Conclusion:
Using a combination of subcision and laser had suitable results regarding scar recovery and satisfaction rate.
Keywords: Atrophic acne scar, fractional carbon dioxide laser, subcision
Introduction
Acne is the most common skin disease in a way that almost every teenager is affected by it to some degree. However, this disease is not limited to a certain age group.[1] It is so widespread that we consider it as a normal event in growing process. It occurs in boys with the age of 16–17 years up to 95–100% and in girls of these ages; the recurrence percent is 83–85%.[2] In most cases, acne recovers in ages 23–25, but in 1% of men and in 5% of women, it continues up to 40.[3] Although acne automatically recovers after several years, we cannot leave it alone. Because if acne is not treated, it may leave ugly scars on skin.[4] This disease happens because sebaceous glands of skin obstruct and after that, acne becomes worse when infection and microbial factors are added to it.
Using enough drug intervention may prevent scars at the beginning phase of the disease. But unfortunately, both surfaces of inflamed and cystic acne lead to scar, and scar occurs in 95% of acne durability before starting treatment.[5] In young age, most scars recover in 2–3 years, but in later years, when skin's firmness decreases and skin oil supply absorbs, scars specifies. From routine treatment, we can mention to coverings, use of topical drugs such as tretinoin, hydroquinone, AHA, Vitamin C, use of gels and silicone and nonsilicone sheets, intralesional corticosteroid injections, Cryotherapy, soft tissue fillers, peeling and microdermabrasion, intense-pulsed light laser, and radiofrequency. Today, some less successful treatments such as dermabrasion and chemical peeling are replaced by ablative carbon dioxide (CO2) lasers and Er-YAG lasers.[6,7] Also, because there is a need to replace the atrophic dermal tissue and subcutaneous tissue in severe cases, upper dermal layers or subcutaneous fillers techniques by doing several autologous techniques such as collagen planting or autologous fibroblasts is common. As acne scars are various regarding the shape and deepness, to reach satisfactory results, we need a combination of these methods. Different classifications are suggested for these scars. In Coranda Consensus Conference scale, acne scars are divided into three types: (1) Hypertrophic and keloid (2) hole or the shape of a volcano crater (3) ice pick shape.[8]
Fractional laser known as fraxel laser is a new generation of skin rejuvenation method using laser developed technology that divides laser ray to thousands of microscopic beams. For this job, 1550 nm erbium laser fibers are used. This laser targets tissues containing water. This is done by narrow skin columns. This method is effective in light-induced skin damages in face and other parts of the body, atrophic acne scars, hypopigmentated scars, and dispigmentated scars.
In one session of treatment, just one part of the body is treated, so 3–6 sessions of treatment with 2–4-week interval are needed.[9] This method does not have any significant side effects and desirable satisfaction was reported.[10]
Fraxel laser affects the surface and central layer of the skin, so it has an extraordinary effect on the skin rejuvenation.
The advantage of fraxel laser when compared to the previous laser is making less damage to the skin as it just affects part of the skin in the form of heater columns. Hence, healing and recovery after the laser happens sooner. Long-lasting side effects after laser such as long duration redness, skin blotches, and scar rarely happen when compared with previous lasers.
Subcision is a simple and certain surgical method for treating atrophic acne scar in which the scar levels are made free from the underneath connections and it decreases the connective tissue formation under the scar without making any damage to the skin surface. Hence, subcision is a valuable method, but as it has a high risk of recurrence, the effectiveness of this method is considered low to medium.[11] For more effectiveness, it can be combined with other methods such as laser.[12]
Side effects such as swelling, bruising, and pain are not stable, but it is possible that in the place of treatment, the swelling remains stable and enduring.[13] In this study, we used G28 needle for each scar separately, but in other studies, subcision was done by nokor needle totally on the scar surface, for example, on the cheeks.
This study aimed to compare the effectiveness of two treatment methods of subcision and fractional CO2 laser and fraxel laser in recovering the atrophic acne scars.
Materials and Methods
This clinical trial study was done on 30 patients with ice pick type and rolling-type atrophic acne scars, referred to Sedigheh Tahereh Research Center of Skin Disease and Leishmaniasis, Isfahan, in 2011–2012. The sample size was calculated using sample size formula with d = 0.3 [Figure 1].
Figure 1.

CONSORT 2010 flow diagram
Inclusion criteria include no pregnancy and lactation, no use of any oral or topical drugs in the recent 6 months, not affected by any disease or active skin infection such as impetigo, herpes simplex, flat wart, or serious skin disease history, and no tendency of keloid. No acne rosacea and not having any psychological disorders. In addition, the patients who did not agree to continue the research were excluded from the study.
Patients were selected based on their needs to entering the study and after the method was explained to them, they filled the consents. Then, each one was treated on the right side of their face in 5 sessions of treatment with 3-week interval by fractional CO2 laser and on the left side of the face, they were treated in a session by subcision with laser (energy 30 pulse, 1 pixel pitch, and Dot cycle 6 with DOSIS M and M, Q ray FRX machine made in Korea) and after 3 weeks, 4 sessions of fractional CO2 laser with 3-week interval were done for them. The status of the scars was almost the same in both sides of the patients’ faces and the side for the two treatment methods was randomly selected.
One hour before subcision, the patients were anesthetized topically by lidocaine P cream under the plastic covers. Then, an insulin needle was entered near the scar and parallel to the skin level, under the scar, and deep in derm, with a fan-like movement to make the fibrose band in derm or subcutaneous surface deep derm, it moved forward and backward. By using the needle, the surgery place passed in order to evacuate extra blood. After using the needle, operation site would pass to evacuate extra blood. This action prevents from making a big hematome. A little hematome is just allowed to protect the place of free scar.
An ice pack was put on the subcision place, and antibiotics and anti-inflammatory drugs were prescribed during 5–7 days after surgery. The laser system was Energy 30, 1 pixel pitch, and dotcyle, and laser type was dosis M and M, Q ray FRX.
The patients were visited 1 and 2 months after treatment. Recovery after 6 months of the treatment was evaluated by comparing previous photos and recent photos and by an ignorant doctor evaluated separately from the kind of treatment based on percent and patient's satisfaction 6 months after the treatment was reported in five levels: (1) I’m not satisfied (2) I’m semi-satisfied (3) I’m satisfied (4) I’m so satisfied (5) I’m completely satisfied, and by visual analog scale score. Side effects were compared in both groups. Information was entered in a computer separately and analyzed by SPSS-18 software (SPSS Inc., Chicago, Illinois, USA) using ANOVA and Wilcoxon rank-sum test.
Results
In this study, 30 patients were affected by atrophic acne scar, ice pick type, and rolling; 80% of the scars was of rolling type, 10% of the scars was of ice pick type, and the rest was of other types. The objects comprised 8 men (26.7) and 22 women (73.3). On the right side of each patient's face, fractional CO2 laser alone and on the left side of the face, fractional CO2 laser with subcision was used. Tables 1 and 2 show the comparison of recovery level and patient's satisfaction.
Table 1.
Recovery level and patient's satisfaction in both groups
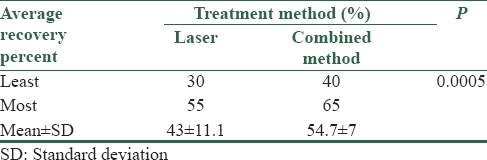
Table 2.
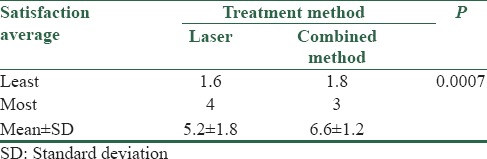
Satisfaction status in both groups
As shown in Table 1, the average recovery percent in the combined method was 54.7 ± 7 and in another method, it was 43 ± 11.1. The recovery average was significantly more than laser alone in a combined method (P < 0.001). The comparison of the satisfaction status in both groups is shown in Table 2.
As shown in Table 2, the satisfaction average in a combined method was 6.6 ± 1.2 and in laser method alone, it was 5.2 ± 1.8.
There was a significant difference between satisfaction average in the combined method and laser method alone (P < 0.001), and it was higher in the former. Bruising side effects, PIP, and hyper pigmentation existed just in combined method, but erythema side effects were seen in both groups.
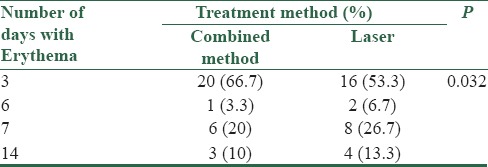
Table 3 shows the state of erythema side effects in both groups. After 6 months, there were no side effects in any of them.
Table 3.
Erythema side effects in both groups
Discussion
Subcision is a simple and certain method selected in patients with atrophic acne scars; it leads to durable and desirable recovery effects with better reply to rolling scars.[13]
Subcision can combine with other methods with certainty and simplicity. Hence, subcision is a valuable method, but because of high risk of recurrence, the effectiveness was considered as low to medium. Suction–subcision is a new combined successful treatment for curing the atrophic acne scars and other depressed scars.[11]
In a study with the use of combination of three methods such as subcision, dot peeling, and laser to treat acne scars, the results showed that severe acne scars decreased up to 53.3% and 80% of the patients recovered, and there was not any significant side effects in the treatment place. It seems that triple treatment can be a certain and effective method in curing atrophic acne scars.[4]
In another similar study, the patients who had undergone subcision reported that it enhanced the outcomes versus the patients who had not.[8]
The result of our study showed subcision with fractional CO2 laser had 54.7% and fractional CO2 laser alone had 43% of recovery. The average recovery rate in the combined method was significantly more than fractional CO2 laser alone.
In addition, satisfaction average of combined method was 6.6% and in fractional laser, it was 5.2%, which showed a significant raise in combined method than fractional laser alone, and it may concluded that laser can be done with subcision. If so, the cure may be reached to the desirable results.
In a study on the subcision method, it has reported that there was 60–90% improvement in depth and size of scars (significant improvement) in the patients with mean 71.73%. About 28.2% of them had “80% improvement or more” (excellent improvement).[11]
Bruising side effects, PIP, and hyperpigmentation was seen in combined method, but 6 months after treatment, there was no sign of them.
To increase the effect of subcision, we can add the sessions of treatment by fractional CO2 laser.
We can finally suggest that fractional CO2 laser in combination with subcision increases subcision efficacy remarkably and causes significant and persistent improvement in a short time, without considerable complication, in depressed scars of the face.
Conclusion
The combination of Fractional carbon dioxide laser and subcision is a safe and effective modality for the treatment of rolling and ice pick acne scars.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors express their gratitude to, Sedigheh Tahereh Research Center of Skin Disease and Leishmaniasis, Isfahan, and also to Novin Laser clinic.
References
- 1.Fife D, Zachary CB. Combining techniques for treating acne scars. Curr Dermatol Rep. 2012;1:82–8. [Google Scholar]
- 2.Fife D. Practical evaluation and management of atrophic acne scars: Tips for the general dermatologist. J Clin Aesthet Dermatol. 2011;4:50–7. [PMC free article] [PubMed] [Google Scholar]
- 3.Hwang EJ. The efficacy and safety of new total combination techniques compared with classic sequential combination therapy with punch, fractional and long-pulsed Er-YAG laser for the treatment of acne scars. J Am Acad Dermatol. 2011;64:AB168. [Google Scholar]
- 4.Kang WH, Kim YJ, Pyo WS, Park SJ, Kim JH. Atrophic acne scar treatment using triple combination therapy: Dot peeling, subcision and fractional laser. J Cosmet Laser Ther. 2009;11:212–5. doi: 10.3109/14764170903134326. [DOI] [PubMed] [Google Scholar]
- 5.Khunger N. Standard guidelines of care for acne surgery. Indian J Dermatol Venereol Leprol. 2008;74(Suppl):S28–36. [PubMed] [Google Scholar]
- 6.Woo SH, Park JH, Kye YC. Resurfacing of different types of facial acne scar with short-pulsed, variable-pulsed, and dual-mode Er: YAG laser. Dermatol Surg. 2004;30(4 Pt 1):488–93. doi: 10.1111/j.1524-4725.2004.30161.x. [DOI] [PubMed] [Google Scholar]
- 7.Weiss RA, Weiss MA, Beasley KL, Munavalli G. Autologous cultured fibroblast injection for facial contour deformities: A prospective, placebo-controlled, Phase III clinical trial. Dermatol Surg. 2007;33:263–8. doi: 10.1111/j.1524-4725.2007.33060.x. [DOI] [PubMed] [Google Scholar]
- 8.Taub AF, Garretson CB. Treatment of acne scars of skin types II to V by sublative fractional bipolar radiofrequency and bipolar radiofrequency combined with diode laser. J Clin Aesthet Dermatol. 2011;4:18–27. [PMC free article] [PubMed] [Google Scholar]
- 9.Tanzi EL, Wanitphakdeedecha R, Alster TS. Fraxel laser indications and long-term follow-up. Aesthet Surg J. 2008;28:675–8. doi: 10.1016/j.asj.2008.09.006. [DOI] [PubMed] [Google Scholar]
- 10.Hu S, Chen MC, Lee MC, Yang LC, Keoprasom N. Fractional resurfacing for the treatment of atrophic facial acne scars in Asian skin. Dermatol Surg. 2009;35:826–32. doi: 10.1111/j.1524-4725.2009.01139.x. [DOI] [PubMed] [Google Scholar]
- 11.Aalami Harandi S, Balighi K, Lajevardi V, Akbari E. Subcision-suction method: A new successful combination therapy in treatment of atrophic acne scars and other depressed scars. J Eur Acad Dermatol Venereol. 2011;25:92–9. doi: 10.1111/j.1468-3083.2010.03711.x. [DOI] [PubMed] [Google Scholar]
- 12.Chandrashekar B, Nandini A. Acne scar subcision. J Cutan Aesthet Surg. 2010;3:125–6. doi: 10.4103/0974-2077.69029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Alam M, Omura N, Kaminer MS. Subcision for acne scarring: Technique and outcomes in 40 patients. Dermatol Surg. 2005;31:310–7. doi: 10.1111/j.1524-4725.2005.31080. [DOI] [PubMed] [Google Scholar]