

Abstract
Background
Accumulating evidence has demonstrated that cyclooxygenase-2 (COX-2) is involved in head and neck cancers, especially in nasopharyngeal carcinoma (NPC). However, the association between COX-2 expression and lymph node metastasis in NPC remains uncertain. This systematic review and meta-analysis meta-analysis investigated the relationship between COX-2 expression and lymph node metastasis and other signs of disease progression in NPC.
Methods
Previously published studies assessing COX-2 expression and lymph node metastasis in NPC were identified in four English databases and three Chinese ones (Pubmed, Embase, Cochrane Database of Systematic Reviews, Web of Science, China National Knowledge Infrastructure, Wanfang, Vip Journal Integration Platform) up to November 2016. Quality of all eligible studies was assessed using the Newcastle-Ottawa Quality Assessment Scale (NOS). Pooled odds ratios (OR) and their 95% confidence intervals (95%CI) were calculated with fixed-effects or random-effects model to evaluate the effects of COX-2 expression on lymph node metastasis.
Results
A total of 27 studies with 1797 NPC patients met the inclusion criteria. The expression of COX-2 was significantly higher in patients with nasopharyngeal carcinoma than those without the carcinoma, with a combined OR of 21.17 (95%CI = 15.02–29.85, I2 = 35.1%, Pheterogeneity = 0.070). A statistically significant association between COX-2 expression and lymph node metastasis in NPC patients, with an OR of 4.44 (95%CI = 3.46–5.70, I2 = 38.3%, Pheterogeneity = 0.024), and with other indicators of disease progression. Subgroup analyses based on COX-2 assay and staging criteria of TNM showed no significant heterogeneity.
Conclusions
The results suggest that expression of COX-2 is associated with lymph node metastasis and disease progression in NPC, indicating a potential role in evaluation of prognosis and in treatment decisions. COX-2 inhibitors have potential in the treatment of NPC that should be further investigated.
Introduction
Nasopharyngeal carcinoma (NPC) is an epithelial malignancy arising from the epithelium of the nasopharynx[1]. It is most common in Southeast Asia, especially in Southern China, and parts of North Africa, and is also seen among indigenous Eskimos living in Greenland and Alaska[2]. Epidemiological studies have suggested that environmental and lifestyle factors, including alcohol, diet and tobacco smoking, play an important role in the etiology of NPC, along with the Epstein–Barr virus (EBV)[3, 4].
The American Joint Committee on Cancer (AJCC) TNM classification of malignant tumors, based on anatomical information, is currently the most commonly used staging system and is used to determine treatment regimens for NPC patients[5]. NPC can invade tissues adjacent to the nasopharynx and even metastasize via blood or lymphatic system to bone and organs such as the liver and lungs[6]. A high proportion (70%-80%) of NPC patients present with cervical lymph node metastases when they are first diagnosed. Early lymph node metastasis and the high incidence rate of distant metastases are responsible for 15% to 42% of treatment failures and represent a significant problem[7].
Increasingly research has recognized that inflammation and the inflammatory microenvironment play an important role in cancer development. Cyclooxygenases, as inflammatory regulators, are responsible for the conversion of arachidonic acid to prostaglandin H2 (PGH2). While one COX isoform, cyclooxygenase-1 (COX-1), is constitutively expressed in most normal tissues and involved in physiological processes under most circumstances[8], a second, cyclooxygenase-2 (COX-2), is an inducible type activated by inflammation or carcinogenic factors. COX-2 can be rapidly induced by mitogenic and inflammatory stimuli, but is usually absent in most normal tissues[9].
Research has shown that COX-2 plays an important role in the carcinogenesis of head and neck cancers (HNC), and in the progression of cancers through modulating cell proliferation and apoptosis in ways that favor tumor growth and metastasis, thus affecting the efficacy of therapies. Therefore, the expression of COX-2 has been proposed as a potential prognostic indicator for prediction of survival in HNC patients, while COX-2 inhibitors may have potential functions as therapeutic agents [10, 11].
However, whereas some studies have concluded that the levels of COX-2 increase when lymph node metastasis occurs in NPC, others have failed to find significant correlations. With insufficient evidence on the association between COX-2 expression and NPC advancement, COX-2’s diagnostic and prognostic values and the role of COX-2 inhibitors in clinical practice remain uncertain.
The purpose of this study was to further investigate the relationship between COX-2 expression and NPC advancement, in particular lymph node metastasis, by systematic review and meta-analysis of existing evidence.
Methods
This systematic review and meta-analysis was conducted according to the guidelines of the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement [12].
Inclusion and exclusion criteria
Studies fulfilling the following criteria were eligible for inclusion:
study subjects were human; no restrictions were imposed on the number of samples included in studies;
methods used to examine COX-2 expression were immunohistochemistry (IHC) or reverse transcription-polymerase chain reaction (RT-PCR) or real-time polymerase chain reaction (real time PCR);
histologically proven NPC patients were distinguishable in two groups: lymph node metastasis group (LNM) and non-lymph node metastasis group (NLNM);
the relationship between COX-2 expression and lymph node metastasis in NPC patient were evaluated and Odds Ratio (OR) and its 95% confidence intervals (CI) for the COX-2-positive or COX-2 high expression rate in the two groups were respectively reported; or else, sufficient data were reported for their calculation;
studies published in English or Chinese language with full text. No restrictions were imposed on region.
If more than one published article by the same authors or group was identified reporting the same data set, the latest article was included. Studies were excluded that considered potentially overlapping study populations, treated cell lines as research objects were performed in vitro, or lacked necessary information for the calculation of ORs. Conference abstracts were also excluded as these seldom provide sufficient information to assess methodology.
Publication search
Literature searches were conducted in Embase, PubMed, Cochrane Database of Systematic Reviews, Web of Science, China National Knowledge Infrastructure (CNKI), Wanfangdata and Vip Journal Integration Platform (VIP) for potentially relevant articles published up to November 2016. Search strategy included the following terms: ((Cyclooxygenase-2) OR (COX-2) OR (PTGS2)) AND ((Nasopharyngeal cancer) OR (Nasopharyngeal carcinoma) OR (Nasopharyngeal neoplasm) OR (Nasopharyngeal tumor) OR (NPC)). Additional pertinent studies were sought through hand searching the bibliographies of identified studies and related meta-analyses. Studies identified by the searches were collated in EndNote X7. After excluding duplicates, titles and abstracts were screened independently by two investigators to remove citations that were clearly ineligible. The full texts of potentially eligible studies were obtained and reviewed in detail independently by the two reviewers. At both stages any disagreements about selection were discussed by the two reviewers to reach a consensus according to the inclusion and exclusion criteria.
Data extraction
From each eligible article, two investigators independently abstracted information about the first author's name, year of publication, study country, methods for COX-2 detection, COX-2 positivity, TNM malignant tumor classification, clinical stage, metastasis status LNM (N0) and NLNM (N1, N2, N3), metastasis stage, tumor size stage, differentiation types and sex. For studies that presented both univariate and multivariate analyses, data were extracted from the latter type because such analyses take into account potential influences of predictive or confounding factors.
Quality of eligible studies
The quality of the included studies was evaluated using the Newcastle-Ottawa Scale (NOS) [13] by two reviewers independently. The stars rating system with a highest score of 9 considers three domains: selection of the study population; comparability and exposure assessment.
Statistical methods
For all analyses, non-lymph node metastases N1, N2 and N3 were combined; malignant tumor classification T1 and T2 were combined, as were T3 and T4; clinical stage I and stage II were combined, as were stage III and stage IV; high differentiation and moderate differentiation were combined, as were low differentiation and dedifferentiation. As the AJCC and UICC NPC staging systems are similar, they were combined for principal analyses. OR was obtained as A vs B. Pooled OR and 95%CI were calculated based on primary data from the selected studies. An OR > 1 implied a higher susceptibility of lymph node metastasis in COX-2-positive NPC patients when 95%CIs did not include 1 (p < 0.05). Statistical heterogeneity among studies was evaluated with the Cochran Chi square-based Q-test and I square test. All tests were two-tailed, and heterogeneity was considered statistically significant when the Cochran Q test p value was less than 0.10 and I2 value was greater than 50%. We combined OR using fixed-effects model (the Mantel-Haenszel method) unless significant heterogeneity was indicated, in which case random-effects model (the DerSimonian-Laired method) was used. Sensitivity analysis was conducted by sequentially omitting selected study to evaluate their effects on pooled OR and 95% CI. Subgroup analyses were conducted to consider variations in findings according to assays used, NPC staging systems used and sex, tumor size stage, metastasis stage, clinical stage and histological differentiation stage. Begg's funnel plot was created to estimate potential publication bias and Egger's test was used to check the symmetry of funnel plots. We considered publication bias to be negligible when p < 0.05 from Egger’s test. All analyses were performed using Stata14.0 Statistical Software.
Results
Selection of studies
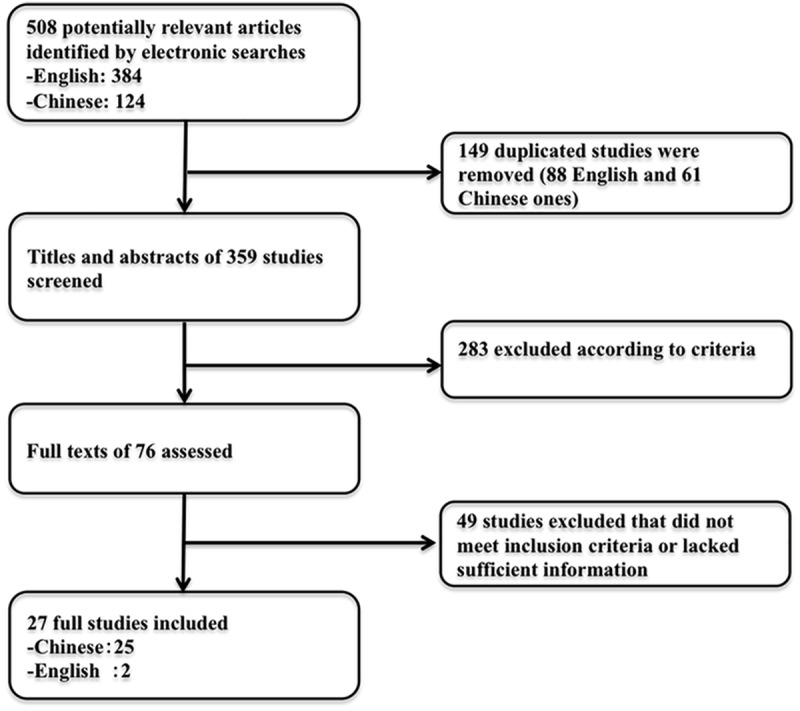
A total of 508 potentially relevant studies were identified by our search strategy. After 149 duplicates were removed, the titles and abstracts of the remaining 359 were screened and 283 studies rejected. After full text assessment, 49 papers that did not meet the eligibility criteria or lacked essential information were rejected, so that 27 studies published after 2004 with 1797 NPC patients were included in our analysis. A flow diagram of article selection is given in Fig 1.
Fig 1. Flow diagram of articles selection.
Characteristics of included studies
The main characteristics of the 27 included studies are summarized in Table 1. Two studies were written in English[14, 15], while the rest were Chinese articles[16–40]. Among the 1797 cases in the included studies, there were 1265 patients with lymph node metastasis and 532 NPC patients without metastasis, and 1346 cases with COX-2 expression and 451 cases without. The cumulative lymph node metastasis rate and COX-2-positive rate of NPC were 70.40% (1265/1797) and 74.90% (1346/1797), respectively. The cumulative COX-2 expression rates were 82.69% (1046/1265) in the LNM group and 56.39% (300/532) in the NLNM group (Table 2). Immunohistochemistry (IHC) was the main method for the evaluation of COX-2 expression in NPC specimens, with 17 studies using IHC-SP and another 5 studies using IHC-SABC. The remaining studies did not reporting detailed information on which IHC assay was used. One study assessed COX-2 mRNA expression with RT–PCR and one with both IHC and real-time PCR. Seven studies used the AJCC/UICC staging system, while seven used the 1992 Chinese staging system. Methodological appraisals of the included studies using the Newcastle Ottawa scale are presented in Table 3.
Table 1. Main characteristics of included studies.
| First author-Year | Country | COX-2 assay | Classification | Patients | Control | Age | NLNM | LNM |
|---|---|---|---|---|---|---|---|---|
| Xu Xinhua-2006 | China | IHC-SP | China 1992 | 86(63) | 10(0) | Median 46 | 10(4) | 76(59) |
| Jiang Daihua-2004 | China | IHC-SABC | - | 62(48) | 10(0) | Mean 48.98 | 18(17) | 44(31) |
| Gu Shanzhi-2006 | China | IHC-SP | China 1992 | 78(40) | - | Median 46 | 24(5) | 54(35) |
| Zhou Leyuan-2006 | China | IHC | China 1992 | 43(34) | - | Mean 54.9 | 7(5) | 36(29) |
| Dou Yanling-2006 | China | IHC-SABC | - | 39(35) | - | Mean 51.2 | 20(16) | 19(19) |
| Luo Weireng-2006 | China | IHC-SP | - | 95(65) | 26(7) | - | 65(40) | 30(25) |
| Fu Yafeng-2007 | China | IHC | China 1992 | 53(46) | 23(10) | - | 21(17) | 32(29) |
| Zhou Fang-2007 | China | IHC-SP | - | 45(32) | 20(2) | Mean 60.3 | 17(9) | 28(23) |
| Zhu Hongyuan-2008 | China | IHC-SP | AJCC | 56(43) | 20(3) | - | 12(6) | 44(37) |
| Miao Beiping-2007 | China | IHC-SP | China 1992 | 60(54) | 30(2) | - | 22(17) | 38(37) |
| Gong Yongqian-2007 | China | IHC-SP | UICC | 97(83) | 20(4) | - | 28(18) | 69(65) |
| Cui Dewei-2008 | China | IHC-SP | - | 86(65) | 30(1) | - | 25(10) | 61(55) |
| Yuan Hong-2008 | China | IHC-SP | UICC | 45(31) | Median 44 | 17(7) | 28(24) | |
| Xie Zhenyu-2008 | China | IHC-SP | China 1992 | 52(33) | 20(4) | Median 45.8 | 19(8) | 33(25) |
| Zhang Tingyou-2009 | China | IHC-SABC | China 1992 | 20(14) | Mean 44.8 | 5(4) | 15(10) | |
| Xiong Danning—2009 | China | IHC-SP | - | 86(69) | - | Mean 43.3 | 32(24) | 54(45) |
| Liu Yangyun-2010 | China | IHC-SP | AJCC | 50(32) | 15(0) | - | 15(4) | 35(28) |
| Jing Qiancheng-2010 | China | IHC-SP | UICC | 33(27) | 12(3) | Mean 49.8 | 13(8) | 20(19) |
| Wu Jingbo-2011 | China | IHC | 45(35) | 20(2) | Mean 58.6 | 14(7) | 31(28) | |
| Wang Zhiyong-2011 | China | IHC-SP | - | 66(52) | 20(2) | - | 26(14) | 40(38) |
| Xi Shaoyan-2012 | China | IHC-SP | AJCC/UICC | 86(61) | - | Mean 45 | 7(5) | 79(56) |
| Li Jianping-2012 | China | RT-PCR | - | 32(22) | 11(3) | - | 17(9) | 15(13) |
| Bai Weiqi-2012 | China | IHC | UICC | 58(46) | 38(3) | Mean 47 | 18(8) | 40(38) |
| Zhang Daqun-2013 | China | IHC | - | 76(56) | 32(2) | Mean 57.9 | 21(10) | 55(46) |
| Zhu Honghai-2014 | China | IHC | - | 104(82) | - | Mean 48.7 | 20(11) | 84(71) |
| Dingbo Shi-2014 | China | IHC | - | 200(138) | - | - | 37(17) | 163(121) |
| Ali Fendri-2008 | Tunisia | Real Time-PCR | - | 44(40) | 10(2) | Media 40 | 2(0) | 42(40) |
| Overall | - | - | - | 1797(1346) | - | - | 532(300) | 1265(1046) |
Abbreviations: NLMN: non-lymph node metastasis; LMN: lymph node metastasis; IHC: immunohistochemistry; SP: streptavidin-peroxidase; SABC: streptavidin avidin-biotin-pcroxidase complex method; RT-PCR: real time polymerase chain reaction; AJCC: The American Joint Committee on Cancer; UICC: Union for International Cancer Control.
Table 2. Other clinical characteristics of included studies.
| First author -Year | Gender | Tumor size stage | Distance metastasis | TNM stage | Differential | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Male(+) | Female(+) | T1/T2(+) | T3/T4(+) | M0(+) | M1(+) | I/II(+) | III/IV(+) | High(+) | Low(+) | |
| Xu Xinhua-2006 | 65 | 21 | - | - | - | - | - | - | 11(5) | 75(58) |
| Jiang Daihua-2004 | 49(38) | 13(10) | - | - | - | - | - | - | - | - |
| Gu Shanzhi-2006 | 61 | 17 | 38(15) | 40(29) | 73(39) | 5(5) | - | - | - | - |
| Zhou Leyuan-2006 | 32(27) | 11(7) | - | - | - | - | 11(6) | 32(29) | - | - |
| Dou Yanling-2006 | 28 | 11 | - | - | 20 | 19 | 11(4) | 28(25) | - | - |
| Luo Weireng-2006 | - | - | - | - | - | - | - | - | - | - |
| Fu Yafeng-2007 | 36(33) | 17(13) | 52(45) | 1(1) | - | - | 39(32) | 14(14) | - | - |
| Zhou Fang-2007 | 31 | 14 | 29(19) | 16(13) | - | - | - | - | - | - |
| Zhu Hongyuan-2008 | - | - | - | - | - | - | 15(8) | 41(35) | - | - |
| Miao Beiping-2007 | - | - | - | - | - | - | 25(20) | 35(34) | 29(24) | 31(30) |
| Gong Yongqian-2007 | 71(61) | 26(22) | - | - | - | - | 44(33) | 53(50) | - | - |
| Cui Dewei-2008 | - | - | - | - | - | - | - | - | - | - |
| Yuan Hong-2008 | 35(24) | 10(7) | - | - | - | - | 18(9) | 27(22) | - | - |
| Xie Zhenyu-2008 | 41(26) | 11(7) | - | - | - | - | 17(7) | 35(26) | - | - |
| Zhang Tingyou-2009 | 15 | 5 | 10(7) | 10(7) | 18(6) | 2(2) | 6(4) | 14(12) | - | - |
| Xiong Danning—2009 | 64(53) | 22(16) | - | - | - | - | 38(33) | 48(46) | - | - |
| Liu Yangyun-2010 | 25(18) | 25(15) | 14(3) | 36(30) | - | - | - | - | - | - |
| Jing Qiancheng-2010 | 25(20) | 8(7) | 15(10) | 18(17) | - | - | - | - | 2(1) | 31(26) |
| Wu Jingbo-2011 | 32(25) | 13(10) | - | - | - | - | - | - | - | - |
| Wang Zhiyong-2011 | 51(40) | 15(12) | - | - | - | - | - | 19(12) | 47(40) | |
| Xi Shaoyan-2012 | 61(40) | 21(21) | 45(30) | 41(31) | - | - | 40(25) | 46(36) | - | - |
| Li Jianping-2012 | - | - | - | - | - | - | - | - | - | - |
| Bai Weiqi-2012 | 40(31) | 18(15) | - | - | - | - | 19(10) | 39(36) | - | - |
| Zhang Daqun-2013 | 53 | 23 | 31(24) | 45(32) | - | - | - | - | - | - |
| Zhu Honghai-2014 | 85(67) | 19(15) | - | - | - | - | - | - | - | - |
| Dingbo Shi-2014 | 145(101) | 55(37) | 76(41) | 124(97) | 153(57) | 47(42) | 78(36) | 122(102) | - | - |
| Ali Fendri-2008 | 30 | 15 | - | - | - | 11 | - | - | - | - |
Table 3. Assessment of study quality according to Newcastle-Ottawa Scale (NOS).
| Studies | Items | NOS score | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5a | 5b | 6 | 7 | 8 | ||
| Xu Xinhua-2006 | * | * | * | - | - | - | * | * | - | 5 |
| Jiang Daihua-2004 | * | * | * | - | - | - | * | * | - | 5 |
| Gu Shanzhi-2006 | * | * | * | * | - | - | * | * | - | 6 |
| Zhou Leyuan-2006 | * | * | * | - | - | - | * | * | - | 5 |
| Dou Yanling-2006 | * | * | * | - | - | - | * | * | - | 5 |
| Luo Weireng-2006 | * | * | * | - | - | - | * | * | - | 5 |
| Fu Yafeng-2007 | * | * | * | - | - | - | * | * | - | 5 |
| Zhou Fang-2007 | * | * | * | - | - | - | * | * | - | 5 |
| Zhu Hongyuan-2008 | * | * | * | * | - | - | * | * | - | 6 |
| Miao Beiping-2007 | * | * | * | - | - | - | * | * | - | 5 |
| Gong Yongqian-2007 | * | * | * | - | - | - | * | * | - | 5 |
| Cui Dewei-2008 | * | * | * | - | - | - | * | * | - | 5 |
| Yuan Hong-2008 | * | * | * | - | - | - | * | * | - | 5 |
| Xie Zhenyu-2008 | * | * | * | - | - | - | * | * | - | 5 |
| Zhang Tingyou-2009 | * | * | * | - | - | - | * | * | - | 5 |
| Xiong Danning—2009 | * | * | * | - | - | - | * | * | - | 5 |
| Liu Yangyun-2010 | * | * | * | - | - | - | * | * | - | 5 |
| Jing Qiancheng-2010 | * | * | * | - | - | - | * | * | - | 5 |
| Wu Jingbo-2011 | * | * | * | - | - | - | * | * | - | 5 |
| Wang Zhiyong-2011 | * | * | * | - | - | - | * | * | - | 5 |
| Xi Shaoyan-2012 | * | * | * | - | - | - | * | * | - | 5 |
| Li Jianping-2012 | * | * | * | - | - | - | * | * | - | 5 |
| Bai Weiqi-2012 | * | * | * | - | - | - | * | * | - | 5 |
| Zhang Daqun-2013 | * | * | * | - | - | - | * | * | - | 5 |
| Zhu Honghai-2014 | * | * | * | * | - | - | * | * | - | 6 |
| Dingbo Shi-2014 | * | * | * | - | - | - | * | * | - | 5 |
| Ali Fendri-2008 | * | - | * | * | - | - | * | * | - | 5 |
Annotations: 1 adequacy of the case definition; 2 representativeness of the cases; 3 selection of controls; 4 definition of controls. 5a multiple ratings for this item for different categories of exposure; 5b other controlled factors; 6 ascertainment of exposure; 7 same method of ascertainment for cases and controls; 8 non-response rate.
Quantitative synthesis
COX-2 expression in NPC and non-NPC tissues
Data from 18 studies were included in meta-analysis comparing COX-2 expression in NPC and non-NPC tissues (Fig 2). No significant between-study heterogeneity was detected across these studies and therefore a fixed-effects model was used to calculate a combined OR. Overall, there was a significant association between COX-2 expression and NPC (OR = 21.17, 95%CI = 15.02–29.85, Pheterogeneity = 0.07).
Fig 2. Forest plot: odds ratio (OR) for COX-2 expression in NPC and normal tissue.

COX-2 expression and lymph node metastasis in NPC
All 27 studies were included in a meta-analysis that determined a statistically significant association between COX-2 expression and lymph node metastasis in NPC (OR = 4.44, 95%CI = 3.46–5.70) (Fig 3). Considered individually, of 24 studies with ORs >1, 19 reported 95%CIs not including 1, indicating a positive correlation between lymph node metastasis of NPC and COX-2 expression; only 3 studies reached ORs <1. As the heterogeneity test showed no significant heterogeneity among studies (I2 = 38.3%, Phetrogeneity = 0.024), a fixed-effects model was used. Subgroup analysis by assay and staging criteria also provided evidence for an association between COX-2 and lymph node metastasis in NPC patients (ORIHC-SP = 6.29, 95%CI = 4.55–8.67; ORIHC-SABC = 2.42, 95%CI = 1.45–4.02)(Table 4).
Fig 3. Forest plot:odds ratio (OR) for COX-2 expression and lymph node metastasis in NPC.

Table 4. Main results from subgroup analyses.
| Subtypes | No. | OR | 95% CI | Z (p) | Pheterogeneity |
|---|---|---|---|---|---|
| Assay | |||||
| IHC-SP | 17 | 6.29 | 4.55,8.67 | 11.19(0.000) | 0.561 |
| IHC-SABC | 5 | 2.42 | 1.45,4.02 | 3.40(0.001) | 0.006 |
| IHC-unclear | 3 | 1.80 | 0.81,4.01 | 1.44(0.150) | 0.947 |
| RT-PCR | 1 | 5.78 | 0.99,33.83 | 1.95(0.052) | - |
|
RT-PCR& IHC-SABC |
1 | 81.00 | 3.01,2183.15 | 2.61(0.009) | - |
| Staging criteria | |||||
| China 1992 | 7 | 3.98 | 2.30,6.86 | 4.96(0.000) | 0.421 |
| AJCC/UICC | 7 | 7.26 | 4.22,12.48 | 7.17(0.000) | 0.24 |
| Unknown | 13 | 3.88 | 2.80,5,39 | 8.12(0.000) | 0.014 |
| Country | |||||
| China | 26 | 4.37 | 3.40,5.61 | 11.55(0.000) | 0.035 |
| Tunisia | 1 | 81.00 | 3.01,2183.15 | 2.61(0.000) | - |
| Overall | 27 | 4.44 | 3.46,5.70 | 11.74(0.000) | 0.024 |
Abbreviations: IHC: immunohistochemistry; SP: streptavidin-peroxidase; SABC: streptavidin avidin-biotin-pcroxidase complex method; RT-PCR: real time polymerase chain reaction; AJCC: The American Joint Committee on Cancer; UICC: Union for International Cancer Control.
COX-2 expression and other clinicopathological parameters
Additional analyses explored potential associations of COX-2 expression with other potentially relevant factors, such as sex, tumor size stage (T3/T4 vs T1/T2), metastasis stage (M1 vs M0), clinical stage (III/IV vs I/II), and histological differentiation stage (no or low vs medium or high) (Fig 4). No statistically significant association was observed between COX-2 expression and sex (OR 1.09, 95%CI = 0.79–1.49). However, there were statistically significant positive associations of Cox 2 expression with more advanced clinical stages (III/IV) compared to early localized stages (I/II) (OR 5.39, 95%CI = 3.79–7.66), with the presence of more advanced metastases (OR 5.15, 95%CI 2.11–12.54), with larger tumor size (T3/T4) compared to smaller (T1/T2) (OR 2.53, 95%CI 1.77–3.63) and with no/low histological differentiation compared to medium/high (OR 4.12, 95%CI = 1.86–9.13).
Fig 4. Forest plots: odds ratio (OR) for other clinicopathological parameters.

(a) sex (male vs female); (b) metastasis (M1 vs M0); (c) tumor size (T1/T2 vs T3/T4); (d) TNM stage (I/II vs III/IV); (e) differentiation (low vs high)
Sensitivity analysis
The influence of individual studies on pooled results were assessed by conducting sensitivity analysis in which each individual study was omitted in turn and pooled ORs were recomputed and compared with the overall OR. The recalculated ORs did not differ significantly from the overall value, indicating that the overall results were stable (Fig 5).
Fig 5. Sensitivity analysis to test the influences of individual studies on overall effects.

Publication bias
Publication bias was evaluated using funnel plots and Begg’s (P = 0.404) and Egger’s (P = 0.658) tests, and none of them suggested significant bias was present, considering the absence of obvious asymmetry in plot shape and values of p = 0.404 and 0.658, respectively, for the statistical tests (Fig 6).
Fig 6. Funnel Plots of publication bias summary for corresponding Meta-analysis (left) and Egger's publication bias plot with pseudo 95%CI (right).

Discussion
This systematic review and meta-analysis found that COX-2 expression was positively associated with NPC lymph node metastasis and with other indicators of disease progression.
Review findings in the context of existing literature
Recent meta-analyses have synthesized evidence on the association between COX-2 expression and various types of cancers[41–44]. While some studies have reported an association between COX-2 levels and lymph node metastasis in NPC, others have found none, and COX-2’s diagnostic and prognostic values in NPC and the role of COX-2 inhibitors in treatment remain uncertain. This new systematic review and meta-analysis demonstrated a clear association of COX-2 expression with NPC-related lymph node metastasis and with other clinicopathological parameters.
The role of COX-2 in oncogenesis has been extensively explored in vitro tests using different tumor cell lines as well as in vivo experiments[45, 46]. Some researchers have suggested that COX-2 is induced by LMP-1 and contributes to the cancer process via the co-expression with VEGF, EGFR or other biomarkers which could enhance several cell survival and proliferation signal pathways[15, 47]. Others suggest that COX-2 expression could promote angiogenesis in NPC [48–50]. Several studies have shown that the anticancer effects of COX-2 inhibitors on NPC cells result from blocking cell cycle and inducing cell apoptosis, which may be partly mediated through the STAT3 pathway or through the inhibition of AKT phosphorylation[51, 52].
Although the precise mechanism by which COX-2 influences cancer development and progression in NPC remains unclear, this study highlights COX-2 expression’s potential as an indicator of cancer progression that can contribute to assessment of prognosis and treatment decisions and the therapeutic potential of COX-2 inhibitors in treatment of NPC.
In pooling and analyzing the data, considerable attention was paid to the methods, characteristics and results of each study individually in order to fully explore possible sources of heterogeneity or other factors that may affect overall results. Detection methods were examined and subgroup analyses conducted to evaluate possible heterogeneity arising from variations in technique and standards for identifying COX-2 positivity. Despite poor standardization of assay methods, no significant heterogeneity was detected resulting from detection methods other than in the 5-study IHC-SABC group. Subgroup analysis found no significant heterogeneity arising from use of either AJCC/UICC or Chinese TNM classification. Between study heterogeneity was not found to be significant in sensitivity analyses in which one study was removed at a time and recalculated ORs compared with the overall ORs.
Implications for clinical practice
In recent decades, advances have been made in the control of severe local invasion associated with NPC treated with chemoradiotherapy (CRT), sometimes combined with targeted drug therapies, and significantly improvements have been achieved in clinical outcomes for NPC patients[53–58]. However, early lymph node metastasis is still common even in newly diagnosed NPC cases. These metastases reduce the potential of treatments to prevent secondary diseases and disease recurrences, and are the major cause of the low survival rate associated with the disease.
Research has shown that COX-2 plays an important role in the carcinogenesis of head and neck cancers (HNC), and in the progression of cancers through modulating cell proliferation and apoptosis in ways that favor tumor growth and metastasis, thus affecting the efficacy of therapies. Therefore, COX-2 inhibitors may have considerable potential as therapeutic agents.
Implications for research
Further clinical research is warranted to develop and investigate ways in which COX-2 expression may be used clinically for assessment of disease progression, consideration of prognosis and treatment decisions in NPC. In addition, research is needed to formally explore and assess the therapeutic potential of COX-2 inhibitors in the disease. The data on which this review is based were obtained from studies with retrospective design; well-designed prospective clinical research and randomized controlled trials are needed to verify our findings.
In order to inform clinical developments that may benefit patients, more work is required to better understand the underlying mechanism of the occurrence and development of NPC-related lymph node metastasis, which remains poorly understood. The identification of molecular biomarkers associated with metastasis and recurrence in NPC is important in prognosis prediction, treatment decision-making and the development of therapies for NPC. In recent years, a great deal of research has focused on molecular biomarkers for cancers, including NPC. To date, researchers have investigated the associations of many biomarkers with the occurrence, progression and metastasis of NPC, including EBV-LMP1[59–61], EGFR[51, 62, 63], COX-2[41, 64–68], VEGF[69–73], etc [74–81].
The development of standardized assays for the detection of biomarkers is vital. RT-PCR is the most standardized technique in the detection of COX-2 expression. IHC is commonly used in most studies, as it is affordable and convenient to operate on formation-fixed tissues in retrospective studies. But this manual testing also has its own limitations, including the use of varied primary antibodies with different dilutions, IHC staining protocols with no definitions for the exact pH and compounds of the solutions or heating methods, and diverse and sometimes arbitrary cut-off values, limited samples and other human factors.
Study limitations
The present study has some limitations that should be noted. Although the quality of included studies as assessed using the NOS were generally adequate individually, few quality scores were high, which lowers the overall reliability of the review’s findings. Some potentially relevant studies, for example, were excluded because they reported insufficient data to extract OR values. In the included studies about the correlation of COX-2 expression with lymph node metastasis, most ORs were determined only by univariate analysis, which might influence the results. Non-Chinese patients accounted for only 2.45% (44/1797) of the total cases, which may be considered to reduce the generalizability of the results. The very high proportion of Chinese studies may reflect higher levels of research activity relating to the clinical area, resulting from the fact that NPC is one of the most common head and neck cancers in Southeast Asia, especially in Southern China. During the conduct of the review, given the overwhelmingly Chinese evidence-base, a second broad search was conducted to assess whether non-Chinese studies had been missed, but none was identified.
Conclusions
The review has strengthened the evidence for the association between COX-2 expression and lymph node metastasis in nasopharyngeal carcinoma patients, and with other indicators of disease progression. This suggests not only that COX-2 may be involved in the occurrence and development of lymph node metastasis and in disease progression, but also that it may have potential in assessing prognosis and in treatment decisions. In addition, it highlights the potential of COX-2 inhibitors in treatment of NPC. Well-designed prospective studies are needed to develop and investigate methods for using COX-2 expression for more accurate assessment of disease progression, and to assess the therapeutic potential of COX-2 inhibitors as treatment for the disease.
Supporting information
(PDF)
Acknowledgments
The authors are grateful to the Center of genetic diagnosis in Zhongnan Hospital of Wuhan University and to Dr Brian Buckley (Visiting Professor at Zhongnan Hospital of Wuhan University) for assistance in preparing the English language Manuscript.
Data Availability
All relevant data are within the paper and its Supporting Information file.
Funding Statement
This study was supported by National Natural Science Funds (no. 81472033 and no. 30901308), www.nsfc.gov.cn; The National Science Foundation of Hubei Province (no. 2013CFB233 and no. 2013CFB235), www.hbstd.gov.cn; The Scientific and technological project of Wuhan City (no. 2014060101010045), www.whst.gov.cn; Hubei Province health and family planning scientific research project (WJ2015Q021), www.hbwsjs.gov.cn; and Training Program of the science and technology innovation from Zhongnan Hospital of Wuhan University (ZNPY2016054), www.znhospital.cn/kxyjsy/index.jhtml. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1.Galletti B, Santoro R, Mannella VK, Caminiti F, Bonanno L, De Salvo S, et al. Olfactory event-related potentials: a new approach for the evaluation of olfaction in nasopharyngeal carcinoma patients treated with chemo-radiotherapy. The Journal of laryngology and otology. 2016;130(5):453–61. Epub 2016/03/05. 10.1017/S0022215116000761 [DOI] [PubMed] [Google Scholar]
- 2.Zhu DD, Zhang J, Deng W, Yip YL, Lung HL, Tsang CM, et al. Significance of NF-kappaB activation in immortalization of nasopharyngeal epithelial cells. International journal of cancer. 2016;138(5):1175–85. Epub 2015/09/16. 10.1002/ijc.29850 [DOI] [PubMed] [Google Scholar]
- 3.Ma L, Li S, Lu Y, Zhang X, Zhao J, Qin X. A pooled analysis of the IL-10-1082 A/G polymorphism and the nasopharyngeal carcinoma susceptibility. European archives of oto-rhino-laryngology: official journal of the European Federation of Oto-Rhino-Laryngological Societies. 2016;273(4):819–25. Epub 2014/12/31. [DOI] [PubMed] [Google Scholar]
- 4.Banko AV, Lazarevic IB, Folic MM, Djukic VB, Cirkovic AM, Karalic DZ, et al. Characterization of the Variability of Epstein-Barr Virus Genes in Nasopharyngeal Biopsies: Potential Predictors for Carcinoma Progression. PloS one. 2016;11(4):e0153498 Epub 2016/04/14. PubMed Central PMCID: PMCPMC4829223. 10.1371/journal.pone.0153498 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Tang LQ, Li CF, Li J, Chen WH, Chen QY, Yuan LX, et al. Establishment and Validation of Prognostic Nomograms for Endemic Nasopharyngeal Carcinoma. Journal of the National Cancer Institute. 2016;108(1). Epub 2015/10/16. [DOI] [PubMed] [Google Scholar]
- 6.Zhou H, Shen G, Zhang W, Cai H, Zhou Y, Li L. 18F-FDG PET/CT for the Diagnosis of Residual or Recurrent Nasopharyngeal Carcinoma After Radiotherapy: A Metaanalysis. Journal of nuclear medicine: official publication, Society of Nuclear Medicine. 2016;57(3):342–7. Epub 2015/11/07. [DOI] [PubMed] [Google Scholar]
- 7.Lim SJ, Iyer NG, Ooi LL, Koong HN, Chung AY, Tan HK, et al. Metastasectomy for metachronous pulmonary and hepatic metastases from nasopharyngeal carcinoma: Report of 6 cases and review of the literature. Head & neck. 2016;38(2):E37–40. Epub 2015/05/02. [DOI] [PubMed] [Google Scholar]
- 8.Yi C, Wang Y, Zhang C, Xuan Y, Zhao S, Liu T, et al. Cleavage and polyadenylation specific factor 4 targets NF-kappaB/cyclooxygenase-2 signaling to promote lung cancer growth and progression. Cancer letters. 2016;381(1):1–13. 10.1016/j.canlet.2016.07.016 [DOI] [PubMed] [Google Scholar]
- 9.Bernard MP, Bancos S, Sime PJ, Phipps RP. Targeting cyclooxygenase-2 in hematological malignancies: rationale and promise. Current pharmaceutical design. 2008;14(21):2051–60. Epub 2008/08/12. PubMed Central PMCID: PMCPMC2745246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yang B, Jia L, Guo Q, Ren H, Hu Y, Xie T. Clinicopathological and prognostic significance of cyclooxygenase-2 expression in head and neck cancer: A meta-analysis. Oncotarget. 2016;7(30):47265–77. 10.18632/oncotarget.10059 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Zhou YY, Hu ZG, Zeng FJ, Han J. Clinical Profile of Cyclooxygenase-2 Inhibitors in Treating Non-Small Cell Lung Cancer: A Meta-Analysis of Nine Randomized Clinical Trials. PloS one. 2016;11(3):e0151939 PubMed Central PMCID: PMCPMC4805232. 10.1371/journal.pone.0151939 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Moher D, Liberati A, Tetzlaff J, Altman DG, The PG. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS medicine. 2009;6(7):e1000097 10.1371/journal.pmed.1000097 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Zeng X, Zhang Y, Kwong JS, Zhang C, Li S, Sun F, et al. The methodological quality assessment tools for preclinical and clinical studies, systematic review and meta-analysis, and clinical practice guideline: a systematic review. Journal of evidence-based medicine. 2015;8(1):2–10. Epub 2015/01/17. 10.1111/jebm.12141 [DOI] [PubMed] [Google Scholar]
- 14.Shi D, Xiao X, Tian Y, Qin L, Xie F, Sun R, et al. Activating enhancer-binding protein-2alpha induces cyclooxygenase-2 expression and promotes nasopharyngeal carcinoma growth. Oncotarget. 2015;6(7):5005–21. Epub 2015/02/12. PubMed Central PMCID: PMCPMC4467130. 10.18632/oncotarget.3215 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Fendri A, Khabir A, Hadhri-Guiga B, Sellami-Boudawara T, Ghorbel A, Daoud J, et al. Overexpression of COX-2 and LMP1 are correlated with lymph node in Tunisian NPC patients. Oral oncology. 2008;44(7):710–5. Epub 2007/12/07. 10.1016/j.oraloncology.2007.09.006 [DOI] [PubMed] [Google Scholar]
- 16.Daihua J, Deyu G, Yousheng L, Limei L. Relationship Between High Expression of CycIooxygenase -2 and VEGF and lymph node metastasis in Nasopharyngeal Carcinoma. China New Medicine. 2004;3(6):16–8. [Google Scholar]
- 17.Leyuan Z, Juying Z, Yuyu W. Relation Between Expression of COX-2 and Survivin in NPC and Their Clinical Signigicance. Suzhou University Journal of Medical Science. 2006;(01):95–7. [Google Scholar]
- 18.Shanzhi G. The Magnetic Resonance Imaging of Nasopharyngeal Carcinoma and Its Correlation with the Expression of CDl05 and Cyclooxygenase-2 in Nasopharyngeal Carcinoma and the Microvesseldensity Stained by CDl05 and CD34. [Master]: Central South University; 2006.
- 19.Xinhua X, Guoqing H, Song L, Feng X, Daojun L, Delan D, et al. Expression of Cyclooxygenase-2 in Nasopharyngeal Carcinoma and Its Relation to Angiogenesis and Prognosis . The Chinese-German Journal of Clinical Oncology. 2006;(02):104–7+49. [Google Scholar]
- 20.Yanling D, Huaizhi F, Chuanyu L. Expression of Cyclooxygenase-2 in Nasopharyngeal Carcinoma and their Significance. Medical Journal of National Defending Force in Southwest China. 2006;(02):124–6. [Google Scholar]
- 21.Beiping M. Prognostic Significance of COX-2, PCNA and p53 in Nasopharyngeal Carcinoma. Journal Otolaryngol Ophthal Shandong University. 2007;21(3). [Google Scholar]
- 22.Fang Z, Zhengxian L, Gengxun L. Expression of Cyclooxygenase-2 in Nasopharyngeal Carcinoma. Chinese Journal of Otorhinolaryngology. 2007;(01):25–7. [Google Scholar]
- 23.Weiren L, Xianyi C, ZhaoTongwei . Expression of COX2 and CD44V6 in Nasopharyngeal Carcinoma and their Relationshiop. Guangdong Medical Journal. 2007;28(8):1213–5. [Google Scholar]
- 24.Yafeng F. Expression of COX2, CD44V33 in Nasopharyngeal Carcinoma and the significance in Cancer Invasion and Metastasis [Master]: Guangdong Medical College; 2007.
- 25.Yongqian G. Research on Expression of elF4E, COX-2 in Nasopharyngeal Carcinoma Tissue and their Clinic Significance [Master]: central South University; 2007.
- 26.Dewei C. Expressions of COX-2 and MMP-2 in Nasopharyngeal Carcinoma and Their Relationship with Lymph Node Metastasis. Journal of Clinical Otorhinolaryngol Head Neck Surgury (China). 2008;22(15). [PubMed] [Google Scholar]
- 27.Hong Y, Haiming W, Jianping L, Jinlong L, Tao W. Expression and Correlation of COX-2 and VEGF-C in Nasopharyngeal Carcinoma. Journal of Clinical Otorhinolaryngol Head Neck Surgury (China). 2008;(01):33–6. [Google Scholar]
- 28.Hongyuan Z. Expressive activities of COX-2 and VEGF and their association with cervical Nodes metastases of poorly diffirentiate squamous cell carcinoma in the nasopharynx. Chinese Journal of Otorhinolaryngology of Integrated Traditional and Western Medicine. 2008;16(2). [Google Scholar]
- 29.Zhenyu X. Expression and Clinical Significance of VEGF-C, COX-2 and VEGFR-3 in Nasopharyngeal Carcinoma [Master]: Fujian Medical University; 2008.
- 30.Danning X. Expression of COX-2 and p73 Proteins in Nasopharyngeal Carcinoma and their Clinical Significance. Journal of Hubei Medical University. 2009;28(4). [Google Scholar]
- 31.Tingyou Z. Clinical Significance of Combined Examination of Three Types Tumor Markers in Nasopharyngeal Carcinoma Tissues [Master]: Zunyi Medical University; 2009.
- 32.Qiancheng J. Expression and Clinic Significance of COX-2 Protein in Nasopharyngeal Carcinoma [硕士]: University of South China; 2010.
- 33.Yangyun L, gengxun L, Lizhengxian, Zhengliang S, Guanghua Z, Wen J. Expression and Clinical Significance of Pcatenin, iNOS and Cyclooxygenase-2 in Nasopharyngeal Carcinoma Tissue. Chinese clinical oncology. 2010;15(4):310–4. [Google Scholar]
- 34.Jinbo W, Shihua C, Zhenjie X, Qingwen Z, Ying W. Expression and Significance of Cyclooxygenase-2 and Inducible Nitric Oxide Synthase in Nasopharyngeal Carcinoma. Jilin Medical Journal. 2011;(33):6983–4. [Google Scholar]
- 35.Zhiyong W, Yulin X, Lian D, Gang L, Shaowei L, Yong F, et al. Expresions of COX-2 and VEGF-C in nasopharyngeal Carcinoma and their Relationship with Lymph Angiogenesis and Lymph Metastasis. Laboratory Medicine and Clinic. 2011;(05):518–20+23. [Google Scholar]
- 36.Jianping L, Xiaoqing Z, Xiong L, Keqiang Z, Ming X. Expression of COX-2 and VEGF-C in Nasopharyngeal Carcinoma. Journal of Hunan Normal University (Med Sci). 2012;(03):25–7+38. [Google Scholar]
- 37.Shaoyan X, Qiuliang W, Yongsheng Z, Jianzhong L, Juanjuan Y, Jinghui H, et al. Clinical Value of COX-2, EFGR and Ki-67 expression in Nasopharyngeal Carcinoma. Guangdong Medical Journal. 2012;(10):1422–5. [Google Scholar]
- 38.Weiqi B, Baohua H, Jianguo T, Xuan L, Rong H, Jixia Y, et al. COX-2 and EGFR Expression in Nasopharyngeal Carcinoma and their Relationship. Zhejiang Practical Mdeicine. 2012;(03):162–4+237. [Google Scholar]
- 39.Daqun Z, Naizun Z. COX-2 and LMP-1 Espression and the value in Nasopharyngeal Carcinoma. Journal of Guzhou Medical College. 2013;31(4):389–90. [Google Scholar]
- 40.Honghai Z, Xiaoyuan Z. RelationshipBetween Cyclooxygenase-2 in Nasopharyngeal Carcinoma and Cervical Lymph Node Metastasis. National Medical Journal of China. 2014;94(18):1409–12. [PubMed] [Google Scholar]
- 41.Leng WD, Wen XJ, Kwong JS, Huang W, Chen JG, Zeng XT. COX-2 rs689466, rs5275, and rs20417 polymorphisms and risk of head and neck squamous cell carcinoma: a meta-analysis of adjusted and unadjusted data. BMC cancer. 2016;16:457 Epub 2016/07/15. PubMed Central PMCID: PMCPMC4942952. 10.1186/s12885-016-2535-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Wan GX, Chen P, Yu XJ, Di QS, Yu YD, Lei JH, et al. Cyclooxygenase-2 polymorphisms and bladder cancer risk: a meta-analysis based on case-control studies. International journal of clinical and experimental medicine. 2015;8(3):3935–45. Epub 2015/06/13. PubMed Central PMCID: PMCPMC4443129. [PMC free article] [PubMed] [Google Scholar]
- 43.Shimizu K, Yukawa T, Okita R, Saisho S, Maeda A, Nojima Y, et al. Cyclooxygenase-2 expression is a prognostic biomarker for non-small cell lung cancer patients treated with adjuvant platinum-based chemotherapy. World journal of surgical oncology. 2015;13:21 Epub 2015/04/19. PubMed Central PMCID: PMCPMC4332968. 10.1186/s12957-014-0426-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Lu SC, Zhong JH, Tan JT, Tang HL, Liu XG, Xiang BD, et al. Association between COX-2 gene polymorphisms and risk of hepatocellular carcinoma development: a meta-analysis. BMJ open. 2015;5(10):e008263 Epub 2015/10/07. PubMed Central PMCID: PMCPMC4606424. 10.1136/bmjopen-2015-008263 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Shao Y, Li P, Zhu ST, Yue JP, Ji XJ, Ma D, et al. MiR-26a and miR-144 inhibit proliferation and metastasis of esophageal squamous cell cancer by inhibiting cyclooxygenase-2. Oncotarget. 2016;7(12):15173–86. PubMed Central PMCID: PMCPMC4924778. 10.18632/oncotarget.7908 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Mitsunari K, Miyata Y, Asai A, Matsuo T, Shida Y, Hakariya T, et al. Human antigen R is positively associated with malignant aggressiveness via upregulation of cell proliferation, migration, and vascular endothelial growth factors and cyclooxygenase-2 in prostate cancer. Transl Res. 2016;175:116–28. 10.1016/j.trsl.2016.04.002 [DOI] [PubMed] [Google Scholar]
- 47.Yi X, Tang A, Qin Y, Wen W, Zhao W. [Expression and relationship of EBV LMP1, COX-2 and VEGF-C in nasopharyngeal carcinoma]. Lin chuang er bi yan hou tou jing wai ke za zhi = Journal of clinical otorhinolaryngology, head, and neck surgery. 2010;24(3):126–8. Epub 2010/05/01. [PubMed] [Google Scholar]
- 48.Liu N, Zhou N, Chai N, Liu X, Jiang H, Wu Q, et al. Helicobacter pylori promotes angiogenesis depending on Wnt/beta-catenin-mediated vascular endothelial growth factor via the cyclooxygenase-2 pathway in gastric cancer. BMC cancer. 2016;16:321 Epub 2016/05/21. PubMed Central PMCID: PMCPMC4873996. 10.1186/s12885-016-2351-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Gregorio H, Raposo TP, Queiroga FL, Prada J, Pires I. Investigating associations of cyclooxygenase-2 expression with angiogenesis, proliferation, macrophage and T-lymphocyte infiltration in canine melanocytic tumours. Melanoma research. 2016;26(4):338–47. Epub 2016/04/23. 10.1097/CMR.0000000000000262 [DOI] [PubMed] [Google Scholar]
- 50.Hsu SJ, Lin TY, Wang SS, Chuang CL, Lee FY, Huang HC, et al. Endothelin receptor blockers reduce shunting and angiogenesis in cirrhotic rats. European journal of clinical investigation. 2016;46(6):572–80. Epub 2016/04/20. 10.1111/eci.12636 [DOI] [PubMed] [Google Scholar]
- 51.Ooft ML, Braunius WW, Heus P, Stegeman I, van Diest PJ, Grolman W, et al. Prognostic significance of the EGFR pathway in nasopharyngeal carcinoma: a systematic review and meta-analysis. Biomarkers in medicine. 2015;9(10):997–1010. Epub 2015/10/07. 10.2217/bmm.15.68 [DOI] [PubMed] [Google Scholar]
- 52.Liu DB, Hu GY, Long GX, Qiu H, Mei Q, Hu GQ. Celecoxib induces apoptosis and cell-cycle arrest in nasopharyngeal carcinoma cell lines via inhibition of STAT3 phosphorylation. Acta Pharmacol Sin. 2012;33(5):682–90. PubMed Central PMCID: PMCPMC4010355. 10.1038/aps.2012.18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Chen Y, Sun Y, Liang SB, Zong JF, Li WF, Chen M, et al. Progress report of a randomized trial comparing long-term survival and late toxicity of concurrent chemoradiotherapy with adjuvant chemotherapy versus radiotherapy alone in patients with stage III to IVB nasopharyngeal carcinoma from endemic regions of China. Cancer. 2013;119(12):2230–8. Epub 2013/04/12. 10.1002/cncr.28049 [DOI] [PubMed] [Google Scholar]
- 54.Chen J, Liu P, Wang Q, Wu L, Zhang X. Influence of Intensity-Modulated Radiation Therapy on the Life Quality of Patients with Nasopharyngeal Carcinoma. Cell biochemistry and biophysics. 2015;73(3):731–6. Epub 2016/06/05. 10.1007/s12013-015-0638-0 [DOI] [PubMed] [Google Scholar]
- 55.Zhang MX, Li J, Shen GP, Zou X, Xu JJ, Jiang R, et al. Intensity-modulated radiotherapy prolongs the survival of patients with nasopharyngeal carcinoma compared with conventional two-dimensional radiotherapy: A 10-year experience with a large cohort and long follow-up. European journal of cancer (Oxford, England: 1990). 2015;51(17):2587–95. Epub 2015/09/01. [DOI] [PubMed] [Google Scholar]
- 56.Wu X, Huang J, Liu L, Li H, Li P, Zhang J, et al. Cetuximab concurrent with IMRT versus cisplatin concurrent with IMRT in locally advanced nasopharyngeal carcinoma: A retrospective matched case-control study. Medicine. 2016;95(39):e4926 Epub 2016/09/30. 10.1097/MD.0000000000004926 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Jiang H, Wang G, Song H, Xu H, Zhang Y, Zhou Y, et al. Analysis of the efficacy of intensity-modulated radiotherapy and two-dimensional conventional radiotherapy in nasopharyngeal carcinoma with involvement of the cervical spine. Oncology letters. 2015;10(5):2731–8. Epub 2016/01/02. PubMed Central PMCID: PMCPMC4665756. 10.3892/ol.2015.3668 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Xu T, Liu Y, Dou S, Li F, Guan X, Zhu G. Weekly cetuximab concurrent with IMRT aggravated radiation-induced oral mucositis in locally advanced nasopharyngeal carcinoma: Results of a randomized phase II study. Oral oncology. 2015;51(9):875–9. Epub 2015/07/15. 10.1016/j.oraloncology.2015.06.008 [DOI] [PubMed] [Google Scholar]
- 59.Chen X, Shi J, Zhong J, Huang Z, Luo X, Huang Y, et al. miR-1, regulated by LMP1, suppresses tumour growth and metastasis by targeting K-ras in nasopharyngeal carcinoma. International journal of experimental pathology. 2015;96(6):427–32. Epub 2016/02/09. PubMed Central PMCID: PMCPMC4744829. 10.1111/iep.12162 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Murata T, Noda C, Narita Y, Watanabe T, Yoshida M, Ashio K, et al. Induction of Epstein-Barr Virus Oncoprotein LMP1 by Transcription Factors AP-2 and Early B Cell Factor. J Virol. 2016;90(8):3873–89. Epub 2016/01/29. 10.1128/JVI.03227-15 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Zhao Y, Wang Y, Zeng S, Hu X. LMP1 expression is positively associated with metastasis of nasopharyngeal carcinoma: evidence from a meta-analysis. J Clin Pathol. 2012;65(1):41–5. Epub 2011/11/01. 10.1136/jclinpath-2011-200198 [DOI] [PubMed] [Google Scholar]
- 62.Brand TM, Iida M, Luthar N, Starr MM, Huppert EJ, Wheeler DL. Nuclear EGFR as a molecular target in cancer. Radiotherapy and Oncology. 2013;108(3):370–7. 10.1016/j.radonc.2013.06.010 [DOI] [PMC free article] [PubMed] [Google Scholar] [Research Misconduct Found]
- 63.Yuan C, Xu XH, Chen Z. Combination treatment with antiEGFR monoclonal antibodies in advanced nasopharyngeal carcinoma: a meta-analysis. Journal of BUON: official journal of the Balkan Union of Oncology. 2015;20(6):1510–7. Epub 2016/02/09. [PubMed] [Google Scholar]
- 64.Wang XF, Huang MZ, Zhang XW, Hua RX, Guo WJ. COX-2-765G>C polymorphism increases the risk of cancer: a meta-analysis. PloS one. 2013;8(9):e73213 Epub 2013/09/12. PubMed Central PMCID: PMCPMC3762903. 10.1371/journal.pone.0073213 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Zhuang M, Zhao M, Qiu H, Shi D, Wang J, Tian Y, et al. Effusanin E suppresses nasopharyngeal carcinoma cell growth by inhibiting NF-kappaB and COX-2 signaling. PloS one. 2014;9(10):e109951 PubMed Central PMCID: PMCPMC4204824. 10.1371/journal.pone.0109951 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Li ZL, Ye SB, OuYang LY, Zhang H, Chen YS, He J, et al. COX-2 promotes metastasis in nasopharyngeal carcinoma by mediating interactions between cancer cells and myeloid-derived suppressor cells. Oncoimmunology. 2015;4(11):e1044712 PubMed Central PMCID: PMCPMC4590030. 10.1080/2162402X.2015.1044712 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Su J, Wen S, Zhu J, Liu R, Yang J. Meta-analysis of cyclooxygenase-2 (COX-2) 765G>C polymorphism and Alzheimer's disease. Journal of clinical neuroscience: official journal of the Neurosurgical Society of Australasia. 2016;31:4–9. Epub 2016/07/23. [DOI] [PubMed] [Google Scholar]
- 68.Tietz O, Wuest M, Marshall A, Glubrecht D, Hamann I, Wang M, et al. PET imaging of cyclooxygenase-2 (COX-2) in a pre-clinical colorectal cancer model. EJNMMI Res. 2016;6(1):37 PubMed Central PMCID: PMCPMC4844587. 10.1186/s13550-016-0192-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Wakisaka N, Hirota K, Kondo S, Sawada-Kitamura S, Endo K, Murono S, et al. Induction of lymphangiogenesis through vascular endothelial growth factor-C/vascular endothelial growth factor receptor 3 axis and its correlation with lymph node metastasis in nasopharyngeal carcinoma. Oral oncology. 2012;48(8):703–8. Epub 2012/03/01. 10.1016/j.oraloncology.2012.02.003 [DOI] [PubMed] [Google Scholar]
- 70.Zhang JX, Cai MB, Wang XP, Duan LP, Shao Q, Tong ZT, et al. Elevated DLL4 expression is correlated with VEGF and predicts poor prognosis of nasopharyngeal carcinoma. Medical oncology. 2013;30(1):390 Epub 2013/01/01. 10.1007/s12032-012-0390-x [DOI] [PubMed] [Google Scholar]
- 71.Zhang R, Zhao Y, Zhang S, Lv J. [The expressions of EphrinB2 and VEGF in nasopharyngeal carcinoma and their clinical significance]. Lin chuang er bi yan hou tou jing wai ke za zhi = Journal of clinical otorhinolaryngology, head, and neck surgery. 2013;27(4):178–80. Epub 2013/05/02. [PubMed] [Google Scholar]
- 72.Chen HH, Weng BQ, Cheng KJ, Liu HY, Wang SQ, Lu YY. Effect of the vascular endothelial growth factor expression level on angiopoietin-2-mediated nasopharyngeal carcinoma growth. Vascular cell. 2014;6(1):4 Epub 2014/03/04. PubMed Central PMCID: PMCPMC4015607. 10.1186/2045-824X-6-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Xie M, He G, Wang R, Shi S, Chen J, Ye Y, et al. Matrine-induced apoptosis of human nasopharyngeal carcinoma cells via in vitro vascular endothelial growth factor-A/extracellular signal-regulated kinase1/2 pathway inactivation. Hormone and metabolic research = Hormon- und Stoffwechselforschung = Hormones et metabolisme. 2014;46(8):556–60. Epub 2014/02/21. 10.1055/s-0034-1367077 [DOI] [PubMed] [Google Scholar]
- 74.Chan SC, Chang KP, Fang YD, Tsang NM, Ng SH, Hsu CL, et al. Tumor heterogeneity measured on F-18 fluorodeoxyglucose positron emission tomography/computed tomography combined with plasma Epstein-Barr Virus load predicts prognosis in patients with primary nasopharyngeal carcinoma. The Laryngoscope. 2016. Epub 2016/07/21. [DOI] [PubMed] [Google Scholar]
- 75.Wang J, Li L, Dong BQ, Xu YJ, Zheng YD, Sun ZW, et al. Post-treatment serum lactic dehydrogenase as a predictive indicator for distant metastasis and survival of patients with nasopharyngeal carcinoma. Oncotarget. 2016;7(19):27458–67. Epub 2016/04/07. PubMed Central PMCID: PMCPMC5053663. 10.18632/oncotarget.8480 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Li XH, Chang H, Xu BQ, Tao YL, Gao J, Chen C, et al. An inflammatory biomarker-based nomogram to predict prognosis of patients with nasopharyngeal carcinoma: an analysis of a prospective study. Cancer medicine. 2016. Epub 2016/11/20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Pan Y, Wang S, Su B, Zhou F, Zhang R, Xu T, et al. Stat3 contributes to cancer progression by regulating Jab1/Csn5 expression. Oncogene. 2016. Epub 2016/08/16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Li S, Xue M, Han L. [Relationship between Testin expression and clinicopathological characteristics in nasopharyngeal carcinoma patients]. Lin chuang er bi yan hou tou jing wai ke za zhi = Journal of clinical otorhinolaryngology, head, and neck surgery. 2016;30(4):310–3. Epub 2016/07/05. [PubMed] [Google Scholar]
- 79.He HL, Lee YE, Liang PI, Lee SW, Chen TJ, Chan TC, et al. Overexpression of JAK2: a predictor of unfavorable prognosis for nasopharyngeal carcinoma. Future oncology (London, England). 2016;12(16):1887–96. Epub 2016/04/19. [DOI] [PubMed] [Google Scholar]
- 80.Deng CC, Xu M, Li J, Luo XL, Zhu YJ, Jiang R, et al. Unconjugated Bilirubin Is a Novel Prognostic Biomarker for Nasopharyngeal Carcinoma and Inhibits Its Metastasis via Antioxidation Activity. Cancer Prev Res (Phila). 2016;9(2):180–8. Epub 2015/09/27. [DOI] [PubMed] [Google Scholar]
- 81.Xu XF, Lu RQ, Xiao R, Zhou L, Zhao XM, Hu XC, et al. Rta-IgG as a biomarker for diagnosis and post treatment prognostic of nasopharyngeal carcinoma. Cancer biomarkers: section A of Disease markers. 2016;16(3):467–76. Epub 2016/04/12. 10.3233/CBM-160586 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(PDF)
Data Availability Statement
All relevant data are within the paper and its Supporting Information file.