

Abstract
Objective
To compare intrauterine device (IUD) use at 6 months postpartum among women who underwent intracesarean delivery (during cesarean delivery) IUD placement versus women who planned for interval IUD placement 6 or more weeks postpartum.
Methods
In this non-blinded randomized trial women who were undergoing a cesarean and desired an IUD were randomized to intracesarean cesarean delivery or interval IUD placement. The primary outcome was IUD use at 6 months postpartum. A sample size of 112 (56 in each group) was planned to detect a 15% difference in IUD use at 6 months postpartum between groups.
Results
From March 2012 to June 2014, 172 women were screened and 112 women were randomized into the trial. Baseline characteristics were similar between groups. Data regarding IUD use at 6 months postpartum was available for 98 women, 48 and 50 women in the intracesarean and interval groups, respectively. A larger proportion of the women in the intracesarean group were using an IUD at 6 months postpartum ((40/48), 83%) compared to those in the interval group ((32/50) 64%, relative risk [RR]=1.3, 95% confidence interval [CI]: 1.02, 1.66). Among the 56 women randomized to interval IUD insertion, 22 (39%) of them never received an IUD; 14 (25%) never returned for IUD placement, five (9%) women declined an IUD, and three (5%) had a failed IUD placement.
Conclusion
IUD placement at the time of cesarean delivery leads to a higher proportion of IUD use at 6 months postpartum when compared to interval IUD placement.
Introduction
Delaying the initiation of effective contraception until the postpartum visit puts some women at risk for rapid, repeat, and unintended pregnancy1. More than 50% of non-breastfeeding women ovulate by 6 weeks postpartum2. Additionally, more than 50% of women are sexually active by 6 weeks postpartum2. Women who intend to use an intrauterine device (IUD) for postpartum contraception are often unable to return for a postpartum visit, and never receive anIUD.3 These women are more likely to be socially and financially disadvantaged4,5 and face barriers such as lack of transportation, lack of stable housing, and difficulty communicating with their healthcare providers.6
IUD placement in the immediate postpartum period has the potential to increase overall IUD use and decrease rates of unintended pregnancy in the US. Immediate postplacental IUD insertion (within ten minutes of placental delivery) is an alternative to interval insertion (insertion 6 or more weeks postpartum); however, little data are available regarding IUDs specifically placed at cesarean delivery.7,8 Existing data suggest that intracesarean delivery (during cesarean delivery) IUD placement may have a lower expulsion risk than placement at time of vaginal delivery.9-11 The purpose of this study was to compare IUD use at 6 months postpartum among women who underwent intracesarean delivery IUD placement versus women who planned for interval IUD placement 6 or more weeks after delivery.
Materials and Methods
This was a parallel, 1:1, non-blinded, randomized trial conducted between March 2012 and June 2014 at the North Carolina Women's Hospital. The study was approved by the University of North Carolina Institutional Review Board and was registered at ClinicalTrials.gov (NCT01539759). We recruited pregnant women aged 18-45 years who were undergoing a cesarean delivery and desired an IUD for contraception postpartum. All study activities adhered to the CONSORT guidelines for reporting clinical trials.12 Screening and recruitment took place during prenatal care or on Labor and Delivery. After providing written consent, women were randomized to intracesarean delivery IUD placement or interval IUD insertion at a visit 6 or more weeks after delivery. After randomization to the timing of IUD placement, women could choose either a LNG-IUS (Mirena) or a Copper IUD (ParaGard). Women were seen at 6 weeks, 3 and 6 months postpartum. IUDs were provided free of charge, and women were reimbursed a nominal amount for each study visit.
Both laboring and non-laboring women were eligible for enrollment into the trial. Inclusion criteria were:1) English or Spanish speaking; 2) intention to comply with follow up 3) delivery of a live-born infant greater than 24 weeks via cesarean delivery. Women were excluded if they had: 1) a positive test for gonorrhea or chlamydia in this pregnancy; 2) a uterine anomaly that was known to distort the uterine cavity; 3) known or suspected cervical, uterine or breast neoplasia; 4) an allergy to any component of the chosen IUD; 5) a diagnosis of chorioamnionitis, intrapartum fever, or ruptured membranes for greater than 24 hours prior to delivery.
All women were consented and enrolled into the trial on Labor and Delivery prior to entry into the operating room. After enrollment, each woman was randomly assigned to the timing of her IUD placement. The investigator opened the next sequentially numbered, opaque, sealed envelope containing the group assignment of intracesarean delivery or interval IUD placement. A research assistant, not otherwise involved with the conduct of this trail, prepared the envelopes using computer-generated random allocation in randomly permutated blocks of four and six. All women were told their allocation assignment prior to their cesarean delivery and were asked to select their desired IUD type.
Women allocated to the intracesarean group had their IUDs placed using the hysterotomy after the delivery of the infant and the placenta. IUDs were placed in a standardized fashion by residents and faculty who had received a ten-minute training by the principal investigators. The IUD was positioned with arms out in the applicator and inserted through the hysterotomy to the uterine fundus. A hand was placed on the exterior of the uterine fundus to stabilize the uterus and to hold the IUD in place. The applicator was then removed through the hysterotomy and the IUD strings were directed into the cervix using a ring forceps. For the LNG-IUS the IUD strings were trimmed at the level of the thread cleft prior to deployment. The Copper IUD strings were not cut. The hysterotomy was then closed in the standard fashion.
The 6-week study visit occurred at the same time as the woman's routine 6 week postpartum visit with her primary obstetrician or midwife. For women allocated to the interval placement group, the IUD was placed by the primary provider or a member of the study team, depending on the woman's preference. IUD strings were trimmed to 3-4 cm after IUD placement. At each study visit, women completed a questionnaire about their satisfaction with their IUD, pain, and bleeding. An examination was done to confirm IUD location. If no IUD strings could be seen protruding from the cervical oson speculum examination, an ultrasonogram was performed for IUD localization. Women were contacted after each missed study visit. We made at least 5 attempts to contact women by phone, email, and certified letter before they were considered lost to follow-up
The primary outcome was IUD use at 6 months postpartum. Secondary outcomes included IUD expulsion, IUD discontinuation, IUD strings visible at 6 months postpartum, and women's satisfaction with the IUD. An expulsion was defined as no IUD within the uterus, either with a clinical history consistent with an IUD expulsion, or confirmed by transvaginal ultrasonography. Women who experienced an IUD expulsion during the 6-month study period were offered an IUD replacement at no charge. Women were considered satisfied with their IUD if they responded yes to the question: “Would you recommend an IUD as a method of contraception to a friend?”
To estimate the sample size, we expected that 66% of women analyzed in the interval group and 91% of women analyzed in the intracesarean group would be using an IUD at the final 6-month study visit. We arrived at 66% because we anticipated that of the women in the interval group, 20% would not return for insertion. We additionally expected 8% of women in the interval arm would discontinue the IUD by 6 months, 13 that 1% of IUD placements would not be completed and 5% of IUDs would be expelled prior to 6 months postpartum14,15. We made an a priori assumption that 25% more women in the intracesarean group would be using an IUD at 6 months than in the interval group. Based on these estimates, using a 2-sided alpha of 0.05% and a beta of 0.20 (power of 80%) we calculated a required analysis sample size of 98 women (49 in each group). We anticipated a loss to follow-up of approximately 10-15% in each arm, so we set out to enroll and randomize 112 women (56 women in each group) to detect a 15% difference in IUD use at 6 months postpartum between groups.
Statistical analysis was performed using Stat a 12 (College Station, Texas, US). Primary analysis used intention-to-treat data. Proportions were compared using Pearson's chi-squared test for the primary outcome. Additionally, risk ratios and exact 95% confidence intervals were calculated for the primary outcome (IUD use at 6 months) as well as the secondary outcomes (IUD expulsions, IUD discontinuation, visible strings at 6 months, and satisfaction with IUD at 6 months).
Results
One hundred and seventy-two women were screened to reach our final enrollment group of 112 (Fig. 1). Our final analysis groups comprised participants from whom we collected outcome data at the 6-month visit; 48 of 56 women (86%) and 50 of 56 women (89%) in the intracesarean and interval arms, respectively.
Figure 1.
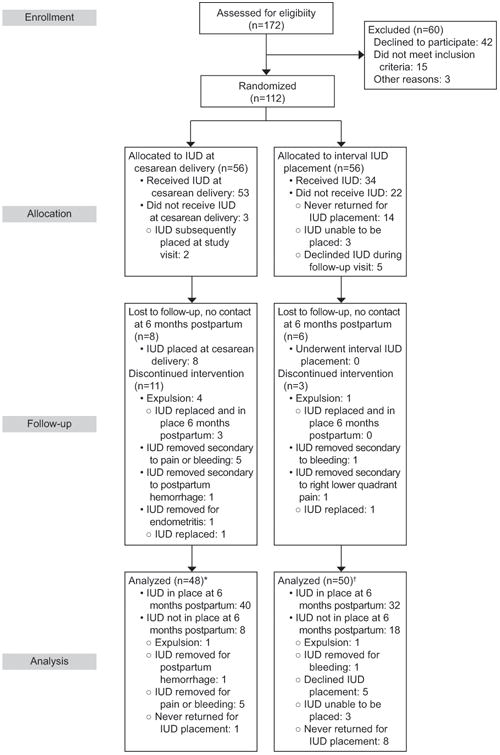
Flowchart of study participants. *Excluded from analysis (lost to follow-up), n=8. †Excluded from analysis (lost to follow-up), n=6.
Baseline characteristics were similar between the randomized groups (Table 1). There were no significant differences in the baseline characteristics of the women lost to follow-up compared to those women for whom follow-up data were available.
Table 1. Baseline characteristics of women allocated to intrauterine device (IUD) placement during cesarean (intracesarean) or interval placement 6 or more weeks after delivery.
| Intracesarean IUD Placement N=56 N (%) | Interval IUD Placement N=56 N (%) | |
|---|---|---|
| Age (years)* | 28 +/- 5.7 | 29 +/- 5.1 |
| Parity at Admission | ||
| 0 | 17 (30) | 12 (21) |
| 1 | 21 (38) | 24 (43) |
| 2 | 13 (23) | 14 (25) |
| >2 | 5 (9) | 6 (10) |
| Race/Ethnicity | ||
| White | 26 (46) | 22 (39) |
| Black | 13 (23) | 15 (27) |
| Hispanic | 13 (23) | 18 (32) |
| Asian | 2 (4) | 0 (0) |
| Other | 2 (4) | 1 (2) |
| Educational Status | ||
| HS or less | 26 (46) | 27 (48) |
| Some College | 23 (41) | 23 (41) |
| Post College | 7 (13) | 6 (11) |
| Marital Status | ||
| Married or Living with Partner | 43 (77) | 43 (77) |
| Single | 13 (33) | 13 (33) |
| Monthly Household Income | ||
| 0-250 | 3 (5) | 3 (5) |
| 251-500 | 3 (5) | 4 (7) |
| 501-1000 | 7 (13) | 3 (5) |
| 1001-2000 | 11 (20) | 22 (39) |
| 2001-3000 | 9 (16) | 3 (5) |
| Over 3000 | 17 (30) | 16 (29) |
| Refuse to answer | 6 (11) | 5 (9) |
| Prior IUD use | 17 (30) | 19 (34) |
| Indication for Cesarean delivery | ||
| Repeat or elective | 41 (73) | 41 (73) |
| Fetal status | 4 (7) | 2 (4) |
| Malpresentation | 6 (11) | 6 (11) |
| Failure to progress | 5 (9) | 7 (13) |
| Cervical Dilation at time of Cesarean delivery | ||
| 0-1cm | 46 (82) | 45 (80) |
| 2-5cm | 6 (11) | 6 (11) |
| 6-10cm | 4 (7) | 5 (9) |
| IUD type placed | N=55 | N=34 |
| LNG-IUS | 40 (73) | 30 (88) |
| Copper IUD | 15 (27) | 4 (12) |
Mean +/- SD
There were no statistically significant differences of any characteristics between the two groups using Pearson's chi-squared and student T-test where appropriate.
Of the women allocated to the intracesarean group 53 of 56 women (95%) received their assigned IUD at the time of cesarean delivery (Fig. 1). Three women did not have their IUD placed at the time of cesarean delivery because the surgical team did not remember or did not know to place the device. Two of these three women subsequently had an IUD placed at their six-week visit. Mean time from placental delivery to IUD insertion was 1.6 minutes (1.2-1.9 95%CI). Of the 55 women in this group who received an IUD, 40 (73%) chose a LNG-IUS and 15 (27%) chose a Copper IUD.
Of the women 56 women allocated to interval IUD insertion, 34 (63%) had an IUD successfully placed. Thirty (86%) women chose a LNG-IUS, and 4 (14%) women opted for a Copper IUD. Of the 22 women who did not receive an IUD, 14 (25%) never returned for any study visit after enrollment. Five (9%) women declined an IUD during their follow-up visit. Three (5%) women underwent an attempt at IUD placement, however, the IUD could not be successfully placed because of an inability to traverse the internal cervical os.
A larger proportion of the intracesarean group were using an IUD at the final 6-month visit (40/48; 83%) compared to the interval group (32/50; 64%) (RR=1.3, 95% CI: 1.02, 1.66) (Table 2). We performed sensitivity analyses to estimate the impact of the women lost to follow-up. Overall we had a 13% loss to follow-up with similar loss to follow-up in both arms, 14% and 11% in the intracesarean and interval IUD placement groups, respectively. Baseline characteristics among those who were lost to follow up were similar to those women for whom follow-up information was available. When we assumed the same proportion of IUDs (83%) in the intracesarean group were retained among the women who were lost-follow-up as in the cohort for whom follow-up data were available, the proportion of IUDs retained was 82% (46/56) in the intracesarean group and 57% (32/56) in the interval group, resulting in an effect size between intervention groups that was slightly larger (RR=1.44; 95% CI: 1.11, 1.86). Using a more conservative approach, when we assumed the unlikely event that all 8 women lost-to-follow-up in the intracesarean group did not have an IUD in place at 6 months postpartum (40/56), the effect size between intervention groups remained similar to our original analysis estimate (RR=1.25; 95% CI: 0.94, 1.66), however, there was no significant difference in IUD use at 6 months between the two groups.
Table 2. Outcomes related to intrauterine device use at 6 months postpartum for women who were allocated to IUD placement during cesarean delivery (intracesarean) or interval placement 6 or more weeks after delivery.
| Intracesarean IUD | Interval IUD | RR (95% CI) | |
|---|---|---|---|
| Primary Outcome: | |||
| IUD use at 6 months postpartum (N=98) | 40/48 (83%) | 32/50 (64%) | 1.3 (1.02-1.66) |
| Secondary Outcomes: | |||
| IUD expulsion (N=98) | 4/48 (8%) | 1/50 (2%) | 4.2 (0.48-35.95) |
| IUD discontinuation (N=98) | 7/48 (15%) | 2/50 (4%) | 3.6 (0.80-16.68) |
| IUD strings visible at 6 months PP (N=55) | 17/31 (56%) | 18/24 (75%) | 0.7 (0.49-1.08) |
| By IUD type: | |||
| LNG-IUS (N=41) | 13/21 (67%) | 16/20 (80%) | |
| Copper IUD (N=14) | 4/10 (40%) | 2/4 (50%) | |
| Satisfaction with IUD (N=69) | 36/39 (92%) | 30/30 (100%) | 0.9 (0.84-1.01) |
IUD, intrauterine device.
All four expulsions in the intracesarean group occurred within the first 3 weeks postpartum; mean time to expulsion was 12.6 days (Table 2). All four of these women had 0-1cm of cervical dilation at the time of cesarean delivery and IUD placement. Three of the women wanted another IUD placed and underwent successful IUD placement at the six week visit. The remaining woman opted to use a contraceptive implant. One woman in the interval group had an IUD expulsion. Although she had a replacement IUD, that second IUD was also expulsed within 10 days of placement. She subsequently chose to use condoms as her contraceptive method. All expulsed IUDs were LNG-IUS devices and were complete expulsions; each woman stated she was aware of the expulsion at the time that it occurred.
In the intracesarean group, seven (15%) women had their IUDs removed prior to 6 months postpartum. One woman had a postpartum hemorrhage in the operating room after IUD placement and hysterotomy closure and she underwent cesarean hysterectomy. Another woman developed endometritis on postpartum day 5, was readmitted to the hospital, and had her IUD removed upon admission. Her IUD strings were not visible and her IUD was removed using an alligator forceps under ultrasound guidance. Her endometritis resolved with 24 hours of treatment with IV antibiotics. She subsequently had an IUD placed at 12 weeks postpartum and was using this IUD at 6 months postpartum. Five women underwent IUD removal due to side effects; primarily bleeding, pelvic pain, or both.
In the interval insertion group two (4%) women had their IUD removed during the study period due to: bleeding (1) and right lower quadrant pain (1). The women who had her IUD removed secondary to right lower quadrant pain was subsequently diagnosed with nephrolithiasis and chose to have her IUD replaced at her 3-month visit.
Fifty five women returned for in person 6-month study visits and underwent a speculum examination to check for IUD strings. The remaining women provided follow-up information by phone. Among the 55 women who underwent a speculum examination, strings were visualized in 56% and 75% of the women in the intracesarean and interval groups respectively. In both groups, women who chose to use a LNG-IUS were more likely to have strings visible at 6 months postpartum than those women who were using a copper IUD.
Overall women in both groups were satisfied with their IUDs. In the intracesarean group, 92% (36/39) and 100% (30/30) of the women in the interval group stated that they would recommend an IUD as a method of contraception to a friend.
The study authors became aware of two pregnancies that occurred among study participants once the 6 months of study follow up had been completed. Both women had been randomized to the interval insertion group. One woman never returned for any subsequent study visits after enrollment but reported during phone follow-up that she had had an ectopic pregnancy 7 months postpartum. She had not been using a method of contraception at that time. One woman had a copper IUD placed at her six week visit. Follow-up ultrasound was consistent with an appropriately positioned IUD when IUD strings were not visualized. More than 1 year after her IUD insertion she became pregnant, and imaging showed her IUD was in her abdomen. She subsequently had an uncomplicated pregnancy with a repeat term cesarean delivery.
Discussion
IUD placement at the time of cesarean delivery resulted in a higher proportion of IUD use at 6 months postpartum. In our study women were offered access to free IUDs and compensation for attendance at each study visit, and still, 25% did not return for any visit following delivery. Existing data suggests that women who don't return for postpartum visits are more likely to be socially and economically disadvantaged6 and that for some women attendance at a visit represents a barrier to IUD initiation and placement16. The results of this study provide another contraceptive option to women without the need for a postpartum visit.
This data from this study add to the growing body of evidence that provision of long-acting reversible contraception (LARC) at the time of delivery leads to increased use of effective contraception.1,17-19 IUDs in this study were placed by the residents and faculty working on Labor and Delivery after only a ten-minute training on IUD placement at the time of cesarean delivery. This suggests that an 8% 6-month IUD expulsion risk among the women who received an IUD at the time of cesarean is achievable for most practitioners without extensive training. Prior studies have examined the cost-effectiveness of providing state-funded immediate postpartum IUDs and have found the intervention to be cost-saving20, however, a cost-benefit analysis was not performed in conjunction with this study.
Women undergoing intracesarean delivery IUD placement should be counseled about the possibility of IUD expulsion and that their IUD strings may not be visible. Possible techniques for IUD removal without visible IUD strings should be discussed. The women in the interval group had an unexpectedly high proportion of non-visible IUD strings21 at 6 months postpartum. It is unclear if placement techniques used by the providers were responsible or if IUDs placed at 6 weeks postpartum (as opposed to at a time not related to a pregnancy) are less likely to have IUD strings visible by 6 months postpartum. Additionally the potential interventions and costs associated with IUD removal in the case of non-visible IUD strings are an important area of future study. Although all of the expulsions in this study were the LNG-IUS, the study was not designed to determine if there is a significant difference in the expulsion risk by IUD type.
Our study population was representative of the population of women served by North Carolina Women's Hospital, but may not be generalizable to other populations. In 2010, the most recent year for which data is available, 49% of women delivering at the Hospital had public insurance. Additionally, there was significant racial, ethnic, and socioeconomic diversity reflected in our study population. Prior studies have shown that women who are financially and socially disadvantaged may be less likely to attend postpartum visits4, and certainly this may have contributed to some loss to follow-up among women in this study.
The missing data from the women who were lost to follow-up is a weakness of our study. Our sensitivity analysis showed that our results remained statistically significant when IUD use at 6 months among those women lost to follow-up maintained proportions similar to those among women for whom follow-up data were available. In the unlikely event that all 8 women who were lost to follow-up in the intracesarean group had their IUDs removed or expulsed by 6 months postpartum, the resulting effect size was similar to the effect we observed for our original estimates, although it did not reach statistical significance.
Reimbursement policies remain a significant barrier to the initiation of LARC methods during the immediate postpartum period. As of December 2014, eleven states in the US have adapted Medicaid policies that allow for reimbursement of LARC devices placed during the admission for delivery. ACOG supports the practice of immediate post-placental IUD placement22, and expert consensus supports aligning practice and reimbursement incentives to promote immediate postpartum initiation of LARC methods17. These recent policy changes and the results from this study support increasing the availability of intracesarean delivery IUD placement. As cesarean delivery represented 32.3% of all births in the United States in 200823, IUD placement at time of cesarean could be a safe, effective and convenient method of postpartum contraception available to 1.4 million women a year.
Acknowledgments
This project was funded by the Society of Family Planning Research Fund. TEVA Women's Health provided the Copper T380A devices for this project. The project was supported by the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health, through Grant Award Number 1UL1TR001111. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
The authors thank the support we received from Karen Dorman and her research team, and all the residents, clinical staff, and clinical faculty at the North Carolina Women's Hospital for their enthusiastic support for the study.
Footnotes
Financial Disclosure: The authors did not report any potential conflicts of interest.
References
- 1.Tocce KM, Sheeder JL, Teal SB. Rapid repeat pregnancy in adolescents: do immediate postpartum contraceptive implants make a difference? American journal of obstetrics and gynecology. 2012 Jun;206(6):481 e481–487. doi: 10.1016/j.ajog.2012.04.015. [DOI] [PubMed] [Google Scholar]
- 2.Speroff L, Mishell DR., Jr The postpartum visit: it's time for a change in order to optimally initiate contraception. Contraception. 2008 Aug;78(2):90–98. doi: 10.1016/j.contraception.2008.04.005. [DOI] [PubMed] [Google Scholar]
- 3.Ogburn JA, Espey E, Stonehocker J. Barriers to intrauterine device insertion in postpartum women. Contraception. 2005 Dec;72(6):426–429. doi: 10.1016/j.contraception.2005.05.016. [DOI] [PubMed] [Google Scholar]
- 4.Lu MC, Prentice J. The postpartum visit: risk factors for nonuse and association with breast-feeding. American journal of obstetrics and gynecology. 2002 Nov;187(5):1329–1336. doi: 10.1067/mob.2002.126848. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.DiBari JN, Yu SM, Chao SM, Lu MC. Use of postpartum care: predictors and barriers. Journal of pregnancy. 2014;2014:530769. doi: 10.1155/2014/530769. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bryant AS, Haas JS, McElrath TF, McCormick MC. Predictors of compliance with the postpartum visit among women living in healthy start project areas. Maternal and child health journal. 2006 Nov;10(6):511–516. doi: 10.1007/s10995-006-0128-5. [DOI] [PubMed] [Google Scholar]
- 7.Grimes DA, Lopez LM, Schulz KF, Van Vliet HA, Stanwood NL. Immediate post-partum insertion of intrauterine devices. Cochrane Database Syst Rev. 2010;(5):CD003036. doi: 10.1002/14651858.CD003036.pub2. [DOI] [PubMed] [Google Scholar]
- 8.Kapp N, Curtis KM. Intrauterine device insertion during the postpartum period: a systematic review. Contraception. 2009 Oct;80(4):327–336. doi: 10.1016/j.contraception.2009.03.024. [DOI] [PubMed] [Google Scholar]
- 9.Zhou SW, Chi IC. Immediate postpartum IUD insertions in a Chinese hospital--a two year follow-up. International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics. 1991 Jun;35(2):157–164. doi: 10.1016/0020-7292(91)90820-u. [DOI] [PubMed] [Google Scholar]
- 10.Celen S, Moroy P, Sucak A, Aktulay A, Danisman N. Clinical outcomes of early postplacental insertion of intrauterine contraceptive devices. Contraception. 2004 Apr;69(4):279–282. doi: 10.1016/j.contraception.2003.12.004. [DOI] [PubMed] [Google Scholar]
- 11.Letti Muller AL, Lopes Ramos JG, Martins-Costa SH, Palma Dias RS, Valerio EG, Hammes LS, et al. Transvaginal ultrasonographic assessment of the expulsion rate of intrauterine devices inserted in the immediate postpartum period: a pilot study. Contraception. 2005 Sep;72(3):192–195. doi: 10.1016/j.contraception.2005.03.014. [DOI] [PubMed] [Google Scholar]
- 12.Schulz KF, Altman DG, Moher D. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials. Trials. 2010;11:32. doi: 10.4103/0976-500X.72352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Peipert JF, Zhao Q, Allsworth JE, Petrosky E, Madden T, Eisenberg D, et al. Continuation and satisfaction of reversible contraception. Obstetrics and gynecology. 2011 May;117(5):1105–1113. doi: 10.1097/AOG.0b013e31821188ad. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sivin I, Schmidt F. Effectiveness of IUDs: a review. Contraception. 1987 Jul;36(1):55–84. doi: 10.1016/0010-7824(87)90061-8. [DOI] [PubMed] [Google Scholar]
- 15.Rivera R, Chen-Mok M, McMullen S. Analysis of client characteristics that may affect early discontinuation of the TCu-380A IUD. Contraception. 1999 Sep;60(3):155–160. doi: 10.1016/s0010-7824(99)00077-3. [DOI] [PubMed] [Google Scholar]
- 16.Bergin A, Tristan S, Terplan M, Gilliam ML, Whitaker AK. A missed opportunity for care: two-visit IUD insertion protocols inhibit placement. Contraception. 2012 Dec;86(6):694–697. doi: 10.1016/j.contraception.2012.05.011. [DOI] [PubMed] [Google Scholar]
- 17.Aiken AR, Creinin MD, Kaunitz AM, Nelson AL, Trussell J. Global fee prohibits postpartum provision of the most effective reversible contraceptives. Contraception. 2014 Nov;90(5):466–467. doi: 10.1016/j.contraception.2014.08.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Baldwin MK, Edelman AB. The effect of long-acting reversible contraception on rapid repeat pregnancy in adolescents: a review. The Journal of adolescent health : official publication of the Society for Adolescent Medicine. 2013 Apr;52(4 Suppl):S47–53. doi: 10.1016/j.jadohealth.2012.10.278. [DOI] [PubMed] [Google Scholar]
- 19.Rodriguez MI, Evans M, Espey E. Advocating for immediate postpartum LARC: increasing access, improving outcomes, and decreasing cost. Contraception. 2014 Nov;90(5):468–471. doi: 10.1016/j.contraception.2014.07.001. [DOI] [PubMed] [Google Scholar]
- 20.Rodriguez MI, Caughey AB, Edelman A, Darney PD, Foster DG. Cost-benefit analysis of state- and hospital-funded postpartum intrauterine contraception at a university hospital for recent immigrants to the United States. Contraception. 2010 Apr;81(4):304–308. doi: 10.1016/j.contraception.2009.11.002. [DOI] [PubMed] [Google Scholar]
- 21.Marchi NM, Castro S, Hidalgo MM, Hidalgo C, Monteiro-Dantas C, Villarroeal M, et al. Management of missing strings in users of intrauterine contraceptives. Contraception. 2012 Oct;86(4):354–358. doi: 10.1016/j.contraception.2012.01.018. [DOI] [PubMed] [Google Scholar]
- 22.American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 121: Long-acting reversible contraception: Implants and intrauterine devices. Obstetrics and gynecology. 2011 Jul;118(1):184–196. doi: 10.1097/AOG.0b013e318227f05e. [DOI] [PubMed] [Google Scholar]
- 23.Osterman MJ, Martin JA, Mathews TJ, Hamilton BE. Expanded data from the new birth certificate, 2008. National vital statistics reports : from the Centers for Disease Control and Prevention, National Center for Health Statistics, National Vital Statistics System. 2011 Jul 27;59(7):1–28. [PubMed] [Google Scholar]