

Abstract
Background:
Toothbrushing is an important aspect of children's oral health self-care. This study aimed to explore toothbrushing frequency among 4–6-year-old Iranian children and associated maternal attitude and sociobehavioral factors.
Materials and Methods:
This cross-sectional study was conducted on 407 mother–child (aged 4–6 years) pairs through stratified random sampling in Tabriz, Iran. Data were collected using self-reported questionnaires including demographic characteristic, maternal attitude, and toothbrushing frequency of both mothers and children. Logistic regression was used to determine the predicators of children's toothbrushing. Statistical significance was set at P < 0.05 for all tests.
Results:
The mean ages were 32.6 ± 4.8 and 5.3 ± 1.1 years for mothers and children respectively. Twice-daily toothbrushing was observed at a relative frequency of 12.8% in children and 18.4% in mothers. About 43.7% of children brushed their teeth once daily. Nearly 38.7% of children started toothbrushing behavior regularly at 4 years of age, and 41% had dental visits. Multiple logistic regression analysis indicated that children's toothbrushing (once daily or more) was associated with maternal brushing frequency (odds ratio [OR] =2.0, 95% confidence interval [CI] =1.53–2.86), maternal attitude toward oral health (OR = 1.15, CI = 1.08–1.22), and children's age (OR = 1.21, 95% CI = 1.02–1.77).
Conclusion:
The descriptive results indicated that maternal and children toothbrushing behaviors are unfavorable. Furthermore, maternal toothbrushing behavior is a strong predicator of children's brushing behavior. Health promotional activities seem necessary for mothers to enhance oral health behavior of their children.
Keywords: Attitude, child, oral health, toothbrushing
INTRODUCTION
Nowadays, dental caries is one of the most common chronic diseasesamong children.[1] According to the WHO, at least one in four of 5–6-year-old children suffer from tooth decay.[2] Iran's National Oral Health Survey reported that 89% of 6-year-old children had dental caries experience, and decayed, missing, and filled teeth (dmft) score was 5 for 6-year-old and 1.9 for 3-year-old children.[3]
Early childhood caries (ECC) influences oral health, well-being of young children, and their quality of life.[4] In addition, it can be associated with processes of socialization, communication, and self-esteem.[5] However, ECC is generally preventable[6,7] and is related to lifestyle,[8] oral health behaviors, feeding habit, and access dental care to a large extent.[9,10]
Promoting toothbrushing and use of fluoride are two main approaches to prevent dental caries in children.[11] “Toothbrushing is the most effective method of oral hygiene, and the universally recommended frequency has been twice a day.”[12] Furthermore, toothbrushing twice daily is a part of recommended children's oral health self-care.[13,14] Parents’ duty to their children's oral health and toothbrushing habits is more important,[15,16] and brushing habits were mainly established by mothers (84%).[17] In a study by Bennadi et al., it was revealed that mother's attitude regarding oral health, knowledge, and practices had been associated with Indian children's dental caries prevalence.[18]
Despite recommendation of tooth brushingtwice-daily, it has been reported that i was less than recommended frequency from 5% (12–36-month-old children) to 46% (9-year-old children).[17,19] A few studies have been performed regarding the patterns of toothbrushing and modifying factors of this behavior.[11,12,13,14,15,16,17,18] Preschool children are only partially capable of toothbrushing, so parents should supervise them during brushing.[20] To the best of our knowledge, this study is one of the few studies that have investigated toothbrushing frequency and influence of mothers’ sociobehavioral factors in 4–6-year-old children in Iran.
Understanding the importance of this issue can be beneficial to design more effective interventions to promote oral health programs. The aims of the present study were as follows: (1) to determine the toothbrushing behavior in Iranian preschool children; (2) to determine the relationship between maternal sociobehavioral factors and toothbrushing frequency among 4–6-year-old children.
MATERIALS AND METHODS
Participants and study design
This cross-sectional study was conducted on 407 mothers of children aged 4–6 years referred to the health centers of the Tabriz University of Medical Sciences from August 2014 to November 2014, Tabriz, Iran.
Stratified sampling was used for sample selection. From a list of all 40 health centers[20] in Tabriz, 15 centers were randomly selected. Then, according to the proportion of clients in each health center, children aged 4–6 years were randomly selected (15–35 children per center).
The sample size was determined as 421 participants based on 48% prevalence of toothbrushing once a day,[17] level of confidence (zα/2 = 1.96), 5% level of precision, and 10% nonresponse rate. The inclusion criteria included children's age between 4 and 6 years, maternal willing to participate in this survey, and not suffering from obvoious physical, mental, and emotional diseases. After obtaining informed consent, children and their mothers voluntarily participated in the study.
Questionnaire
Data were collected through the self-administered questionnaires which were completed by the mothers of 4–6-year-old children.
The questionnaire included sociodemographic variables, maternal attitude toward oral, and toothbrushing frequency of both mothers and children.
Sociodemographic characteristics included maternal and child age (in year), maternal employment status and educational level (illiterate, primary school, secondary school, high school, diploma, and academic education), child's gender, and the number of children in houshold.
The frequency of child toothbrushing was measured through a statement asking from mothers, “How often do you usually brush your child's teeth or your child brushes his/her own teeth?” using the 5-point scale (1 = never, 2 = rarely, 3 = a few times a week, 4 = once daily, and 5 = twice daily or more). Reasons were categorized in two levels:[21] once a day or more (once daily and twice daily or more) and less than once a day (never, rarely, and a few times a week) for use in logistic analyses.
The maternal attitude was measured using six statements describing mothers’ opinion about children oral health adapted in the previous study, in which the reliability was reported (0.86).[22] The responses of each attitude statement were ranged from “strongly agree” to “strongly disagree” in a 5-point Likert scale. The possible score range was 6–30, and a higher score indicated a higher attitude. The examples of attitude items are as follows: “it is important to do routine dental examination for children,” “oral health problems can lead to general health problems in children,” and “toothbrushing is an important aspect of child’ oral health care.”
The content validity of the questionnaire was confirmed by the expert panel of ten academicians (dental public health, health education, and health workers). The mean content validity ratio (CVR) was calculated as 0.85. For calculating the CVR, the experts rated each item of the questionnaire on a 3-point rating scale (1 = it is essential, 2 = it is useful but not essential, and 3 = it is not essential). The CVR for each item was calculated using the formula, CVR = (Ne – [N/2])/(N/2) where Ne is the number of experts indicating “essential” for each item of the questionnaire and N is the total number of experts. The numeric value of CVR is determined by Lawshe table, and the CVR value of 0.62 or above is acceptable. The reliability of the questionnaire was assessed by test–retest (2-week interval) among 30 eligible mothers in a health center, and the obtained data were not included in the final analysis. The test–retest reliability coefficient was 0.81.
Statistical analysis
Descriptive statistics were performed to explore the data (means and standard deviation [SD] for quantitative variables and frequencies for categorical variables). Simple and multiple logistic regression models (results were reported as odds ratio [OR] with 95% confidence interval [CI]) were performed to assess the association between dependent and independent variables. SPSS version 20 (SPSS, Inc., Chicago, IL, USA) statistical software was used to analyze the data. The P value of <0.05 was taken as statistically significant.
Ethical issues
After approval of the Ethics Committee of Isfahan University of Medical Sciences, Iran (Project Number 393296), written consent was obtained from participating mothers who volunteered to enter the study. The purpose of the study was explained, and the questionnaires were completed anonymously.
RESULTS
A total number of 407 pairs of mothers and children aged 4–6 years participated in this study. The participation rate was 95.2.
The mean age of mothers was 32.6 years (range: 20–48 years, SD = 4.8) and of children 5.3 years (range: 4–6, SD = 1.1). According to the results, 23.2% (n = 95) of mothers were in higher educational level and 1.7% (n = 7) were illiterate. The majority (89.7%) of mothers were unemployed [Table 1].
Table 1.
Socio-demographic and clinical characteristics for mothers and children
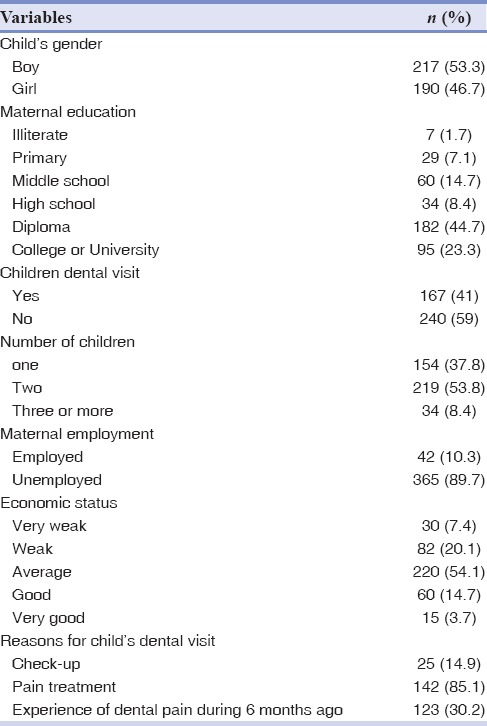
Based on the results as shown in Table 1, the prevalence for brushing frequency twice a day was 18.4% (n = 75) and 12.8% (n = 52) for mothers and children, respectively. The majority (43.7%) of children brushed their teeth once a day (95% CI = 38.9%–48.5%). In addition, brushing frequency rarely or never was reported 7.3% (n = 30) for mothers and 24.3% (n = 99) for children.
The mean of maternal attitude score toward oral health was 23.8 (range: 6–30; SD = 4.5). The most of children (38.7%) started toothbrushing behavior from 4 years.
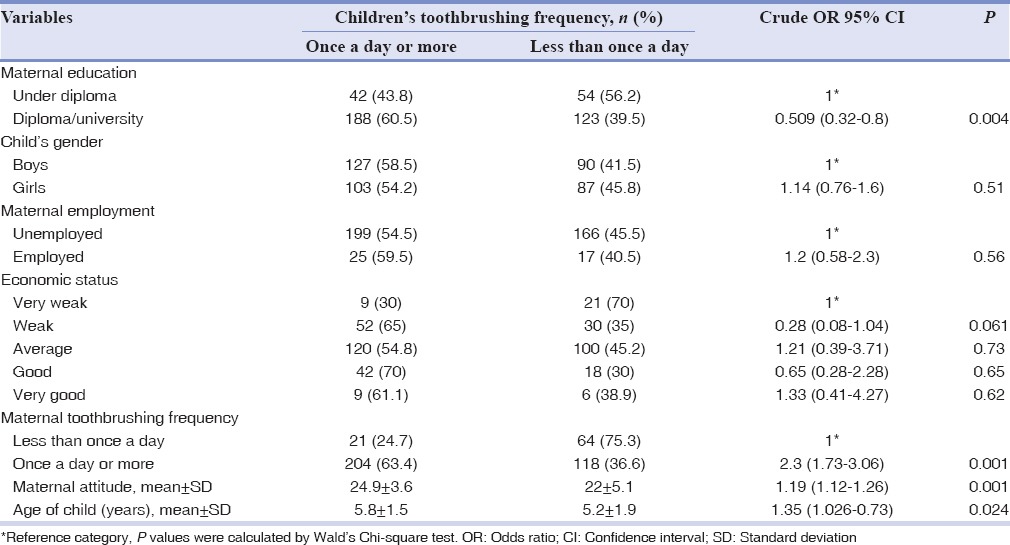
The simple logistic regression analysis indicated that children frequency of toothbrushing had a significant relationship with maternal frequency of toothbrushing, educational level, and attitude toward oral health [Table 2]. Furthermore, there was a significant difference between child toothbrushing and his/her age. There was no statistically significant difference between toothbrushing frequency and child's gender [Table 3].
Table 2.
Tooth brushing frequency for maternal and children of the study sample
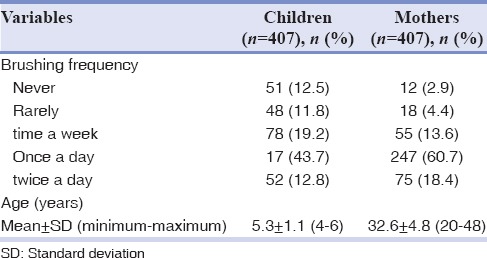
Table 3.
Simple logistic regression analysis for children's brushing (once a day or more vs. less than once a day)
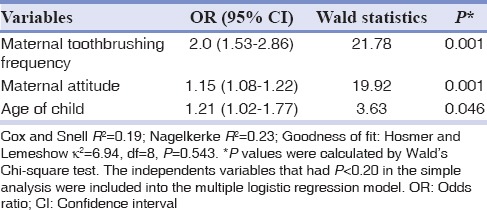
Based on the results as shown in Table 4, the multiple logistic regression analysis indicated that maternal toothbrushing frequency (OR = 2.0, 95% CI = 1.53–2.86), attitude toward oral health (OR = 1.15, 95% CI = 1.08–1.22), and child's age (OR = 1.21, 95% CI = 1.0–1.77) were the significant predicting factors for children's toothbrushing once a day or more.
Table 4.
Multiple logistic regressions for children's brushing frequency (once a day or more vs. less than once a day) and intendant variables
DISCUSSION
According to the results of this study, children's brushing frequency twice a day was 12.8% and once a day 43.7%. In Asgari et al.'s study, it was found that “twice a day” brushing frequency was 14.3% among individuals aged between 6 and 70 years.[23] In another study performed in Iran, mothers reported twice-daily oral cleaning by 5% of children aged 12–36 months.[13] Furthermore, in a cross-sectional study in India, it was 16.3%.[17] This finding contrasts with of some other studies in this filed. The results of some other studies about children's toothbrushing behavior are more desirable than that of the present study; for instance, in Chu et al.'s study 75% of preschool children[24] and in Wigen and Wang longitudinal study 61% of 3-year-old and 79% of 5-year-old children were reported twice-daily toothbrushing, respectively.[11] Twice-daily brushing in Poland and Australia was reported by 18% and 61%, respectively.[25,26]
This low toothbrushing frequency can be related to the health determiners such as socioeconomic, sociodemographic,[22] and primary health-care delivery system. Hence, appropriate program to promote oral health behaviors is an urgent need. “Pattern of oral health behavior–toothbrushing–learned during early years of life is stabilized during preschool age.”[11] Hence, appropriate program to promote oral health behaviors is an urgent need.
The present study has observed a significant association between maternal and children toothbrushing frequency. The logistic regression analysis indicated that mothers’ toothbrushing frequency was the significant predicting factor for children's toothbrushing. This finding is consistent with several previous studies that found a significant association between mothers and their children toothbrushing frequency.[13,16,27]
In a cross-sectional study in southern Taiwan, caregivers’ toothbrushing was a significant indicator for the toothbrushing behavior of the children.[16] In the study by Mohebbi et al., the frequency of oral cleaning for the child was directly related to the mother's toothbrushing frequency.[13] The brushing habits were mainly introduced by mothers.[17] Hence, mothers should not only obtain oral health knowledge but also be aware of their role-modeling responsibility to children. Health promotional activities seem necessary for maternal to enhance oral health behavior of their children.
This study showed that child's toothbrushing was significantly associated with maternal attitude toward oral health. In mothers with higher attitude, frequency of children's toothbrushing (once daily or more) was higher as compared to children of mothers with low attitude. This finding confirms other studies; it was found a positive relationship between maternal attitude toward oral health and children's toothbrushing frequency.[28] Bennadi et al. also found maternal attitude as a risk factor for caries prevalence in 3–6-year-old children.[18] Saied-Moallemi et al. also reported a significant relationship between maternal positive attitude and their third-grade school children's toothbrushing in Tehran city.[15]
Attitude is one of the predisposing factors toward achieving health promoting behaviors. Health-care professionals should implement programs to increase maternal attitude regarding oral health which could lead to healthy dental habits and promotion in children's brushing.
This study demonstrated a significant relationship between age and toothbrushing frequency. These findings are in line with accordance with earlier findings. A longitudinal study by Wigen and Wang demonstrated toothbrushing twice daily increase in 1.5-year-old children from 52% to 76% in 5-year-old children.[11] In other studies, once-daily oral cleaning had significant deference with age (18% of 16–23-month-old children vs. 48% of 24–36).[13] Furthermore, this finding was in line with Maes et al.'s study about toothbrushing in adolescents in 32 countries which showed an increase in brushing frequency with age increasing.[12]
The results of this study showed that majority (38.7%) of children started toothbrushing from about 4 years. According to a study performed in Hong Kong, toothbrushing starting age was reported >24 months for 41% of preschool children.[24] In a cross-sectional study by Pullishery et al., the mean age of toothbrushing starting was 22.4 months.[17] The results of these findings about toothbrushing starting age are better than the results of this study finding. This hesitation in starting toothbrushing can be due to the inadequate oral health-related knowledge and dental health-care delivery system for children. The American Academy of Pediatric Dentistry recommends that oral cleaning starting time is no later than the time of eruption of the first primary tooth.[29]
The results of the simple regression analysis are shown in Table 3. Maternal education level is associated with children toothbrushing frequency, so that children of mothers with higher education are more likely to have better oral health behaviors (OR = 0.509). This finding is consistent with Vallejos-Sánchez et al.'s study.[28] An important socioeconomic indicator is mother education level which reflects knowledge and skills for making health behavior choices such as oral health-related behavior.[30]
There were some limitations in this study. First, this was a cross-sectional study, and the questionnaire was self-reported that can be a subject to recall error. Furthermore, there was no clinical examination (dental caries or plaque index) which was the another limitation of this study.
CONCLUSION
Based on the results of this study, toothbrushing frequency was not in desirable status with regard to recommendations. In addition, maternal toothbrushing and attitude were the strongest predicators of child toothbrushing. Hence, health promotion interventions based on mothers training needs about oral health seem necessary. Health providers in health centers, who provide primary health care for mothers and children, need to disseminate educational interventions and accurate information about oral health care for mothers. It is necessary to encourage mothers own regular toothbrushing behavior and promote educational activities through dentists, health-care providers, and pediatrics.
Financial support and sponsorship
Nil.
Conflicts of interest
The authors of this manuscript declare that they have no conflicts of interest, real or perceived, financial or non-financial in this article.
Acknowledgments
The authors appreciate the Education Deputy of Isfahan University of Medical Sciences for their financial support, participants who participated in completing the questionnaires, and the staff of health centers in Tabriz for their cooperation.
REFERENCES
- 1.Tanaka K, Miyake Y, Sasaki S, Hirota Y. Socioeconomic status and risk of dental caries in Japanese preschool children: The Osaka Maternal and child health study. J Public Health Dent. 2013;73:217–23. doi: 10.1111/jphd.12016. [DOI] [PubMed] [Google Scholar]
- 2.World Health Organization. Information Series on School Health Document Seven, Oral Health Promotion: An Essential Element of Health Promoting School. Geneva: World Health Organization; 2002. [Google Scholar]
- 3.Bayat-Movahed S, Samadzadeh H, Ziyarati L, Memary N, Khosravi R, Sadr-Eshkevari PS. Oral health of Iranian children in 2004: A national pathfinder survey of dental caries and treatment needs. East Mediterr Health J. 2011;17:243–9. [PubMed] [Google Scholar]
- 4.Braun PA, Lind KE, Henderson WG, Brega AG, Quissell DO, Albino J. Validation of a pediatric oral health-related quality of life scale in Navajo children. Qual Life Res. 2015;24:231–9. doi: 10.1007/s11136-014-0751-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Rowan-Legg A. Canadian Paediatric Society. Community Paediatrics Committee. Oral health care for children – A call for action. Paediatr Child Health. 2013;18:37–50. doi: 10.1093/pch/18.1.37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Trubey RJ, Moore SC, Chestnutt IG. Children's toothbrushing frequency: The influence of parents’ rationale for brushing, habits and family routines. Caries Res. 2015;49:157–64. doi: 10.1159/000365152. [DOI] [PubMed] [Google Scholar]
- 7.Paterson JE, Gao W, Sundborn G, Cartwright S. Maternal self-report of oral health in six-year-old Pacific children from South Auckland, New Zealand. Community Dent Oral Epidemiol. 2011;39:19–28. doi: 10.1111/j.1600-0528.2010.00575.x. [DOI] [PubMed] [Google Scholar]
- 8.Nakayama Y, Mori M. Association between nocturnal breastfeeding and snacking habits and the risk of early childhood caries in 18- to 23-month-old Japanese children. J Epidemiol. 2015;25:142–7. doi: 10.2188/jea.JE20140097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Van den Branden S, Van den Broucke S, Leroy R, Declerck D, Bogaerts K, Hoppenbrouwers K. Effect evaluation of an oral health promotion intervention in preschool children. Eur J Public Health. 2014;24:893–8. doi: 10.1093/eurpub/ckt204. [DOI] [PubMed] [Google Scholar]
- 10.Naidu R, Nunn J, Forde M. Oral healthcare of preschool children in Trinidad: A qualitative study of parents and caregivers. BMC Oral Health. 2012;12:27. doi: 10.1186/1472-6831-12-27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Wigen TI, Wang NJ. Tooth brushing frequency and use of fluoride lozenges in children from 1.5 to 5 years of age: A longitudinal study. Community Dent Oral Epidemiol. 2014;42:395–403. doi: 10.1111/cdoe.12094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Maes L, Vereecken C, Vanobbergen J, Honkala S. Tooth brushing and social characteristics of families in 32 countries. Int Dent J. 2006;56:159–67. doi: 10.1111/j.1875-595x.2006.tb00089.x. [DOI] [PubMed] [Google Scholar]
- 13.Mohebbi SZ, Virtanen JI, Murtomaa H, Vahid-Golpayegani M, Vehkalahti MM. Mothers as facilitators of oral hygiene in early childhood. Int J Paediatr Dent. 2008;18:48–55. doi: 10.1111/j.1365-263X.2007.00861.x. [DOI] [PubMed] [Google Scholar]
- 14.Polk DE, Geng M, Levy S, Koerber A, Flay BR. Frequency of daily tooth brushing: Predictors of change in 9- to 11-year old US children. Community Dent Health. 2014;31:136–40. [PMC free article] [PubMed] [Google Scholar]
- 15.Saied-Moallemi Z, Virtanen JI, Ghofranipour F, Murtomaa H. Influence of mothers’ oral health knowledge and attitudes on their children's dental health. Eur Arch Paediatr Dent. 2008;9:79–83. doi: 10.1007/BF03262614. [DOI] [PubMed] [Google Scholar]
- 16.Hsieh HJ, Huang ST, Tsai CC, Hsiao SY. Toothbrushing habits and risk indicators of severe early childhood caries among aboriginal Taiwanese. Asia Pac J Public Health. 2014;26:238–47. doi: 10.1177/1010539511430721. [DOI] [PubMed] [Google Scholar]
- 17.Pullishery F, Shenoy Panchmal G, Shenoy R. Parental attitudes and tooth brushing habits in preschool children in Mangalore, Karnataka: A Cross-sectional Study. Int J Clin Pediatr Dent. 2013;6:156–60. doi: 10.5005/jp-journals-10005-1210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bennadi D, Reddy C, Sunitha S, Kshetrimayum N. Oral health status of 3-6 years old children and their mother's oral health related knowledge, attitude and practice in Mysore city, India. Asian J Med Sci. 2014;6:66–71. [Google Scholar]
- 19.Finlayson TL, Siefert K, Ismail AI, Sohn W. Maternal self-efficacy and 1-5-year-old children's brushing habits. Community Dent Oral Epidemiol. 2007;35:272–81. doi: 10.1111/j.1600-0528.2007.00313.x. [DOI] [PubMed] [Google Scholar]
- 20.Iranzad I, Bani S, Hasanpour S, Mohammadalizadeh S, Mirghafourvand M. Perceived social support and stress among pregnant women at health centers of Iran- Tabriz. J Caring Sci. 2014;3:287–95. doi: 10.5681/jcs.2014.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Casanova-Rosado AJ, Medina-Solís CE, Casanova-Rosado JF, Vallejos-Sánchez AA, Minaya-Sánchez M, Mendoza-Rodríguez M, et al. Tooth brushing frequency in Mexican schoolchildren and associated socio-demographic, socioeconomic, and dental variables. Med Sci Monit. 2014;20:938–44. doi: 10.12659/MSM.890106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Soltani R, Sharifirad G, Hasanzadeh A, Golshiri P, Barati M. Mothers’ knowledge and attitude on oral health preschool children in Isfahan, Iran. J Health Syst Res. 2013;9:712–9. [Google Scholar]
- 23.Asgari F, Majidi A, Koohpayehzadeh J, Etemad K, Rafei A. Oral hygiene status in a general population of Iran, 2011: A key lifestyle marker in relation to common risk factors of non-communicable diseases. Int J Health Policy Manag. 2015;4:343–52. doi: 10.15171/ijhpm.2015.18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Chu CH, Ho PL, Lo EC. Oral health status and behaviours of preschool children in Hong Kong. BMC Public Health. 2012;12:767. doi: 10.1186/1471-2458-12-767. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Baginska J, Rodakowska E. Knowledge and practice of caries prevention in mothers from Bialystok, Poland. Int J Collab Res Intern Med Public Health. 2012;4:256–66. [Google Scholar]
- 26.Kilpatrick NM, Neumann A, Lucas N, Chapman J, Nicholson JM. Oral health inequalities in a national sample of Australian children aged 2-3 and 6-7 years. Aust Dent J. 2012;57:38–44. doi: 10.1111/j.1834-7819.2011.01644.x. [DOI] [PubMed] [Google Scholar]
- 27.Manipal S, Joseph A, Adusumilli P, Ahmed A. Knowledge, attitude, of mothers on oral hygiene practices among 1-5 year old children and association with their oral hygiene practices – A comparitive study. Ann Essences Dent. 2012;4:19–24. [Google Scholar]
- 28.Vallejos-Sánchez AA, Medina-Solís CE, Maupomé G, Casanova-Rosado JF, Minaya-Sánchez M, Villalobos-Rodelo JJ, et al. Sociobehavioral factors influencing toothbrushing frequency among schoolchildren. J Am Dent Assoc. 2008;139:743–9. doi: 10.14219/jada.archive.2008.0256. [DOI] [PubMed] [Google Scholar]
- 29.Al-Zahrani AM, Al-Mushayt AS, Otaibi MF, Wyne AH. Knowledge and attitude of Saudi mothers towards their preschool children's oral health. Pak J Med Sci. 2014;30:720–4. doi: 10.12669/pjms.304.5069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Hooley M, Skouteris H, Boganin C, Satur J, Kilpatrick N. Parental influence and the development of dental caries in children aged 0-6 years: A systematic review of the literature. J Dent. 2012;40:873–85. doi: 10.1016/j.jdent.2012.07.013. [DOI] [PubMed] [Google Scholar]