

Abstract
Recent studies have confirmed that a single high-fat meal (HFM) leads to increased airway inflammation. However exercise is a natural anti-inflammatory and may modify post-prandial airway inflammation. The post-prandial airway inflammatory response is likely to be modified by chronic physical activity (PA) level.
Purpose
To investigate whether chronic PA modifies the airway inflammatory response to an acute bout of exercise in the post-prandial period in both insufficiently active and active subjects.
Methods
Thirty-nine non-asthmatic subjects (twenty active (ACT), 13M/7F) who exceeded PA guidelines (≥150 min moderate-vigorous PA/week) and (nineteen insufficiently active (IN), 6M/13F) underwent an incremental treadmill test to exhaustion to determine VO2peak. Subjects were then randomized to a condition (COND), either remaining sedentary (CON) or exercising (EX) post-HFM. Exercise was performed at the heart rate corresponding to 60% VO2peak on a treadmill one-hour post-HFM (63% fat, 10kcal/kgbw). Blood lipids and exhaled nitric oxide (eNO: marker of airway inflammation) were measured at baseline, 2 h and 4 h post-HFM. Sputum differential cell counts were performed at baseline and 4 h post-HFM.
Results
The mean eNO response for all groups increased at 2 h post-HFM (∼6%) and returned to baseline by 4 h (p=0.03). There was a time*COND interaction (p=0.04), where EX had a greater eNO response at 4 hours compared to CON. Sputum neutrophils increased at 4 hours post-HFM (p<0.05).
Conclusion
These findings suggest that airway inflammation occurs after a HFM when exercise is performed in the postprandial period, regardless of habitual activity level.
Keywords: energy balance, exercise, physical activity, inflammation, pulmonary physiology
Introduction
High-fat diets may lead to respiratory complications (Butler et al. 2006), as well as an increase in risk of developing asthma (GINA Executive and Science Committees, 2007). Even after a single high-fat meal (HFM), airway inflammation (measured via exhaled nitric oxide (eNO) (Rosenkranz et al. 2010; Johnson et al. 2015)) and sputum neutrophils increase in non-asthmatic individuals (Kurti et al. 2015). Researchers have also reported an increase in airway inflammation in asthmatic individuals (Wood et al. 2011). The increase in airway inflammation that occurs post-HFM may be due to mechanisms that are both toll-like receptor-4 (TLR4) independent and TLR4-dependent (Zhang et al. 2005; Teng et al. 2014). Previous research has shown that lipopolyssacharide (LPS) may increase TLR messenger RNA (mRNA) expression and lead to the increase in sputum neutrophils (Wood et al. 2011). However, there is also evidence that suggests that dietary fats may increase reactive oxygen species (ROS), leading to the upregulation of I-kappaB kinase beta and nuclear factor kappa-B (NFkB) (Kim and Sears 2010). These pathways converge on the inducible nitric oxide synthase (iNOS) pathway and may increase eNO (Gaston et al. 1994) post-HFM. The increase in eNO may also be reflective of eosinophilic airway inflammation, however changes in eNO and the percentage increase in eosinophils may not be strongly associated with each other in non-asthmatics (Berlyne et al. 2000). Therefore both LPS, as well as ROS may contribute to post-prandial airway inflammation.
Exercise is both a natural antioxidant and an anti-inflammatory agent, and an acute bout of physical activity may be a potential method for attenuating the post-prandial airway inflammatory response to a HFM. However, post-prandial HFM modifications in airway inflammation will likely be dependent on energy expenditure during and in response to the bout of physical activity, as well as the participant's chronic physical activity level. A single bout of exercise has been shown to reduce post-prandial lipemia (PPL) (Gill and Hardman 2003; Freese et al. 2014). However, results have been conflicting, likely because energy expenditure may need to be high in order to elicit reductions in lipemia. In a review written by Katsanos and Moffatt (2004), the authors estimated that between 600 and 700 kcals may need to be expended to produce an attenuated lipemic response. However, physically inactive individuals may achieve a reduction in lipemic response to a HFM with a smaller energy expenditure compared to physically active individuals (Katsanos and Moffatt 2004; Brandauer et al. 2013). In fact, an energy expenditure as minimal as 300 to 500 kilocalories may elicit a reduction in lipemia in inactive participants when performed without caloric replacement following the exercise bout (Murphy et al. 2000).
While an increase in lipemia has been reported to increase oxidative stress systemically (Tushuizen et al. 2006), physically trained individuals have increased antioxidant defenses to combat oxidative stress (Gomez-Cabrera et al. 2008). We recently reported that active, non-asthmatic individuals experience airway inflammation post-HFM, and an acute bout of exercise does not modify this response (Kurti et al. 2015; Johnson et al. 2015). However given that ROS can increase after a single HFM (Mohanty et al. 2002; Tushuizen et al. 2006) and may result in airway inflammation, individuals who are insufficiently active, with reduced antioxidant defenses, may have a greater magnitude of the cellular oxidative stress and inflammatory response to a HFM as compared to physically active individuals.
Therefore the current study sought to determine whether chronic PA modified the airway inflammatory response to an acute bout of exercise in the post-prandial period. We hypothesized that the reduction in airway inflammation after post-prandial exercise would be more apparent in insufficiently active participants (<150 minutes of moderate to vigorous PA per week)) compared to active (≥150 minutes of moderate to vigorous PA) participants.
Methods
Subjects
Forty participants between the ages of 18 and 45 were recruited for the study. Participants were separated by chronic physical activity level by guidelines in the Physical activity guidelines advisory committee report (2008). If participants were meeting or exceeding PA guidelines (acquiring greater than or equal to 150 minutes of moderate to vigorous PA/week), they were placed in the active group (ACT). If they were not, they were placed into the insufficiently active (IN) group. The amount of PA per week was determined by International Physical Activity Questionnaire (IPAQ) screening tool. Physically active participants (13M/7F: age: 24.3±5.5 years) and insufficiently active participants (6M/13F: age: 25.9±5.4 years) completed the study. There was one dropout due to dislike for the HFM and inability to complete the protocol in the time allotted for meal consumption. Prior to the study, all subjects completed a medical history questionnaire, ensuring they did not have any cardiovascular disease risk factors, were non-smokers and non-asthmatics. Subjects were excluded if they were taking any medications for heart or respiratory disease. Before the protocol was performed, subjects were briefed regarding the purpose of the study and written and verbal consent were obtained. The study was approved by the Institutional Review Board at Kansas State University and conformed to the ethical principles set forth in the Declaration of Helsinki.
Experimental Design
A pretest-posttest parallel groups design was utilized, and all participants visited the laboratory two times with one week in between sessions. The full experimental protocol has been previously published and is outlined here briefly (Kurti et al. 2015; Teeman et al. 2016).
Session 1: Initial measurements
During the initial visit, subjects completed the required paperwork including a medical history questionnaire and the international physical activity questionnaire (IPAQ). This questionnaire has been validated to assess PA by requiring subjects to recall their PA behavior for the previous seven days (Dinger et al. 2006). The PA is categorized into sedentary time, walking, moderate or vigorous activity each day and representative of a typical week of PA. Subjects then underwent initial measurements, including height, weight, dual X-ray absorptiometry (DEXA) scan and pulmonary function testing. Subjects then performed an incremental exercise test to exhaustion in order to determine peak aerobic capacity (VO2peak) as well as to identify the duration of the acute exercise bout if randomized into the exercise (EX) group. Following the exercise test, insufficiently active and physically active subjects were randomized into either the post-meal exercise condition (IN EX or ACT EX, respectively) or the no exercise condition, in which subjects remained sedentary in the post-meal period (IN CON or ACT CON).
Experimental measurements performed at session 1: Initial assessment
Anthropometrics
Anthropometrics were assessed according to standard guidelines. Height was measured to the nearest 0.1 cm with a portable stadiometer (Invictus Plastics, Leicaster, England) and weight was measured to the nearest 0.1 kg with a digital scale (Pelstar LLC, Alsip, IL, USA). A DEXA scan was then performed to assess body composition, including body fat percentage and lean mass (GE Lunar Prodigy, Madison, WI, USA).
Pulmonary function testing
Standardized pulmonary function tests, according to American Thoracic Society criteria, were performed to ensure that subjects were non-asthmatic and had normal pulmonary health (MIR Winspiro Pro, Waukesha, WI, USA). Subjects completed the standardized pulmonary function tests evaluated by the maximum flow volume loop (MFVL) (Miller et al. 2005). The MFVL assesses peak expiratory flow (PEF), forced vital capacity (FVC), forced expiratory volume in 1-s (FEV1), and forced expiratory flow at 25-75% of FVC (FEF25-75). The MFVL was performed until three attempts were within 10% of one another and the highest values derived from the MFVL were used for analyses. An acceptable MFVL was achieved if the subject refrained from coughing, refrained from hesitation, no extra breath was taken, did not inhale too early, there was no obstruction or leak in the mouthpiece, or the expiratory volume (FEV1) was <5% of the FVC or within 0.150, whichever was greater. Percent of predicted values were calculated according to reference values (Knudson et al. 1983).
Incremental test to exhaustion (peak aerobic oxygen consumption: VO2peak)
An incremental test to exhaustion was performed on a treadmill (Precor 932i) using a standardized protocol for establishing peak oxygen consumption (VO2peak) previously utilized in our laboratory (Kurti et al. 2015; Teeman et al. 2016). During the test, heart rate (HR) was monitored using a Polar WearLink Coded chest strap HR monitor, and rating of perceived exertion (RPE) was reported using a modified Borg scale (0-10) to assess effort at the end of each stage. Throughout the entire test, metabolic and ventilatory data were recorded by breath-by-breath analysis (Parvomedics TrueOne 2400 Metabolic Cart, Sandy, Utah). At the end of each stage and completion of the protocol, HR and VO2 data were recorded. Thirty seconds into each stage, RPE was recorded. The VO2peak test started at a 2% incline at the subjects perceived fastest 5k pace per mile. Every 2 minutes the speed increased by 0.5 miles per hour (mph), and increased 1% incline and 0.5 mph every two minutes following the third stage. The test was terminated when the subject could not maintain the speed and chose to stop the test. All subjects reported an RPE indicating they perceived their work to be very hard (greater than 7 on the 1-10 Borg scale), and achieved a HR at termination of the test that was within 10 beats per minute of their age-predicted maximum HR.
Session 2: High-fat meal testing session and exercise (EX) or no exercise (CON) post-prandially
Subjects visited the laboratory to pick up pre-packaged food the night prior to the HFM session. Subjects were required to consume only the pre-packaged food and to return any food that was not consumed prior to their HFM session. After a 12-hour overnight fast and 24 hours of abstaining from exercise, alcohol and caffeine, subjects visited the laboratory in the morning for the HFM session. Subjects first completed baseline (fasting) measures prior to consumption of the HFM. The fasting measurements included: airway inflammation and baseline blood draw, followed by the HFM. Subjects in the EX condition were required to perform an acute bout of exercise (energy expenditure equal to half of HFM caloric intake) one hour after the final bite of the HFM. The subjects exercised at the heart rate that corresponded to 60% of VO2peak to expend half of the calories from the HFM. Experimental measurements (airway inflammation, blood draw) were performed at two and four hours post-HFM. Sputum induction for confirmation of which inflammatory processes were involved, was successfully performed in a subset of subjects (n=21) at baseline and four hours post-HFM. All experimental measures are described below according to the session in which they were completed, and are displayed in figure 1.
Figure 1.
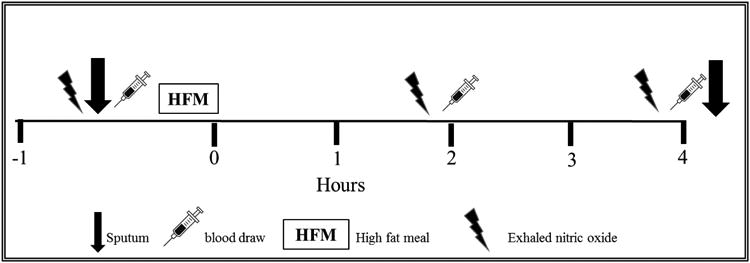
Schematic of the study.
Experimental measurements performed at session 2: High-Fat meal testing session
High-fat meal
Thirty-nine of the forty subjects initially recruited were able to finish the HFM testing session, with one dropout who did not finish the entire HFM protocol. The HFM consisted of a Jimmy Dean's Meat Lover's breakfast bowl (10kcal/kg/body weight: 63% fat, 15% carbohydrate). The nutritional make-up of the meal was 460 calories per bowl, 33 grams of fat, 13 grams of saturated fat, 265 milligrams of cholesterol, 17 grams of total carbohydrate and 24 grams of protein. Subjects had 20 minutes to consume the HFM, and time began from the first bite of the meal. Time for the session began at the last bite of the HFM. Energy consumed was determined according to subject body weight, and ranged from 450 to 1113 kcals. Calories from fat ranged from 280 to 700 fat kcals.
Exercise bout
One hour following the last bite of the HFM, the subjects randomized to the EX group completed at bout of treadmill exercise (a brisk walk on a moderate incline) at HR equal to 60% VO2peak to expend half of the calories they consumed from the HFM. Exercise time ranged from 25 to 70 minutes in participants randomized to the EX condition. The subject who exercised for more than one hour interrupted their exercise bout to perform the 2-hour blood draw, then completed their last 10 minutes of exercise.
Exhaled nitric oxide
The measurement of exhaled nitric oxide via chemiluminescence is a validated method for assessment of airway inflammation (Borland et al. 1993) (Sievers Nitric Oxide Analyzer 280, Sievers Instruments Inc, Boulder, CO, USA). Measurements were performed before the HFM, and at two hours and four hours post-meal. The test was performed according to American Thoracic Society guidelines (Kharitonov et al. 1997). Subjects were instructed to sit up straight with their feet flat on the floor without wearing a nose-clip. Subjects first performed a maximal inhalation, and then performed a steady exhalation that lasted approximately 6 seconds at a constant flow rate while data were recorded in real time. Testing was performed three times, with measurements within 5% of one another, and the average value was used for analysis. Exhaled nitric oxide data were positively skewed and required a square root transformation of the raw data prior to analysis.
Sputum induction, processing and analyses
Twenty-one of the thirty-nine subjects (53.8%) performed sputum induction to confirm which inflammatory process was involved in the post-prandial airway inflammatory response. Previous research has reported that an allergen-induced T-helper 2 (TH2) immune activation increases the influx of eosinophils into the airway, whereas a neutrophilic pattern is caused by an innate immune dysfunction (Gleich 2000; Simpson et al. 2006; Simpson et al. 2007). Therefore both eosinophils and neutrophils were measured in the subset of subjects that underwent sputum induction to confirm which inflammatory processes were involved. Hypertonic saline (5%) was administered using an ultrasonic nebulizer (Omron Healthcare, Lake Forest, IL, USA) with an aerodynamic diameter of 5μm and a 0.7 mL/min output. The same methods for sputum induction have been previous published in work from our laboratory (Kurti et al. 2015). The test was completed when a selective plug could be obtained, or was terminated if the subject was not able to expectorate within 30 minutes of breathing in the nebulized saline (Pin et al. 1992). Processing of sputum samples was completed within two hours of induction, and processing methods for these samples from our work have also been previously published (Kurti et al. 2015). Briefly, treatment of samples was performed with 0.1% dithiothreitol (DTT) in diluted water (4 times by weight) as well as phosphate-buffered saline (PBS). The typan blue exclusion method was performed to assess cell viability and counts were done on the hemacytometer. The remainder of the filtrate was resuspended, and then three cytospins (Shandon CytoSpin 2) were prepared with 100-150 μL sample at 500 rpm for 15 minutes. A modified Wright's stain (Harleco Hemacolor, Gibbstown, NJ) was used to stain slides, and all were then mounted with Permount (Fisher Scientific, Fairlawn, NJ). Salivary contamination was evaluated using methods published by Pizzichini et al. (1996). A second investigator blinded to condition performed sputum cell differentials, and differentials were performed as according to previously validated methods (Telenga et al. 2012; Kurti et al. 2015).
Blood sampling
An intravenous catheter was inserted into the antecubital vein and blood samples were drawn during fasting before the HFM, and at 2 hours and 4 hours post-meal. Blood samples were assessed for triglycerides. Triglycerides were significantly different at baseline between ACT and IN, and were not normally distributed. Triglycerides at baseline were added as a covariate and were log transformed prior to analysis. Methods for the assessment of triglycerides have been previously published (Kurti et al. 2015; Teeman et al. 2016). The current study was part of a larger study, and the purpose of the present study was to determine the airway inflammatory response post-HFM, therefore all blood lipid (other than triglycerides) and glucose values for these subjects can be found in Teeman et al. (2016) and are not reported here.
Statistical Analyses
Data were analyzed using SPSS Statistical Software v.23 (IBM, Armonk, NY). Descriptive data are expressed as mean±SD. All data were checked for normality using the Shapiro-Wilk test and to verify that parametric assumptions were met. Data were log10 transformed or transformed by computing the square root of the absolute values when parametric assumptions were not met. Three-way analyses of variance (within-subject factor= time: baseline, 2 hours, 4 hours) and (between-subjects factors =activity level (AL): active (ACT) or inactive (IN); condition (COND): no exercise (CON) or exercise (EX)) were performed. Interaction effects are included for AL*time, COND*time, and AL*COND*time for blood analytes and exhaled nitric oxide. Airway inflammation via sputum cell counts was assessed with a one-way analysis of covariance, using baseline neutrophils and eosinophils as the covariate, to identify which inflammatory processes were involved. To assess correlations between sputum cell counts and eNO, Pearson Product moment correlation coefficients were used. For all analyses, significance was set at p<0.05.
Results
Subject characteristics
Baseline subject characteristics are displayed in Table 1. There was significantly higher baseline blood pressure (p=0.04), heart rate (p<0.01), waist circumference (p=0.03), body fat percentage (p<0.01) and absolute (p<0.01) and relative VO2peak (p<0.01) in IN compared to ACT. The only significant difference in resting pulmonary function was a significantly lower FEV1 in IN participants compared to ACT participants. However FEV1 in both groups was still above 100% of age and height-predicted values. Also, FVC was smaller in IN compared to ACT. However IN participants were also significantly shorter (p=0.03), therefore differences in FEV1 were likely due to the fact that they had smaller lungs. All subjects had never been diagnosed with asthma, which they indicated on the medical history questionnaire and was confirmed via pulmonary function testing in which all subjects exhibited an FEV1/FVC of >70%.
Table 1. Subject Characteristics.
| ACTIVE (13M/7F) | INACTIVE (6M/13F) | sex difference (IN) | sex difference (ACT) | |
|---|---|---|---|---|
| Value SD | Value SD | (p-value) | (p-value) | |
| Age (years) | 24.3 ± 5.5 | 25.9 ± 5.4 | 0.07 | 0.66 |
| Height (cm) | 174.3 ± 9.5 | 167.7 ± 10.4* | <0.01˄ | <0.01˄ |
| Weight (kg) | 76.1 ± 14.2 | 74.1 ± 19.3 | 0.21 | <0.01˄ |
| Body mass index (BMI) (kg/m2) | 24.9 ± 2.8 | 26.3 ± 6.7 | 0.75 | 0.27 |
| Body Fat (%) | 20.5 ± 9.8 | 34.1 ± 11.5* | 0.02˄ | <0.01˄ |
| Waist circumference (cm) | 85.7 ± 5.4 | 92.9 ± 13.0* | 0.91 | 0.53 |
| Systolic (mmHg) | 119.3 ± 12.9 | 110.8 ± 11.1* | 0.05˄ | 0.08 |
| Diastolic (mmHg) | 67.3 ± 9.4 | 71.5 ± 8.7* | 0.56 | 0.52 |
| VO2peak (L/min) | 4.2 ± 1.0 | 2.9 ± 1.0* | <0.01˄ | <0.01˄ |
| VO2peak (ml/kg/min) | 54.5 ± 7.7 | 38.9 ± 9.5* | <0.01˄ | <0.01˄ |
| Resting Heart Rate (bpm) | 64 ± 10 | 75 ± 9.0* | 0.76 | 0.34 |
| Baseline Pulmonary Function Tests | ||||
| ACTIVE (13M/7F) | INACTIVE (6M/13F) | sex difference (IN) | sex difference (ACT) | |
| Value SD | Value SD | (p-value) | (p-value) | |
|
| ||||
| PEF (L/s) | 9.0 ± 2.7 | 7.7 ± 1.9 | <0.01˄ | <0.01˄ |
| FVC (L) | 5.5 ± 1.7 | 4.5 ± 2.0 | 0.01˄ | <0.01˄ |
| FEV1 (L) | 4.7 ± 1.4 | 3.7 ± 1.2* | 0.03˄ | <0.01˄ |
| FEV1/FVC (%) | 86.0 ± 5.9 | 86.3 ± 12.5 | 0.08 | 0.53 |
| FEF25-75% (L/s) | 5 ± 1.4 | 4.3 ± 1.4 | 0.24 | <0.01˄ |
Values are expressed as mean ± SD.
Significance difference between active (ACT) and inactive (IN) participants p<0.05
shows sex difference between males and females in ACT and IN groups
bpm, beats per minute; PEF, peak expiratory flow; FVC, forced vital capacity; FEV1, forced expiratory volume in 1-second
FEF25-75%, forced expiratory flow rates between 25-75% of FVC
Triglycerides
Data for triglycerides are displayed in Figure 2. Triglycerides significantly increased over time for ACT and IN subjects at 2 hour (61±48%) and were further increased at 4 hours post-HFM by (27±32%; p<0.001). The overall increase from baseline to four hours in ACT and IN was 100±76%. There were no significant differences based on AL (p=0.97) or COND (p=0.82). There were no significant interactions for time*AL (p=0.296), time*COND (p=0.74), or time*AL*COND (p=0.62).
Figure 2.

Triglyceride response post-HFM in ACT CON (●), ACT EX (○), IN CON (▼), IN EX (Δ). Data are shown as absolute means±SD. Triglycerides increased significantly from baseline to 2 hours and 4 hours, with no differences by activity level (AL) or condition (CON). Data points are offset to more clearly display the data. *Significant at p<0.05.
Energy Balance
Energy balance information is displayed in Table 2. There were no significant differences between ACT CON and IN CON based on energy consumed (p=0.70), energy balance at four hours (p=0.89), or caloric balance between food and exercise (p=0.19). However, for ACT EX as compared to IN EX, there was a significant difference in the minutes of exercise required to expend half of the calories of the HFM, where the IN EX walked longer than the ACT EX (d=1.61, p<0.01). In the IN EX compared with IN CON, the IN EX had significantly lower caloric balance after the HFM compared with IN CON (d=-1.40, p=0.01), however the amount of food consumed was not significantly different (p=0.98). In ACT EX compared with ACT CON, the exercising group had a greater energy deficit at 4 hours (d=-1.77, p<0.01) due to greater energy expenditure. The amount of food consumed was not significantly different between groups (p =0.68).
Table 2. Energy Balance.
| ACT CON | ACT EX | IN CON | IN EX | |
|---|---|---|---|---|
| Energy Consumed | 774.4 ± 164.6 | 747.5 ± 123.7 | 741.8 ± 199.3 | 739.3 ± 199.3 |
| Energy expended on treadmill | N/A ± N/A | 373.7 ± 61.9˄ | N/A ± N/A | 369.7 ± 99.6˄ |
| Caloric Balance (Food + EX) | 874.4 ± 395.7 | 373.7 ± 61.9˄ | 666.3 ± 282.6 | 369.7 ± 99.6˄ |
| Energy Balance at 4 hr | 458.7 ± 87.6 | 103.6 ± 43.5˄ | 466.3 ± 139.1 | 146.2 ± 72.93˄ |
| Exercise time (minutes) | N/A ± N/A | 32.1 ± 6.2*˄ | N/A ± N/A | 47.1 ± 11.6˄ |
All data are represented as kilocalories (kcals) unless otherwise noted.
p<0.05. Indicates significant difference between ACT CON and ACT EX, IN CON and IN EX
Denotes significance between ACT EX and IN EX or ACT CON and IN CON
Airway inflammation- eNO
Exhaled nitric oxide was our primary dependent variable; however, to determine which inflammatory processes were involved, sputum induction was performed in a subset of subjects. Not all subjects completed eNO testing due to technical difficulties with the flow sensor towards the end of the study, but the following completed eNO in each group: ACT CON, n=9; IN CON, n=9, ACT EX, n=7; IN EX, n=9. At baseline, eNO was not significantly different based on AL (p=0.77) or COND (p=0.77). However, eNO was significant as a quadratic function over time for all subjects (p=0.03), increasing at 2 hours and returning to baseline at 4 hours post meal. There was also a significant time*COND interaction (p=0.04), where the eNO response in EX compared to CON was different over the 4 hours, increasing in EX and remaining elevated, while it increased and returned to baseline in CON. There were no significant time*AL (p=0.37) or time*AL*COND (p=0.58) interactions. The mean eNO response in each cohort post-HFM is displayed in figure 3.
Figure 3.

The mean eNO response in ACT CON (●), ACT EX (○), IN CON (▼), IN EX (Δ). There was a significant increase as a main effect of time (*), where eNO increased from baseline to 2 hours and then started to return to baseline by 4 hours post-HFM. There was a higher eNO response over time by CON (˄). Data points are offset to more clearly display the data. *Significant at p<0.05.
Confirmatory tests-sputum induction
To assess the neutrophil response post-HFM, analyses were performed using the number of neutrophils at baseline as a covariate because the percentage change in neutrophils was impacted by the percentage present at baseline. The percentage of neutrophils increased significantly in the post-prandial period in a subset of 21 subjects who underwent sputum induction. The mean increase in neutrophils was 10.9±4.5% (95% CI: 1.5-20.4%). The study was not powered to detect differences in neutrophils and eosinophils for each group, given the small sample available (IN CON, n=6; ACT CON, n=5; IN EX, n=4; ACT EX, n=6). When performing a post-hoc sample size calculation, we found a moderate effect for the increase in neutrophils by COND alone (d=0.44), and 8 subjects in each group would be needed to show a significant increase in neutrophils in the walking condition compared to the no walking condition. By AL alone, there was a small to moderate effect (d=0.36) and 12 subjects would be needed in each group to show an increase in neutrophils in ACT compared to IN subjects.
The ACT CON and ACT EX data, however, have been previously published as the main outcome in a preliminary study from our laboratory (Kurti et al. 2015). Eosinophils were also assessed post-HFM to determine which inflammatory processes were involved. Eosinophils did not significantly increase from baseline (0.5±0.5%) to four hours (0.5±0.6%) post-HFM (p=0.89). Percent change from baseline to 4 hours post-HFM was not significant (0.0±0.9%; 95% CI: -0.4-0.4%).
Associations between airway inflammation and eNO
To assess associations between markers of airway inflammation, bivariate correlations were performed. Eighteen of twenty-one subjects that performed sputum induction also had performed eNO at all time points. The percentage change in neutrophils from baseline was not associated with the percentage change in eNO from baseline to 2 hours (r=0.36, p=0.16) or baseline to four hours (r=0.26, p=0.31). The percentage change in eosinophils was also not associated with the percentage change in eNO from baseline to 2 hours (r=-0.03, p=0.92), or baseline to 4 hours (r=-0.12, p=0.65). The percentage change in neutrophils was not associated with the change in eosinophils from baseline to 4 hours (r=0.09, p=0.70).
Discussion
Main findings
The major finding in this study was that physically active and insufficiently active participants in the walking condition had a larger eNO response compared with the no walking condition. This finding was in contrast to our hypothesis that IN subjects would have a greater attenuation in post-prandial eNO compared to CON. There may be many factors contributing to the lipemic and airway inflammatory response post-exercise and post-meal, many of which may interact with one another, therefore these factors will be the focus of our discussion.
Airway inflammation post-HFM
In many of our previous studies, as well as the current study, eNO significantly increased as a main effect of time after a high-fat meal (Rosenkranz et al. 2010; Ade et al. 2014; Johnson et al. 2015). We have previously shown that eNO increases post-prandially from baseline to 2 hours with a subsequent return to baseline by 4 hours post-HFM (Kurti el al. 2015, Johnson et al. 2015). Wood et al. (2011) showed that at 4-hours post-HFM in non-asthmatic subjects, there was not an increase in eNO, but there was a 15.3±6.2% increase in neutrophils. Wood and colleagues did not measure eNO at 2 hours, and therefore at 4 hours post-meal eNO may have started to return to baseline values. The difference in time course for changes in eNO and neutrophils may be why there are not significant associations between markers of airway inflammation in Wood and colleagues work as well as the present study. Additionally, the change in eNO was not associated with changes in eosinophils. The airway inflammatory response in neutrophils, eosinophils, and eNO indicated independence of the responses of these markers of airway inflammation. Therefore, it is possible that the increase in eNO is not only due to inflammatory processes, but may suggest that oxidative processes are involved, where eNO is increased because there is a reduced clearance in NO systemically. The competition of antioxidant enzymes following a HFM may inhibit the reduction of NO production, leading to an increase in exhaled NO due to the attenuation or absence of an increase in iNOS activity (Bonini et al. 2014).
We are confident that oxidative stress and inflammatory processes were involved in the eNO response following a HFM. Possible mechanisms contributing to the eNO response may be either TLR4 dependent or independent. Wood and colleagues showed that 4 hours post-HFM, expression of TLR4 mRNA significantly increases via a NFkB-driven cascade (Wood et al. 2011). However the increase in exhaled NO may also occur due to the direct upregulation of iNOS in the airways (Gaston et al. 1994). For example, in rats injected with lipopolyssaccharide (LPS), iNOS expression has been shown to increase (Sugita et al. 2002). Dietary fats also increase reactive oxygen species (ROS), which may increase neutrophils in the airway. Dietary fats increase NFkB and I-kappaB kinase beta (Ricciardolo et al. 2004), upregulating iNOS and contributing to the increase in exhaled NO (Gaston et al. 1994).
Impact of physical activity level of post-prandial airway inflammation
Basal eNO in asthmatics can be lowered by physical activity interventions (Mendes et al. 2011). Additionally, a recent study by Scott et al. (2015) indicated that even an acute bout of physical activity lowers eNO in insufficiently active asthmatics, suggesting that an acute bout of exercise may attenuate increases in eNO in insufficiently active non-asthmatic individuals. However in the current study, we did not find differences based on activity level (active or insufficiently active), but did find differences based on whether subjects exercised or remained sedentary (EX or CON) in the post-prandial period. Given that all of our subjects were non-asthmatic, the post-prandial eNO response following a HFM was unexpected.
Researchers have reported that physically active and trained subjects have greater antioxidant defenses with which to combat ROS (Gomez-Cabrera et al. 2008). Reactive oxygen species increase post-HFM (Mohanty et al. 2002), therefore we hypothesized that active individuals with a greater antioxidant status would have an attenuated airway inflammatory response, due to the ability to clear ROS produced and lead to less activation of iNOS. Stewart and colleagues showed that active individuals have an attenuated inflammatory response when injected with LPS systemically, and this is likely due to lower activation of TLR4 (Stewart et al. 2005). The active individuals in our study did not display an attenuation of the eNO response post-HFM, and therefore it is possible that there was not a reduction in ROS due to chronic PA level. It is also possible the insufficiently active participants had lower oxidative stress because they were young; since it has been shown that younger individuals have lower oxidative stress compared to older individuals (Cadenas and Davies 2000). Therefore measuring the airway inflammatory response after performing post-prandial exercise may be an important topic to investigate in an aging population.
While chronic effects of training did not reduce post-prandial airway inflammation in the present study, there were acute effects on airway inflammation and cellular stress after the bout of exercise. The participants were walking to expend half the calories of the HFM, and it is possible that sheer rate via increases in ventilation could have increased activation of NO isoforms (Sheel and McKenzie 1999). However, eNO typically decreases immediately after exercise when ventilation is higher (Mehta et al. 1997). It is possible the IN EX subjects had a more reduced eNO response than the ACT EX subjects because they had higher ventilation during the exercise bout at 60% VO2peak, and exercised longer, which they were not accustomed to. The mechanisms contributing to airway inflammatory and oxidative processes during and after an acute bout of exercise should be explored further, and specifically researchers should determine the origin of eNO at different intensities to better understand the post-prandial and post-exercise responses.
Exercise: acute or chronic, and post-prandial lipemia
Chronic physical activity has been shown to result in lower triglycerides after a high-fat meal (Merrill et al. 1989) compared to low physical activity levels, and this has been confirmed in many other studies (Hardman and Aldred 1995; Katsanos and Moffatt 2004). However the impact of an acute bout of physical activity on PPL is somewhat unclear. We recruited two cohorts of subjects (IN and ACT) because the reduction in PPL is likely to be dependent on chronic activity level. The fact that there was not a reduction in PPL in either group, further contributes to a large body of conflicting literature. Several systematic reviews suggest that higher energy expenditures are required to see reductions in PPL (Katsanos and Moffatt 2004), and more than what individuals may realistically perform following a high-fat meal. The bout of physical activity utilized in our study represented a more true-to-life exercise bout (a brisk walk), that an individual may perform one hour after consuming a HFM. In light of recent studies, we believed the bout would lead to a reduction in PPL, particularly in the insufficiently active group. The average energy expenditure in the EX group was approximately 370 kcal. This level of energy expenditure has recently been shown to reduce PPL in sedentary overweight men (Chu et al. 2016). In fact, the researchers report that exercise duration of only 20 minutes at 60% power elicited a 20% reduction in PPL. Interestingly, subjects in the study performed by Chu and colleagues had a higher VO2max (40.4 ±8.6 mL/kg/min) and lower body fat percentage (19.0 ±5.3%) compared to participants in the present study. Gabriel and colleagues (2012) found a trend for reductions in PPL after an exercise energy expenditure of 103.2±5.1 kcals during a high-intensity interval trial, and subjects were recreationally active but not endurance trained. Conversely, active participants may need as much as 600 to 700 kilocalories of energy expenditure to see a reduction in PPL. We previously reported that this group of active subjects did not have a reduction in PPL following acute exercise (Kurti et al. 2015), and it is possible that the insufficiently active subjects in the current study engaged in more PA as compared to previous studies where a relatively low exercise energy expenditure elicited a reduced lipemic response. Most of our subjects were living on a college campus, and therefore even the short amount of time that they walk to and from class may be sufficient to have beneficial training adaptations. Subjects in our study reported getting only 29±41 minutes of moderate to vigorous activity over 7 days, which is lower than the ACSM guidelines. Nonetheless, insufficiently active subjects reported walking for 220±280 minutes per week, which may be enough to show beneficial training adaptations with regard to post-prandial responses to a HFM.
Limitations
There are several factors that may have influenced our results. Given that active individuals have an increased antioxidant capacity compared to insufficiently active individuals, antioxidant status should be considered. If the antioxidant status of subjects was not different at baseline and eNO may be reflective of oxidative and inflammatory processes, total antioxidant status and/or capacity may account for the eNO responses seen in the current study. We have previously shown that increasing fruit and vegetable consumption (Chenoweth et al. 2015) or vitamin supplementation (Kurti et al. 2015), which likely improves total antioxidant capacity, improves post-exercise lung-function. Therefore measurement of antioxidant capacity in our subjects would allow for further exploration of potential mechanisms from our current results. Additionally, it would have been ideal to perform sputum analysis in all of the subjects enrolled to determine differences by activity level and condition. Considering our study was intended to determine whether chronic PA level modified the post-prandial eNO response, detecting differences in sputum cell differentials by AL and COND was not a primary aim. Still, additional information on inflammatory cell presence by chronic PA level and condition would be ideal and will be included in future studies. It would have also been useful to assess airway hyper-responsiveness after sputum induction, however this was not possible in our protocol. We have previously found 25% hypertonic saline was used to elicit airway hyper-responsiveness in healthy non-asthmatic subjects (Smith et al. 2015), while a lower hypertonic saline concentration (5%) has not been shown to be effective in eliciting airway hyper-responsiveness in this population. Lastly, the triglyceride levels of our subjects were low, and even the inactive individuals did not have a large magnitude of increase in the post-prandial period. Therefore, the low levels of triglycerides in our subject pool may have prevented a further attenuation of lipemia, particularly considering the fact that triglycerides didn't increase above 150 mg/dL post-prandially.
Future research
Future research should elucidate the mechanisms contributing to the post-prandial increase in eNO. Given that several inflammatory and oxidative stress pathways may contribute to the effects of both a HFM and a bout of exercise on the airways in the post-prandial period, investigating longer or more intense bouts of exercise, and utilizing different timing around the meal is important in future research. Also, the modification of the postprandial airway inflammatory response should be investigated in populations such as obese individuals or asthmatics. Researchers should focus on determining what happens to the airway inflammatory response post-HFM in these individuals when a reduction in PPL is evident.
Conclusions
Results from the current study indicate that an acute bout of moderate intensity exercise following a HFM does not affect PPL in either insufficiently active or active non-asthmatics, but does impact the airway inflammatory response. In individuals who are chronically physically active, eNO increases when exercise is performed post-prandially compared to those not engaging in physical activity in the post-prandial period. Additionally, results from this study suggest that mechanisms contributing to post-prandial airway inflammation are independent, with no associations between the eNO, neutrophilic and eosinophilic responses following a HFM.
Acknowledgments
We thank all the participants that completed this study. The work was funded by SK Rosenkranz University Small Research Grant (USRG) and SK Chapes laboratory funding from NASA grants NNX13AN34G and NNX15AB45G and NIH grant GM103418.
Footnotes
Authors report no conflicts of interest associated with this manuscript.
References
- Ade CJ, Rosenkranz SK, Harms CA. The effects of short-term fish oil supplementation on pulmonary function and airway inflammation following a high-fat meal. Eur J Appl Physiol. 2014;114(4):675–682. doi: 10.1007/s00421-013-2792-7. [DOI] [PubMed] [Google Scholar]
- Berlyne GS, Parameswaran K, Kamada D, Efthimiadis A, Hargreave FE. A comparison of exhaled nitric oxide and induced sputum as markers of airway inflammation. J Allergy Clin Immunol. 2000;106(4):638–644. doi: 10.1067/mai.2000.109622. [DOI] [PubMed] [Google Scholar]
- Bonini MG, Dull RO, Minshall RD. In Systems Biology of Free Radicals and Antioxidants. Springer Berlin; Heidelberg: 2014. Caveolin-1 Regulation of Endothelial Nitric Oxide Synthase (eNOS) Function and Oxidative Stress in the Endothelium; pp. 1343–1363. [Google Scholar]
- Borland C, Cox Y, Higenbottam T. Measurement of exhaled nitric oxide in man. Thorax. 1993;48(11):1160–1162. doi: 10.1136/thx.48.11.1160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brandauer J, Landers-Ramos RQ, Jenkins NT, Spangenburg EE, Hagberg JM, Prior SJ. Effects of prior acute exercise on circulating cytokine concentration responses to a high-fat meal. Physiol Rep. 2013;1(3):e00040. doi: 10.1002/phy2.40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Butler LM, Koh WP, Lee HP, Tseng M, Yu MC, London SJ. Prospective study of dietary patterns and persistent cough with phlegm among Chinese Singaporeans. Am J Respir Crit Care Med. 2006;173(3):264–270. doi: 10.1164/rccm.200506-901OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cadenas E, Davies KJ. Mitochondrial free radical generation, oxidative stress, and aging. Free Rad Biol, Med. 2000;29(3):222–230. doi: 10.1016/s0891-5849(00)00317-8. [DOI] [PubMed] [Google Scholar]
- Chenoweth LM, Smith JR, Ferguson CS, Downey AE, Harms CA. The effects of antioxidant vitamin supplementation on expiratory flow rates at rest and during exercise. Eur J Appl Physiol. 2015;115(10):2049–2058. doi: 10.1007/s00421-015-3183-z. [DOI] [PubMed] [Google Scholar]
- Chu A, Boutcher YN, Boutcher SH. Effect of acute interval sprinting exercise on postprandial lipemia of sedentary young men. J Exerc Nutr Biochem. 2016;20(1):9–14. doi: 10.20463/jenb.2016.03.20.1.7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dinger M, Behrens T, Hans J. Validity and reliability on the international physical activity questionnaire in college students. Am J Health Educ. 2006;37:337–43. [Google Scholar]
- Freese EC, Gist NH, Cureton KJ. Effect of prior exercise on postprandial lipemia: an updated quantitative review. J Appl Physiol. 2014;116(1):67–75. doi: 10.1152/japplphysiol.00623.2013. [DOI] [PubMed] [Google Scholar]
- Gabriel B, Ratkevicius A, Gray P, Frenneaux MP, Gray SR. High-intensity exercise attenuates postprandial lipaemia and markers of oxidative stress. Clinical science. 2012;123(5):313–321.43. doi: 10.1042/CS20110600. [DOI] [PubMed] [Google Scholar]
- Gaston B, Drazen JM, Loscalzo J, Stamler JS. The biology of nitrogen oxides in the airways. Amer J Respir Crit Care Med. 1994;149(2):538–551. doi: 10.1164/ajrccm.149.2.7508323. [DOI] [PubMed] [Google Scholar]
- Gill JM, Hardman AE. Exercise and postprandial lipid metabolism: an update on potential mechanisms and interactions with high carbohydrate diets (review) J Nutr Biochem. 2003;14(3):122–132. doi: 10.1016/S0955-2863(02)00275-9. [DOI] [PubMed] [Google Scholar]
- GINA Executive and Science Committees. GINA Report, Global Strategy for Asthma Management and Prevention. [accessed August 2008];2007 www.ginasthma.org.
- Gleich GJ. Mechanisms of eosinophil-associated inflammation. J Allergy Clin Immunol. 2000;105(4):651–663. doi: 10.1067/mai.2000.105712. [DOI] [PubMed] [Google Scholar]
- Gomez-Cabrera MC, Domenech E, Viña J. Moderate exercise is an antioxidant: upregulation of antioxidant genes by training. Free Rad Biol Med. 2008;44(2):126–131. doi: 10.1016/j.freeradbiomed.2007.02.001. [DOI] [PubMed] [Google Scholar]
- Hardman AE, Aldred HE. Walking during the postprandial period decreases alimentary lipaemia. J Cardiovasc Risk. 1995;2:71–78. [PubMed] [Google Scholar]
- Johnson AM, Kurti SP, Smith JR, Rosenkranz SK, Harms CA. Effects of an acute bout of moderate intensity exercise on postprandial lipemia and airway inflammation. Appl Physiol Nutr Metabol. 2015;41(3):284–291. doi: 10.1139/apnm-2015-0314. [DOI] [PubMed] [Google Scholar]
- Katsanos CS, Moffatt RJ. Acute effects of premeal versus postmeal exercise on postprandial hypertriglyceridemia. Clin J Sport Med. 2004;14(1):33–39. doi: 10.1097/00042752-200401000-00006. [DOI] [PubMed] [Google Scholar]
- Kharitonov S, Alving K, Barnes PJ. Exhaled and nasal nitric oxide measurements: recommendations. ERS Task Force Report Eur Respir J. 1997;10:1683. doi: 10.1183/09031936.97.10071683. [DOI] [PubMed] [Google Scholar]
- Kim JJ, Sears DD. TLR4 and insulin resistance. Gastroenterol Res Pract. 2010;2010:212563. doi: 10.1155/2010/212563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knudson RJ, Lebowitz MD, Holberg CJ, Burrows B. Changes in the Normal Maximal Expiratory Flow-Volume Curve with Growth and Aging 1–3. Amer Rev Respir Dis. 1983;127(6):725–734. doi: 10.1164/arrd.1983.127.6.725. [DOI] [PubMed] [Google Scholar]
- Kurti SP, Rosenkranz SK, Levitt M, Cull BJ, Teeman CS, Emerson SR, Harms CA. Does moderate intensity exercise attenuate the postprandial lipemic and airway inflammatory response to a high-fat meal? BioMed research international. 2015 doi: 10.1155/2015/647952. Article ID: 647952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mehta S, Magder S, Levy RD. The effects of changes in ventilation and cardiac output on expired nitric oxide. Chest. 1997;111(4):1045–1049. doi: 10.1378/chest.111.4.1045. [DOI] [PubMed] [Google Scholar]
- Mendes FA, Almeida FM, Cukier A, Stelmach R, Jacob-Filho W, Martins MA, Carvalho CR. Effects of aerobic training on airway inflammation in asthmatic patients. Med Sci Sports Exerc. 2011;43(2):197–203. doi: 10.1249/MSS.0b013e3181ed0ea3. [DOI] [PubMed] [Google Scholar]
- Merrill JR, Holly RG, Anderson RL, Rifai N, King ME, DeMeersman R. Hyperlipemic response of young trained and untrained men after a high fat meal. Arteriosclerosis, Thrombosis, Vasc Biol. 1989;9(2):217–223. doi: 10.1161/01.atv.9.2.217. [DOI] [PubMed] [Google Scholar]
- Mohanty P, Ghanim H, Hamouda W, Aljada A, Garg R, Dandona P. Both lipid and protein intakes stimulate increased generation of reactive oxygen species by polymorphonuclear leukocytes and mononuclear cells. Amer J Clin Nutr. 2002;75(4):767–72. doi: 10.1093/ajcn/75.4.767. [DOI] [PubMed] [Google Scholar]
- Murphy MH, Nevill AM, Hardman AE. Different patterns of brisk walking are equally effective in decreasing postprandial lipaemia. Int J Obes Relat Metab Disord. 2000;24:1303–9. doi: 10.1038/sj.ijo.0801399. [DOI] [PubMed] [Google Scholar]
- Physical Activity Guidelines Advisory Committee. Physical activity guidelines advisory committee report, 2008. Vol. 2008. Washington, DC: US Department of Health and Human Services; 2008. pp. A1–H14. [Google Scholar]
- Pin I, Gibson PG, Kolendowicz R, Girgis-Garbardo A, Denburg JA, Hargreave FE, et al. Use of induced sputum cell counts to investigate airway inflammation in asthma. Thorax. 1992;47(1):25–29. doi: 10.1136/thx.47.1.25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pizzichini E, Pizzichini MMM, Efthimiadis A, Evans S, Morris MM, Squillace D, et al. Indices of airway inflammation in induced sputum: reproducibility and validity of cell and fluid-phase measurements. Amer J Respir Crit Care Med. 1996;154(2):308–317. doi: 10.1164/ajrccm.154.2.8756799. [DOI] [PubMed] [Google Scholar]
- Ricciardolo FL, Sterk PJ, Gaston B, Folkerts G. Nitric oxide in health and disease of the respiratory system. Physiol Rev. 2004;84(3):731–765. doi: 10.1152/physrev.00034.2003. [DOI] [PubMed] [Google Scholar]
- Rosenkranz SK, Townsend DK, Steffens SE, Harms CA. Effects of a high-fat meal on pulmonary function in healthy subjects. Eur J Appl Physiol. 2010;109(3):499–506. doi: 10.1007/s00421-010-1390-1. [DOI] [PubMed] [Google Scholar]
- Scott HA, Latham JR, Callister R, Pretto JJ, Baines K, Saltos N, et al. Acute exercise is associated with reduced exhaled nitric oxide in physically inactive adults with asthma. Annals Allergy Asthma Immunol. 2015;114(6):470–479. doi: 10.1016/j.anai.2015.04.002. [DOI] [PubMed] [Google Scholar]
- Sheel AW, McKenzie DC. Exhaled nitric oxide during exercise. Sports Med. 1999;28(2):83–90. doi: 10.2165/00007256-199928020-00003. [DOI] [PubMed] [Google Scholar]
- Simpson JL, Grissell TV, Douwes J, Scott RJ, Boyle MJ, Gibson PG. Innate immune activation in neutrophilic asthma and bronchiectasis. Thorax. 2007;62(3):211–218. doi: 10.1136/thx.2006.061358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simpson JL, Scott RJ, Boyle MJ, Gibson PG. Inflammatory subtypes in asthma: assessment and identification using induced sputum. Respirology. 2006;11:54–61. doi: 10.1111/j.1440-1843.2006.00784.x. [DOI] [PubMed] [Google Scholar]
- Smith JR, Kurti SP, Johnson AM, Kolmer SA, Harms CA. Impact of varying physical activity levels on airway sensitivity and bronchodilation in healthy humans. Appl Physiol Nutr Metab. 2015;40(12):1287–1293. doi: 10.1139/apnm-2015-0185. [DOI] [PubMed] [Google Scholar]
- Stewart LK, Flynn MG, Campbell WW, Craig BA, Robinson JP, McFarlin BK, et al. Influence of exercise training and age on CD14+ cell-surface expression of toll-like receptor 2 and 4. Brain, behavior, Immunity. 2005;19(5):389–397. doi: 10.1016/j.bbi.2005.04.003. [DOI] [PubMed] [Google Scholar]
- Sugita H, Kaneki M, Tokunaga E, Sugita M, Koike C, Yasuhara S, et al. Inducible nitric oxide synthase plays a role in LPS-induced hyperglycemia and insulin resistance. Amer J Physiol, Endocrinol, Metab. 2002;282(2):E386–E394. doi: 10.1152/ajpendo.00087.2001. [DOI] [PubMed] [Google Scholar]
- Teeman CS, Kurti SP, Cull BJ, Emerson SR, Haub MD, Rosenkranz SK. The effect of moderate intensity exercise in the postprandial period on the inflammatory response to a high-fat meal: an experimental study. Nutrition J. 2016;15(1):1. doi: 10.1186/s12937-016-0134-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Teng KT, Chang CY, Chang LF, Nesaretnam K. Modulation of obesity-induced inflammation by dietary fats: mechanisms and clinical evidence. Nutrition J. 2014;13(1):1. doi: 10.1186/1475-2891-13-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tushuizen ME, Nieuwland R, Scheffer PG, Sturk A, Heine RJ, Diamant M. Two consecutive high-fat meals affect endothelial-dependent vasodilation, oxidative stress and cellular microparticles in healthy men. J Thromb, Haemost. 2006;4:1003–1010. doi: 10.1111/j.1538-7836.2006.01914.x. [DOI] [PubMed] [Google Scholar]
- Telenga ED, Tideman SW, Kerstjens HAM, ten Hacken NHT, Timens W, Postma DS, et al. Obesity in asthma: more neutrophilic inflammation as a possible explanation for a reduced treatment response. Allergy: Eur J Allergy Clin Immunol. 2012;67(8):1060–1068. doi: 10.1111/j.1398-9995.2012.02855.x. [DOI] [PubMed] [Google Scholar]
- Wood LG, Garg ML, Gibson PG. A high-fat challenge increases airway inflammation and impairs bronchodilator recovery in asthma. J Allergy Clin Immunol. 2011;127(5):1133–1140. doi: 10.1016/j.jaci.2011.01.036. [DOI] [PubMed] [Google Scholar]
- Zhang X, Dong F, Ren J, Driscoll MJ, Culver B. High dietary fat induces NADPH oxidase-associated oxidative stress and inflammation in rat cerebral cortex. Exp Neurol. 2005;191(2):318–325. doi: 10.1016/j.expneurol.2004.10.011. [DOI] [PubMed] [Google Scholar]