

Abstract
Background and Purpose
Best practice recommendations indicate aerobic exercise (AEX) should be incorporated into stroke rehabilitation. However, this may be challenging in clinical settings. The purpose of this study was to assess physical therapist (PT) AEX prescription for patients with stroke, including AEX utilization, barriers to AEX prescription, dosing parameters and safety considerations.
Methods
A cross-sectional web-based survey study was conducted. PTs with valid email addresses on file with the state boards of Florida, New Jersey, Ohio, Texas and Wyoming were eligible to participate. Survey invitations were emailed to all licensed PT in these states. Analysis focused on respondents who were currently involved with clinical stroke rehabilitation in common practice settings.
Results
Results from 568 respondents were analyzed. Most respondents (88%) agreed that AEX should be incorporated into stroke rehabilitation, but 84% perceived at least one barrier. Median prescribed AEX volume varied between practice settings from 20 to 30 minute AEX sessions, 3 to 5 days per week for 2 to 8 weeks. Prescribed intensity was most commonly light or moderate; intensity was determined by the general response to AEX and patient feedback. Only 2% of respondents reported that the majority of their patients with stroke had stress tests.
Discussion and Conclusions
Most United States PTs appear to recognize the importance of AEX for persons post stroke, but clinical implementation can be challenging. Future studies and consensus are needed to clarify best practices and to develop implementation interventions to optimize AEX utilization in stroke rehabilitation.
Keywords: cardiovascular, cardiorespiratory, endurance, aerobic, walking
Introduction
Cardiovascular deconditioning is common after stroke and has negative implications for stroke recovery,1,2 participation in normal daily activities,1,3 and risk for cardiac events4,5 and recurrent stroke.6,7 To address post-stroke deconditioning, the American Heart Association (AHA) recommends that aerobic exercise (AEX) should be a fundamental component of stroke rehabilitation.8 The recommended intensity of AEX is 40-70% of oxygen uptake (VO2) or heart rate (HR) reserve, 55-80% of HR max, or 11-14 on the 6-20 scale for rating of perceived exertion.8 The recommended duration and frequency of AEX are 20-60 minutes, 3-5 days/week and the recommended mode is treadmill walking, whenever feasible.8 With 3-6 months of such AEX, persons with stroke have achieved significant improvements in aerobic capacity,9-12 gait endurance,9,12 self-reported general mobility,9 cardiovascular risk factors,10,13 blood flow (peripheral14 and cerebral15), brain activation12 and cognition.16 AEX has also been associated with significant improvements in lower extremity power17 and spasticity17 after stroke.
While AEX is not risk-free, the benefits are considered to outweigh the potential risks for the majority of people, including those who have had a stroke.8 However, 20-40% of persons post stroke have been found to have signs of silent myocardial ischemia during exercise and hypertension is a common comorbidity in this population.5,8 Therefore, it is recommended that exercise stress testing with electrocardiographic (ECG) and blood pressure (BP) monitoring should be part of a baseline pre-exercise medical evaluation whenever possible.8 When ECG stress testing is not feasible, continuous ECG monitoring during AEX or lower intensity AEX have been suggested as alternative options.8
Although these recommendations have been in place since 2004,18 small observational studies19-21 and a recent survey of Canadian physical therapists (PTs)22 indicate that adherence may be challenging in clinical stroke rehabilitation practice. However, no previous studies have evaluated post-stroke AEX prescription among PTs in the United States (U.S.) healthcare system. Therefore, the purpose of this study was to assess AEX prescription for individuals post stroke by U.S. PTs currently involved in clinical stroke rehabilitation, including AEX utilization, barriers to AEX prescription, dosing parameters and safety considerations.
Methods
Study Design
A cross-sectional web-based survey study was conducted. This study was approved by the University of Cincinnati Institutional Review Board. The survey instrument was developed using expert review and a PT focus group, including PTs from a variety of practice settings. Email address listings were obtained from state PT licensing boards in states where such listings were publicly available at no cost. This included Florida, New Jersey, Ohio, Texas and Wyoming. Survey invitations were then sent to all licensed PTs with email addresses on file in these states. Survey response analysis included all licensees with valid email addresses and all respondents. Eligibility criteria for the remaining analyses were: 1) currently involved in direct clinical patient care; 2) evaluated or treated at least one patient for stroke rehabilitation within the past 3 months; and 3) primary practice setting of acute care, home health, inpatient rehabilitation, extended care (skilled nursing or assisted living facility) or outpatient rehabilitation (not school, academic/research or ‘other’).
Survey Instrument
A draft survey instrument was developed by adapting a previous questionnaire used to assess AEX prescription in neurological rehabilitation among Canadian PTs.22 The draft instrument was reviewed by the study team and an additional expert in post stroke AEX (Ada Tang PT, PhD). After revisions, a clinical PT focus group was conducted to pilot test the survey and to provide additional feedback to further refine the instrument. The focus group included 6 PTs currently practicing in a variety of settings, including acute care, inpatient rehabilitation, extended care, home health and outpatient rehabilitation. All focus group participants had been in practice for at least one year and provided written informed consent prior to participation. Participants were asked to provide feedback on all aspects of the survey, including the invitation to participate, overall organization, wording, redundant questions, important missing content and length.
The final survey instrument contained 30 closed-ended questions with either a list of response choices (categorical variables) or a field for numerical data entry (continuous variables; see Appendix, Supplemental Digital Content 2, for complete survey instrument). There were 8 questions regarding respondent characteristics, 10 regarding AEX utilization and barriers, 5 regarding dosing parameters and 7 regarding safety considerations. The survey was adaptive based on the responses to filtering questions. For example, the survey only asked questions about AEX prescription for individuals with stroke if the respondent indicated that they had evaluated or treated at least one patient for stroke rehabilitation within the past 3 months. The survey was written at a Flesch-Kincaid grade level23 of 11.1 and took approximately 15 to 20 minutes to complete.
Survey Deployment
Survey deployment and data management were performed through the REDCap web-based system.24 After pilot testing of the survey deployment system by the study team, email invitations to complete the survey were sent to non-duplicate, valid email addresses of actively licensed PTs on file with the state licensing boards of Florida, New Jersey, Ohio, Texas and Wyoming. The invitation explained the purpose of the survey, stated that individual responses would be confidential, provided the primary author's contact information and contained a link to additional information about the study, including voluntary consent statements (see Appendix, Supplemental Digital Content 3, for example email invitation). Each invitation contained a unique link to the survey to allow response tracking and prevent respondents from completing the survey multiple times. Several tactics were used as an attempt to increase the response rate22,25: 1) email invitations were scheduled to deploy before 9 AM; 2) the invitation informed participants that they would be able to see some of the preliminary results after survey completion; 3) a page counter made participants aware of their progress in completing the survey; 4) respondents could save the survey and return to it later; 5) up to two follow up emails were sent to non-respondents in 2 to 3 week intervals; and 6) the survey was available for 3 months for each potential respondent and was open from 7/31/14 to 11/12/14.
Statistical Analysis
For categorical variables, percentages were calculated by dividing the frequency of a particular response by the total number of responses for that item. Continuous variables were described by mean (standard deviation) when normally distributed and median (interquartile range) when non-normally distributed (i.e. significant Kolmogorov-Smirnov test).
To assess for non-response bias, the number of years licensed was calculated from state board data and compared between respondents and non-respondents using the non-parametric Wilcoxon rank-sum test. If a significant difference in years licensed was found between respondents and non-respondents, we planned to do a sensitivity analysis to assess the potential extent of non-response bias. This analysis would compare the AEX utilization responses between the underrepresented subgroup and the full sample used for analysis. The magnitude of the differences between the subgroup and the full sample would be used to estimate the amount of non-response bias.
To determine whether to report results separately for different practice settings, we tested for statistical differences in responses between respondents with different primary practice settings. This analysis was performed for each question. Chi-squared tests were used for categorical variables and Kruskal-Wallis tests were used for continuous variables, because they were not normally distributed. When significant (p<0.05) differences between practice settings were found for an item, pairwise comparisons were obtained using Bonferroni adjustment for multiple comparisons. The Benjamini-Hochberg procedure26 was additionally used to control the false discovery rate for multiple response variables. Practice settings that were not significantly different from each other were pooled together when reporting descriptive statistics.
Results
Respondent Characteristics
A total of 32,544 survey invitations were sent to valid email addresses and 1,212 surveys were submitted (3.7% overall response rate). The individual state response rate varied from 3.3% to 7.5% (Table 1). Respondents had been licensed significantly longer than non-respondents in all states except Wyoming. For the overall group of respondents, therapists with 0-10 years of state licensure were somewhat under-represented and therapists with 20+ years of state licensure were somewhat over-represented. However, the 1,212 respondents were generally similar to American Physical Therapy Association (APTA) members and the U.S. PT workforce in that they were approximately 70% female, most commonly had doctoral physical therapy degrees, had been practicing for approximately 18 years on average, largely did not have specialty certification, were most commonly employed in outpatient clinics and were primarily engaged in the musculoskeletal practice pattern (Table 2).
Table 1. Assessment of Non-Response Bias.
| Respondents | Non-Respondents | P value† | |
|---|---|---|---|
| Full sample | 1,212 (3.7%) | 31,332 (96.3%) | |
| Years licensed*, median (IQR) | 14.6 (5.6-23.0) | 11.8 (3.9-20.5) | <0.0001 |
| 0-10 | 474 (39.4%) | 14,921 (48.0%) | |
| 11-20 | 360 (29.9%) | 8,997 (28.9%) | |
| 21+ | 369 (30.7%) | 7,814 (23.1%) | |
| Florida | 331 (3.3%) | 9,663 (96.7%) | |
| Years licensed*, median (IQR) | 15.7 (5.1-22.3) | 11.8 (4.0-20.0) | 0.0002 |
| 0-10 | 118 (36.2%) | 4,564 (48.0%) | |
| 11-20 | 114 (35.0%) | 2,950 (31.0%) | |
| 21+ | 94 (28.8%) | 2,002 (21.0%) | |
| New Jersey | 202 (4.4%) | 4,407 (95.6%) | |
| Years licensed*, median (IQR) | 15.9 (9.3-25.6) | 13.4 (7.5-21.1) | 0.0017 |
| 0-10 | 63 (31.7%) | 1,670 (38.5%) | |
| 11-20 | 65 (32.7%) | 1,584 (36.5%) | |
| 21+ | 71 (35.7%) | 1,088 (25.1%) | |
| Ohio | 304 (3.7%) | 7,823 (96.3%) | |
| Years licensed*, median (IQR) | 14.6 (6.7-24.5) | 13.1 (5.0-21.6) | 0.0332 |
| 0-10 | 114 (37.5%) | 3,346 (42.8%) | |
| 11-20 | 95 (31.3%) | 2,436 (31.1%) | |
| 21+ | 95 (31.3%) | 2,041 (26.1%) | |
| Texas | 347 (3.7%) | 9,092 (96.3%) | |
| Years licensed*, median (IQR) | 12.1 (2.7-22.6) | 8.1 (2.0-19.6) | 0.0002 |
| 0-10 | 165 (47.7%) | 5,169 (57.0%) | |
| 11-20 | 77 (22.3%) | 1,902 (21.0%) | |
| 21+ | 104 (30.1%) | 1,995 (22.0%) | |
| Wyoming | 28 (7.5%) | 347 (92.5%) | |
| Years licensed*, median (IQR) | 10.2 (3.5-19.8) | 9.2 (3.6-17.8) | 0.6578 |
| 0-10 | 14 (50.0%) | 190 (54.8%) | |
| 11-20 | 9 (32.1%) | 110 (31.7%) | |
| 21+ | 5 (17.9%) | 47 (13.5%) |
Values are n (%) unless otherwise noted. Bolded percentages are calculated by row. Non-bolded percentages are calculated by column. Some percentages are based on a lower denominator due to missing data for years licensed. IQR, Interquartile range
Calculated using initial license date from state board and survey deployment date
P values are from Mann-Whitney U tests comparing years licensed between respondents and non-respondents
Table 2. Physical Therapist Respondent Characteristics.
| Respondents Currently Involved in Clinical Stroke Rehab | All Respondents | National APTA Member Data27,28 | ABPTS / APTA National PT Workforce Data29,30 | |
|---|---|---|---|---|
| Total N | 568 | 1,212 | N/A | 198,686 |
| Female sex | 407/566 (71.9%) | 843/1,172 (71.9%) | (69.9%) | N/A |
| Highest earned degree | n=565 | n=1,173 | n=N/A | |
| Baccalaureate | 163 (28.9%) | 342 (29.2%) | (19.0%) | N/A |
| Master's | 150 (26.6%) | 304 (25.9%) | (27.8%) | N/A |
| DPT | 235 (41.6%) | 468 (39.9%) | (44.4%) | N/A |
| PhD | 6 (1.1%) | 28 (2.4%) | (5.6%) | N/A |
| PhD and DPT | 3 (0.5%) | 9 (0.8%) | (1.2%) | N/A |
| Other | 8 (1.4%) | 22 (1.9%) | (2.0%) | N/A |
| Years in practice | n=566 | n=1,175 | n=N/A | |
| Mean (SD) | 16.7 (11.4) | 18.2 (11.6) | 18.4 (N/A) | N/A |
| 0-10 | 195 (34.5%) | 344 (29.3%) | (33.6%) | N/A |
| 11-20 | 178 (31.5%) | 365 (31.1%) | (24.2%) | N/A |
| 21+ | 193 (34.1%) | 466 (39.7%) | (42.3%) | N/A |
| Specialty certification | n=525 | n=1,103 | n=198,686 | |
| ABPTS Cardiovascular Pulmonary Clinical Specialist (CCS) | 0 (0.0%) | 0 (0.0%) | N/A | 174 (0.1%) |
| ABPTS Geriatric Clinical Specialist (GCS) | 17 (3.2%) | 28 (2.5%) | N/A | 1,399 (0.7%) |
| ABPTS Neurologic Clinical Specialist (NCS) | 10 (1.9%) | 15 (1.4%) | N/A | 1,317 (0.7%) |
| Any ABPTS Certification | 59 (11.2%) | 146 (13.2%) | N/A | 13,399 (6.7%) |
| APTA Certified Exercise Expert for the Aging Adult (CEEAA) | 7 (1.3%) | 9 (0.8%) | N/A | N/A |
| ACSM Certified Exercise Specialist (CES) | 7 (1.3%) | 9 (0.8%) | N/A | N/A |
| NSCA Certified Strength and Conditioning Specialist (CSCS) | 0 (0.0%) | 33 (3.0%) | N/A | N/A |
| Practice setting | n=568 | n=1,176 | n=N/A | |
| Outpatient clinic | 253 (40.9%) | 576 (49.0%) | (53.3%) | N/A |
| Home health | 84 (13.6%) | 143 (12.2%) | (6.7%) | N/A |
| Extended care facility | 78 (12.6%) | 90 (7.8%) | (4.2%) | N/A |
| Inpatient rehabilitation facility | 55 (8.9%) | 61 (5.2%) | (3.9%) | N/A |
| Acute care hospital | 98 (15.9%) | 113 (9.6%) | (11.0%) | N/A |
| Primary practice pattern | n=568 | n=1,048 | n=N/A | |
| Musculoskeletal | 398 (70.1%) | 772 (73.7%) | (68.0%) | N/A |
| Neuromuscular | 125 (22.0%) | 217 (20.7%) | (22.0%) | N/A |
| Cardiopulmonary | 41 (7.2%) | 48 (4.6%) | (6.3%) | N/A |
| Integumentary | 4 (0.7%) | 11 (1.1%) | (3.7%) | N/A |
Values are n (%) unless otherwise noted. APTA, American Physical Therapy Association; ABPTS, American Board of Physical Therapy Specialties; N/A, not available; ACSM, American College of Sports Medicine; NSCA, National Strength and Conditioning Association
A total of 568 respondents indicated that they were currently involved in clinical practice (in a setting other than school, academic/research or ‘other’) and had evaluated or treated at least one patient for stroke rehabilitation within the past 3 months. This subset of respondents was used for the remaining analyses. Within this subset, 76.9% [437/568] completed the last page of the survey, 63.2% [359/568] completed all questions presented (but were not necessarily presented every question based on responses to filtering questions) and 55.3% [314/568] completed all questions of interest for the analyses (Figure 1).
Figure 1. Survey Response, Completion and Completeness Rates.

AEX Utilization and Barriers
Most respondents (87.8% [423/482]) agreed or strongly agreed that AEX should be incorporated into treatment programs of individuals with stroke, but fewer (72.1% [346/480]) reported that they were able to prescribe AEX for every individual with stroke for whom it was indicated (Table 3). These results did not significantly differ between practice settings. Reported AEX prescription rates were also similar between practice settings, except that acute care was significantly different from other practice settings. Therefore, the descriptive statistics for these questions are provided separately for acute care, as described in the methods section. AEX was prescribed for at least some individuals with stroke by 66.7% [54/81] of acute care therapists and 93.1% [375/403] of therapists in other settings. AEX was prescribed for the majority of individuals with stroke by 24.7% [20/81] of acute care therapists and 61.3% [247/403] of therapists in other settings. Most respondents across all practice settings (83.8% [402/480]) perceived at least one barrier to routine AEX prescription for individuals with stroke. In the sensitivity analysis comparing the under-represented subset of respondents with 0-10 years of state licensure to the full sample of respondents, the above results varied by <6% across all questions.
Table 3. AEX utilization for individuals with stroke by U.S. PTs.
| Agree that AEX should be part of stroke rehab (n=482) | 423 (87.8%) |
| Able to prescribe AEX for every individual with stroke for whom it is indicated (n=480) | 346 (72.1%) |
| Perceive ≥ 1 barrier to routine AEX prescription for individuals with stroke (n=480) | 402 (83.8%) |
| Acute care (n=81) | |
| -Prescribe AEX for >0% of individuals with stroke | 54 (66.7%) |
| -Prescribe AEX for >50% of individuals with stroke | 20 (24.7%) |
| Non-acute clinical practice settings (n=403) | |
| -Prescribe AEX for >0% of individuals with stroke | 375 (93.1%) |
| -Prescribe AEX for >50% of individuals with stroke | 247 (61.3%) |
Values are n (%). Multiple survey questions. There were no significant differences among practice settings for the top 3 rows.
Among acute care PTs (n=81), the most common perceived patient-related barriers to AEX prescription post stroke were: limited ability to exercise at a training level (71.6%), balance impairments (69.1%) and cognitive/perceptual impairments (67.9%) (Figure 2). In this same subgroup, the most common perceived institutional barriers were: short length of stay (79.0%), lack of exercise equipment (51.9%) and lack of time (45.7%).
Figure 2. Perceived Barriers to Aerobic Exercise Prescription for Individuals with Stroke.
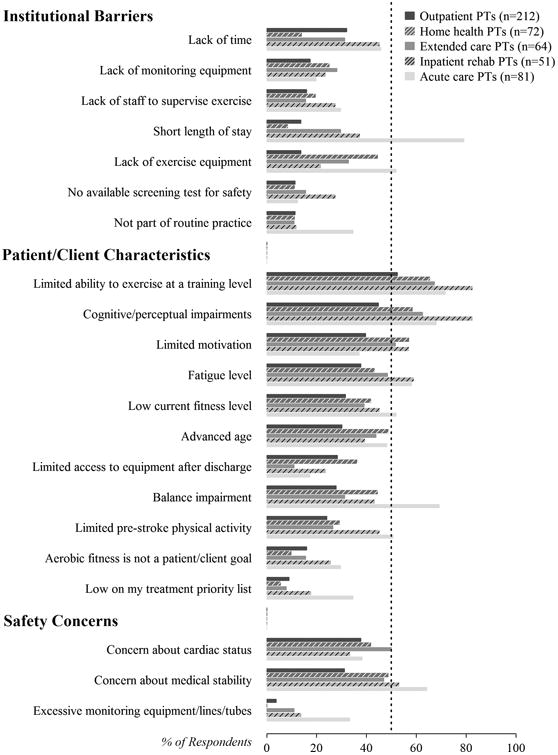
Multiple response variable. Within each barrier category (institutional barriers, patient/client characteristics and safety concerns), perceived barriers are ordered from most to least often reported among outpatient PTs. Barriers reported by less than 25% of respondents in all practice settings are not shown. Inpatient rehabilitation did not significantly differ from extended care for any perceived barriers. All other pairwise comparisons between practice settings were significant for at least one perceived barrier.
Among non-acute care PTs (n=399), the most common perceived patient-related barriers were: limited ability to exercise at a training level (52.4-82.4%, depending on practice setting), cognitive/perceptual impairments (44.8-82.4%, depending on practice setting) and limited motivation (37.0-56.9%, depending on practice setting). In this same subgroup, the most common perceived institutional barriers differed between practice settings (Figure 2).
A slight majority of acute care PTs (59.5% [47/79]) and a lower proportion of non-acute care PTs (32.3% [129/399]) reported that exercise stress testing with ECG was available for individuals with stroke (either at their facility or by referral). Most respondents across all practice settings (98.0% [432/441]) reported that they did not have access to exercise ECG equipment for their patients/clients with stroke (Table 4). Only 38.7% [161/416] of respondents were confident about all aspects of AEX prescription for individuals with stroke (Table 5). Leading areas of uncertainty were: strategies to increase motivation (26.2% [109/416]), intensity (23.8% [99/416]) and strategies to increase self-efficacy (23.1% [96/416]). In addition, 54.6% [252/462] of respondents reported that they were unfamiliar with American College of Sports Medicine Guidelines for Exercise Testing and Prescription and 84.6% [391/462] reported that they were unfamiliar with AHA Physical Activity and Exercise Recommendations for Stroke Survivors. Among outpatient PT respondents, 53.7% [103/192] reported that they were not aware of any community-based programs in their area that provide supervised AEX opportunities appropriate for individuals with stroke.
Table 4. AEX Resources Available for Individuals with Stroke by Practice Setting (n=441).
| Outpatient PTs (n=193) | Home health PTs (n=65) | Extended care PTs (n=58) | Inpatient rehab PTs (n=49) | Acute care PTs (n=76) | |
|---|---|---|---|---|---|
| Treadmill | 174 (90.2%) | 8 (12.3%) | 20 (34.5%) | 39 (79.6%) | 13 (17.1%) |
| Body weight support system | 52 (26.9%) | 0 (0.0%) | 6 (10.3%) | 33 (67.3%) | 12 (15.8%) |
| Fall prevention harness system | 23 (11.9%) | 0 (0.0%) | 3 (5.2%) | 11 (22.4%) | 10 (13.2%) |
| Lower extremity ergometer | 180 (93.3%) | 23 (35.4%) | 49 (84.5%) | 37 (75.5%) | 24 (31.6%) |
| Upper extremity ergometer | 159 (82.4%) | 12 (18.5%) | 40 (69.0%) | 37 (75.5%) | 22 (28.9%) |
| Total body ergometer | 106 (54.9%) | 3 (4.6%) | 43 (74.1%) | 30 (61.2%) | 10 (13.2%) |
| Accessible pool | 55 (28.5%) | 5 (7.7%) | 5 (8.6%) | 10 (20.4%) | 3 (3.9%) |
| Exercise ECG equipment | 3 (1.6%) | 0 (0.0%) | 1 (1.7%) | 1 (2.0%) | 4 (5.3%) |
| Continuous heart rate monitors | 56 (29.0%) | 11 (16.9%) | 11 (19.0%) | 15 (30.6%) | 47 (61.8%) |
| Pulse oximetry equipment | 140 (72.5%) | 40 (61.5%) | 55 (94.8%) | 43 (87.8%) | 66 (86.8%) |
| Metabolic measurement system | 2 (1.0%) | 0 (0.0%) | 0 (0.0%) | 2 (4.1%) | 4 (5.3%) |
| Activity monitors | 22 (11.4%) | 10 (15.4%) | 8 (13.8%) | 6 (12.2%) | 7 (9.2%) |
Values are n (%). Multiple response variable. All pairwise comparisons between practice settings were significant for at least one AEX resource.
Table 5. Are you uncertain about any aspects of AEX prescription for individuals with stroke? (n=416).
| No, I am confident in all aspects | 161 (38.7%) |
| Strategies to increase motivation | 109 (26.2%) |
| Intensity (workload, HR, RPE) | 99 (23.8%) |
| Strategies to increase self-efficacy | 96 (23.1%) |
| Personnel involvement | 51 (12.3%) |
| Safety screening or monitoring | 50 (12.0%) |
| Duration (minutes / session) | 38 (9.1%) |
| Mode | 37 (8.9%) |
| Frequency (days / week) | 18 (4.3%) |
| Individual vs. group | 9 (2.2%) |
Values are n (%). Multiple response variable. There were no significant differences among practice settings.
AEX Dosing Parameters
The majority of PTs in all practice settings reported prescribing standing exercises (80.0-96.6%, depending on practice setting), sitting/lying exercises (73.9-93.1%, depending on practice setting) and over ground walking (72.7-93.1%, depending on practice setting) for AEX among individuals with stroke (Figure 3). Other AEX modes differed between practice settings. The majority of non-acute care PTs reported prescribing some form of ergometry (65.5%-94.6%, depending on practice setting). The majority of inpatient rehab (67.4% [31/46]) and home health (53.5% [31/58]) PTs reported prescribing stair climbing. The majority of outpatient PTs (56.2% [100/178]) reported prescribing treadmill walking/jogging.
Figure 3. AEX Modes Prescribed for Individuals with Stroke.
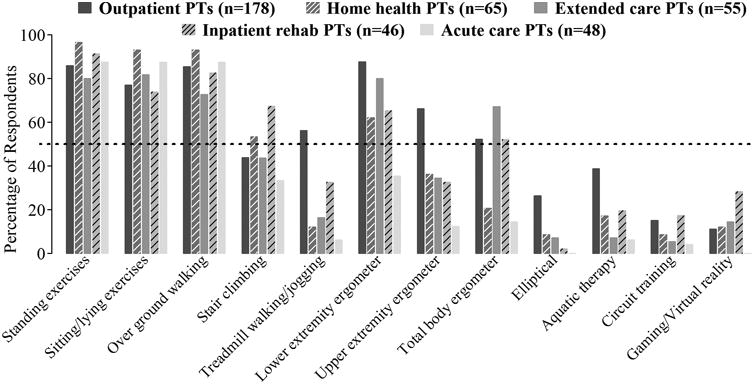
Multiple response variable. Inpatient rehabilitation did not significantly differ from extended care and acute care did not significantly differ from home health for any AEX mode. All other pairwise comparisons between practice settings were significant for at least one AEX mode.
To determine the initial AEX intensity for individuals with stroke, 99.2% [383/386] of respondents reported using at least one subjective method, 79.5% [307/386] reported using at least one target HR method and 32.6% [126/386] reported using at least one target workload method (additional details in Table 6). Light intensity was the most commonly prescribed intensity reported by acute care and outpatient PTs, while moderate intensity was the most common in other practice settings (Table 7). The volume of prescribed AEX for individuals with stroke is described in Table 8. Some volume parameters differed significantly between several practice settings, so ranges are reported across practice settings. Median AEX volume ranged from 20-30 minutes, 3-5 times per week for 2-8 weeks.
Table 6. Methods used to determine initial AEX intensity for individuals with stroke (n=386).
| Subjective Methods | |
|---|---|
| General observed response | 367 (95.1%) |
| Patient/client feedback about difficulty | 346 (89.6%) |
| Rating of perceived exertion | 280 (72.5%) |
| Talk test | 198 (51.3%) |
| Target Heart Rate (HR) | |
| % predicted maximal HR | 202 (52.3%) |
| An absolute HR (e.g. 120 bpm) | 104 (26.9%) |
| % HR reserve based on predicted maximal HR | 64 (16.6%) |
| % peak HR from exercise test | 52 (13.5%) |
| Below HR threshold of an abnormal exercise test response | 30 (7.8%) |
| % HR reserve based on peak HR from exercise test | 14 (3.6%) |
| HR at first ventilatory threshold | 4 (1.0%) |
| Target Workload | |
| Below workload threshold of an abnormal exercise test response | 51 (13.2%) |
| An absolute workload (e.g. 3 METs, 100 W, 1.0 mph) | 39 (10.1%) |
| Workload for target % of predicted VO2max/VO2max reserve | 37 (9.6%) |
| Workload for target % of VO2peak/VO2peak reserve from exercise test | 17 (4.4%) |
| Workload at first ventilatory threshold | 9 (2.3%) |
| Other/None | |
| Other | 12 (3.1%) |
| None | 128 (33.2%) |
Values are n (%). Multiple response variable. VO2, Oxygen consumption rate. There were no significant differences among practice settings. Within each category (subjective methods, target HR, target workload), methods are ordered from most to least often reported.
Table 7. Average AEX Intensity Prescribed for Individuals with Stroke by Practice Setting (n=381).
| Outpatient PTs (n=177) | Home health PTs (n=55) | Extended care PTs (n=54) | Inpatient rehab PTs (n=46) | Acute care PTs (n=49) | |
|---|---|---|---|---|---|
| Very light | 12 (6.8%) | 3 (5.5%) | 7 (13.0%) | 2 (4.4%) | 12 (24.5%) |
| Light | 77 (43.5%) | 17 (30.9%) | 17 (31.5%) | 17 (37.0%) | 22 (44.9%) |
| Moderate | 75 (42.4%) | 34 (61.8%) | 24 (44.4%) | 23 (50.0%) | 12 (24.5%) |
| Hard/Vigorous | 3 (1.7%) | 0 (0.0%) | 0 (0.0%) | 1 (2.2%) | 0 (0.0%) |
| Unknown | 10 (5.7%) | 1 (1.8%) | 6 (11.1%) | 3 (6.5%) | 3 (6.1%) |
Values are n (%). Single response variable. Acute care was significantly different from inpatient rehabilitation, home health and outpatient. No respondents reported prescribing intensity higher than hard/vigorous. Intensity categories were defined on the survey as follows: Very light, <10 rating of perceived exertion (RPE 6-20), <50% HRmax, <20% HRreserve; Light, 10-11 RPE, 50-63% HRmax, 20-39% HRreserve; Moderate, 12-13 RPE, 64-76% HRmax, 40-59% HRreserve; Hard/Vigorous, 14-16 RPE, 77-93% HRmax, 60-84% HRreserve.
Table 8. Volume of prescribed AEX for individuals with stroke.
| Practice setting | N | Session duration (minutes) | Frequency (sessions / week) | Total duration (weeks) | Total no. of sessions | Total volume (minutes) |
|---|---|---|---|---|---|---|
| Outpatient | 168 | 20 (15-30) | 3 (3-5) | 8 (6-12) | 31 (24-48) | 720 (360-1,200) |
| Home health | 54 | 20 (15-30) | 4 (3-5) | 6 (4-8) | 24 (18-40) | 540 (300-840) |
| Extended care | 53 | 20 (15-30) | 5 (4-5) | 6 (4-8) | 30 (20-40) | 720 (360-1,200) |
| Inpatient rehabilitation | 42 | 30 (15-30) | 5 (4-5) | 4 (3-8) | 20 (12-32) | 600 (240-1,200) |
| Acute care | 43 | 20 (15-30) | 5 (3-6) | 2 (1-4) | 10 (6-20) | 180 (90-360) |
Values are median (interquartile range). Total no. of sessions = frequency (sessions / week) × total duration (weeks). Total volume = session duration × total no. of sessions. All pairwise comparisons between practice settings were significant for at least one aspect of AEX volume.
AEX Safety Considerations
To screen for safety before prescribing AEX for individuals with stroke, 22.7% [96/423] of respondents reported using some type of exercise test, 0.0-11.5% (depending on practice setting) reported using an exercise ECG, 73.5-92.2% (depending on practice setting) reported using HR response to exercise and 70.5% [298/423] reported using BP response to exercise (Table 9). A quarter of respondents (25.0% [116/465]) believed that an exercise ECG stress test is needed for individuals with stroke before prescribing AEX and only (1.8% [7/398]) had stress test results for the majority of their patients/clients (Table 10). To monitor for safety during AEX for individuals with stroke, 89.3% [341/382] of respondents reported monitoring HR, 75.9% [290/382] reported monitoring BP and 0.0-14.3% (depending on practice setting) reported monitoring ECG (Table 11).
Table 9. Safety Screening Methods Used for Individuals with Stroke Before Prescribing AEX by Practice Setting (n=423).
| Outpatient PTs (n=197) | Home health PTs (n=64) | Extended care PTs (n=61) | Inpatient rehab PTs (n=49) | Acute care PTs (n=52) | |
|---|---|---|---|---|---|
| Past medical history | 193 (98.0%) | 61 (95.3%) | 57 (93.4%) | 46 (93.9%) | 49 (94.2%) |
| General presentation | 181 (91.9%) | 61 (95.3%) | 54 (88.5%) | 42 (85.7%) | 51 (98.1%) |
| ACSM AEX contraindications | 63 (32.0%) | 20 (31.3%) | 18 (29.5%) | 12 (24.5%) | 13 (25.0%) |
| A risk stratification category | 17 (8.6%) | 4 (6.3%) | 5 (8.2%) | 3 (6.1%) | 1 (1.9%) |
| Six-minute walk test | 63 (32.0%) | 24 (37.5%) | 12 (19.7%) | 11 (22.4%) | 8 (15.4%) |
| Symptom-limited exercise test | 37 (18.8%) | 13 (20.3%) | 11 (18.0%) | 8 (16.3%) | 10 (19.2%) |
| Submaximal exercise test | 15 (7.6%) | 10 (15.6%) | 4 (6.6%) | 5 (10.2%) | 1 (1.9%) |
| Pulse/HR response to exercise | 148 (75.1%) | 59 (92.2%) | 54 (88.5%) | 36 (73.5%) | 44 (84.6%) |
| Resting BP | 147 (74.6%) | 56 (87.5%) | 43 (70.5%) | 33 (67.3%) | 41 (78.8%) |
| BP response to exercise | 131 (66.5%) | 54 (84.4%) | 42 (68.9%) | 33 (67.3%) | 38 (73.1%) |
| Resting ECG | 4 (2.0%) | 1 (1.6%) | 1 (1.6%) | 3 (6.1%) | 9 (17.3%) |
| Exercise ECG | 4 (2.0%) | 1 (1.6%) | 0 (0.0%) | 1 (2.0%) | 6 (11.5%) |
| Consultation with a physician | 59 (29.9%) | 17 (26.6%) | 17 (27.9%) | 20 (40.8%) | 19 (36.5%) |
Values are n (%).Multiple response variable. Acute care, home health and outpatient were each significantly different from each other for at least one safety screening method. All other pairwise comparisons between practice settings were not significant. ACSM, American College of Sports Medicine
Table 10. Utilization and beliefs about exercise ECG testing for individuals with stroke.
| Beliefs (n=465) | |
|---|---|
| Believe exercise ECG stress testing is needed before AEX | 116 (25.0%) |
| Believe ECG monitoring is needed during initial AEX sessions | |
| -Acute care PTs (n=75) | 33 (44.0%) |
| -Non-acute PTs (n= 390) | 79 (20.3%) |
| Believe at least one type of exercise ECG testing above is needed | |
| -Acute care PTs (n= 75) | 42 (56.0%) |
| -Non-acute PTs (n= 390) | 119 (30.5%) |
| Utilization (n=398) | |
| Have results from ECG stress test for >0% of individuals with stroke | 89 (22.4%) |
| Have results from ECG stress test for >50% of individuals with stroke | 7 (1.8%) |
| Monitor ECG in initial AEX sessions for >0% of individuals with stroke | |
| -Acute care PTs (n=44) | 14 (31.8%) |
| -Non-acute PTs (n= 354) | 17 (4.8%) |
| Monitor ECG in initial AEX sessions for >50% of individuals with stroke | |
| -Acute care PTs (n=44) | 7 (15.9%) |
| -Non-acute PTs (n= 354) | 3 (0.9%) |
| Use at least one type of exercise ECG testing above for >0% of individuals | |
| -Acute care PTs (n=44) | 21 (47.7%) |
| -Non-acute PTs (n= 354) | 81 (22.9%) |
| Use at least one type of exercise ECG testing above for >50% of individuals | |
| -Acute care PTs (n=44) | 7 (15.9%) |
| -Non-acute PTs (n= 354) | 8 (2.3%) |
Values are n (%). Multiple survey questions.
Table 11. Monitoring Used During AEX for Individuals with Stroke by Practice Setting (n=382).
| Outpatient PTs (n=176) | Home health PTs (n=56) | Extended care PTs (n=55) | Inpatient rehab PTs (n=46) | Acute care PTs (n=49) | |
|---|---|---|---|---|---|
| General observation | 161 (91.5%) | 53 (94.6%) | 54 (98.2%) | 43 (93.5%) | 48 (98.0%) |
| Rating of perceived exertion | 116 (65.9%) | 40 (71.4%) | 35 (63.6%) | 30 (65.2%) | 25 (51.0%) |
| HR – measured manually | 101 (57.4%) | 36 (64.3%) | 24 (43.6%) | 21 (45.7%) | 16 (32.7%) |
| HR – HR monitor or oximeter | 109 (61.9%) | 46 (82.1%) | 45 (81.8%) | 39 (84.8%) | 45 (91.8%) |
| Blood pressure | 128 (72.7%) | 48 (85.7%) | 39 (70.9%) | 34 (73.9%) | 41 (83.7%) |
| ECG | 2 (1.1%) | 1 (1.8%) | 0 (0.0%) | 0 (0.0%) | 7 (14.3%) |
| Oxygen saturation | 113 (64.2%) | 41 (73.2%) | 52 (94.5%) | 38 (82.6%) | 44 (89.8%) |
Values are n (%). Multiple response variable. Outpatient was not significantly different from home health and inpatient rehabilitation was not significantly different from acute care, extended care or home health for any monitoring methods. All other pairwise comparisons between practice settings were significant for at least one monitoring method.
Regarding serious adverse events observed during or immediately after AEX, 9.9% [43/436] of respondents reported having witnessed at least one individual with stroke having a cardiac event (myocardial infarction or cardiac arrest) and 11.0% [48/437] of respondents reported having witnessed at least one individual having a recurrent stroke.
Discussion
This survey aimed to assess AEX prescription for individuals with stroke among U.S. PTs currently involved with clinical stroke rehabilitation. Although most respondents believed that AEX should be incorporated into rehabilitation programs for individuals with stroke, several barriers to routine AEX prescription were identified. These barriers included institutional characteristics (e.g. lack of time, staff, equipment and safety screening methods), patient/client characteristics (e.g. limited ability and motivation to exercise at a training level, cognitive/perceptual impairments and balance impairments), safety concerns, lack of familiarity with AEX guidelines/recommendations and limited availability of stress testing and community-based AEX opportunities for individuals with stroke after rehabilitation discharge.
Despite these barriers, our survey results indicate that the majority of PTs across all practice settings appear to be prescribing at least the minimum recommended AEX session duration and frequency for individuals with stroke (20 minutes, 3 days/week).8 However, median total duration of prescribed AEX ranged from 2-8 weeks across practice settings and these durations are shorter than those used in most previous AEX studies (3-6 months)9-16 and recommendations.8 Greater availability and awareness of community-based programs for persons with stroke to continue AEX after rehabilitation discharge could help to extend these total durations and make AEX a life-long habit after stroke.31
One of the most common areas of uncertainty reported by respondents was in prescribing AEX intensity, and this variable is a critical determinant of AEX safety and efficacy.32,33 While moderate to vigorous intensity AEX is recommended during the rehabilitation phase of stroke recovery,8 light intensity (e.g. <40% HR reserve) was the most commonly prescribed intensity among outpatient PTs and was also common in other settings. This intensity is generally not considered to be AEX,19,20 nor to require a pre-exercise stress test.8,33 Therefore, it is possible that PTs are commonly prescribing light intensity because of safety concerns or limited availability of stress testing or ECG monitoring. It is also important to note that respondents reported primarily using subjective methods to determine AEX intensity and primarily based target HR calculations on age-predicted HR max, rather than on an exercise test. This practice increases the difficulty of determining AEX intensity with certainty.32,33
Although ECG stress testing is recommended prior to initiating AEX among persons with stroke,8 only 2% of non-acute care PT respondents reported having results from an ECG stress test or monitoring an ECG during initial AEX sessions for the majority of patients/clients. Remarkably, this number is identical to the number of respondents who reported using stress testing in a previous survey of Canadian PTs involved with neurologic rehabilitation.22 Based on responses to the rest of our survey, this low utilization of ECG testing is most likely related to the use of light intensity exercise and/or the limited availability of stress testing and exercise ECG equipment. In addition, the low utilization of ECG testing also appears to be related to a prevalent belief that it is not needed. For example, 69% of non-acute care PT respondents believed that neither stress testing nor ECG monitoring are necessary for most individuals with stroke. This belief is inconsistent with AEX guidelines34 and stroke-specific AEX recommendations,8,18 and could lead to safety issues. For example, a previous study that involved ECG stress testing on 98 consecutive individuals with stroke identified previously unknown clinically relevant abnormalities in 11 individuals, including 6 persons with no history of coronary artery disease.35 Continuing education programming emphasizing these data and post-stroke AEX recommendations could help increase utilization of ECG stress testing.
However, it has also been recognized that stress testing is not available in all settings (e.g. rural areas) and that avoiding AEX in these situations may itself present a health risk. For example, AHA recommendations state that individualized AEX prescription should not be delayed if stress testing is not feasible or the individual's physician determines it is not indicated.8 Unfortunately, no stroke studies have directly evaluated the relative safety of AEX compared to AEX avoidance in the absence of baseline ECG testing. Given the results of this survey, this is clearly an area where more research is needed to inform best practices.
In our survey, 10% of respondents reported that they had witnessed a person with stroke having a myocardial infarction or cardiac arrest in temporal proximity to AEX and 11% reported that they had witnessed a temporally-related recurrent stroke. These rates are not entirely surprising, given that persons with stroke have a high risk of myocardial infarction (3 to 5% incidence per year) and recurrent stroke (~30% lifetime incidence).8 Further, it is well established that AEX can precipitate plaque disruption or ventricular arrhythmias in a small number of susceptible individuals.8,36 However, the percentages reported on this survey do seem to be rather high since the typical rate of exercise-related serious cardiac events in cardiac rehabilitation is only 1 per 81,670 exercise hours.34 In addition, previous stroke studies have not reported any serious cardiac events or recurrent strokes related to AEX.37 Both cardiac rehabilitation and post-stroke AEX studies generally involve medical screening, baseline ECG stress testing and/or ECG monitoring during initial AEX sessions. Therefore, it is possible that the rates of serious adverse events reported by survey respondents could be reduced by increasing the frequency of these safety practices in clinical stroke rehabilitation. It is also important to remember that long-term AEX reduces the risk of cardiovascular events8,36 and the benefits of AEX are widely considered to outweigh the risks,36 including after stroke.8
Data from this survey estimate that about half of licensed PTs (568 out of 1,212) are currently involved with clinical stroke rehabilitation to some degree. This large proportion speaks to the high incidence and prevalence of stroke,7 as well as the importance of PTs in the stroke recovery process. However, our data also indicate that most PTs involved with stroke rehabilitation are likely not focused on this practice area, as only 22% reported being primarily engaged in the neuromuscular practice pattern. Specialization could make it easier to keep up with current best-practice recommendations and stroke-related continuing education or to establish relationships to facilitate comprehensive and integrated stroke care (e.g. referrals for stress testing, transitions to community-based AEX programs appropriate for individuals with stroke). Future studies are needed to determine whether PT specialization and continuing education have an impact on stroke recovery outcomes.
Limitations
The primary limitation to this study is the low response rate (3.7%). While it is possible that the response rate in the population of interest (PTs currently involved in clinical stroke rehabilitation in common practice settings) was higher, there is no way to know how many survey invitations were sent to PTs meeting these criteria. The low response rate may have been partially related to survey fatigue, because states were sampled where email address listings of licensed PTs were publicly available at no cost. Therefore, PTs in these states may receive many survey and solicitation emails. Yet despite this low response rate, the number of responses received (n=1,212) and analyzed (n=568) was larger than in previous related studies (n=155 to 230)22,31 and respondents appeared to be representative of the U.S. PT workforce. One exception was that PTs with 0-10 years of licensure were somewhat under-represented. However, sensitivity analyses indicated that this likely had minimal impact on the results. It is possible that respondents may have been more favorable to AEX prescription than non-respondents. To decrease this possibility, the email invitation specifically asked PTs to participate even if they did not typically prescribe AEX. Another limitation to this study is the possibility of response bias. Although all questions were posed with neutral, non-judgmental phasing, respondents may have answered some questions in a manner anticipated to please the researchers.38 This tendency could have artificially inflated the results regarding AEX utilization, dosing and safety practices.
Conclusions
Results of this survey study indicate that most U.S. PTs believe AEX should be incorporated within stroke rehabilitation. However, several barriers to routine AEX prescription were identified. While most PTs reported prescribing the recommended AEX session duration and frequency, reported intensity and total duration of AEX were generally lower than recommended and use of exercise testing was very limited. In terms of research, studies are needed to identify the best ways to address the identified barriers. More specific clinical guidelines for post-stroke exercise testing and training may also be beneficial. For PT education, greater focus on the application of exercise physiology principles to rehabilitation could help. In clinical practice, greater collaboration between stroke and cardiac rehabilitation teams would likely facilitate better adherence to post-stroke AEX recommendations.
Supplementary Material
SDC 2. Appendix, Survey Instrument.docx
SDC 3. Appendix, Example Email Invitation to Participate.docx
Supplemental Digital Content: SDC 1. Video Abstract.wmv
Acknowledgments
The authors thank Dr. Ada Tang and physical therapist focus group participants for their assistance with survey development and Jennifer Westover for her assistance with data management.This work was conducted in partial fulfillment of the requirements for a PhD in Epidemiology (PB) in the Department of Environmental Health at the University of Cincinnati College of Medicine.
Funding: This research was supported by a Promotion of Doctoral Studies Scholarship from the Foundation for Physical Therapy (PB). Institutional support was provided by an NIH Clinical and Translational Science Award (8UL1-TR000077). SB was supported in part by K01HD067318 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
Footnotes
A portion of this work was presented at the IV Step Conference (Columbus, OH; July 2016).
Conflicts of Interest: None
Video Abstract available for more insights from the authors (see Video, Supplemental Digital Content 1)
References
- 1.Billinger SA, Coughenour E, Mackay-Lyons MJ, Ivey FM. Reduced cardiorespiratory fitness after stroke: Biological consequences and exercise-induced adaptations. Stroke Res Treat. 2012;2012:959120. doi: 10.1155/2012/959120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Macko RF, Ivey FM, Forrester LW. Task-oriented aerobic exercise in chronic hemiparetic stroke: Training protocols and treatment effects. Topics in Stroke Rehabilitation. 2005;12(1):45–57. doi: 10.1310/PJQN-KAN9-TTVY-HYQH. [DOI] [PubMed] [Google Scholar]
- 3.Ivey FM, Hafer-Macko CE, Macko RF. Exercise rehabilitation after stroke. NeuroRX. 2006;3(4):439–450. doi: 10.1016/j.nurx.2006.07.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lackland DT, Elkind MS, D'Agostino RS, et al. Inclusion of stroke in cardiovascular risk prediction instruments: A statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2012;43(7):1998–2027. doi: 10.1161/STR.0b013e31825bcdac. [DOI] [PubMed] [Google Scholar]
- 5.Adams RJ, Chimowitz MI, Alpert JS, et al. Coronary risk evaluation in patients with transient ischemic attack and ischemic stroke: A scientific statement for healthcare professionals from the stroke council and the council on clinical cardiology of the American Heart Association/American Stroke Association. Circulation. 2003;108(10):1278–1290. doi: 10.1161/01.CIR.0000090444.87006.CF. [DOI] [PubMed] [Google Scholar]
- 6.Furie KL, Kasner SE, Adams RJ, et al. Guidelines for the prevention of stroke in patients with stroke or transient ischemic attack: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2011;42(1):227–276. doi: 10.1161/STR.0b013e3181f7d043. [DOI] [PubMed] [Google Scholar]
- 7.Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics-2016 update: A report from the American Heart Association. Circulation. 2016;133(4):e38–e360. doi: 10.1161/CIR.0000000000000350. [DOI] [PubMed] [Google Scholar]
- 8.Billinger SA, Arena R, Bernhardt J, et al. Physical activity and exercise recommendations for stroke survivors: A statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45(8):2532–53. doi: 10.1161/STR.0000000000000022. [DOI] [PubMed] [Google Scholar]
- 9.Macko RF, Ivey FM, Forrester LW, et al. Treadmill exercise rehabilitation improves ambulatory function and cardiovascular fitness in patients with chronic stroke: A randomized, controlled trial. Stroke. 2005;36(10):2206–2211. doi: 10.1161/01.STR.0000181076.91805.89. [DOI] [PubMed] [Google Scholar]
- 10.Ivey FM, Ryan AS, Hafer-Macko CE, Goldberg AP, Macko RF. Treadmill aerobic training improves glucose tolerance and indices of insulin sensitivity in disabled stroke survivors: A preliminary report. Stroke. 2007;38(10):2752–2758. doi: 10.1161/STROKEAHA.107.490391. [DOI] [PubMed] [Google Scholar]
- 11.Teixeira da Cunha Filho I, Lim PA, Qureshy H, Henson H, Monga T, Protas EJ. A comparison of regular rehabilitation and regular rehabilitation with supported treadmill ambulation training for acute stroke patients. J Rehabil Res Dev. 2001;38(2):245–255. [PubMed] [Google Scholar]
- 12.Luft AR, Macko RF, Forrester LW, et al. Treadmill exercise activates subcortical neural networks and improves walking after stroke. A randomized controlled trial. Stroke. 2008;39(12):3341–50. doi: 10.1161/STROKEAHA.108.527531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Rimmer JH, Rauworth AE, Wang EC, Nicola TL, Hill B. A preliminary study to examine the effects of aerobic and therapeutic (nonaerobic) exercise on cardiorespiratory fitness and coronary risk reduction in stroke survivors. Arch Phys Med Rehabil. 2009;90(3):407–412. doi: 10.1016/j.apmr.2008.07.032. [DOI] [PubMed] [Google Scholar]
- 14.Ivey FM, Hafer-Macko CE, Ryan AS, Macko RF. Impaired leg vasodilatory function after stroke: Adaptations with treadmill exercise training. Stroke. 2010;41(12):2913–2917. doi: 10.1161/STROKEAHA.110.599977. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ivey FM, Ryan AS, Hafer-Macko CE, Macko RF. Improved cerebral vasomotor reactivity after exercise training in hemiparetic stroke survivors. Stroke. 2011;42(7):1994–2000. doi: 10.1161/STROKEAHA.110.607879. [DOI] [PubMed] [Google Scholar]
- 16.Quaney BM, Boyd LA, McDowd JM, et al. Aerobic exercise improves cognition and motor function poststroke. Neurorehabil Neural Repair. 2009;23(9):879–885. doi: 10.1177/1545968309338193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Smith GV, Silver KH, Goldberg AP, Macko RF. “Task-oriented” exercise improves hamstring strength and spastic reflexes in chronic stroke patients. Stroke. 1999;30(10):2112–2118. doi: 10.1161/01.str.30.10.2112. [DOI] [PubMed] [Google Scholar]
- 18.Gordon NF, Gulanick M, Costa F, et al. Physical activity and exercise recommendations for stroke survivors: An American Heart Association scientific statement from the council on clinical cardiology, subcommittee on exercise, cardiac rehabilitation, and prevention; the council on cardiovascular nursing; the council on nutrition, physical activity, and metabolism; and the stroke council. Circulation. 2004;109(16):2031–2041. doi: 10.1161/01.CIR.0000126280.65777.A4. [DOI] [PubMed] [Google Scholar]
- 19.MacKay-Lyons MJ, Makrides L. Cardiovascular stress during a contemporary stroke rehabilitation program: Is the intensity adequate to induce a training effect? Arch Phys Med Rehabil. 2002;83(10):1378–1383. doi: 10.1053/apmr.2002.35089. [DOI] [PubMed] [Google Scholar]
- 20.Kuys S, Brauer S, Ada L. Routine physiotherapy does not induce a cardiorespiratory training effect post-stroke, regardless of walking ability. Physiother Res Int. 2006;11(4):219–227. doi: 10.1002/pri.344. [DOI] [PubMed] [Google Scholar]
- 21.Schmid AA, Butterbaugh L, Egolf C, Richards V, Williams L. Prevention of secondary stroke in VA: Role of occupational therapists and physical therapists. J Rehabil Res Dev. 2008;45(7):1019–1026. doi: 10.1682/jrrd.2007.10.0162. [DOI] [PubMed] [Google Scholar]
- 22.Doyle L, Mackay-Lyons M. Utilization of aerobic exercise in adult neurological rehabilitation by physical therapists in Canada. J Neurol Phys Ther. 2013;37(1):20–26. doi: 10.1097/NPT.0b013e318282975c. [DOI] [PubMed] [Google Scholar]
- 23.Microsoft Office Support. Test your document's readability. [Accessed 2/9 2016]; https://support.office.com/en-us/article/test-your-document-s-readability-0adc0e9a-b3fb-4bde-85f4-c9e88926c6aa. Updated 2016.
- 24.Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi: 10.1016/j.jbi.2008.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Baruch Y, Holtom B. Survey response rate levels and trends in organizational research. Hum Relat. 2008;61(8):1139–1160. [Google Scholar]
- 26.Benjamini Y, Hochberg Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J R Statist Soc B. 1995;57(1):289–300. [Google Scholar]
- 27.American Physical Therapy Association. Physical therapist member demographic profile 2013. [Accessed 1/20 2016]; http://www.apta.org/WorkforceData/. Updated 2014.
- 28.American Physical Therapy Association. Patient types and time management by facility. [Accessed 1/20 2016]; http://www.apta.org/WorkforceData/. Updated 2010.
- 29.American Physical Therapy Association. Licensed PTs by state (as of july 1, 2014) [Accessed 1/20 2016]; http://www.apta.org/WorkforceData/. Updated 2015.
- 30.Number of certified specialists in physical therapy by state (july 2014) [Accessed 7/27 2015]; American Board of Physical Therapy Specialties. http://www.abpts.org/About/Statistics/. Updated 2014.
- 31.Lau C, Chitussi D, Elliot S, et al. Facilitating community-based exercise for people with stroke: Cross-sectional e-survey of physical therapist practice and perceived needs. Phys Ther. 2015 doi: 10.2522/ptj.20150117. Epub ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Boyne P, Buhr S, Rockwell B, et al. Predicting heart rate at the ventilatory threshold for aerobic exercise prescription in persons with chronic stroke. J Neurol Phys Ther. 2015;39(4):233–240. doi: 10.1097/NPT.0000000000000102. [DOI] [PubMed] [Google Scholar]
- 33.Billinger SA, Boyne P, Coughenour E, Dunning K, Mattlage A. Does aerobic exercise and the FITT principle fit into stroke recovery? Curr Neurol Neurosci Rep. 2015;15(2) doi: 10.1007/s11910-014-0519-8. 519-014-0519-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.American College of Sports Medicine (ACSM) ACSM's guidelines for exercise testing and prescription. 9th. Philadephia, PA: Lippincott Williams & Wilkins; 2014. [Google Scholar]
- 35.Marzolini S, Oh P, McIlroy W, Brooks D. The feasibility of cardiopulmonary exercise testing for prescribing exercise to people after stroke. Stroke. 2012;43(4):1075–1081. doi: 10.1161/STROKEAHA.111.635128. [DOI] [PubMed] [Google Scholar]
- 36.Thompson PD, Franklin BA, Balady GJ, et al. Exercise and acute cardiovascular events placing the risks into perspective: A scientific statement from the American Heart Association council on nutrition, physical activity, and metabolism and the council on clinical cardiology. Circulation. 2007;115(17):2358–2368. doi: 10.1161/CIRCULATIONAHA.107.181485. [DOI] [PubMed] [Google Scholar]
- 37.Ivey FM, Hafer-Macko CE, Macko RF. Task-oriented treadmill exercise training in chronic hemiparetic stroke. J Rehabil Res Dev. 2008;45(2):249–259. doi: 10.1682/JRRD.2007.02.0035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Gnambs T, Kaspar K. Socially desirable responding in web-based questionnaires: A meta-analytic review of the candor hypothesis. Assessment. 2016 doi: 10.1177/1073191115624547. Epub ahead of print. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
SDC 2. Appendix, Survey Instrument.docx
SDC 3. Appendix, Example Email Invitation to Participate.docx
Supplemental Digital Content: SDC 1. Video Abstract.wmv