

Abstract
Characteristics of the spreads of platelet-rich plasma (PRP) are not widely known despite commonly use. This study aims to evaluate whether PRP stays within the injected area by using ultrasonography, to improve understanding of the spreads of intratendinous injected PRP. Thirty-nine patients (15 males, 24 females; mean age, 49.3 years), who had symptoms on their elbows (> 6 months) and diagnosed as lateral (25 elbows) or medial (14 elbows) tendinopathies of elbow, were included. The severity of tendon pathology was assessed by ultrasonography as tear or no tear. Immediately after ultrasound-guided PRP injection, ultrasound images were evaluated to assess the area of PRP distribution, which was defined as the presence of fluid or microbubbles. Ultrasound revealed that 13 elbows had tendon tear and 26 had no tear, respectively. Post-injection ultrasound confirmed the injected PRP was within the tendon in all cases. The mean distance of distribution from the injection site was 12.6 mm (5.0–26.0 mm). There was no difference in the distance of PRP distribution between tendon tear and no tear. Injected PRP spread to soft tissue outside the tendon in 20 of 39 cases. Intra-articular extension of PRP was observed in 5 cases. Although PRP remained intratendinous after the injection in all cases, some portion tended to spread outside from the injection site in a short space of time. Postinjection ultrasonographic imaging has a value for observing the spreading patterns of intratendinous PRP injection.
Key points.
This study aims to evaluate whether PRP stays within the injected area by using ultrasonography, to improve understanding of the spreads of intratendinous injected PRP.
Although PRP remained intratendinous after the injection in all cases, some portion tended to spread outside from the injection site in a short space of time.
Key words: Tendons, tennis elbow, sports, pain, inflammation
Introduction
Tendinopathy is characterized by micro-tears of collagen fibers due to repetitive overuse and scarring. Once tendinopathy occurs, it adversely affects function and increases the risk of re-injury. Furthermore, because of their poor vascularization, tendons have poor healing properties and heal more slowly compared to other connective tissues (Fenwick et al., 2002; Hayem, 2001). The major histologic characteristic of chronic tendinopathy is not inflammation but rather angiofibroblastic degeneration (Edwards and Calandruccio, 2003; Mishra and Pavelko, 2006). Therefore, new treatment options including dry needling, prolotherapy, and extracorporeal shockwave therapy are used to embrace inflammation rather than suppress it (Sampson et al., 2008).
Platelet-rich plasma (PRP) is a fraction of autologous blood that has a platelet concentration above the autologous blood from which it was derived. PRP aids healing in response to musculoskeletal trauma (Foster et al., 2009). PRP contains high levels of growth factors, which play important roles in tissue healing; these factors include transforming growth factor-β1, insulin-like growth factors 1 and 2, vascular endothelial growth factor, basic fibroblast growth factor, and hepatocyte growth factor (Alsousou et al., 2009; Molloy et al., 2003). Growth factors influence the cellular processes for tissue repair, facilitate healing by activating intracellular signal pathways via binding growth factor receptor, and play important roles in revascularization (Tabata, 2004).
PRP is obtained by sequestering and concentrating platelets using gradient density centrifugation (Marx et al., 1998). As a concentrated source of autologous platelets, PRP contains several different platelet-derived growth factors and other cytokines that promote soft tissue and bone healing. Autologous PRP was first used in the field of oral and maxillofacial surgery (Anitua, 1999; Marx et al., 1998) and has also been widely used in the other fields (Everts et al., 2007; 2008; Radice et al., 2010; Sampson et al., 2008). Injection is the preferred method to administer PRP into the injured tendon and various injectable PRP preparations are available for the management of various tendinopathies. PRP injection is increasingly being used as a regenerative therapy to treat tendinopathies. PRP can be used in the treatment of chronic non-healing tendon injuries, including the lateral and medial epicondylar, patellar, and Achilles tendons, among others. Several studies demonstrate PRP injection has beneficial effect on tendinopathy of elbow (Gosens et al., 2011; Mishra and Pavelko, 2006; Nguyen et al., 2011; Peerbooms et al., 2010). However, its effectiveness remains controversial, because only a few high-quality randomized controlled trials have evaluated PRP for the treatment of tendinopathy of elbow (Krogh et al., 2013).
Ultrasound-guided injection makes more sophisticated delivery possible by enabling the visualization of the injected products in the region of tendon injury (Loftus et al., 2012). Because the core premise of PRP is to increase the concentrations of active cellular components at the injury site, it is important to determine how much of the delivered PRP actually stays at the injection site and how much is distributed into the surrounding tissues. However, there are only a few reports about the post-injection distribution of PRP products (de Vos et al., 2010; Loftus et al., 2012).
Characteristics of the spreads of platelet-rich plasma (PRP) are not widely known despite commonly use. This study aims to evaluate whether PRP stays within the injected area by using ultrasonography, to improve understanding of the spreads of intratendinous injected PRP.
Methods
Participants
Patients with elbow pain who had visited the outpatient clinic of a university hospital between June 2013 and February 2015.
Inclusion criteria were as followed, (1) more than 6 months of elbow pain; (2) pain score of the affected elbow greater than 4 on the visual analog scale (from 0–10); (3) diagnosis of tendinopathies of elbow; and (4) no or little response to conservative care for at least 3 months. The exclusion criteria were as followed: (1) presence of another diagnosis of elbow, such as fracture, rheumatologic or neurologic diseases; (2) any prior surgery of the elbow region; (3) history of any injections on affected elbows, such as steroid or prolotherapy, within 3 months prior to visit; (4) unstable medical condition or known uncontrolled systemic diseases. This study was approved by the hospital’s institutional review board, and written informed consent was obtained from all participants after they were briefed about the study’s purpose and examination procedures.
Procedure
A physiatrist with 11 years of musculoskeletal ultrasonography experience performed ultrasound-guided PRP injection and ultrasonographic examinations of the affected elbow before and after the procedure. All examinations were performed using an Antares ultrasound scanner (Siemens, Berlin, Germany) with a 5–13-MHz multifrequency linear transducer. All PRP products were prepared using the sPRP kit (Huons Inc., Seoul, Korea). Ultrasonography of the tendons of the elbow was performed before the injection to plan the specific site for PRP and obtain baseline images. The severity of tendon pathology was assessed by ultrasonography as tear or no tear.
For PRP preparation, 20 mL venous blood was drawn from the antecubital vein using an aseptic technique and mixed with the anticoagulant citrate phosphate dextrose adenine (CPDA-1). The blood was subsequently placed into the PRP kit and centrifuged for 3 minutes at 3,200 rpm to separate it into platelet-poor plasma, red cells, and PRP. The platelet-poor plasma was extracted via a special port and discarded from the device. After blood was collected, 1.5 mL PRP was made and used for injection.
Using a sterile technique with a sterile probe cover, real-time ultrasound guidance was provided during the PRP injection procedure. A sterile field was set up and maintained throughout the procedure. Before PRP administration, single fenestration by 23-gauge needle was performed under ultrasound guidance into affected tendons at the lateral or medial epicondyle of the elbow. Needle tip was positioned at the region of tendinopathy and PRP (1.5 mL) was subsequently injected. Longitudinal ultrasound images during the injection were obtained to verify the injection site. Additional longitudinal and transverse ultrasonographic images were scanned 5 minutes after injection to assess the area of PRP distribution. The patients were instructed not to move their elbows or wrists until finishing additional ultrasonographic scan. To measuring the distribution distance after needle removed, the site of needle tip was marked on the skin during the injection.
Imaging analysis
Pre- and post-injection images were reviewed to evaluate PRP distribution independently by 2 authors with 19 and 9 years of musculoskeletal ultrasonography experience, respectively. Injected PRP was considered to be 1) aggregated within the tendon, 2) along the outer layer of tendon, or 3) diffused into the surrounding soft tissues or an adjacent joint after injection. The distribution of PRP was determined according to the presence of fluid or microbubbles after injection. The greatest distance was measured from needle tip to fluid/microbubbles. Intra-articular extension was defined by the presence of new microbubbles or fluid that was not present in pre-injection images.
Statistical analysis
SPSS version 18.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. The Mann–Whitney U-test was used to compare the distribution of injected PRP with respect to the location of the tendon or tendon pathology. The level of significance was set at p < 0.05.
Results
The study population comprised 39 patients including 15 male (38.5%) and 24 female(61.5%) patients with a mean age 49.3 years (range, 29–61 years). Three patients were excluded because steroid injections had been done to 2 patients and prolotherapy to one. There were 25 (64.1%) and 14 (35.9%) cases of tendinopathies in lateral and medial elbow, respectively. Mean symptom duration was 20.7 months (range, 6–28 months). Pre-injection ultrasonographic evaluation showed that there were 13 (33.3%) cases with tear and 26 (66.7%) cases with no tear.
All 39 cases were considered adequate for evaluating the distribution of injected PRP on ultrasonographic images. The ultrasonographic images verified the injected PRP within the common extensor/flexor tendon in all cases. Figure 1 shows ultrasound images of the common extensor tendon during the PRP injection procedure.
Figure 1.
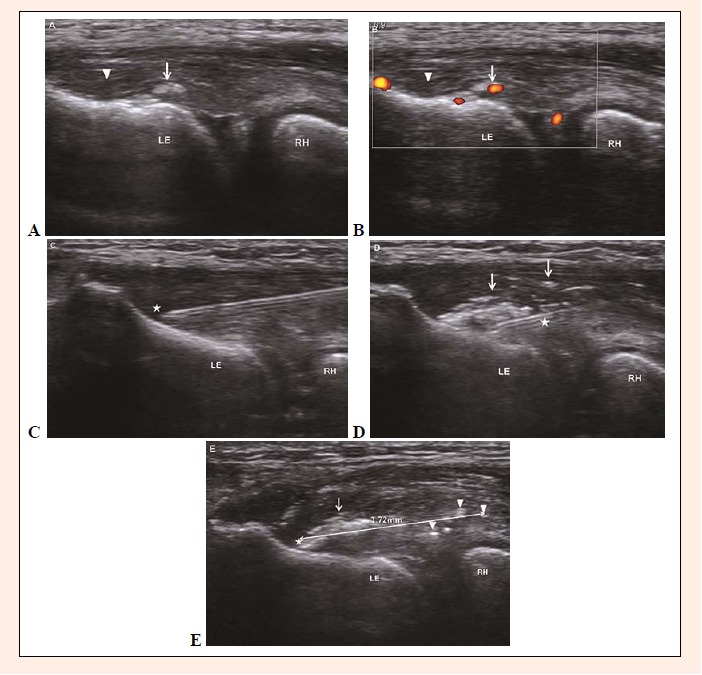
Ultrasonographic findings of the common extensor tendon in a 44-year-old woman during PRP injection
A. Longitudinal image showing amorphous hyperechoic calcification (arrow) and a partial-thickness tear (arrow head) in the common extensor tendon. B. Longitudinal power Doppler image showing increased vascularity around a calcification (arrow) and partial-thickness tear (arrow head) in the common extensor tendon. C. Longitudinal image showing the needle tip (star) located in the area of a partial-thickness tear. D. Post-injection ultrasonographic image showing injected PRP (arrow) spread within the tendon; the star indicates the injected needle. E. Image 5 minutes post-injection showing some of the injected PRP remaining (arrow) near the injection site (star) and the rest extending up to 1.72 mm (arrowhead) beyond injection site surrounding soft tissues. LE: lateral epicondyle of the humerus, RH: radius head.
The mean (± SD) distance of PRP from the injection site was 12.6 ± 5.7 mm (range, 5.0–26.0 mm). There was no significant difference in the mean distance between injections to the common extensor tendon (13.4 ± 5.6 mm) and common flexor tendon (11.9 ± 6.5 mm) (p = 0.604). The mean distance of PRP post-injection did not differ significantly in cases in which the tendon had torn (13.0 ± 4.3 mm) or not (12.9 ± 6.4 mm) (p = 0.588). Injected PRP spread to soft tissue outside the tendon in 20 of 39 cases. Intra-articular extension of injected PRP was observed in 5 cases; consisting of 3 cases had tendon tear and 2 had no tear, respectively (Figure 2).
Figure 2.
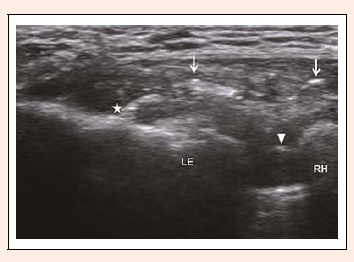
Intra-articular extension of injected PRP.
Longitudinal ultrasonographic image showing the injected PRP extending beyond the injection site (star) to the surrounding soft tissues (arrow) and within the elbow joint (arrowhead). LE: lateral epicondyle of the humerus, RH: radius head.
Discussion
In the present study, 1.5 mL injected PRP spread a mean of 12.6 mm from the injection site. And 20 out of 39 (51%) subjects showed soft tissue spread beyond tendon and even extension to joint space was observed in 5 out of 39 cases. There was no difference between common flexor tendon and common extensor tendon. Tendon tear did not affect the distance of distribution. These findings suggest that injected PRP tends not to stay at the injection site and rather diffuses away from it, regardless of the conditions such as kind of tendon, severity of tendon pathology, presence of inflammation. Similarly, in another study for chronic elbow tendinopathy, 3.5 mL injected PRP diffused > 20.0 mm from the injection site in most cases (48 of 49, 98%) and diffused into the adjacent soft tissue in 25 of 49 (51%) cases (Loftus et al., 2012). Although smaller volume (1.5 ml) of PRP was injected in present study such as previous study (Mishra and Pavelko, 2006; Peerbooms et al., 2010), the proportion of spread beyond tendon was similar with the study of Loftus et al. (2012) used 3.5 ml of volume.
Though in all cases fluid also remained at the injection site, some fluid diffuses out of the tendon in many cases indeed. The patients’ motion might be another explanation that the remaining fluid diffuses out of the tendon (so after 5 minutes in the present study). If the injected PRP spreads from target area like these results, we cannot evaluate the precise effect of injected PRP, because it is difficult to predict how many growth factors contained in PRP will stay in the degenerated area of the tendon. In order to administer sufficient growth factor with PRP injections, greater volume of PRP could be an option. However, greater volume can lead to further diffusion and require much more blood collection, which is undesirable. The solidification of PRP helps it remain at the injection site long enough to heal the damaged tendon of shoulder (Rha et al., 2013). Calcium chloride and bovine thrombin are combined with PRP to form a gel matrix; they are usually used in surgical applications for grafting or intra-articular injections (Sampson et al., 2008). If these exogenous activators can be used to treat tendinopathies of the elbow, the amount of growth factors maintained close to injection site could be potentially be maintained for a long time.
Loftus et al. (2012) showed that the injected PRP extended beyond the injection site and frequently diffused along the tendon or peritendinous soft tissues in their study. The authors had indicated that a single puncture may be adequate whereas a peppering technique performed in a blind injection was not necessary for extensive delivery (Loftus et al., 2012). The results of this study were very similar with ours; however they had focused on the efficiency of injection technique and concluded that single puncture was enough to deliver PRP rather than peppering technique in blind injection. In our study, we had used ultrasonographic injection technique and the accuracy of injection was regarded to be guaranteed. Therefore we had concentrated how far diffuse the injected PRP. Some studies have called into question the efficacy of PRP injections because the duration the platelets remain at the site after injection into the degenerated area was not enough and platelets were slowly activated by exposure to tendon collagen (Mishra et al., 2009) (de Vos et al., 2010). The pressure within the tendon may cause a large amount of PRP to diffuse rapidly out of the tendon, thereby reducing its effect (de Vos et al., 2010). As the results of our study, unexpected distribution of the injected PRP to extratendinous soft tissue or joint space can reduce the effect of PRP. As our knowledge, exogenous activators had not been used for chronic elbow tendinopathy. Therefore, further studies are required to verify the effects of exogenous activators in the treatment of tendinopathies of the elbow. The main limitations of the present study are the small sample size, and heterogeneity of the subjects. And another limitation is that the study is not controlled and that the follow-up period was very short. These limitations made that causal relationships cannot be determined. Further studies are required to confirm whether PRP spread after injection correlate with the clinical outcome, and how long the exogenous activator such as calcium chloride and bovine thrombin can keep the injected PRP within the target area.
Conclusion
Although PRP remained intratendinous after the injection in all cases, some portion tended to spread outside from the injection site in a short space of time. Postinjection ultrasonographic imaging has a value for observing the spreading patterns of intratendinous PRP injection.
Biographies

Gi-Young PARK
Employment
Professor, Department of Rehabilitation Medicine, Catholic University of Daegu School of Medicine, Daegu, Korea
Degree
MD, PhD
Research interest
Musculoskeletal pain, ultrasonography for musculoskeletal problem, post-stroke rehabilitation
E-mail: parkgy@cu.ac.kr

Dong Rak KWON
Employment
Professor, Department of Rehabilitation Medicine, Catholic University of Daegu School of Medicine, Daegu, Korea
Degree
MD, PhD
Research interest
Musculoskeletal pain, pediatric rehabilitation, post-stroke rehabilitation
E-mail: coolkwon@cu.ac.kr

Hee Kyung CHO
Employment
Professor, Department of Rehabilitation Medicine, Catholic University of Daegu School of Medicine, Daegu, Korea
Degree
MD
Research interest
Rehabilitation for rheumatic disease, spinal cord injury, cancer, and pulmonary rehabilitation
E-mail: hkcho@cu.ac.kr

Jinyoung PARK
Employment
Assistant Clinical Research Professor, Department of Rehabilitation Medicine, Gangnam Severance Hospital, Rehabilitation Institute of Neuromuscular Disease, Yonsei University College of Medicine, Seoul, Korea
Degree
MD
Research interest
Musculoskeletal pain, rehabilitation for spinal cord injury, post-stroke rehabilitation, electrodiagnostic medicine
E-mail: pjyblue511@gmail.com

Jung Hyun PARK
Employment
Associate Professor, Department of Rehabilitation Medicine, Gangnam Severance Hospital, Rehabilitation Institute of Neuromuscular Disease, Yonsei University College of Medicine, Seoul, Korea
Degree
MD, PhD
Research interest
Musculoskeletal pain, rehabilitation for spinal cord injury
E-mail: rmpjh@yuhs.ac
References
- Alsousou J., Thompson M., Hulley P., Noble A., Willett K. (2009) The biology of platelet-rich plasma and its application in trauma and orthopaedic surgery: a review of the literature. Journal of Bone and Joint Surgery British Volume 91(8), 987-996. [DOI] [PubMed] [Google Scholar]
- Anitua E. (1999) Plasma rich in growth factors: preliminary results of use in the preparation of future sites for implants. International Journal of Oral and Maxillofacial Implants 14(4), 529-535. [PubMed] [Google Scholar]
- de Vos R.J., Weir A., van Schie H.T., Bierma-Zeinstra S.M., Verhaar J.A., Weinans H., Tol J.L. (2010) Platelet-rich plasma injection for chronic Achilles tendinopathy: a randomized controlled trial. JAMA 303(2), 144-149. [DOI] [PubMed] [Google Scholar]
- Edwards S.G., Calandruccio J.H. (2003) Autologous blood injections for refractory lateral epicondylitis. The Journal of Hand Surgery 28(2): 272-278. [DOI] [PubMed] [Google Scholar]
- Everts P.A., Devilee R.J., Brown Mahoney C., van Erp A., Oosterbos C.J., Stellenboom M., Knape J.T., van Zundert A. (2008) Exogenous application of platelet-leukocyte gel during open subacromial decompression contributes to improved patient outcome. A prospective randomized double-blind study. European Surgical Research 40(2), 203-210. [DOI] [PubMed] [Google Scholar]
- Everts P.A., Jakimowicz J.J., van Beek M., Schanberger J.P., Devilee R.J., Overdevest E.P., Knape J.T., van Zundert A. (2007) Reviewing the structural features of autologous platelet-leukocyte gel and suggestions for use in surgery. European Surgical Research 39(4), 199-207. [DOI] [PubMed] [Google Scholar]
- Fenwick S.A., Hazleman B.L., Riley G.P. (2002) The vasculature and its role in the damaged and healing tendon. Arthritis Research & Therapy 4(4), 252-260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Foster T.E., Puskas B.L., Mandelbaum B.R., Gerhardt M.B., Rodeo S.A. (2009) Platelet-rich plasma: from basic science to clinical applications. The American Journal of Sports Medicine 37(11), 2259-2272. [DOI] [PubMed] [Google Scholar]
- Gosens T., Peerbooms J.C., van Laar W., den Oudsten B.L. (2011) Ongoing positive effect of platelet-rich plasma versus corticosteroid injection in lateral epicondylitis: a double-blind randomized controlled trial with 2-year follow-up. The American Journal of Sports Medicine 39(6), 1200-1208. [DOI] [PubMed] [Google Scholar]
- Hayem G. (2001) Tenology: a new frontier. Joint, Bone, Spine: Revue du Rhumatisme 68(1), 19-25. [DOI] [PubMed] [Google Scholar]
- Krogh T.P., Bartels E.M., Ellingsen T., Stengaard Pedersen K., Buchbinder R., Fredberg U., Bliddal H., Christensen R. (2013) Comparative effectiveness of injection therapies in lateral epicondylitis: a systematic review and network meta-analysis of randomized controlled trials. The American Journal of Sports Medicine 41(6), 1435-1446. [DOI] [PubMed] [Google Scholar]
- Loftus M.L., Endo Y., Adler R.S. (2012) Retrospective analysis of postinjection ultrasound imaging after platelet-rich plasma or autologous blood: observational review of anatomic distribution of injected material. American Journal of Roentgenology 199(4), W501-W505. [DOI] [PubMed] [Google Scholar]
- Marx R.E., Carlson E.R., Eichstaedt R.M., Schimmele S.R., Strauss J.E., Georgeff K.R. (1998). Platelet-rich plasma: growth factor enhancement for bone grafts. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology 85(6), 638-646. [DOI] [PubMed] [Google Scholar]
- Mishra A., Pavelko T. (2006) Treatment of chronic elbow tendinosis with buffered platelet-rich plasma. The American Journal of Sports Medicine 34(11), 1774-1778. [DOI] [PubMed] [Google Scholar]
- Mishra A., Woodall J., Vieira A. (2009) Treatment of tendon and muscle using platelet-rich plasma. Clinics in Sports Medicine 28(1), 113-125. [DOI] [PubMed] [Google Scholar]
- Molloy T., Wang Y., Murrell G. (2003) The roles of growth factors in tendon and ligament healing. Sports Medicine 33(5), 381-394. [DOI] [PubMed] [Google Scholar]
- Nguyen R.T., Borg-Stein J., McInnis K. (2011) Applications of platelet-rich plasma in musculoskeletal and sports medicine: an evidence-based approach. Physical Medicine & Rehabilitation 3(3), 226-250. [DOI] [PubMed] [Google Scholar]
- Peerbooms J.C., Sluimer J., Bruijn D.J., Gosens T. (2010) Positive effect of an autologous platelet concentrate in lateral epicondylitis in a double-blind randomized controlled trial platelet-rich plasma versus corticosteroid injection with a 1-year follow-up. The American Journal of Sports Medicine 38(2), 255-262. [DOI] [PubMed] [Google Scholar]
- Radice F., YÃnez R., GutiÃrrez V., Rosales J., Pinedo M., Coda S. (2010) Comparison of magnetic resonance imaging findings in anterior cruciate ligament grafts with and without autologous platelet-derived growth factors. Arthroscopy: The Journal of Arthroscopic & Related Surgery 26(1), 50-57. [DOI] [PubMed] [Google Scholar]
- Rha D., Park G., Kim Y., Kim M.T., Lee S.C. (2013) Comparison of the therapeutic effects of ultrasound-guided platelet-rich plasma injection and dry needling in rotator cuff disease: a randomized controlled trial. Clinical Rehabilitation 27(2), 113-122. [DOI] [PubMed] [Google Scholar]
- Sampson S., Gerhardt M., Mandelbaum B. (2008) Platelet rich plasma injection grafts for musculoskeletal injuries: a review. Current reviews in Musculoskeletal Medicine 1(3-4), 165-174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tabata Y. (2004) Tissue regeneration based on tissue engineering technology. Congenital Anomalies 44(3), 111-124. [DOI] [PubMed] [Google Scholar]