

Abstract
The prevention of type 2 diabetes in persons at risk for diabetes is of utmost importance. Physical activity in general and even exercises at moderate intensities such as walking significantly reduce the risk of the development of type 2 diabetes. However, it is still a matter of debate whether lipids and glucose metabolism are differently affected by regular concentric (e.g., uphill walking) and eccentric (e.g., downhill walking) endurance exercise. The aim of this study was to investigate the effects of short-term (3 weeks) uphill and downhill walking on glucose metabolism and blood lipids in pre-diabetic middle-aged men in a real world setting. The study was designed as an investigator-initiated 2 group random selection pre-test post-test trial. Sixteen pre-diabetic men (age: 56.9 ± 5.1 years; BMI: 28.1 ± 2.3 kg·m-2) performed 9 uphill (n = 8) or 9 downhill (n = 8) walking sessions within 3 weeks. The primary outcomes were the markers of glucose metabolism and blood lipids measured before and after the training period. After uphill walking glucose tolerance (area under the curve of the oral glucose tolerance test: -43.25 ± 53.12 mg·dl-1; p = 0.05; effect size: 0.81), triglycerides (-48.75 ± 54.49 mg·dl-1; p = 0.036; effect size: 0.89), HDL-C (+7.86 ± 9.54 mg·dl-1; p = 0.05; effect size: 0.82) and total cholesterol/HDL-C ratio (-0.58 ± 0.41; p = 0.012; effect size: 1.39) had significantly improved. No significant metabolic adaptations were found after downhill walking. However, when adjusted for estimated energy expenditure, uphill and downhill walking had equal effects on almost all metabolic parameters. Moreover, the magnitude of the baseline impairments of glucose tolerance was significantly related to the extent of change in both groups. Depending on the fitness level and individual preferences both types of exercise may be useful for the prevention of type 2 diabetes and disorders in lipid metabolism.
Key points.
In contrast to downhill walking, 3 weeks of uphill walking effectively improved glucose tolerance and most of the measured lipid markers in pre-diabetic men
However, when considering the related estimated energy expenditure both types of walking could possibly have equal effects
Moreover, persons with more pronounced impairments of the glucose metabolism benefited from both training regimens
Thus, depending on the fitness level and individual preferences both types of exercise may be useful for the prevention of type 2 diabetes and disorders in lipid metabolism
Key words: Impaired glucose tolerance, concentric exercise, eccentric exercise, insulin resistance
Introduction
The WHO projects diabetes to be the 7th leading cause of death in 2030 (Mathers et al., 2006). Type 2 diabetes develops most often in middle-aged or older adults and is a risk factor for other diseases such as heart attacks, strokes, diabetic retinopathy, diabetic neuropathy and kidney failure. Lifestyle changes focusing on weight reduction, eating habits and physical activity can reduce the risk of type 2 diabetes by 58% (Eriksson et al., 1999; Tuomilehto et al., 2001). Among these factors physical activity seems to have the highest protective effect for individuals at highest risk of developing type 2 diabetes (Ivy, 1997). Even exercise at moderate intensities such as walking significantly reduces the risk of the development of type 2 diabetes (Jeon et al., 2007). Besides impairments in glucose metabolism, type 2 diabetes is associated with dyslipidemia, especially with lower high-density lipoprotein-cholesterol (HDL-C) levels and higher very-low-density lipoprotein (VLDL-C) levels, increasing the cardiovascular risk in this population (Taskinen, 2002).
There is general agreement that exercise training results in improved insulin sensitivity and glucose tolerance in healthy subjects as well as in persons suffering from type 2 diabetes (Hansen et al., 2010; Jensen et al., 2011; Sigal et al., 2007; Snowling et al., 2006). Moreover, aerobic as well as resistance exercise reportedly improved blood lipids (Durstine et al., 2001; Gordon et al., 2014; Kelley and Kelley, 2009; Kodama et al., 2007; Slentz et al., 2007).
While a single bout of concentric endurance exercise (CE = muscle shortening contraction form) is generally associated with improved insulin action and glucose transport (Wojtaszewski et al., 2002), unaccustomed muscle damaging eccentric endurance exercise (EE = muscle lengthening contraction form) is associated with reduced glucose transporter type 4 (GLUT4) levels that seem to be the major reason for transient insulin resistance (Asp et al., 1995; Jensen and Richter, 2012; Richter and Hargreaves, 2013). In contrast, a single bout of not muscle damaging EE was associated with energy dependent positive changes of glucose tolerance in young and healthy subjects (Philippe et al., 2016).
Only a few studies have investigated metabolic adaptations to regular eccentric exercise (Drexel et al., 2008; Marcus et al., 2009; Paschalis et al., 2010; 2011; Zeppetzauer et al., 2013). Pre-diabetic persons could benefit from regular eccentric exercise since regular eccentric resistance exercise and regular downhill walking were associated with a significant decrease of LDL-C and IR as well as an increased glucose tolerance in healthy men and women (Drexel et al., 2008; Marcus et al., 2009; Paschalis et al., 2010; Paschalis et al., 2011). When considering estimated energy expenditure, the positive adaptations to glucose tolerance after prolonged downhill walking seem to be superior to those elicited by prolonged uphill walking (Zeppetzauer et al., 2013). However, Marcus et al. (2009) failed to demonstrate positive adaptations with regard to insulin sensitivity after 12 weeks of eccentric ergometer training in women with impaired glucose tolerance. Thus, the effects of EE on glucose metabolism remain controversial and may depend on the characteristics of the individual and the type of EE performed.
Data on the distinct effects of glucose metabolism and lipid profiles due to regular CE and EE are scarce but would be of utmost importance considering the increasing number of persons suffering from impaired glucose tolerance or diabetes. The aim of this study was to investigate the effects of short-term (3 weeks) uphill and downhill walking in a real world setting (e.g. summer holidays in the Alps) on glucose metabolism and blood lipids in pre-diabetic men. We hypothesized that both CE and EE would elicit beneficial effects on glucose and lipid metabolism in pre-diabetic men but likely in a manner dependent upon the energy expenditure.
Methods
Study participants
Based on the study of Smutok et al. (1994) which investigated the area under the oral glucose tolerance curve after exercise training, a total sample size of n = 16 for 80% power has been calculated (G*Power, Version 3.1.5). 13 local physicians were involved in the recruitment process. 16 middle-aged male pre-diabetic participants (aged between 50 and 67 years) living in or close to Innsbruck gave their written informed consent to participate in the study. The inclusion criterion was a diagnosed increased risk for diabetes (pre-diabetes) as defined by the American Diabetes Association (American Diabetes Association, 2015). We enrolled patients with impaired fasting glucose [defined as: IFG: fasting plasma glucose 100 mg·dl-1 (5.6 mmol·l-1) to 125 mg · dl-1 (6.9 mmol·l-1)] and/or impaired glucose tolerance [IGT: 2-h plasma glucose in the 75-g oral glucose tolerance test 140 mg·dl-1 (7.8 mmol·l-1) to 199 mg·dl-1 (11.0 mmol·l-1)] not receiving glucose metabolism relevant medication. Exclusion criteria were any other kind of acute or chronic disease, smoking, BMI > 30 kg·m-2. After stratification for fasting glucose and the 2-hours value of the oral glucose tolerance test the subjects were randomly assigned to the CE (= uphill walking) or the EE (= downhill walking) group. The study was carried out in conformity with the ethical standards laid down in the declaration of Helsinki and the protocol was approved by the ethics committee of the Medical University of Innsbruck (Protocol ID: AN5029; ClinicalTrials.gov ID: NCT01890876)
Study protocol
Throughout the manuscript we use the terms eccentric and concentric exercise for downhill and uphill walking. This is justifiable as the leading as well as the trailing leg do not perform any positive, respectively negative mechanical work when walking downhill or uphill at a grade of ± 6° (i.e. ± 10.51 %) (Franz et al. 2012).
The study was conducted with one group of 8 participants (4 CE, 4 EE) in spring 2013 and with another 8 participants in fall 2013 (4 CE, 4 EE). The study consisted of 2 pre-test days, 9 uphill (CE) or downhill (EE) walking sessions and 2 post-test days. On the first pre-test day the subject appeared in a fasting state and underwent routine examination, anthropometric measurements, venous blood sampling and an oral glucose tolerance test (OGTT). On the second pre-test day the subjects performed incremental exercise testing (cycle ergometer test). The exercise program started 1 week after the second pre-test day. The 9 walking sessions were performed on Mondays, Wednesdays and Fridays of 3 consecutive weeks. Exercise testing after the training program was conducted on the same day as the last walking session. Metabolic (OGTT and blood sampling) and anthropometric post-tests took place 1-2 days after the last walking session.
Routine examination and anthropometric measurements
Each participant underwent routine medical examination including medical history, health status, red and white blood cell count and ECG. Stature and body mass were assessed using standard techniques. A tetrapolar multi-frequency bioelectrical impedance analysis (BIA-101, RJL/Akern Systems, Clinton Township, MI, USA) was used to determine the percentage of lean body mass, body cell mass, muscle mass and fat mass. The device was calibrated every morning using the standard control circuit supplied by the manufacturer with a known impedance (resistance (R) = 380 V; reactance (Xc) =47 V). The accuracy of the device was 1% for R and 1% for Xc.
Exercise capacity
Exercise capacity was assessed on a cycle ergometer (Excalibur Sport, Lode, the Netherlands) by an incremental spiro-ergometry (Oxycon Alpha, Jaeger, Germany). We expected a peak performance of our study participants between 150 and 200 watts. Since the recommended duration for incremental exercise tests to exhaustion is generally between 8 and 12 min we decided to start with an initial load of 50 W for 3 min followed by 50 W increments every 3 min up to exhaustion, resulting in total test duration of 9 to 12 min. During the test the participants were continuously monitored by ECG (Schiller AT-10, Austria).
Measurements of glucose and lipid metabolism
Fasting venous blood samples were taken to assess approximated insulin resistance pre- and post-test by using the homeostasis model assessment (HOMA = fasting insulin (tU·ml-1) · fasting glucose (mg·dl-1) / 405) (Matthews et al., 1985). Additionally, markers of lipid metabolism were determined pre- and post-test from fasting venous blood samples. All parameters were assessed using standard procedures at the laboratory of the Medical University of Innsbruck. Plasma glucose was quantified using a commercially available enzymatic kit (Roche Diagnostic Systems, Basel, Switzerland) on a Hitachi 902 autoanalyzer (Roche Diagnostic Systems, Basel, Switzerland). Insulin was determined using automated analyzers within the central clinical laboratory at the University Hospital Innsbruck based on a Quantikine Human Insulin 4.5 hour solid-phase enzyme linked immunosorbent assay (ELISA; R&D Systems, Inc. Minneapolis, USA) following the manufacturer’s instructions. LDL-C and VLDL-C were calculated by the Friedewald formula (Friedewald et al., 1972). Glucose tolerance was assessed via an oral glucose tolerance test (OGTT). Participants had to drink 75 g glucose dissolved in 300 ml of water. Capillary blood samples were drawn and analyzed before (fasting), 1 hour and 2 hours after ingestion (Biosen C-Line, Germany). The total area under the curve (AUC) of the OGTT was calculated with the trapezoidal rule as proposed by Le Floch et al. (1990).
CE and EE training sessions
Three times per week for 3 weeks, the subjects performed supervised training sessions of uphill or downhill walking on a standardized path at low altitude. The exercise intensity was regulated over the rate of perceived exertion defined by BORG RPE scale (Borg, 1970). The CE participants were asked to walk at a maximum intensity corresponding to RPE 15. The EE participants were asked to walk as fast as possible or at a maximum intensity corresponding to RPE 15 but without running. During the walking sessions, the participants were only allowed to drink water. The starting point for the CE group was 850 m above sea level and the finish point 1360 m above sea level. The path had a relatively continuous slope of 10.2 % and a length of 5000 m. Each participant covered 45000 horizontal and 4590 vertical meters over the 9 walking sessions. The EE group walked the same path as the CE group but in the opposite direction. Both groups were brought to their starting point by car.
Measurements during walking
The heart rate and walking time of each participant was monitored and stored for every walking session by a Polar watch (RS800CX, Polar Electro OY, Kempele, Finland). The average rate of perceived exertion was noted after each walking session. At the beginning of each walking session delayed onset muscle soreness (DOMS) of the previous walking session was assessed via a graded scale for muscle-pain and muscle-soreness, ranging from 1-10 (1 meaning no pain/soreness and 10 meaning maximal pain/soreness).
Estimated energy expenditure during walking
Knowing the walking time, walking distance, slope gradient and the body mass of a participant we calculated his average VO2 using a formula elaborated by Kramer (2010): mlO2·s-1 = 5.4V2 + 0.37M + 0.0054MGV +0.011G2V - 3.8X – 17 (V = velocity [m · s-1]; M = body mass [kg]; G = gradient [%]; X = gender [0 = female, 1 = male]).
Assuming a respiratory quotient (RQ) of 0.85 we calculated the caloric equivalent for O2 and the mean estimated energy expenditure per walking session and the total estimated energy expenditure during the study.
Statistical analysis
Due to the relatively small sample size non-parametric statistical tests were used (IBM, SPSS Statistics, Version 20). Changes from pre-test to post-test within each group were calculated with Wilcoxon Matched Pairs Test. Interactions (time x group) between CE and EE were computed from the differences of post-test minus pre-test values with Mann-Whitney U-Test. Differences of training data between CE and EE were calculated with Mann-Whitney U-Test. Relations between metabolic parameters were calculated with Pearson product-moment correlation coefficient. The effect sizes were quantified using Cohen’s d (small effect size: 0.2 ≤ d < 0.5; medium effect size: 0.5 ≤ d < 0.8; large effect size 0.8 ≤ d). Statistical significance was set at p ≤ 0.05.
Results
Baseline anthropometric and performance characteristics of the participants are presented in Table 1.
Table 1.
Baseline anthropometric and performance characteristics of the study participants. Data are means (±SD).
| CE (n = 8) | EE (n =8) | |
|---|---|---|
| Age, years | 56.4 (5.3) | 57.4 (5.1) |
| Height, m | 1.77 (.07) | 1.73 (.04) |
| Body mass, kg | 88.1 (11.7) | 84.0 (9.7) |
| BMI, kg·m-2 | 28.0 (1.6) | 28.2 (3.0) |
| Lean body mass, kg | 65.0 (6.0) | 62.4 (7.6) |
| Body cell mass, kg | 36.8 (2.6) | 35.1 (5.9) |
| Fat mass, kg | 23.1 (7.6) | 21.6 (4.4) |
| Muscle mass, kg | 45.0 (3.3) | 42.9 (6.7) |
| Physical activity, h·week-1 | 4.5 (2.8) | 5.9 (3.8) |
| Systolic BP, mm Hg | 131.5 (14.1) | 129.0 (13.6) |
| Diastolic BP, mm Hg | 85.9 (3.8) | 81.0 (8.0) |
| Hfmax, bpm | 154.9 (23.4) | 153.1 (15.7) |
| Pmax, W | 191.0 (22.9) | 173.8 (42.2) |
CE: concentric exercise (uphill walking); EE: eccentric exercise (downhill walking); BMI: Body mass index; Hfmax: maximum heart frequency reached during exercise capacity testing; BP: blood pressure; Pmax: maximum power reached during exercise capacity testing; No significant group difference (calculated with Mann-Whitney U-Test)
Each of the 16 participants completed all 9 walking sessions. No metabolic baseline parameter differed significantly between CE and EE (Table 2).
Table 2.
Baseline metabolic values of the CE and the EE group. Data are means (±SD).
| CE (n = 8) | EE (n =8) | |
|---|---|---|
| AUC, mmol·l-1·h-1 | 17.91 (3.86) | 16.41 (6.69) |
| Plasma glucose, mmol·l-1 | 6.85 (.83) | 6.70 (1.75) |
| Insulin, pmol·l-1 | 66.59 (29.04) | 83.95 (64.03) |
| HOMA-IR | 2.90 (1.28) | 3.92 (3.51) |
| Total cholesterol, mmol·l-1 | 5.33 (.98) | 4.74 (1.09) |
| Triglycerides, mmol·l-1 | 1.89 (1.04) | 1.51 (.99) |
| HDL-C, mmol·l-1 | 1.17 (.16) | 1.12 (.26) |
| LDL-C, mmol·l-1 | 3.30 (1.01) | 2.94 (.93) |
| LDL-C/HDL-C ratio | 2.84 (.88) | 2.74 (.93) |
| TC/HDL-C ratio | 4.57 (.83) | 4.39 (1.15) |
| CK, µkat·l-1 | 2.48 (.93) | 3.05 (3.72) |
CE: concentric exercise (uphill walking); EE: eccentric exercise (downhill walking); AUC: area under the curve of the oral glucose tolerance test; HOMA-IR: homeostasis model assessment of insulin resistance; HDL-C: high-density lipoprotein-cholesterol; LDL-C: low-density lipoprotein-cholesterol; TC: total cholesterol; CK: creatine kinase; No significant group difference (calculated with Mann-Whitney U-Test)
Responses to the exercise program
The walking time, heart rate, oxygen uptake, estimated energy expenditure and RPE were significantly higher during CE than EE. However, there was no significant difference of muscle pain and soreness after CE compared to EE (Table 3).
Table 3.
Walking session results. Data are means (±SD).
| CE (N = 8) | EE (N = 8) | |
|---|---|---|
| Mean walking time pws, s | 4496.3 (365.9) * | 4070.7 (278.7) |
| Mean walking speed pws, m·s-1 | 1.1 (0.1) * | 1.2 (0.1) |
| Mean VO2rel pws, ml·kg-1·min-1 | 17.1 (1.6) *** | 10.1 (1.0) |
| Mean rel. e.e. pws, kJ·kg-1·min-1 | 0.35 (0.03) *** | 0.21 (0.02) |
| Mean absolute e.e. pws, kJ | 2309.5 (470.2) *** | 1177.0 (245.7) |
| Total e.e., kJ | 20785.0 (4232.2) *** | 10593.1 (2211.6) |
| Hfmean, bpm | 126.6 (9.8) *** | 92.8 (10.2) |
| RPEmean, 6-20 | 13.4 (0.6) *** | 8.8 (1.4) |
| Pain mean, 1-10 | 1.3 (0.3) | 1.1 (0.1) |
| Soreness mean, 1-10 | 1.4 (0.4) | 1.2 (0.2) |
CE: concentric exercise (uphill walking); EE: eccentric exercise (downhill walking); pws: per walking session; VO2rel: relative oxygen uptake; e.e.: estimated energy expenditure; Hfmean: mean heart frequency; RPEmean: mean rate of perceived exertion
* and *** denote p < 0.05 and p < 0.001, respectively, between group differences (calculated with Mann-Whitney U-Test).
Anthropometric and performance characteristics before and after 3 weeks of exercise
The maximum heart rate reached during the exercise capacity test increased significantly from pre-test to post-test in the CE group (154.9 ± 23.5 vs. 163.3 ± 14.9 bpm; p = 0.028; effect size: 0.80) but not in the EE group (153.1 ± 15.7 vs. 151.3 ± 20.8 bpm; p = 0.752). No other parameter reached significance and no interaction (time x group) was found for any parameter (Table 4).
Table 4.
Mean differences of anthropometric and exercise capacity post-test values minus metabolic pre-test values. Data are means (±SD).
| CE (N = 8) | EE (N = 8) | |
|---|---|---|
| Body mass, kg | -.7 (1.2) | -.2 (1.0) |
| Lean body mass, kg | -.9 (2.3) | .2 (.8) |
| Body cell mass, kg | .2 (1.0) | .7 (1.4) |
| Muscle mass, kg | .1 (1.3) | .8 (1.4) |
| Fat mass, kg | .2 (1.5) | -.4 (.9) |
| Hfmax, bpm | 8.4 (10.5) * | .7 (8.8) |
| Pmax, W | 10.3 (18.0) | 3.4 (15.7) |
CE: concentric exercise (uphill walking); EE: eccentric exercise (downhill walking); Hfmax: maximum heart rate reached during exercise capacity testing; Pmax: maximum power; n.s.: not significant
* p < 0.05 within group change (calculated with Wilcoxon test).
Metabolic parameters before and after 3 weeks of exercise
Glucose tolerance improved significantly (area under the curve (AUC); OGTT1) after CE but not after EE. Triglycerides and TC/HDL-C ratio significantly decreased and HDL-C significantly increased after CE but not after EE. LDL-C/HDL-C ratio tended to decreased after EE but not after CE. No significant interaction (time x group) was found for any parameter (Table 5).
Table 5.
Mean differences of metabolic post-test values minus pre-test values. Data are mean (±SD).
| CE (n = 8) | Effect size | EE (N = 8) | Effect size | |
|---|---|---|---|---|
| AUC, mmol · l-1 · h-1 | -2.40 (2.95) * | .81 | -.70 (2.83) | - |
| Fasting plasma glucose, mmol · l-1 | -.51 (1.12) | - | -.19 (1.95) | - |
| Insulin, pmol · l-1 | 2.69 (37.42) | - | 5.95 (52.15) | - |
| HOMA-IR | .04 (1.81) | - | -.10 (2.84) | - |
| Total cholesterol, mmol · l-1 | .08 (.75) | - | -.15 (.60) | - |
| Triglycerides, mmol · l-1 | -.56 (.62) * | .89 | .05 (.62) | - |
| HDL-C, mmol · l-1 | .20 (.25) * | .82 | .11 (.33) | - |
| LDL-C, mmol · l-1 | .13 (.67) | - | -.28 (.41) | - |
| LDL-C/HDL-C ratio | -.30 (.52) | - | -.47 (.70) | .67 |
| TC/HDL-C ratio | -.57 (.41) * | 1.39 | -.53 (.98) | - |
| CK, µkat · l-1 | .44 (1.68) | - | .44 (1.94) | - |
CE: concentric exercise (uphill walking); EE: eccentric exercise (downhill walking); AUC: area under the curve of the oral glucose tolerance test; HOMA-IR: homeostasis model assessment of insulin resistance; HDL-C: high-density lipoprotein-cholesterol; LDL-C: low-density lipoprotein-cholesterol; TC: total cholesterol; CK: creatine kinase
* p < 0.05 within group change (calculated with Wilcoxon test).
Pre-test to post-test metabolic changes as a function of estimated energy expenditure
When the changes from pre-test to post-test were divided by the total estimated energy expenditure over the 9 walking session no significant difference were found between CE and EE for fasting plasma glucose (-0.02 ± 0.05 vs. -0.01 ± 0.19 mmol·l-1·MJ-1; p = 1.000), AUC (-0.11 ± 0.13 vs. -0.08 ± 0.27 mmol·l-1·h-1·MJ-1; p = 0.345), insulin (-0.01 ± 1.79 vs. 0.28 ± 4.09 pmol·l-1·MJ-1; p = 0.817 ), HOMA (-4.18· 0-3 ± 8.32·10-2 vs. -1.86·10-2 ± 0.24 per MJ; p = 0.908); triglycerides (-0.03 ± 0.04 vs. 0.01 ± 0.06 mmol·l-1·MJ-1; p = 0.203), total cholesterol (2.33·10-3 ± 0.03 vs. -0.02 ± 0.05 mmol·l-1·MJ-1; p = 0.418 ) HDL-C (0.01 ± 0.02 vs. 0.01 ± 0.03 mmol·l-1·MJ-1; p = 0.643), LDL-C/HDL-C ratio (-1.61·10-2 ± 3.02·10-2 vs. -3.91·10-2 ± 6.23·10-2 per MJ; p = 0.203), TC/HDL-C ratio (-3.02·10-2 ± 2.63·10-2 vs. -4.11·10-2 ± 8.62·10-2 per MJ; p = 0.298). However the decrease of LDL-C tended to be more pronounced after EE than after CE (-0.03 ± 0.04 vs. 0.01 ± 0.03 mmol·l-1·MJ-1; p =0.083; effect size: 0.99.
Correlations between metabolic parameters
There was a significant negative correlation between the pre-test AUC and the AUC difference (post-test minus pre-test) in the CE group (r = -0.728; p = 0.041) and in the EE group (r = -0.730; P = 0.040) (Figure 1 and Figure 2).
Figure 1.
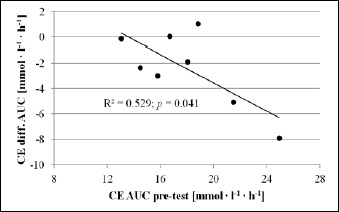
Relationship between AUC baseline values and AUC change (post-test minus pre-test) of the CE group. CE: concentric exercise (uphill walking); AUC: area under the curve of the oral glucose tolerance test
Figure 2.
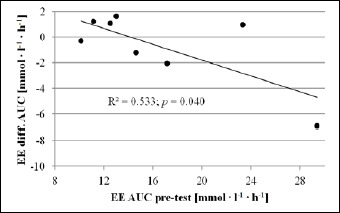
Relationship between AUC baseline values and AUC change (post-test minus pre-test) of the EE group. EE: eccentric exercise (downhill walking); AUC: area under the curve of the oral glucose tolerance test
There was a positive correlation between the decrease of TG and AUC for the entire group (r = 0.682; p = 0.005) and for EE (r = 0.857; p = 0.014) but not for CE.
Discussion
The main findings of this study are as follows. First, uphill walking effectively improved glucose tolerance in pre-diabetic men while downhill walking did not. However, when adjusted for estimated energy expenditure, uphill and downhill walking had equal effects on all metabolic parameters. Secondly, high baseline values of the AUC were the best predictor for improvements in glucose tolerance independent of the intervention.
Our findings do not confirm the results of prior studies which showed that downhill walking is equally or even more effective in improving glucose tolerance when compared to uphill walking (Drexel et al., 2008; Zeppetzauer et al., 2013). Although we found no interaction between CE and EE regarding changes of glucose tolerance, only CE lead to significant changes of the glucose tolerance. When adjusted for estimated energy expenditure, CE an EE have been equally effective but no superior effects of EE could be found as reported before (Zeppetzauer et al., 2013).
The overall metabolic changes seen after 3 weeks of supervised training in pre-diabetic men were much lower than found by Drexel et al. (2008) after 3 times per week exercise for 8 weeks in healthy subjects. Although using a comparable walking path but a shorter training period and a different population than Drexel et al. (2008), our results do not indicate that superior effects of EE on any parameter of the glucose metabolism could be expected after a longer training regimen.
The approximated insulin resistance remained nearly unchanged after 3 weeks of exercise with 3 training sessions per week. This result is in agreement with Marcus et al. (2009) who investigated the effects of regular EE on insulin sensitivity in pre-diabetic women using an eccentric ergometer 3 times per week for 12 weeks and performing hyperinsulinemic-euglycemic clamps. In contrast, Paschalis et al. (2011) found a reduced HOMA index after 8 trainings sessions over 8 weeks on an isokinetic dynamometer after EE but not after CE and Drexel et al. (2008) found significant reductions of approximated insulin resistance after CE and EE in healthy subjects. These findings may suggests that the effectiveness of EE in modulating insulin resistance and sensitivity is perhaps less pronounced in pre-diabetic than in healthy persons.
Despite the unaltered insulin resistance after both exercise modes, the AUC significantly improved after CE. This could be explained by an enhanced insulin independent glucose transport mediated via energy dependent (e.g. interleukin 6) and mechanical stress dependent (e.g. GTPase Rac1) pathways (Carey et al., 2006; Sylow et al., 2015). However further investigation is needed to confirm such assumptions.
In contrast to Drexel et al. (2008), where HDL-C remained unchanged after CE and EE, we found a significant rise of HDL-C cholesterol and a significant decrease of TC/HDL-C ratio after CE but not after EE. Even if the results are still controversial, high volume aerobic exercise, especially with an energy expenditure exceeding 1200 kcal/wk is often associated with elevations in HDL-C levels (Durstine et al., 2001; Kodama et al., 2007; Slentz et al., 2007). Our CE group averaged an estimated energy expenditure of approximately 1654 kcal/wk whereas the EE group averaged approximately 843 kcal/wk. On the one hand, uphill walking as performed by our CE group is more comparable to “classic” aerobic exercise than downhill walking. The higher energy expenditure and the characteristics of CE may be reasons for the higher effectiveness in elevating HDL-C levels compared to EE. On the other hand, downhill walking induces high strain on the muscle while the metabolic cost is relatively low compared to level or uphill walking (Camillo et al., 2015; Johnson et al., 2002). EE may therefore be more comparable to a resistance endurance training than to aerobic exercise. Resistance training and low volume and intensity aerobic exercise are associated with LDL-C lowering without influencing HDL-C (Gordon et al., 2014; Kelley, 2004; Kelley and Kelley, 2009; Slentz et al., 2007). Both features apply to downhill walking which may explain that EE tended to decrease LDL-C/HDL-C ratio that was mostly affected by a not significant but still important decrease of LDL-C without changing HDL-C. When adjusted for estimated energy expenditure, the decrease of LDL-C even tended to be more pronounced after EE than after CE.
TG was significantly lowered by CE but not by EE. Aerobic exercise is commonly related to triglyceride decreases in men (Durstine et al., 2001; Gordon et al., 2014). The higher aerobic component and higher energy expenditure of CE compared to EE may explain the superior effects of CE on TG (Durstine et al., 2001).
As type 2 diabetes is associated with dyslipidemia and an increased cardiovascular risk (Taskinen, 2002), persons at risk for diabetes benefit from an improved lipid profile which is confirmed by the correlation between the decrease of TG and AUC. Our findings suggest that CE is more effective in improving HDL-C and TG levels while EE may be more effective in improving LDL-C levels. Unfortunately the improvements of lipid profile did not result in significant changes of IR. Because insulin resistance (IR) is closely related to oxidized LDL-C and an increased HDL-C catabolism (Linna et al., 2015; Pont et al., 2002), we may assume that the concentration changes of lipids seen after CE and EE did not result in changes of HDL-C and LDL-C metabolism. Type 2 diabetes and dyslipidemia are commonly associated (Taskinen, 2002) and the correlation between TG and AUC confirms the close relationship between decreases of impaired glucose tolerance and dyslipidemia.
Figures 1 and 2 illustrate that positive change of the glucose tolerance seen after CE and EE are the highest in persons with higher baseline values. The negative correlations found between the baseline AUC value and the extent of change after the training intervention in both groups confirm that high baseline values were the best predictor for improvements independent of the intervention. Our results are not consistent with the observations of Solomon et al. (2013) who found that improvements of glycemic control were negatively influenced by high pre-training hyperglycemia after a 12 to 16-week aerobic exercise training period in type 2 diabetes patients. A recent meta-analysis by Ishiguro et al. (2016) showed that resistance training using high set numbers was the most effective strength training strategy to reduce glycosylated hemoglobin (HbA1c) in type 2 diabetes patients. Additionally, outcomes where positively influenced by a short medical history of type 2 diabetes and by high baseline HbA1c levels. Both walking downhill and uphill are mixed forms of aerobic and strength endurance exercises. When considering that our participants were pre-diabetic, without any medical history of type 2 diabetes, the mixed exercise form and presumably higher HbA1c levels in the participants with higher IFG and/or IGT, might explain the negative correlations found between the baseline AUC value and the extent of change after the training intervention.
However, even if we did not find significant interactions between CE and EE and no significant correlations between the estimated energy expenditure and metabolic changes, the results still indicate that the higher metabolic cost of CE was at least co-responsible for the effectiveness of CE compared to EE. For example, AUC improved in 6 out of 8 persons after CE but only in 4 out of 8 persons after EE.
Moreover, our data suggest that there might be responders and non-responders to both training regimens.
Maximum heart rate during exercise capacity testing significantly increased in the CE but not in the EE group. As uphill walking was more intensive than downhill walking (see Table 4), we might assume that exercise tolerance increased after uphill walking allowing the participants to better explore their exercise capacity and thus, heart rate limits.
Limitations
The relatively small sample size may be considered as a limitation. However, the a priori sample size calculation suggested a minimum of 8 participants per group. Without any drop-outs this goal could be achieved and a sufficient sample size is also supported by the large effect sizes demonstrated for all significant metabolic adaptations. Moreover, our findings related to estimated energy expenditure should outweigh a potential sample size issue. Another limitation may arise from placing the post-test close to the last training session. This could have led to an overestimation or an underestimation of certain metabolic changes. Furthermore, we neither monitored diet and caloric intake nor physical activity patterns during the study phase. Although we explicitly asked the study participants not to change their eating, drinking or physical activity habits during the study period, we cannot entirely rule out that additional life style changes might have influenced our results. Although our data do not suggest that downhill walking may become more effective than uphill walking when performed over a longer period, we cannot exclude potential changes over a longer training period (Drexel et al., 2008; Zeppetzauer et al., 2013). In addition, presented effects could be transferred to a 3-week period of mountain holidays.
In contrast to studies displaying indoor or laboratory training regimens, outdoor training cannot be comparably standardized. For example, participants had to encounter changing weather conditions, also due to different seasons. These uncontrollable external factors may have influenced the results.
Metabolic effects per kJ were only estimated and may not reflect the real effects seen after EE when performed at the same energy expenditure as CE. However, in a real world setting where participants go downhill at fast speeds but without running, the energy expenditure will normally not be as pronounced as when walking uphill.
Conclusion
In contrast to downhill walking, 3 weeks of walking uphill the same hiking trail effectively improved glucose tolerance, triglycerides, HDL-C and TC/HDL-C ratio in middle-aged pre-diabetic men. However, when considering the related estimated energy expenditure, both types of walking could possibly have equal effects. Persons with more pronounced impairments of glucose tolerance benefited in particular from both training regimens. Thus, uphill walking represents the preferential mode of exercise but in patients with a low aerobic capacity and low exercise tolerance, walking downhill may be an appropriate preparation for later uphill walking. Thus, depending on the fitness level and individual preferences both types of exercise may be useful for the prevention of type 2 diabetes and disorders in lipid metabolism.
Acknowledgements
The present project is supported by the National Research Fund, Luxembourg. We would like to thank all the participants who were willing to sacrifice their free time for this study. The authors declared no conflict of interests regarding the publication of this manuscript.
Biographies

Marc PHILIPPE
Employment
Department of Sports Medicine, Institute of Sports Sciences, Justus-Liebig-University, Giessen, Germany
Department of Sport Science, Medical Section, University of Innsbruck, Innsbruck, Austria
Degree
MSc
Research interests
Exercise physiology, diabetes prevention, cytokines and exercise, high altitude physiology
E-mail: marc.philippe@sport.uni-giessen.de
Hannes GATTERER
Employment
Department of Sport Science, Medical Section, University of Innsbruck, Innsbruck, Austria
Degree
PhD
Research interests
High altitude physiology, altitude training, intermittent hypoxia, exercise physiology, body composition
E-mail: hannes.gatterer@uibk.ac.at
Erika Maria EDER
Employment
Department of Sport Science, Medical Section, University of Innsbruck, Innsbruck, Austria
Degree
BSc
Research interests
Exercise physiology, high altitude physiology
E-mail: erika.eder@tirol-kliniken.at
Alexander DZIEN
Employment
Internal Medicine, Medical Center Hentschelhof, Innsbruck, Austria
Degree
MD
Research interests
Epidemiology, metabolic syndrome, body composition
E-mail: alexander@dzien.at
Matthias SOMAVILLA
Employment
General Medicine, Praxisgemeinschaft Dr. Somavilla, Fulpmes, Austria
Degree
MD
Research interests
Metabolic syndrome, diabetes prevention, concentric and eccentric exercise
E-mail: praxis@dr-somavilla.at
Andreas MELMER
Employment
Department of Internal Medicine I, Medical University of Innsbruck, Innsbruck, Austria
Degree
PhD, MD
Research interests
Diabetes, metabolism, nutrition, bariatric surgery, epidemiology, genomics
E-mail: andreas.melmer@tirol-kliniken.at
Christoph EBENBICHLER
Employment
Professor, Department of Internal Medicine I, Medical University of Innsbruck, Innsbruck, Austria
Degree
MD
Research interests
Diabetes, metabolism, nutrition, bariatric surgery, epidemiology, genomics
E-mail: christoph.ebenbichler@i-med.ac.at
Tom MÜLLER
Employment
Kueser Akademie für Europäische Geistesgeschichte, Mathematische Sektion, Bernkastel-Kues, Germany
Degree
PhD
Research interests
Applied mathematics, biomechanics
E-mail: tom.mueller@kueser-akademie.de
Martin BURTSCHER
Employment
Department of Sport Science, Medical Section, University of Innsbruck, Innsbruck, Austria
Degree
PhD, MD
Research interests
Exercise physiology with emphasis on mountain sports activities, physiological and pathophysiological effects of altitude and hypoxia, epidemiology and prevention of accidents and emergencies in skiing and mountaineering, lifestyle interventions in health and disease mainly focusing on exercise, environmental and nutritional aspects
E-mail: martin.burtscher@uibk.ac.at
References
- American Diabetes Association (2015) 2. Classification and Diagnosis of Diabetes. Diabetes Care 38, S8-S16. [DOI] [PubMed] [Google Scholar]
- Asp S., Daugaard J.R., Richter E.A. (1995) Eccentric exercise decreases glucose transporter GLUT4 protein in human skeletal muscle. The Journal of Physiology 482, 705-712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borg G. (1970) Perceived exertion as an indicator of somatic stress. Scandinavian Journal of Rehabilitation Medicine 2, 92-98. [PubMed] [Google Scholar]
- Camillo C.A., Burtin C., Hornikx M., Demeyer H., de Bent K., van Remoortel H., Osadnik C.R., Janssens W., Troosters T. (2015) Physiological responses during downhill walking: A new exercise modality for subjects with chronic obstructive pulmonary disease? Chronic Respiratory Disease 12, 155-164. [DOI] [PubMed] [Google Scholar]
- Carey A.L., Steinberg G.R., Macaulay S.L., Thomas W.G., Holmes A.G., Ramm G., Prelovsek O., Hohnen-Behrens C., Watt M.J., James D.E., Kemp B.E., Pedersen B.K., Febbraio M.A. (2006) Interleukin-6 Increases Insulin-Stimulated Glucose Disposal in Humans and Glucose Uptake and Fatty Acid Oxidation In Vitro via AMP-Activated Protein Kinase. Diabetes 55, 2688-2697. [DOI] [PubMed] [Google Scholar]
- Drexel H., Saely C.H., Langer P., Loruenser G., Marte T., Risch L., Hoefle G., Aczel S. (2008) Metabolic and anti-inflammatory benefits of eccentric endurance exercise - a pilot study. European journal of clinical investigation 38, 218-226. [DOI] [PubMed] [Google Scholar]
- Durstine J.L., Grandjean P.W., Davis P.G., Ferguson M.A., Alderson N.L., DuBose K.D. (2001) Blood lipid and lipoprotein adaptations to exercise: a quantitative analysis. Sports medicine 31, 1033-1062. [DOI] [PubMed] [Google Scholar]
- Eriksson J., Lindström J., Valle T., Aunola S., Hämäläinen H., Ilanne-Parikka P., Keinänen-Kiukaanniemi S., Laakso M., Lauhkonen M., Lehto P., Lehtonen A., Louheranta A., Mannelin M., Martikkala V., Rastas M., Sundvall J., Turpeinen A., Viljanen T., Uusitupa M., Tuomilehto J. (1999) Prevention of Type II diabetes in subjects with impaired glucose tolerance: the Diabetes Prevention Study (DPS) in Finland. Diabetologia 42, 793-801. [DOI] [PubMed] [Google Scholar]
- Franz J.R., Lyddon N.E., Kram R. (2012) Mechanical work performed by the individual legs during uphill and downhill walking. Journal of Biomechanics 45, 257-262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Friedewald W.T., Levy R.I., Fredrickson D.S. (1972) Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clinical Chemistry 18, 499-502. [PubMed] [Google Scholar]
- Gordon B., Chen S., Durstine J.L. (2014) The Effects of Exercise Training on the Traditional Lipid Profile and Beyond. Current Sports Medicine Reports 13, 253-259. [DOI] [PubMed] [Google Scholar]
- Hansen D., Dendale P., van Loon L.J., Meeusen R. (2010) The Impact of Training Modalities on the Clinical Benefits of Exercise Intervention in Patients with Cardiovascular Disease Risk or Type 2 Diabetes Mellitus. Sports Medicine 40, 921-940. [DOI] [PubMed] [Google Scholar]
- Ishiguro H., Kodama S., Horikawa C., Fujihara K., Hirose A.S., Hirasawa R., Yachi Y., Ohara N., Shimano H., Hanyu O., Sone H. (2016) In Search of the Ideal Resistance Training Program to Improve Glycemic Control and its Indication for Patients with Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Sports Medicine 46, 67-77. [DOI] [PubMed] [Google Scholar]
- Ivy J.L. (1997) Role of Exercise Training in the Prevention and Treatment of Insulin Resistance and Non-Insulin-Dependent Diabetes Mellitus. Sports Medicine 24, 321-336. [DOI] [PubMed] [Google Scholar]
- Jensen J., Rustad P.I., Kolnes A.J., Lai Y.-C. (2011) The Role of Skeletal Muscle Glycogen Breakdown for Regulation of Insulin Sensitivity by Exercise. Frontiers in Physiology 2, 112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jensen T.E., Richter E.A. (2012) Regulation of glucose and glycogen metabolism during and after exercise. The Journal of Physiology 590, 1069-1076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jeon C.Y., Lokken R.P., Hu F.B., van Dam R.M. (2007) Physical Activity of Moderate Intensity and Risk of Type 2 Diabetes: A systematic review. Diabetes Care 30, 744-752. [DOI] [PubMed] [Google Scholar]
- Johnson A.T., Benhur Benjamin M., Silverman N. (2002) Oxygen consumption, heat production, and muscular efficiency during uphill and downhill walking. Applied Ergonomics 33, 485-491. [DOI] [PubMed] [Google Scholar]
- Kelley G. (2004) Walking, lipids, and lipoproteins: a meta-analysis of randomized controlled trials. Preventive Medicine 38, 651-661. [DOI] [PubMed] [Google Scholar]
- Kelley G.A., Kelley K.S. (2009) Impact of progressive resistance training on lipids and lipoproteins in adults: A meta-analysis of randomized controlled trials. Preventive Medicine 48, 9-19. [DOI] [PubMed] [Google Scholar]
- Kodama S., Tanaka S., Saito K., Shu M., Sone Y., Onitake F., Suzuki E., Shimano H., Yamamoto S., Kondo K., Ohashi Y., Yamada N., Sone H. (2007) Effect of aerobic exercise training on serum levels of high-density lipoprotein cholesterol: a meta-analysis. Archives of Internal Medicine 167, 999-1008. [DOI] [PubMed] [Google Scholar]
- Kramer P.A. (2010) The effect on energy expenditure of walking on gradients or carrying burdens. American Journal of Human Biology 22, 497-507. [DOI] [PubMed] [Google Scholar]
- Le Floch J.P., Escuyer P., Baudin E., Baudon D., Perlemuter L. (1990) Blood glucose area under the curve. Methodological aspects. Diabetes Care 13, 172-175. [DOI] [PubMed] [Google Scholar]
- Linna M.S., Ahotupa M., Kukkonen-Harjula K., Fogelholm M., Vasankari T.J. (2015) Co-existence of insulin resistance and high concentrations of circulating oxidized LDL lipids. Annals of Medicine 47, 394-398. [DOI] [PubMed] [Google Scholar]
- Marcus R.L., LaStayo P.C., Dibble L.E., Hill L., McClain D.A. (2009) Increased Strength and Physical Performance with Eccentric Training in Women with Impaired Glucose Tolerance: A Pilot Study. Journal of Women's Health 18, 253-260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mathers C.D., Loncar D., Samet J. (2006) Projections of Global Mortality and Burden of Disease from 2002 to 2030. PLoS Medicine 3, e442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Matthews D.R., Hosker J.P., Rudenski A.S., Naylor B.A., Treacher D.F., Turner R.C. (1985) Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28, 412-419. [DOI] [PubMed] [Google Scholar]
- Paschalis V., Nikolaidis M.G., Giakas G., Theodorou A.A., Sakellariou G.K., Fatouros I.G., Koutedakis Y., Jamurtas A.Z. (2010) Beneficial changes in energy expenditure and lipid profile after eccentric exercise in overweight and lean women. Scandinavian Journal of Medicine & Science in Sports 20, e103-e111. [DOI] [PubMed] [Google Scholar]
- Paschalis V., Nikolaidis M.G., Theodorou A.A., Panayiotou G., Fatouros I.G., Koutedakis Y., Jamurtas A.Z. (2011) A weekly bout of eccentric exercise is sufficient to induce health-promoting effects. Medicine and Science in Sports and Exercise 43, 64-73. [DOI] [PubMed] [Google Scholar]
- Philippe M., Krüsmann P., Mersa L., Eder E., Gatterer H., Melmer A., Ebenbichler C., Burtscher M. (2016) Acute effects of concentric and eccentric exercise on glucose metabolism and interleukin-6 concentration in healthy males. Biology of Sport 33, 153-158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pont F., Duvillard L., Florentin E., Gambert P., Vergès B. (2002) High-density lipoprotein apolipoprotein A-I kinetics in obese insulin resistant patients. An in vivo stable isotope study. International Journal of Obesity Related Metabolic Disorders 26, 1151-1158. [DOI] [PubMed] [Google Scholar]
- Richter E.A., Hargreaves M. (2013) Exercise, GLUT4, and skeletal muscle glucose uptake. Physiological reviews 93, 993–1017. [DOI] [PubMed] [Google Scholar]
- Sigal R.J., Kenny G.P., Boule N.G., Wells G.A., Prud'homme D., Fortier M., Reid R.D., Tulloch H., Coyle D., Phillips P., Jennings A., Jaffey J. (2007) Effects of aerobic training, resistance training, or both on glycemic control in type 2 diabetes: a randomized trial. Annals of Internal Medicine 147, 357-369. [DOI] [PubMed] [Google Scholar]
- Slentz C.A., Houmard J.A., Johnson J.L., Bateman L.A., Tanner C.J., McCartney J.S., Duscha B.D., Kraus W.E. (2007) Inactivity, exercise training and detraining, and plasma lipoproteins. STRRIDE: a randomized, controlled study of exercise intensity and amount. Journal of Applied Physiology 103, 432-442. [DOI] [PubMed] [Google Scholar]
- Smutok M., Reece C., Kokkinos P., Farmer C., Dawson P., de Vane J., Patterson J., Goldberg A., Hurley B. (1994) Effects of Exercise Training Modality on Glucose Tolerance in Men with Abnormal Glucose Regulation. International Journal of Sports Medicine 15, 283-289. [DOI] [PubMed] [Google Scholar]
- Snowling N.J., Hopkins W.G. (2006) Effects of Different Modes of Exercise Training on Glucose Control and Risk Factors for Complications in Type 2 Diabetic Patients: A meta-analysis. Diabetes Care 29, 2518-2527. [DOI] [PubMed] [Google Scholar]
- Solomon T.P., Malin S.K., Karstoft K., Haus J.M., Kirwan J.P. (2013) The influence of hyperglycemia on the therapeutic effect of exercise on glycemic control in patients with type 2 diabetes mellitus. JAMA Internal Medicine 173, 1834-1836. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sylow L., Møller L.L.V., Kleinert M., Richter E.A., Jensen T.E. (2015) Stretch-stimulated glucose transport in skeletal muscle is regulated by Rac1. The Journal of Physiology 593, 645–656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taskinen M.-R. (2002) Diabetic dyslipidemia. Atherosclerosis 3, 47-51. [DOI] [PubMed] [Google Scholar]
- Tuomilehto J., Lindström J., Eriksson J.G., Valle T.T., Hämäläinen H., Ilanne-Parikka P., Keinänen-Kiukaanniemi S., Laakso M., Louheranta A., Rastas M., Salminen V., Aunola S., Cepaitis Z., Moltchanov V., Hakumäki M., Mannelin M., Martikkala V., Sundvall J., Uusitupa M. (2001) Prevention of Type 2 Diabetes Mellitus by Changes in Lifestyle among Subjects with Impaired Glucose Tolerance. New England Journal of Medicine 344, 1343-1350. [DOI] [PubMed] [Google Scholar]
- Wojtaszewski J.F.P., Nielsen J.N., Richter E.A. (2002) Invited review: effect of acute exercise on insulin signaling and action in humans. Journal of applied physiology 93, 384-392. [DOI] [PubMed] [Google Scholar]
- Zeppetzauer M., Drexel H., Vonbank A., Rein P., Aczel S., Saely C.H. (2013) Eccentric endurance exercise economically improves metabolic and inflammatory risk factors. European journal of preventive cardiology 20, 577-584. [DOI] [PubMed] [Google Scholar]