

To the Editor: Diaphragmatic myoclonus, as a typical unusual focal dyskinesia, is characterized by repetitive involuntary synchronous contractions of the diaphragm and other respiratory muscles.[1] Various clinical presentations and difficulties in identifying etiology might lead to its late diagnoses and ineffective treatment in many cases. Botulinum toxin A has a paralyzing effect on muscles. However, to the best of our knowledge, there have been few reports of injecting botulinum toxin A to the diaphragm. In this case, we reported that diaphragmatic myoclonus was successfully treated by injecting botulinum toxin A into the diaphragm and the rectus abdominis (RA) under needle electromyography (EMG) guidance.
A 51-year-old man presented with a 5-year history of involuntary abdominal movements [Video 1]. These movements, which were suppressed by sitting, standing, or distraction and exacerbated by lying down or relaxing, did not persist when he was asleep. Due to these abdominal movements, he could not concentrate on his work and lost confidence in interpersonal relationships. He even twice attempted to commit suicide. Previous treatments with scopolamine, baclofen, valproate, clonazepam, carbamazepine, traditional Chinese herbal medicine, and acupuncture had no effect on his abdominal movements and brought side effects such as drowsiness. The patient had a 20-year history of depression and two manic episodes, taking sertraline 50 mg, lithium carbonate 500 mg, and clozapine 25 mg daily. Given the possible adverse effects, his psychiatrist suggested stopping taking clozapine over a period, but he got no improvement. In the clinical examination, the patient showed symptoms of irregular twitches and spasms of the abdominal wall associated with sagittal oscillations of the upper body and sounds from the larynx. No abnormal movements in his limbs, neck, or head were observed. The 24-h video electroencephalogram and magnetic resonance imaging of the brain showed no abnormality. Outcomes of blood tests, including thyroid hormones, liver and renal function, and autoimmune tests, were all normal. Considering body's bending up and interruption to speech during the twitches, both RA and diaphragm were speculated to participate in these abnormal movements. Further examination with fluoroscopy and needle EMG confirmed the speculation by revealing the involvement of the diaphragm and RA [Video 1] during these abdominal movements, and the diagnosis of “diaphragmatic myoclonus” was verified. With the consent of the patient and his family regarding potential risks and benefits, we performed botulinum toxin A (Allergen Pharmaceuticals Ltd., Westport, Ireland) injection into the diaphragm under EMG guidance, including 50 units in the right hemidiaphragm, 25 units in the left hemidiaphragm, and 100 units in each RA [Figure 1]. A total of 275 units of botulinum toxin A were used in this case. The oxyhemoglobin saturation was monitored throughout the process. One week later, the patient reported that the intensity and frequency of the abdominal involuntary movements decreased significantly, without dyspnea, weakness of truncal flexion, or other unexpected effects. Moreover, he could handle his work much better than before and became more confident to get along with other people. No flash of suicidal thought was observed since those abnormal movement symptoms got relieved. Clinical examination showed relative abdominal muscular relaxation and slight twitches captured only a few times. Four months after the injection, the positive treatment effect was still maintained [Video 2].
Figure 1.
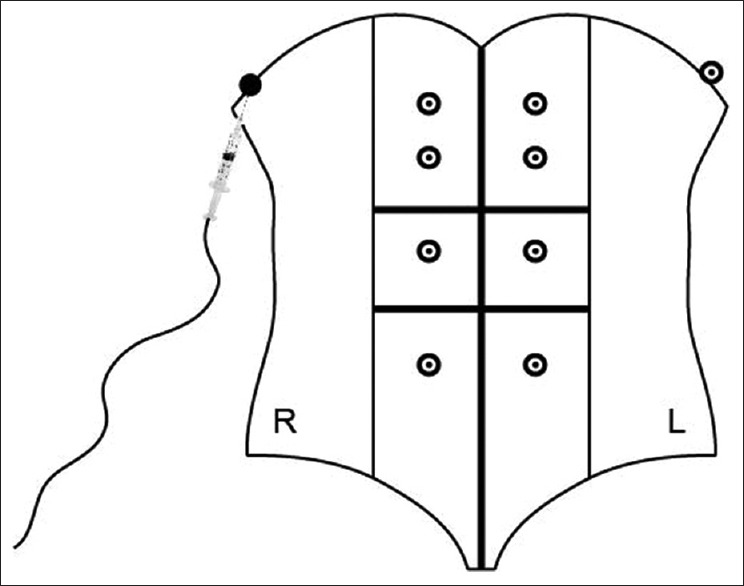
Two sites on the diaphragm and eight sites on the rectus abdominis were injected with botulinum toxin A. The place and dose of each injection site are indicated by ⨀ (25 units) and ● (50 units).
Brief, repetitive, and involuntary contractions of the diaphragm can be defined as “diaphragmatic myoclonus”.[2] It has also been referred to as Leeuwenhoek disease, respiratory myoclonus, and diaphragmatic flutter.[1] Complaints are different among patients, usually including dyskinetic movements in abdominal wall, thoraco-abdominal pain, and respiratory disorder.[3] Besides the clinical suspicion and abnormal diaphragm movements under fluoroscopy, EMG studies showing myoclonus-related potential of diaphragm make a reliable diagnosis.[4] Although several pharmacological and nonpharmacological treatments were reported to be effective in some cases, there is still no recommendation for treating diaphragmatic myoclonus.[1] Currently, treatments of diaphragmatic myoclonus include cervical plexus block, phrenic neurectomy, and medications such as carbamazepine and phenytoin. Due to its effect of blocking the action of acetylcholine at neuromuscular junction, botulinum toxin A is very helpful in relieving muscle spasms. In this case, symptoms of abdominal movements resulted from the abnormal diaphragm and RA contractions, and that is the reason why we injected botulinum toxin A to these muscles.
In contrast to other mature protocols for botulinum toxin A application, local botulinum toxin A injection into the diaphragm is a novel attempt. Based on impaction of botulinum toxin A volume and concentration on curative effect,[5] high concentration and low volume botulinum toxin A (50 unit/ml) was utilized to avoid paralysis of adjacent tissues. Taking into consideration the limited space for injections, single point for each side of diaphragm was selected, with 50 units on the right side and 25 units on the left side to reduce the risk of respiratory depression after botulinum toxin A injection. Despite the difficulty of injection and risk of complications, it does constitute an option to apply botulinum toxin A in the case of diaphragmatic myoclonus under EMG guidance, especially when there is no other more effective treatment method. Further studies, standardizing procedures, and doses of botulinum toxin A injections into the diaphragm are warranted.
Financial support and sponsorship
This study was supported by grants from Shuguang Program (No: 14SG21), and Talent Development Foundation of Putuo district (No: 2014-A-21).
Conflicts of interest
There are no conflicts of interest.
Videos available on: www.cmj.org
Footnotes
Edited by: Xin Chen
References
- 1.Ramírez JD, Gonzales M, Hoyos JA, Grisales L. Diaphragmatic flutter: A case report and literature review. Neurologia. 2015;30:249–51. doi: 10.1016/j.nrl.2013.06.016. doi: 10.1016/j.nrl.2013.06.016. [DOI] [PubMed] [Google Scholar]
- 2.Aggarwal A, Thompson PD. Unusual focal dyskinesias. Handb Clin Neurol. 2011;100:617–28. doi: 10.1016/B978-0-444-52014-2.00044-6. doi: 10.1016/B978-0-444-52014-2.00044-6. [DOI] [PubMed] [Google Scholar]
- 3.Larner AJ. Antony van Leeuwenhoek and the description of diaphragmatic flutter (respiratory myoclonus) Mov Disord. 2005;20:917–8. doi: 10.1002/mds.20614. doi: 10.1002/mds.20614. [DOI] [PubMed] [Google Scholar]
- 4.Lim EC, Seet RC. Botulinum toxin injections to treat belly dancer's dyskinesia. Mov Disord. 2009;24:1401. doi: 10.1002/mds.22523. doi: 10.1002/mds.22523. [DOI] [PubMed] [Google Scholar]
- 5.Hsu TS, Dover JS, Arndt KA. Effect of volume and concentration on the diffusion of botulinum exotoxin A. Arch Dermatol. 2004;140:1351–4. doi: 10.1001/archderm.140.11.1351. doi: 10.1001/archderm.140.11.1351. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.