

Abstract
Understanding alterations in perceptual experiences as a component of the basic symptom structure of psychosis may improve early detection and the identification of subtle shifts that can precede symptom exacerbation. We explored the phenomenological construct of absorption and psychotic experiences in both clinical (bipolar psychosis and schizophrenia spectrum) and non-clinical participants. Participants with psychosis endorsed significantly higher absorption compared to the non-clinical group. Absorption was positively correlated with all types of hallucinations and multiple types of delusions. The analysis yielded two distinct cluster groups that demarcated a distinction along the continuum of self-disturbance: on characterized by attenuated ego boundaries and the other stable ego boundaries. The study suggests that absorption is a potentially important but under-researched component of psychosis that overlaps with, but is not identical to the more heavily theorized constructs of aberrant salience and hyperreflexivity.
Keywords: Phenomenology, Absorption, Aberrant Salience, Hallucinations, Delusions, Psychosis
1. Introduction
Over the last century, psychopathologists have developed a substantial body of research on the psychogenesis of psychosis; much of this work has focused on the prodrome and first episode, widely seen as windows into the underlying mechanisms of more acute or persistent psychotic states (Jaspers, 1968; Sass, 2001). Across sub-disciplines (spanning psychoanalysis and cognitive neuroscience), disruptions of the basic sense of self (ipseity) and self-other or self-world processing have been widely implicated (Gross, Huber, Klosterkotter, & Linz, 1987; Kapur, 2003; Gross, Huber, Klosterkotter, & Linz, 2008; Parnas et al., 2005; Corlett, Taylor, Wang, Fletcher, & Krystal, 2010). Beneath this broader umbrella, however, multiple different, overlapping but distinct, psychogenetic constructs have been proposed. For the purposes of the current study, we focus on three: the ipseity hypothesis put forward by Sass & Parnas, 2003 and colleagues; aberrant salience as described by Gray 1995; Kapur, 2003 and absorption as conceptualized by Tellegen & Atkinson, 1974.
Drawing on the work of European phenomenological psychiatrists, including the German basic symptoms school (Gross et al., 1987; Gross & Huber, 2010; Sass & Parnas, 2003) Sass and Parnas have postulated the ipseity hypothesis of schizophrenia, involving two core components of disturbed basic sense of self: hyperreflexivity and diminished self-affection. Hyerpreflexivity refers to the process by which events, sensations and cognitions that would normally be experienced as tacit (or pre-reflective) become explicit; for instance, a subject’s own thoughts may come to seem foreign, externalized and/or object-like. Diminished self-affection describes the loss or attenuation of a normal sense of the self existing as the subject (rather than object) of consciousness. In extreme cases, a patient might feel that their thoughts or bodily processes are controlled by external forces, or can no longer maintain the privacy of their own thoughts. Sass & Parnas, 2001 have also suggested that hyperreflective processes may come into play in the crystallization of psychosis: viz., the patient’s self-conscious and at least quasi-agentive investment in and/or preoccupation with subtle changes in perception, affect and sense of self. Recent phenomenological research lends further support to the role of quasi-agentive processes in both patients’ initial reaction to and subsequent self-conscious participation in the elaboration of nascent psychotic changes (Jones & Luhrmann, 2015).
Meanwhile, inspired by biological findings regarding the role of mesolimbic dopamine in schizophrenia, (Gray, Feldon, Rawlins, Hemsley and Smith, 1991; Kapur, 2003) has proposed a “unified” theory of psychosis, revolving around abnormal or aberrant salience and altered stimulus-reinforcement learning, beginning in the prodrome and ultimately leading to frank delusions and hallucinations. Conversely, the efficacy of antipsychotic medication has been attributed to the attenuation of heightened salience by acting as a dopamine receptor antogonist. A translational construct, salience refers to the process whereby particular stimuli, whether external or internal, are perceived as ‘standing out’ from other stimuli and/or capture a subject’s attention (Braver et al., 2014). Incentive or motivational salience, more narrowly, describes attention to a stimulus driven by a reflective or pre-reflective desire or by motivated interest (Jensen & Walter, 2014). In psychosis, aberrant salience has been hypothesized to contribute to misattributions of meaning or significance to random or unimportant objects, to the perception of meaningful connections between otherwise unremarkable events, and to disruptions of self-other boundaries common in delusions (and proto-delusions) of reference. For example, a subject with psychosis who comes to view the random gestures of strangers on a subway platform as not only pointedly meaning-laden but also self-referential.
Various neuronal circuits have been proposed to underlie psychosis, including, but not limited to dopaminergic, serotonergic and glutaminergic pathways (Lang, Puls, Muller, Strutz-Seebohm, & Gallinat, 2007). Recently, more global factors beyond the neuron, such as inflammation, are being examined for their role in the psychogenesis of psychotic breaks (Chase, Cone, Rosen, & Sharma, 2016). One of the primary biological mechanisms linking salience and psychosis is associated with the dopaminergic neurotransmitter system and hypothalamic-pituitary-adrenal (HPA) axis dysregulation (Davis, Kahn, Ko, & Davidson, 1991; Seeman & Kapur, 2000; Seeman, 1987). Hyperactivity of the dopaminergic system is thought to play a critical role in the development of aberrant salience (Gray 1995; Kapur, 2003). Hyperactive dopamine transmission may also increase aberrant salience underpinning the process of self-disturbance (Nelson & Sass, 2009), though researchers generally agree that excessive dopamine cannot and does not serve as a monothetic explanation for psychosis. Likewise, environmental influences including trauma, drug abuse, and urban background have all been identified as contributing factors in the development of psychosis (van Os et al., 2002; Beards et al., 2013; Varese et al., 2012; Isvoranu, Borsboom, van Os, & Guloksuz, 2016). However, the most widely considered hypothesis of the psychogenesis of psychosis integrates epigenetic reactions to environmental influences and causative genes (Roth, Lubin, Sodhi, & Kleinman, 2009). As psychotic symptoms crystalize, they form a complex multimodal experience by which hallucinations and delusions emerge against the backdrop of altered sense of basic self (Jaspers, 1963; Sass, 2010; Sass, 2014; Sass & Parnas, 2003; Rosen et al., 2016a).
In contrast to disturbed ipseity and aberrant salience, both of which are constructs explicitly elaborated to explain psychotic psychopathology, the concept of absorption has been theorized by Tellegen & Atkinson, 1974 and others as a dispositional trait, distributed across the general population. Absorption describes a state of immersion in (or capture by) mental imagery or perceptual stimuli and correlates with vivid imagination or fantasy. During a period of intense absorption “objects of […] attention” are hypothesized to “acquire an importance and intimacy that are normally reserved for the self and may therefore acquire a self-like quality” (Tellegen & Atkinson, 1974).
Conceptual overlap between absorption and disturbed ipseity and aberrant salience is significant; however there are also important differences. For instance, unlike self-affection, a non-clinical subject ‘absorbed’ in the experience of beautiful music or a breathtaking landscape may feel a subjective attenuation of self-object boundaries but does not necessarily experience a loss of self-affection in the sense of no longer inhabiting the world as a subject of awareness. The stimuli captured in the Tellegen Absorption Scale include beautiful sunsets and intense colors, rather than random gestures, kinesthetic sensations or the otherwise generic white shoes an unknown passenger happens to be wearing on a bus; it is less that tacit processes are suddenly rendered explicit, than that the subject is able (or tends) to lose him or herself in already culturally salient experiences. Further, although the subject of absorption may temporarily enter a state of altered consciousness, such changes are temporary and he or she retains agentive control and the capacity for socially normative ‘reality testing.’
Empirically, absorption also correlates with hypnotizeability, proneness to spiritual experiences, included altered meditative or dissociative states, and the intensity of response to LSD and other psychedelics (Tellegen & Atkinson, 1974; Luhrmann, Nusbaum, & Thisted, 2010; Humpston et al., 2016; Tagliazucchi, Carhart-Harris, Leech, Nutt, & Chialvo, 2014). In contrast, patients with schizophrenia have shown diminished hypnotizeability relative to patients with dissociative disorders on at least some dimensions (Frischholz et al., 1992). Psychosis more strongly implicates confusion between mental imagery and perception rather than an intense and active imagination per se (Brebion, Ohlsen, Pilowsky, & David, 2008). Historically and cross-culturally, there has been significant overlap between spiritual altered states (including Shamanic dissociation) and at least some aspects or manifestations of psychosis. Dissociation itself occupies a still ambiguous role, and researchers continue to debate overlap and distinctions between dissociative psychopathology, spiritual dissociation and more classical (‘non-dissociative’) psychosis/schizophrenia (Haugen and Castillo, 1999; Castillo, 2003; Luhrmann, 2005).
Only a few studies to date have investigated absorption in psychosis. Humpston et al., (2016) found that both absorption and “detachment-type” dissociation versus “compartmentalization-type” dissociation significantly predicted psychotic-like experiences in a non-clinical population. Similarly, absorption and depersonalization (which is a type of detachment-type dissociation) have been found to predict hallucination proneness in healthy subjects (Perona-Garcelán et al., 2013). Another study found that patients with schizophrenia who were currently experiencing hallucinations scored significantly higher on absorption than either schizophrenia patients with current delusions but no hallucinations or schizophrenia patients in symptomatic remission (Perona-Garcelan et al., 2012). Abnormal salience is also hypothesized to inform subjects’ developing understanding of their experiences, and contribute to the crystallization of hallucinations and delusions (Kapur, 2003; Corlett et al., 2010).
Phenomenologically oriented researchers hypothesize that these anomalous self-experiencess (ASE) and disturbance of the basic sense of self represent the core alterations of a psychotic process, initially manifesting in the prodrome (Nelson, Whitford, Lavoie, & Sass, 2014b; Parnas, Handest, Jansson, & Saebye, 2005; Sass & Parnas, 2003; Waters & Badcock, 2010; Sass, 2014). Over time, initially subtle changes in self experience may become more pronounced, leading to existential anxiety, disorientation and subjective need to resolve ambiguity through the interpretation of anomalous experiences, leading to more overt delusions or theories of an altered world (Jones & Luhrmann, 2015). Anomalous self experiences may also engender attributions of increased salience, as the subject fixates on those objects or aspects of his or her experience that seem strange and unexplainable.
Tellegen & Atkinson (1974), conducted a series of studies examining state-like manifestations of absorption, defined as a “heightened sense of the reality of the attentional object, an imperviousness to normally distracting events, and an altered sense of reality in general and of the self in particular.” Phenomenologically, absorption involves an experience in which one’s perceptual, cognitive resources are fully engaged, and the focus of attention is either narrowed or widened, so that the person enters a subtly altered state of reality that includes a shift in the demarcation of self (Tellegen & Atkinson, 1974).
1.1. Aims of the study
The purpose of this study was to explore the phenomenological construct of absorption at the crossroads of self, absorption and psychosis in a psychiatric population sample (schizophrenia and bipolar disorder) compared to non-clinical participants. We investigated the following questions:
Is absorption more prevalent in a clinical sample with psychosis when compared to a nonclinical sample?
Is there a diagnostic difference in absorption between schizophrenia and bipolar disorder with psychosis?
Is increased absorption associated with specifics types of hallucinations and/or forms of delusions?
Are there sub-categories/clusters of absorption that are distinct and identifiable? If so, what is the phenomenological symptom presentation associated with these sub-categories/clusters?
2. Methods
2.1. Participants
There were a total of 115 participants, of which there were 44 (38%) participants with schizophrenia, 30 (26%) participants with bipolar disorder with psychosis, and 41 (36%) nonclinical controls who were included in this study. Non-clinical controls were defined as persons who did not meet DSM criteria for a major psychiatric disorder. The clinical sample was randomly selected from a large urban university medical center but included referrals from community treatment facilities. The non-clinical participants were recruited from neighboring communities. The study was approved by the University of Illinois at Chicago Internal Review Board, and signed consent was obtained prior to initiation of study procedures. Inclusion criteria for the study included participants between the ages of 21 – 60 who met criteria for schizophrenia or bipolar disorder with psychosis and non-clinical controls. Consensus diagnoses for participants with schizophrenia and bipolar disorder with psychosis were determined by the clinical and research team using the SCID (First et al., 2002), and available collateral information. The SCID was also administered to the non-clinical sample to identify any current or past psychiatric diagnosis that would exclude them from participating in the nonclinical sample. Exclusion criteria for the clinical and non-clinical samples included current substance dependence, seizure disorders, current pregnancy, and neurological conditions. Demographic characteristics for the sample and clinical metrics were obtained at the study evaluation.
2.2. Measures used to assess the phenomenology of absorption
The primary clinical measures for this study included the SCID, PANSS, and TAS. Psychopathological assessments of types of hallucinations and forms of delusions were based on the SCID and scored as absent (score of “1”), subthreshold (“2”) and threshold or true present (“3”) (First et al., 2002). The SCID includes an assessment of various types of hallucinations, including auditory, visual, tactile, gustatory and olfactory; and forms of delusions such as referential, persecutory, grandiose, somatic, religious, guilt, jealous, erotomanic, control, thought insertion, thought withdrawal, and thought broadcasting. Inter-evaluator reliability was Kappa 0.83.
The PANSS was scored along a continuum of severity between one (asymptomatic) to seven (extreme symptom severity). Analysis was conducted via data reduction strategies guided by prior empirical studies of symptom domains assessed by the PANSS(Kay et al., 1987). Scores were calculated for five-factors: 1) Positive symptoms (delusions, grandiosity, suspiciousness/persecution, unusual thought content), 2) Negative symptoms (blunted affect, emotional withdrawal, poor rapport, passive/apathetic social withdrawal, lack of spontaneity and flow of conversation, and active social avoidance), 3) Cognitive Disorganization (conceptual disorganization, difficulty in abstract thinking, mannerisms and posturing, disorientation, and poor attention), 4) Excitement (excitement, hostility, tension, and poor impulse control), and 5) Depression (somatic concern, anxiety, guilt feelings, depression, and preoccupation). Items were pooled in this way based on previous factor analytic findings (Lindenmayer, Bernstein-Hyman, & Grochowski, 1994; Lehoux, Gobeil, Lefebvre, Maziade, & Roy, 2009). In addition, PANSS items that have been shown to identify related symptom domains in cluster analyses that assess Anergia (blunted affect, emotional withdrawal, motor retardation, and disorientation), Thought Disturbance (conceptual disorganization, hallucinatory behavior, grandiosity, and unusual thought content), and Paranoia (suspiciousness/persecution, hostility, and uncooperativeness) were obtained. PANSS items were pooled into these dimensions based on previous cluster analysis research (Farmer, McGuffin, & Spitznagel, 1983; Morrison, Bellack, Wixted, & Mueser, 1990; Dollfus et al., 1996). Kay et al., (1987) reported high levels of internal reliability (ranging from r = 0.77 to 0.89) and the test–retest reliability (r = 0.80). Additionally, inter-evaluator reliability was Kappa 0.85. Absorption was measured using the Tellegen Absorption Scale (TAS). The TAS is a 34 item true/false questionnaire designed to measure levels of mental involvement with the object of experience (Tellegen & Atkinson, 1974). Tellegen (1982) reported high levels of internal reliability (r = 0.88) and high levels of test–retest reliability (r = 0.91). Absorption was formulated in terms of “total attention involving a full commitment of available perceptual, motoric, imaginative and ideational resources to a unified representation of attentional object” (Tellegen & Atkinson, 1974). The TAS consists of nine content factors that include: responsiveness to engaging stimuli, responsiveness to inductive stimuli, imagistic thought, ability to summon vivid and suggestive images, and cross-modal experiences (e.g. synesthesia), absorption in thoughts and imaginings, vivid memories of the past, episodes of expanded awareness, and altered states of consciousness (Tellegen, 1982).
2.3. Data Analyses
Demographic data were analyzed using Fisher exact tests and analyses of variance (ANOVAs). For ANOVAs that yielded significant results, Tukey post hoc tests were used to identify significant pair-wise group differences. Spearman’s bivariate correlations were conducted to determine associations between absorption and types of hallucinations and forms of delusions. Two-step cluster analyses were conducted to identify distinct sub-categories of absorption followed by independent sample t-test to compare PANSS 5-factor scores between the identified subgroup clusters.
3. Results
3.1. Descriptive characteristics
Group comparisons of demographic characteristics show a significant difference in race between groups, with a larger sample of African American participants (p <0.05, Fisher’s exact test), as noted in Table 1. There was no significant difference between sex and age and diagnostic group.
Table 1. Participant demographic information.
Demographic characteristic of subjects and diagnostic differences. Differences between diagnostic groups was determined by Student’s t-test, with significant levels indicated
| Demographic Measures | Schizophrenia (n=44) |
Bipolar Disorder w/Psychosis (n=30) |
Control (n=41) |
p Value | |||
|---|---|---|---|---|---|---|---|
| Sex | n.s. | ||||||
| Male | 22 (50%) | 13 (43%) | 19 (46%) | ||||
| Female | 22 (50%) | 17 (57%) | 22 (54%) | ||||
| Race | 0.005 | ||||||
| African American | 34 (77%) | 23 (77%) | 19 (46%) | ||||
| Asian | 2 (5%) | 0 (0%) | 8 (20%) | ||||
| Caucasian | 4 (9%) | 4 (13%) | 11 (27%) | ||||
| Hispanic | 4 (9%) | 3 (10%) | 3 (7%) | ||||
| Mean | SD | Mean | SD | Mean | SD | n.s. | |
| Current Age | 44 | 12.53 | 44 | 12.69 | 41 | 13.99 | |
n.s.=not significant; SD=standard deviation
We examined differences in absorption between schizophrenia, bipolar disorder with psychosis and non-clinical groups using the TAS and found a statistically significant difference between groups as determined by a one-way ANOVA showing that participants with schizophrenia endorsed significantly more TAS items than either the bipolar disorder with psychosis and the non-clinical control groups (F2,114=6.23, p=0.003). As noted in Figure 1, Post hoc comparisons using the Tukey HSD test indicated that the mean score for participants with schizophrenia (M=16.11, SD=8.50) was significantly higher than the non-clinical control group (M=10.07, SD=7.91). Although the TAS mean score was higher in persons with schizophrenia compared to participants in the bipolar disorder with psychosis group (M=14.53, SD=7.66) there was not a significant difference between the groups.
Figure 1.
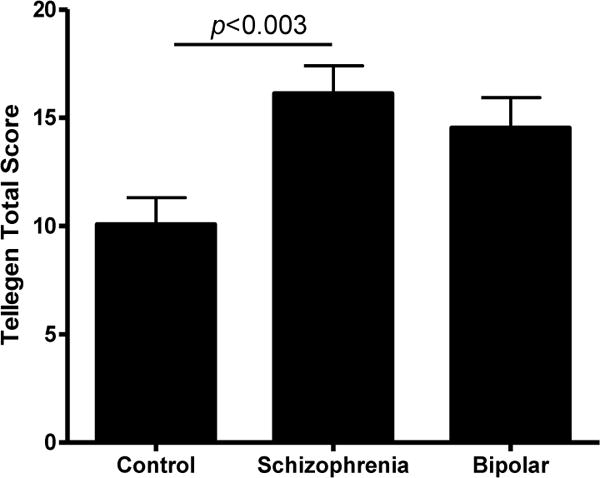
The comparison of absorption in schizophrenia, bipolar disorder with psychosis and non-clinical participants.
3.2. Dimensions of absorption
To better understand the construct of absorption and psychosis in both the clinical and non-clinical sample (n=115), we conducted bivariate correlations between TAS, types of hallucinations (Table 2) and forms of delusions (Table 3). As shown in Table 2 (clinical and nonclinical sample column), regardless of diagnosis, we found a highly positive correlation between TAS and auditory, visual, tactile, gustatory, and olfactory hallucinations. As shown in Table 3 (clinical and non-clinical sample column) we found positive correlations between absorption and delusions of reference, persecution, grandiosity, somatic, religious, control, thought insertion, thought withdrawal, and thought broadcasting.
Table 2. Correlations between absorption and types of hallucinations.
Spearman Correlations between salience and types of hallucinations.
| Variables | Clinical and non-clinical sample (n=115) |
Clinical sample (n=74) |
|
|---|---|---|---|
| 1. | Absorption | ~ | ~ |
| 2. | Auditory | 0.402*** | 0.238* |
| 3. | Visual | 0.378*** | 0.298** |
| 4. | Tactile | 0.397*** | 0.316** |
| 5. | Gustatory | 0.390*** | 0.395*** |
| 6. | Olfactory | 0.382*** | 0.337** |
p<0.05,
p<0.01,
p<0.001.
Table 3. Correlations between absorption and forms of delusions.
Spearman Correlations between salience and forms of delusions.
| Variables | Clinical and non-clinical sample (n=115) |
Clinical sample (n=74) |
|
|---|---|---|---|
| 1. | Absorption | ~ | ~ |
| 2. | Referential Delusions | 0.404*** | 0.284** |
| 3. | Persecutory Delusions | 0.350*** | 0.088 |
| 4. | Grandiose Delusions | 0.301*** | 0.168 |
| 5. | Somatic Delusions | 0.230*** | 0.124 |
| 6. | Religious Delusions | 0.226* | 0.156 |
| 7. | Delusions of Guilt | 0.061 | 0.039 |
| 8. | Jealous Delusions | 0.158 | 0.115 |
| 9. | Erotomanic Delusions | 0.060 | 0.002 |
| 10. | Delusions of control | 0.345*** | 0.241* |
| 11. | Delusions of thought insertion | 0.285** | 0.174 |
| 12. | Delusions of thought withdrawal | 0.337*** | 0.311* |
| 13. | Delusions of thought broadcasting | 0.237** | 0.117 |
p<0.05,
p<0.01,
p<0.001.
We also examined absorption within all subjects with psychosis (n=74), including participants with schizophrenia to participants with bipolar disorder with psychosis. Here we found a significant positive correlation between TAS and auditory, visual, tactile, gustatory, and olfactory hallucinations (Table 2; Clinical sample column). The clinical group (schizophrenia and bipolar disorder with psychosis) also showed a significant positive correlation between TAS and specific forms of delusions such as referential delusions, delusions of control, and delusions of thought withdrawal (Table 3; Clinical sample column).
Next, to identify and examine subtypes of absorption within the sample, we conducted a two-step cluster analysis that consisted of preclustering and standard algorithmic hierarchical clustering of individual TAS items (Zhang, Ramakrishnon, & Livny, 1996; Chiu, Fang, Chen, Wang, & Jeris, 2001). Within the sample, the analysis yielded two distinct cluster groups that demarcated a distinction along the continuum of self-disturbance. Cluster One, which we titled Attenuated Ego Boundaries (AEB), consisted of 55 participants (48%), of which 27 participants met SCID diagnostic criteria for schizophrenia, 18 bipolar disorder with psychosis, and 10 nonclinical control subjects. Cluster Two, Stable Ego Boundaries (SEB), consisted of 60 participants (52%), of which 17 participants met SCID diagnostic criteria for schizophrenia, 12 bipolar disorder with psychosis, and 31 non-clinical control subjects. As noted in Figure 2, “felt presence” (TQ31 and TQ14), the experience to “step outside” self (TQ9), “fluidity of thoughts and images” (TQ32), and the experience that things were “doubly real” (TQ11) contributed most to the identification of cluster subtypes in the primary cluster predictor algorithm, while experiences of “delighting in” (TQ23), “stimulate imagination” (TQ15) and feeling “moved by” (TQ2) were least predictive.
Figure 2. Cluster Predictor Importance.
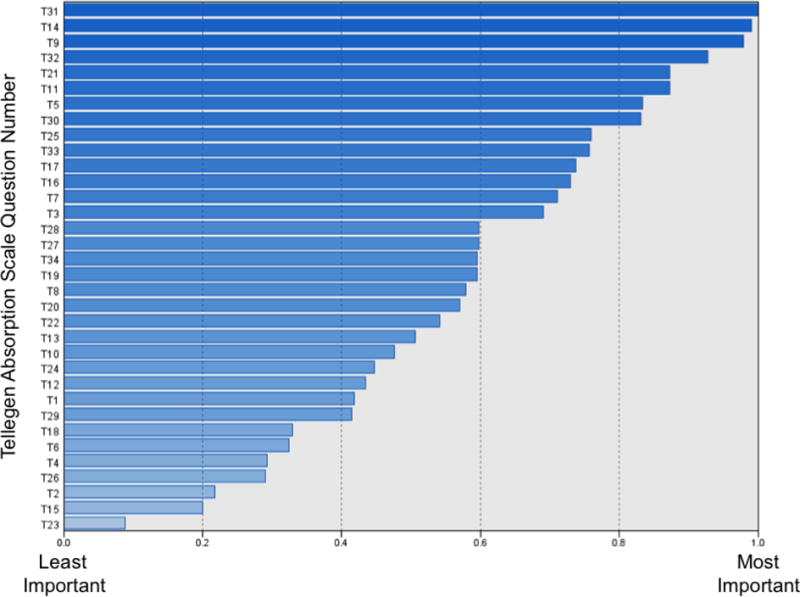
The cluster predictor importance measure of subgroups within TAS using the Two-Step cluster algorithm.
We next conducted Fisher exact tests to examine the supporting structures of individual items of the TAS in AEB compared to SEB clusters. We found significant differences in individual TAS items that reflect ego-disturbances of ‘self and environment’, ‘self and others’, and ‘self with one’s own thoughts’. For example, there was a significant difference between AEB compared to SEB clusters in ‘self and environment’ grouping that includes items such as “I feel as if my mind could envelop the whole world” (TQ5), (p<0.000, Fisher exact test); “I often have physical memories…after I have been swimming I am still feel as if I am still in the water (TQ29),(p<0.000, Fisher exact test); or a merging of senses as in “different odors have different colors” (TQ33), (p<0.000, Fisher exact test). We also found a significant difference between AEB versus SEB clusters in experiences of attenuated ego boundaries between ‘self and others’ grouping which includes items such as, “I sometimes sense the presence of another person before I actually see him/her (TQ14), (p<0.000, Fisher exact test) and ‘self and owns own thoughts’ grouping which includes items such as “sometimes thoughts and images come to me without the slightest effort on my part” (TQ32), (p<0.000, Fisher exact test). In all instances, AEB participants were more likely to endorse TAS items that capture this diffusion of ego demarcation.
Our data demonstrate a significant diagnostic difference between the cluster groups with a higher percentage of participants with schizophrenia in the AEB cluster (p<0.001). Diagnostic differences in AEB compared to SEB clusters in relation to persons with bipolar disorder with psychosis and non-clinical controls were analyzed using Fisher exact tests and show a significant difference between groups (p<0.003, Fisher’s exact test). The analysis indicated that a higher percentage of person with Bipolar disorder with psychosis were categorized to the AEB cluster and conversely, a higher percentage of non-clinical controls were categorized to the SEB cluster.
Lastly, we conducted an independent sample t-test to compare PANSS 5-factor subscales comparing the Attenuated Ego Boundaries (AEB) and Stable Ego Boundaries (SEB) factor groups. There was a significant increase in PANSS positive factor scores (t113=4.98, p=0.001) in the AEB cluster compared to the SEB cluster. We also found significantly higher rates of PANSS cognitive factor scores (t113=3.96, p=0.001) in the AEB cluster compared to the SEB cluster. Additionally, there was a significant elevation in PANSS excitement factor scores (t113=3.38, p=0.001) and PANSS depression factor scores (t113=5.30, p=0.001) in the AEB cluster compared to the SEB cluster. However, there were no significant differences between cluster groups in PANSS negative factor scores.
4. Discussion
We found that absorption, operationalized as the capacity and tendency for deep immersion in perceptual stimuli and/or mental imagery was significantly elevated in clinical participants with a schizophrenia diagnosis compared to controls, and elevated, though not to a significant degree, in participants with affective psychosis. Absorption scores correlated significantly with most types of hallucinations and many forms of delusions. We also found that a subset of absorption items, specifically those involving the dissolution or temporary alteration of ego boundaries, as well as synthaesthetic experiences such as a fluidity of thoughts and images, formed a cluster with a significantly higher percentage of schizophrenia spectrum subjects. Membership in the AEB group also predicted higher positive symptoms. Importantly, however, some bipolar and non-clinical participants were also categorized as members of this cluster, suggesting that absorption may be an important dimension of psychosis (or psychotic like experiences) understood not as a categorical construct but a dimensional population level continuum. This finding aligns with prior research finding elevated absorption scores among healthy adults with psychotic-like experiences (Humpston et al., 2016).
4.1. Absorption, Aberrant Salience & Hyperreflexivity
While absorption has received relatively little attention in the schizophrenia literature, aberrant salience, as noted above, is viewed as a core phenomenological construct and linked directly to hyper-dopaminergic processes (Gray, Feldon, Rawlins, Hemsley and Smith, 1991; Kapur, 2003; Howes & Kapur, 2009). Aberrant attributions of salience and the perception of special meaning associated with socioenvironmental perceptions have in turn been tied to phenomenological theories of psychosis as a self-disorder involving foundational disruptions to the basic sense of self (Sass & Parnas, 2003; Parnas, 2011; Sass, 2001; Nelson & Raballo, 2015). Specifically, Sass, Parnas and colleagues have posited hyperreflexivity, or the self-conscious experience of what are normally tacit or pre-reflective events and perceptions, as a foundational component of psychosis. Once they are no longer experienced as taken-for-granted and arising prior to and outside of reflective awareness, a subject’s own thoughts may come to feel strange and object-like, as if they had originated elsewhere. Eventually, in synergistic combination with other factors and processes, such object-like thoughts may be asserted as autochthonous thoughts, “voices” or delusions of thought-control (Stanghellini, 2004; de Vries et al., 2013).
Together, aberrant salience and disturbed sense of basic self have been posited as core drivers of the psychotic experience (Moller & Husby, 2000; Bell, Halligan, & Ellis, 2006; B. Nelson, Whitford, Lavoie, & Sass, 2014b; Nelson, Whitford, Lavoie, & Sass, 2014a). However, our research suggests that absorption, particularly as it implicates altered ego boundaries, including the temporary loss of a more clearly delineated self, and the blurring of cognitive and sensory modalities, may also represent a core predisposition that precedes the onset of acute psychosis and subsequently capacitates the development and maintenance of frank positive symptomatology. Contrasted with aberrant salience, absorption potentially represents the tendency or ability to “lose oneself” in the act of perception. A personality-driven tendency to blur modalities (e.g. imagery and thoughts) may further contribute to the transformation of instances of aberrant salience and/or other alterations of self-experience into relatively ‘fixed’ hallucinations or delusions.
Returning to our study, the significant differences in absorption scores between the three groups, showing the non-clinical sample with the lowest mean score of absorption and the participants with schizophrenia with highest mean score of absorption, supports the contention that while absorption is a population-level continua construct, and conventionally theorized as a ‘normal’ personality characteristic, heightened levels of absorption are nevertheless found in those with psychotic disorders. This finding is consistent with other studies that have reported an association between absorption, hallucinatory experiences and ASEs (Glicksohn & Barrett, 2003; Humpston et al., 2016; Perona-Garcelan et al., 2012).
In keeping with this dimensional approach, we also examined the correlation between TAS and types of hallucinations and forms of delusions. We found that absorption is highly sensitive to alterations in sensory-perceptual experiences as seen in all types of hallucinations, as well as delusions involving alterations of self and/or thought (e.g. delusions of reference, thought withdrawal, thought insertion). These findings align with phenomenological conceptualizations of schizophrenia that distinguish between “understandable” thematic delusions (such as jealousy and guilt) and more bizarre alterations of experience ostensibly grounded in basic alterations of self (Cermolacce, Sass, & Parnas, 2010; J. Parnas, 2004; (Schneider, 1959; Rosen, Grossman, Harrow, Bonner-Jackson, & Faull, 2011; Rosen et al., 2016b). These findings also build on prior research suggesting a distinction between voices and thought delusions, and between voices and thematic delusions (Rosen et al., 2016a). Thought delusions are a cluster of delusions that typically revolve around alterations in basic sense of self and the fluidity of internal/external boundaries, while thematic type delusions cluster around exaggerated processes of social internalization (e.g. guilt) or externalization (jealousy/delusions of infidelity). Our findings regarding absorption in the current project suggest a potentially provocative role for absorption as a further dimension of altered self experience that maps more strongly onto thought delusions than thematic delusions, and also more strongly onto schizophrenia (traditionally associated with bizarre, non-thematic delusions) than affective psychosis.
We also note that while quantitative measures of absorption are under-represented in the psychosis literature, descriptions that clearly map onto absorption are common in the qualitative phenomenology literature. For example:
“I developed a greater awareness of…. My senses were sharpened. I became fascinated by little insignificant things around me” (Bowers & Freedman, 1966; Kapur, 2003)
“I felt that there was some overwhelming significance in this” (McDonald, 1960)
“My capacities for aesthetic appreciation and heightened sensory receptiveness…were very keen. I had had the same intensity of experience at other times when I was normal, but such periods were not sustained for long and had also been integrated with other feelings” (1955) (Kapur, 2003).
“…sometimes an object really seems to stand out from the rest of what I see. My eyes then fix on it. It’s like being spellbound, even though I don’t want to look at it at all” (Schultze-Lutter, 2009)
“I become everything I experience to a point where it ultimately resolves into a state of considering myself the universe. I can open myself completely. It means my sense of identity is expanded and there is no longer a me” (Lysaker & Lysaker, 2010)
“I feel the mental states of others and I can no more find myself sometimes, I vibrate with things around me, and when I watch a person or a thing, I become part of it” (Stanghellini & Ballerini, 2011).
Absorption is not only a potentially important phenomenological target for further unpacking the subjective and psychological pathogenesis of psychosis, but also for further delineating the intersections of altered sense of self, absorption, aberrant salience as they intersect in the initial development of psychosis (Parnas, Handest, Saebye, & Jansson, 2003; Parnas, 2000; Parnas & Sass, 2001).
4.2. Absorption and ego-boundary sub-types
Absorption has been characterized as an intense experience of the object of attention accompanied by impermeability to other, potentially distracting stimuli (Tellegen & Atkinson, 1974). Tellegen and Atkinson (1974; S. 268) defined absorption as “a disposition for having episodes of ‘total’ attention that fully engage one’s representational (i.e., perceptual, enactive, imaginative, and ideational) resources.” The focus of attention is either narrowed or widened, so that the person enters an altered state of consciousness. Jamieson, 2005 expanded his definition of absorption to include “the capacity for marked restructuring of one’s phenomenal field, especially sense of self and its boundaries.” It has been hypothesized that full-fledged hallucinations and delusions are downstream from a more core alteration of basic self-experience, while increased salience is often reported in conjunction with increased self-disturbance (Sass, 2014). Hallucinations and delusions may arise on a similar path as a result of aberrant attribution of salience (Gray 1995; Kapur, 2003). Research has shown that when compared to individuals who do not experience AVH, individuals who do experience AVH, have a strongly focused attention style that is self-focused towards private events (Jamieson, 2005; Perona-Garcelan et al., 2008).
Along these lines, McGurk and MacDonald (1976) showed that perception is multisensory, in that auditory and visual experience can be fused, and that in the absence of a dominant sensory modality, such as visual or auditory inputs, information processing can become disturbed. Similarly, the phenomenological experience of absorption can involve a fusion of a multisensory saturation and diminished ego-demarcation. Of particular interest is our finding of two distinct clusters within the framework of absorption as a layer together with aberrant salience and self-disturbance: Attenuated Ego Boundaries (AEB) and Stable Ego Boundaries. The phenomenological structure of these clusters when mapped on to clinical symptomology such as PANSS factor domains for positive symptoms, cognitive deficits, excitement, and depression support the hypothesis that absorption and alteration in self-other boundaries interrelate within the architecture of psychosis. This finding is in keeping with the work of other researchers who have suggested that the sub-clinical phenomenological changes in the basic symptom structure in connection with changes in sense of self-demarcate differential parameters often seen in early onset of illness, residual states and symptom exacerbation. These subclinical alterations lead to impaired source monitoring and positive symptoms that may result from alterations in self-experience (Gross & Huber, 2010; Postmes et al., 2014); Parnas & Sass, 2001; Sass & Parnas, 2003).
4.3. Limitations
The limitations of this study include a modest number of participants across the samples. However, few studies that have focused on subjective perception in psychosis have reported greater sample size. Another limitation to the generalizability of these results is that the data are based largely on self-report. Culture significantly influences the subjective experience of psychosis and our results may not generalize to other regions and populations. Given established links between spiritual experience/openness and absorption, research explicitly designed to unpack this intersection (spirituality, psychosis and absorption) is also needed. An additional limitation of the study is that we did not apply an instrument that could measure both absorption and depersonalization in parallel. Finally, this is a cross sectional study and cannot directly address the potentially causal or mechanistic role of absorption in the development of psychosis. For instance, it is possible that elevated absorption in our sample was a consequence, rather than a cause, of participants’ altered thoughts and perceptions. We nevertheless believe that this study provides relevant results that contribute to the understanding of the role of absorption as it relates to self-disorder, aberrant salience and psychosis.
4.4. Self, salience, psychosis and clinical implications
Cognitive behavioral therapy for psychosis (CBTp) is the recommended first-line psychosocial treatment for hallucinations and delusions (Lehman et al., 2004; National Collaborating Centre for Mental Health, 2014). However, CBTp is not always effective, and researchers are actively exploring other treatment strategies (Farhall & Thomas, 2013). Likewise, often there is only a suboptimal response to antipsychotic medications leaving residual symptoms such as hallucination and delusions active. An orientation to absorption rather than the more cognitive mechanisms of psychosis may suggest that value of approaches that focus on embodied states (or the embodiment of emotions), mindfulness and awareness of self and world (Fielding-Smith et al., 2015; Stanghellini & Lysaker, 2007; Lysaker & Dimaggio, 2014). In addition, the quasi-agentive nature of absorption further underscores the potential clinical importance of greater attention to the role of agency in the subjective experience of psychosis and the clinical implications of agentive processes (Jones et al., 2016). These include the potential to engage much more directly with clinical high risk and/or early psychosis clients to capitalize on existing self-awareness and agency and to explicitly attend to the role of perceptual and cognitive absorption as well as altered salience before these experiences are submerged in full-fledged hallucinations and delusions.
5. Conclusion and future directions
The present study provides cross-sectional evidence that absorption exists along a continuum in non-clinical and clinical populations. This present study also validates the hypothesis that increased levels of absorption and associated self-disturbance significantly correlate with schizophrenia and are also elevated in affective psychosis. As an earlier description of the subjective experience by a person with schizophrenia noted, “What I do want to explain, if I can, is the exaggerated state of awareness in which I lived before and after my acute illness…” (MacDonald, 1960). Our research suggests a potentially important and under-investigated subjective component of psychotic experience that overlaps with, but is not identical to, the constructs of aberrant salience and hyperreflexivity. Our findings also suggest that the phenomenology of absorption and self-disorder are particularly sensitive to shifts in perceptual intersensory and multisensory experiences of both a narrowing of external connectivity, and simultaneously, an expansion of internal connectivity. Studying changes in early alterations of perception may improve early detection, the definition and differentiation of residual states, and identification of subtle shifts that can precede symptom exacerbation or relapses (Gray 1995; Kapur, 2003; Sass & Parnas, 2003; Schultze-Lutter, 2009). Future research should further unpack these phenomenological distinctions.
Acknowledgments
The authors would like to thank all the individuals who participated in this study.
Funding: This work was supported in part by PHS grant (NIH) R01MH094358 (R.P.S.)
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Beards S, Gayer-Anderson C, Borges S, Dewey ME, Fisher HL, Morgan C. Life events and psychosis: A review and meta-analysis. Schizophrenia Bulletin. 2013;39(4):740–747. doi: 10.1093/schbul/sbt065. doi:10.1093/schbul/sbt065 [doi] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bell V, Halligan PW, Ellis HD. Explaining delusions: A cognitive perspective. Trends in Cognitive Sciences. 2006;10(5):219–226. doi: 10.1016/j.tics.2006.03.004. doi:S1364-6613(06)00076-3 [pii] [DOI] [PubMed] [Google Scholar]
- Bowers MB, Jr, Freedman DX. “Psychedelic” experiences in acute psychoses. Archives of General Psychiatry. 1966;15(3):240–248. doi: 10.1001/archpsyc.1966.01730150016003. [DOI] [PubMed] [Google Scholar]
- Braver TS, Krug MK, Chiew KS, Kool W, Westbrook JA, Clement NJ, MOMCAI group Mechanisms of motivation-cognition interaction: Challenges and opportunities. Cognitive, Affective & Behavioral Neuroscience. 2014;14(2):443–472. doi: 10.3758/s13415-014-0300-0. doi:10.3758/s13415-014-0300-0 [doi] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brebion G, Ohlsen RI, Pilowsky LS, David AS. Visual hallucinations in schizophrenia: Confusion between imagination and perception. Neuropsychology. 2008;22(3):383–389. doi: 10.1037/0894-4105.22.3.383. doi:10.1037/0894-4105.22.3.383 [doi] [DOI] [PubMed] [Google Scholar]
- Castillo RJ. Trance, functional psychosis, and culture. Psychiatry. 2003;6(1) doi: 10.1521/psyc.66.1.9.20285. 17-17-34. [DOI] [PubMed] [Google Scholar]
- Cermolacce M, Sass L, Parnas J. What is bizarre in bizarre delusions? A critical review. Schizophrenia Bulletin. 2010;36(4):667–679. doi: 10.1093/schbul/sbq001. doi:10.1093/schbul/sbq001 [doi] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chase KA, Cone JJ, Rosen C, Sharma RP. The value of interleukin 6 as a peripheral diagnostic marker in schizophrenia. BMC Psychiatry. 2016 doi: 10.1186/s12888-016-0866-x. 1-1-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chiu T, Fang D, Chen J, Wang Y, Jeris C. Proceedings of the Seventh ACM SIGKDD International Conference on Knowledge Discovery and Data Mining. San Francisco, CA: ACM; 2001. A robust and scalable clustering algorithm for mixed type attributes in large database environment. [Google Scholar]
- Corlett PR, Taylor JR, Wang XJ, Fletcher PC, Krystal JH. Toward a neurobiology of delusions. Progress in Neurobiology. 2010;92(3):345–369. doi: 10.1016/j.pneurobio.2010.06.007. doi:10.1016/j.pneurobio.2010.06.007 [doi] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davis KL, Kahn RS, Ko G, Davidson M. Dopamine in schizophrenia: A review and reconceptualization. The American Journal of Psychiatry. 1991;148(11):1474–1486. doi: 10.1176/ajp.148.11.1474. doi:10.1176/ajp.148.11.1474 [doi] [DOI] [PubMed] [Google Scholar]
- de Vries R, Heering HD, Postmes L, Goedhart S, Sno HN, de Haan L. Self-disturbance in schizophrenia: A phenomenological approach to better understand our patients. The Primary Care Companion to CNS Disorders. 2013;15(1) doi: 10.4088/PCC.12m01382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dollfus S, Everitt B, Ribeye JM, Assouly-Besse F, Sharp C, Petit M. Identifying subtypes of schizophrenia by cluster analyses. Schizophr Bull. 1996;22(3) doi: 10.1093/schbul/22.3.545. 545-545-555. [DOI] [PubMed] [Google Scholar]
- Farhall J, Thomas N. Cognitive and behavioural therapies for psychosis. The Australian and New Zealand Journal of Psychiatry. 2013;47(6):508–511. doi: 10.1177/0004867413483370. doi:10.1177/0004867413483370 [doi] [DOI] [PubMed] [Google Scholar]
- Farmer AE, McGuffin P, Spitznagel EL. Heterogeneity in schizophrenia: A cluster-analytic approach. Psychiatry Research. 1983;8(1):1–12. doi: 10.1016/0165-1781(83)90132-4. doi:0165-1781(83)90132-4 [pii] [DOI] [PubMed] [Google Scholar]
- Fielding-Smith SF, Hayward M, Strauss C, Fowler D, Paulik G, Thomas N. Bringing the “self” into focus: Conceptualising the role of self-experience for understanding and working with distressing voices. Frontiers in Psychology. 2015;6:1129. doi: 10.3389/fpsyg.2015.01129. doi:10.3389/fpsyg.2015.01129 [doi] [DOI] [PMC free article] [PubMed] [Google Scholar]
- First M, Spitzer R, Gibbon M, Williams J. Structured clinical interview for DSM-IV-TR axis I disorders, research version, patient edition. Biometrics Research 2002 [Google Scholar]
- Frischholz EJ, Braun BG, Sachs RG, Schwartz DR, Lewis J, Shaeffer D, Pasquotto J. Construct validity of the dissociative experiences scale: II. its relationship to hypnotizability. The American Journal of Clinical Hypnosis. 1992;35(2):145–152. doi: 10.1080/00029157.1992.10402997. doi:10.1080/00029157.1992.10402997 [doi] [DOI] [PubMed] [Google Scholar]
- Glicksohn J, Barrett TR. Absorption and hallucinatory experience. Applied Cognitive Psychology. 2003;17 833-833-849. [Google Scholar]
- Gray JA, Feldon J, Rawlins JNP, Hemsley DR, Smith AD. The neuropsychology of schizophrenia. Behavioral and Brain Science. 1991;14:56–84. [Google Scholar]
- Gray JA. Dopamine release in the nucleus accumbens: the perspective from aberrations of consciousness in schizophrenia. Neuropsychologia. 1995;33(9):1143–53. doi: 10.1016/0028-3932(95)00054-7. [DOI] [PubMed] [Google Scholar]
- Gross G, Huber G. The history of the basic symptom concept. Acta Clinica Croatica. 2010;49(2) [Google Scholar]
- Gross G, Huber G, Klosterkotter J, Linz M. BSABS bonn scale for the assessment of basic symptoms. 1st. Germany: Shaker Verlag; 2008. [Google Scholar]
- Gross G, Huber G, Klosterkotter J, Linz M. BSABS bonner skala fur die beurteilung von basissymptomen. manual, kommentar, dokumentationsbogen. Springer; Berlin: 1987. (Ed.) [Google Scholar]
- Haugen MC, Castillo RJ. Unrecognized dissociation in psychotic outpatients and implications of ethnicity. The Journal of nervous and mental disease. 1999;187(12):751–754. doi: 10.1097/00005053-199912000-00007. [DOI] [PubMed] [Google Scholar]
- Howes OD, Kapur S. The dopamine hypothesis of schizophrenia: Version III–the final common pathway. Schizophrenia Bulletin. 2009;35(3):549–562. doi: 10.1093/schbul/sbp006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Humpston CS, Walsh E, Oakley DA, Mehta MA, Bell V, Deeley Q. The relationship between different types of dissociation and psychosis-like experiences in a non-clinical sample. Consciousness and Cognition. 2016;41:83–92. doi: 10.1016/j.concog.2016.02.009. [DOI] [PubMed] [Google Scholar]
- Isvoranu AM, Borsboom D, van Os J, Guloksuz S. A network approach to environmental impact in psychotic disorder: Brief theoretical framework. Schizophrenia Bulletin. 2016 doi: 10.1093/schbul/sbw049. doi:sbw049 [pii] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jamieson GA. The modified tellegen absorption scale: A clearer window on the stucture and meaning of absorption. Australian Journal of Clinical and Experimental Hypnosis. 2005;33(2) 119-119-139. [Google Scholar]
- Jaspers K. General psychopathology. Chicago, IL: 1963. [Google Scholar]
- Jaspers K. The phenomenological approach in psychopathology. The British Journal of Psychiatry: The Journal of Mental Science. 1968;114(516):1313–1323. doi: 10.1192/bjp.114.516.1313. [DOI] [PubMed] [Google Scholar]
- Jensen J, Walter H. Incentive motivational salience and the human brain. Restorative Neurology and Neuroscience. 2014;32(1):141–147. doi: 10.3233/RNN-139006. doi:10.3233/RNN-139006 [doi] [DOI] [PubMed] [Google Scholar]
- Jones N, Luhrmann T. Beyond the sensory: Findings from an in-depth analysis of the phenomenology of ‘auditory hallucinations’ in schizophrenia. Psychosis. 2015 doi: 10.1080/17522439.2015.1100670. [DOI] [Google Scholar]
- Jones N, Shattell M, Kelly T, Brown R, Robinson L, Renfro R, Luhrmann T. Did I push myself over the edge?: Complications of agency in psychosis onset and development. Psychosis. 2016 doi: 10.1080/17522439.2016.1150501. [DOI] [Google Scholar]
- Kapur S. Psychosis as a state of aberrant salience: A framework linking biology, phenomenology, and pharmacology in schizophrenia. The American Journal of Psychiatry. 2003;160(1):13–23. doi: 10.1176/appi.ajp.160.1.13. doi:10.1176/appi.ajp.160.1.13 [doi] [DOI] [PubMed] [Google Scholar]
- Kay SR, Fiszbein A, Opler L. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophrenia Bulletin. 1987;13(2) doi: 10.1093/schbul/13.2.261. 261-261-276. [DOI] [PubMed] [Google Scholar]
- Lang UE, Puls I, Muller DJ, Strutz-Seebohm N, Gallinat J. Molecular mechanisms of schizophrenia. Cellular Physiology and Biochemistry: International Journal of Experimental Cellular Physiology, Biochemistry, and Pharmacology. 2007;20(6):687–702. doi: 10.1159/000110430. doi:10.1159/000110430 [doi] [DOI] [PubMed] [Google Scholar]
- Lehman AF, Lieberman JA, Dixon LB, McGlashan TH, Miller AL, Perkins DO, Steering Committee on Practice Guidelines Practice guideline for the treatment of patients with schizophrenia, second edition. The American Journal of Psychiatry. 2004;161(2 Suppl):1–56. [PubMed] [Google Scholar]
- Lehoux C, Gobeil MH, Lefebvre AA, Maziade M, Roy MA. The five-factor structure of the PANSS: A critical review of its consistency across studies. Clinical Schizophrenia and Related Psychoses. 2009;3(2) 103-103-110. [Google Scholar]
- Lindenmayer JP, Bernstein-Hyman R, Grochowski S. Five-factor model of schizophrenia. initial validation. The Journal of Nervous and Mental Disease. 1994;182(11):631–638. doi: 10.1097/00005053-199411000-00006. [DOI] [PubMed] [Google Scholar]
- Luhrmann TM. The art of hearing God: Absorption, dissociation, and contemporary American spirituality. Spiritus: A Journal of Christian Spirituality. 2005;5(2):133–157. [Google Scholar]
- Luhrmann TM, Nusbaum H, Thisted R. The absorption hypothesis: Learning to hear god in evangelical christianity. American Anthropologist. 2010;112(1) 66-66-78. [Google Scholar]
- Lysaker PH, Dimaggio G. Metacognitive capacities for reflection in schizophrenia: Implications for developing treatments. Schizophrenia Bulletin. 2014;40(3):487–491. doi: 10.1093/schbul/sbu038. doi:10.1093/schbul/sbu038 [doi] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lysaker PH, Lysaker JT. Schizophrenia and alterations in self-experience: A comparison of 6 perspectives. Schizophrenia Bulletin. 2010;36(2):331–340. doi: 10.1093/schbul/sbn077. doi:10.1093/schbul/sbn077 [doi] [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacDonald N. Living with schizophrenia. Canadian Medical Association Journal. 1960;82:218–221. [PMC free article] [PubMed] [Google Scholar]
- McDonald N. Living with schizophrenia. Can Med Assoc J. 1960;82:218–221. [PMC free article] [PubMed] [Google Scholar]
- McGurk H, MacDonald J. Hearing lips and seeing voices. Nature. 1976;264(5588):746–748. doi: 10.1038/264746a0. [DOI] [PubMed] [Google Scholar]
- Moller P, Husby R. The initial prodrome in schizophrenia: Searching for naturalistic core dimensions of experience and behavior. Schizophrenia Bulletin. 2000;26(1):217–232. doi: 10.1093/oxfordjournals.schbul.a033442. [DOI] [PubMed] [Google Scholar]
- Morrison RL, Bellack AS, Wixted JT, Mueser KT. Positive and negative symptoms in schizophrenia. A cluster-analytic approach. The Journal of Nervous and Mental Disease. 1990;178(6):377–384. doi: 10.1097/00005053-199006000-00006. [DOI] [PubMed] [Google Scholar]
- National Collarborating Centre for Mental Health. Psychosis and schizophreni in adults: Treatment and management. Nice Clinical Guideline. 2014;178 1-1-59. [Google Scholar]
- Nelson B, Sass LA. Medusa’s stare: A case study of working with self-disturbance in the early phase of schizophrenia. Clinical Case Studies. 2009;8:489. doi: 10.1177/1534650109351931. [DOI] [Google Scholar]
- Nelson B, Raballo A. Basic self-disturbance in the schizophrenia spectrum: Taking stock and moving forward. Psychopathology. 2015;48(5):301–309. doi: 10.1159/000437211. doi:10.1159/000437211 [doi] [DOI] [PubMed] [Google Scholar]
- Nelson B, Whitford TJ, Lavoie S, Sass LA. What are the neurocognitive correlates of basic self-disturbance in schizophrenia? integrating phenomenology and neurocognition: Part 2 (aberrant salience) Schizophrenia Research. 2014a;152(1):20–27. doi: 10.1016/j.schres.2013.06.033. doi:10.1016/j.schres.2013.06.033 [doi] [DOI] [PubMed] [Google Scholar]
- Nelson B, Whitford TJ, Lavoie S, Sass LA. What are the neurocognitive correlates of basic self-disturbance in schizophrenia?: Integrating phenomenology and neurocognition. part 1 (source monitoring deficits) Schizophrenia Research. 2014b;152(1):12–19. doi: 10.1016/j.schres.2013.06.022. doi:10.1016/j.schres.2013.06.022 [doi] [DOI] [PubMed] [Google Scholar]
- Parnas J. The self and intentionality in the pre-psychotic stages of schizophrenia 2000 [Google Scholar]
- Parnas J. Belief and pathology of self-awareness. Journal of Consciousness Studies. 2004;11(10–11) 148-148-161. [Google Scholar]
- Parnas J, Sass LA. Solipsism, self, and schizophrenic delusions. Philos Psychiatry Psychol. 2001;8 101-101-120. [Google Scholar]
- Parnas J. A disappearing heritage: The clinical core of schizophrenia. Schizophrenia Bulletin. 2011;37(6):1121–1130. doi: 10.1093/schbul/sbr081. doi:10.1093/schbul/sbr081 [doi] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Parnas J, Handest P, Jansson L, Saebye D. Anomalous subjective experience among first-admitted schizophrenia spectrum patients: Empirical investigation. Psychopathology. 2005;38(5):259–267. doi: 10.1159/000088442. [DOI] [PubMed] [Google Scholar]
- Parnas J, Handest P, Saebye D, Jansson L. Anomalies of subjective experience in schizophrenia and psychotic bipolar illness. Acta Psychiatrica Scandinavica. 2003;108(2):126–133. doi: 10.1034/j.1600-0447.2003.00105.x. doi:105 [pii] [DOI] [PubMed] [Google Scholar]
- Parnas J, Moller P, Kircher T, Thalbitzer J, Jansson L, Handest P, Zahavi D. EASE: Examination of anomalous self-experience. Psychopathology. 2005;38(5):236–258. doi: 10.1159/000088441. doi:88441 [pii] [DOI] [PubMed] [Google Scholar]
- Perona-Garcelán S, García-Montes JM, Rodríguez-Testal JF, Ruiz-Veguilla M, Benítez-Hernández MDM, López-Jiménez AM, Pérez-Álvarez M. Relationship of absorption, depersonalisation, and self-focused attention in subjects with and without hallucination proneness. Cognitive Neuropsychiatry. 2013;18(5) doi: 10.1080/13546805.2012.728133. [DOI] [PubMed] [Google Scholar]
- Perona-Garcelan S, Cuevas-Yust C, Garcia-Montes JM, Perez-Alvarez M, Ductor-Recuerda MJ, Salas-Azcona R, Rodriguez-Martin B. Relationship between self-focused attention and dissociation in patients with and without auditory hallucinations. The Journal of Nervous and Mental Disease. 2008;196(3):190–197. doi: 10.1097/NMD.0b013e318165c7c1. doi:10.1097/NMD.0b013e318165c7c1 [doi] [DOI] [PubMed] [Google Scholar]
- Perona-Garcelan S, Garcia-Montes JM, Ductor-Recuerda MJ, Vallina-Fernandez O, Cuevas-Yust C, Perez-Alvarez M, Gomez-Gomez MT. Relationship of metacognition, absorption, and depersonalization in patients with auditory hallucinations. The British Journal of Clinical Psychology/the British Psychological Society. 2012;51(1):100–118. doi: 10.1111/j.2044-8260.2011.02015.x. doi:10.1111/j.2044-8260.2011.02015x [doi] [DOI] [PubMed] [Google Scholar]
- Postmes L, Sno HN, Goedhart S, van der Stel J, Heering HD, de Haan L. Schizophrenia as a self-disorder due to perceptual incoherence. Schizophrenia Research. 2014;152(1):41–50. doi: 10.1016/j.schres.2013.07.027. doi:10.1016/j.schres.2013.07.027 [doi] [DOI] [PubMed] [Google Scholar]
- Rosen C, Jones N, Chase KA, Gin H, Grossman LS, Sharma RP. The intrasubjectivity of self, voices and delusions: A phenomenological analysis. Psychosis. 2016a:1–12. doi: 10.1080/17522439.2016.1162839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosen C, Chase KA, Jones N, Grossman LS, Gin H, Sharma RP. Listening to schneiderian voices: A novel phenomenological analysis. Psychopathology. 2016b doi: 10.1159/000446546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosen C, Grossman LS, Harrow M, Bonner-Jackson A, Faull R. Diagnostic and prognostic significance of schneiderian first-rank symptoms: A 20-year longitudinal study of schizophrenia and bipolar disorder. Comprehensive Psychiatry. 2011;52(2):126–131. doi: 10.1016/j.comppsych.2010.06.005. doi:10.1016/j.comppsych.2010.06.005 [doi] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roth TL, Lubin FD, Sodhi M, Kleinman JE. Epigenetic mechanisms in schizophrenia. Biochimica Et Biophysica Acta. 2009;1790(9):869–877. doi: 10.1016/j.bbagen.2009.06.009. doi:10.1016/j.bbagen.2009.06.009 [doi] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sass LA. Self and world in schizophrenia: Three classic approaches. Philos Psychiatry Psychol. 2001 108-108-112. [Google Scholar]
- Sass LA. Phenomenology as description and as explanation: The case of schizophrenia. Springer; Netherlands: 2010. [Google Scholar]
- Sass LA, Parnas J. Phenomenology of self-disturbance in schizophrenia: Some research findings and directions. Philosophy, Psychiatry and Psychology. 2001;8 347-347-356. [Google Scholar]
- Sass LA. Self-disturbance and schizophrenia: Structure, specificity, pathogenesis (current issues, new directions) Schizophrenia Research. 2014;152(1):5–11. doi: 10.1016/j.schres.2013.05.017. doi:10.1016/j.schres.2013.05.017 [doi] [DOI] [PubMed] [Google Scholar]
- Sass LA, Parnas J. Schizophrenia, consciousness, and the self. Schizophrenia Bulletin. 2003;29(3):427–444. doi: 10.1093/oxfordjournals.schbul.a007017. [DOI] [PubMed] [Google Scholar]
- Schneider K. Clinical psychopathology. Indiana University; Grune & Stratton: 1959. [Google Scholar]
- Schultze-Lutter F. Subjective symptoms of schizophrenia in research and the clinic: The basic symptom concept. Schizophrenia Bulletin. 2009;35(1):5–8. doi: 10.1093/schbul/sbn139;10.1093/schbul/sbn139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seeman P. Dopamine receptors and the dopamine hypothesis of schizophrenia. Synapse (New York, NY) 1987;1(2):133–152. doi: 10.1002/syn.890010203. doi:10.1002/syn.890010203 [doi] [DOI] [PubMed] [Google Scholar]
- Seeman P, Kapur S. Schizophrenia: More dopamine, more D2 receptors. Proceedings of the National Academy of Sciences of the United States of America. 2000;97(14):7673–7675. doi: 10.1073/pnas.97.14.7673. doi:97/14/7673 [pii] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stanghellini G. Disembodied spirits and deanimated bodies: The psychopathology of common sense. Oxford University Press; 2004. [Google Scholar]
- Stanghellini G, Ballerini M. What is it like to be a person with schizophrenia in the social world? A first-person perspective study on schizophrenic dissociality–part 2: Methodological issues and empirical findings. Psychopathology. 2011;44(3):183–192. doi: 10.1159/000322638. doi:10.1159/000322638 [doi] [DOI] [PubMed] [Google Scholar]
- Stanghellini G, Lysaker PH. The psychotherapy of schizophrenia through the lens of phenomenology: Intersubjectivity and the search for the recovery of first- and second-person awareness. American Journal of Psychotherapy. 2007;61(2):163–179. doi: 10.1176/appi.psychotherapy.2007.61.2.163. [DOI] [PubMed] [Google Scholar]
- Tagliazucchi E, Carhart-Harris R, Leech R, Nutt D, Chialvo DR. Enhanced repertoire of brain dynamical states during the psychedelic experience. Human Brain Mapping. 2014;35(11):5442–5456. doi: 10.1002/hbm.22562. doi:10.1002/hbm.22562 [doi] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tellegen A, Atkinson G. Openness to absorbing and self-altering experiences (“absorption”), a trait related to hypnotic susceptibility. Journal of Abnormal Psychology. 1974;83(3):268–277. doi: 10.1037/h0036681. [DOI] [PubMed] [Google Scholar]
- Tellegen A. Content categories: Absorption Items (Revised) University of Minnesota; 1982. Oct 10, Unpublished manuscript. [Google Scholar]
- van Os J, Bak M, Hanssen M, Bijl RV, de Graaf R, Verdoux H. Cannabis use and psychosis: A longitudinal population-based study. American Journal of Epidemiology. 2002;156(4):319–327. doi: 10.1093/aje/kwf043. [DOI] [PubMed] [Google Scholar]
- Varese F, Smeets F, Drukker M, Lieverse R, Lataster T, Viechtbauer W, Bentall RP. Childhood adversities increase the risk of psychosis: A meta-analysis of patient-control, prospective- and cross-sectional cohort studies. Schizophrenia Bulletin. 2012;38(4):661–671. doi: 10.1093/schbul/sbs050. doi:10.1093/schbul/sbs050 [doi] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Velligan DI. Cognitive behavior therapy for psychosis: Where have we been and where are we going? Schizophrenia Bulletin. 2009;35(5):857–858. doi: 10.1093/schbul/sbp076. doi:10.1093/schbul/sbp076 [doi] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Waters FA, Badcock JC. First-rank symptoms in schizophrenia: Reexamining mechanisms of self-recognition. Schizophrenia Bulletin. 2010;36(3):510–517. doi: 10.1093/schbul/sbn112. doi:10.1093/schbul/sbn112 [doi] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang T, Ramakrishnon R, Livny M. BIRCH: An efficient data clustering method for very large databases. Proceedings of the ACM SIGMOD Conference on Management of Data 1996 [Google Scholar]