

Abstract
Case summary
A 14-year-old, neutered male European shorthair cat was evaluated for a routine health check. The owner did not report any clinical signs except for respiratory stridor. On physical examination the main findings were broad facial features and increased interdental spaces. On haematology, a mild, non-regenerative anaemia was detected, whereas the serum biochemistry profile and urinalysis were unremarkable. The serum glucose concentration was within the reference interval. Serum insulin-like growth factor-1 concentration was markedly elevated (>1600 ng/ml). The basal serum growth hormone concentration was elevated and decreased only mildly after somatostatin administration. Basal serum insulin concentration was high, and the insulin concentration increased considerably after glucose loading, consistent with insulin resistance. CT scanning of the skull showed an enlarged pituitary gland and increased skull bone thickness. The final diagnosis was acromegaly.
Relevance and novel information
These findings demonstrate that acromegaly should be pursued and suspected in cats other than those with diabetes mellitus.
Introduction
Chronic hypersecretion of growth hormone (GH) by a functional somatotroph adenoma causes acromegaly, a disease characterised by insulin resistance and progressive overgrowth of connective tissue, bone and viscera. The clinical signs of the disease are mainly due to the catabolic effects of GH and the anabolic effects of insulin-like growth factor-1 (IGF-1).1,2 Excessive GH causes hypersecretion of IGF-1, predominantly by the liver, resulting in increased protein synthesis and excessive tissue growth. In addition, clinical signs may result from compression of the brain by a large somatotroph adenoma.
In cats, reported clinical features of acromegaly include prognathia inferior, broad face, enlarged paws, hypertrophic cardiomyopathy, abdominal organomegaly, respiratory stridor and increased body weight.1–7 However, these features appear gradually and often the only abnormality recognised in acromegalic cats is the presence of diabetes mellitus.8
The development of diabetes mellitus is associated with the catabolic effects of GH. These catabolic effects can mainly be attributed to a postreceptor defect in the action of insulin on target cells, leading to decreased carbohydrate utilisation, gluconeogenesis and reduced insulin sensitivity. The net effect of the catabolic actions of GH is promotion of hyperglycaemia. In people, hypersecretion of GH induces insulin resistance and glucose intolerance in 16–78% of cases and overt diabetes mellitus develops in 19–52% of acromegalic patients.9 In contrast, 100% of cats with acromegaly are reported to have diabetes mellitus.2 A veterinary textbook mentions that not all acromegalic cats have diabetes mellitus,10 but peer-reviewed articles about this issue are lacking. However, the present article describes a cat with acromegaly and insulin resistance that did not have diabetes mellitus.
Case description
A 14-year-old, neutered male European shorthair cat, with a body weight of 6.5 kg, was evaluated during an annual routine medical examination. The owner did not report any clinical problems except for respiratory stridor, which had started a few months before. On physical examination, morphological facial changes, such as broad facial features (Figure 1) and increased interdental spaces, were noticed. These anomalies were not evident in a photograph of the cat taken 3 years before presentation (Figure 1). Other abnormal clinical findings were a left systolic cardiac murmur (grade 1/6), mild dehydration and keratitis of the left eye. The only abnormal result on routine laboratory examination was a mild, non-regenerative anaemia (haematocrit 0.26 l/l; reference interval [RI] 0.30–0.45 l/l). Serum concentrations of urea, creatinine, total proteins, albumin, alkaline phosphatase, aspartate aminotransferase, alanine aminotransferase, gamma-glutamyl transferase, creatine kinase, cholesterol, bile acids, sodium, potassium, total calcium, phosphate and total thyroxin were within the respective RIs. Serum glucose concentration was 6.0 mmol/l (RI 4.7–6.4 mmol/l) and the serum fructosamine concentration was 352 μmol/l (RI 228–356 μmol/l). Urinalysis was unremarkable.
Figure 1.

A male European shorthair cat at (a) 11 years of age and at (b) 14 years of age, when acromegaly was diagnosed. Notice the morphological facial changes, such as broad facial features
The serum IGF-I concentration, measured by a commercially available radioimmunoassay system (RIA; Cambridge Specialist Laboratories Services), developed for humans and previously validated for cats,11 was significantly elevated (>1600 ng/ml; RI <800 ng/ml). Basal serum GH concentrations, measured by a commercially available RIA (PGH-46HK; Linco Research) for porcine, canine and feline GH were markedly elevated in two blood samples collected 15 mins apart (15 and 19 ng/ml, respectively; RI 0.8–7.2 ng/ml).12 These concentrations were the first two results of the somatostatin suppression test that was performed by collecting blood samples for measurement of the GH concentration at −15, 0, 15, 30 and 60 mins after the intravenous administration of 5 µg somatostatin (Somatostatina; IBP Pharma) per kg body weight.12 Serum GH concentration decreased mildly in the somatostatin suppression test but remained above 5 ng/ml (Figure 2).
Figure 2.
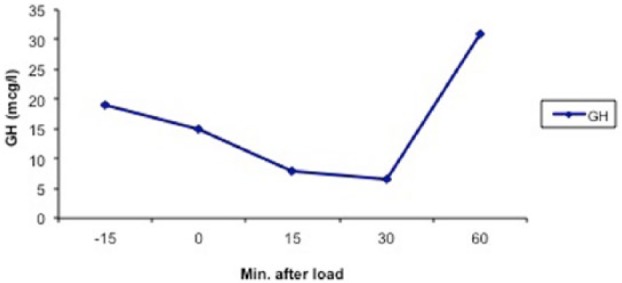
Serum growth hormone concentrations at −15, 0, 15, 30 and 60 mins after intravenous administration of 5 µg somatostatin per kg body weight in a 14-year-old male European shorthair cat with acromegaly but without diabetes mellitus
A glucose tolerance test was performed by giving a 50% glucose solution intravenously (0.5 g/kg body weight) and measuring concentrations of insulin and glucose at 0, 60 and 120 mins after glucose administration. Serum glucose concentrations were 7.3 mmol/l, 15.7 mmol/l and 5.0 mmol/l before and 60 and 120 mins after glucose loading, respectively. Basal serum insulin concentration was high (85 μlU/ml; RI 3.7–11.4 μlU/ml) and the insulin concentration became considerably higher at 60 mins after glucose loading (141 μlU/ml) and decreased at 120 mins after glucose loading (31 μlU/ml). Serum insulin to glucose ratios were 11.6 (RI 0.24–4.76), 9.0 (RI 1.04–7.04) and 6.2 (RI 0.84–5.62) before and at 60 and 120 mins after glucose loading, respectively.13 These results indicate that glucose tolerance was impaired, despite the absence of diabetes mellitus.
Thorax radiographs and echocardiography were unremarkable. CT was performed with a single-slice helical CT device (GE Fx/i). Imaging was performed with the cat in sternal recumbency under general anaesthesia. Transverse CT slices, in bone and soft tissue algorithm, were obtained from the tip of the nose to C2 with 3 mm thickness, while scanning of the pituitary region was done with 1 mm thickness pre- and postcontrast. CT examination showed an enlarged pituitary gland (4.0 mm in height, 6.6 mm in width, 4.5 in length) (Figure 3). A thickening of the cranial bones was also observed: parietal bone 6.4 mm (RI 2.3–3.5), frontal bone 4.0 mm (RI 0.2–2.6) and depth of skull 3.2 (RI 2.1–2.7) (Figure 4); moreover, the surface of the mandibular condyles was slightly concave bilaterally. CT scanning of the rest of the body was unremarkable.
Figure 3.
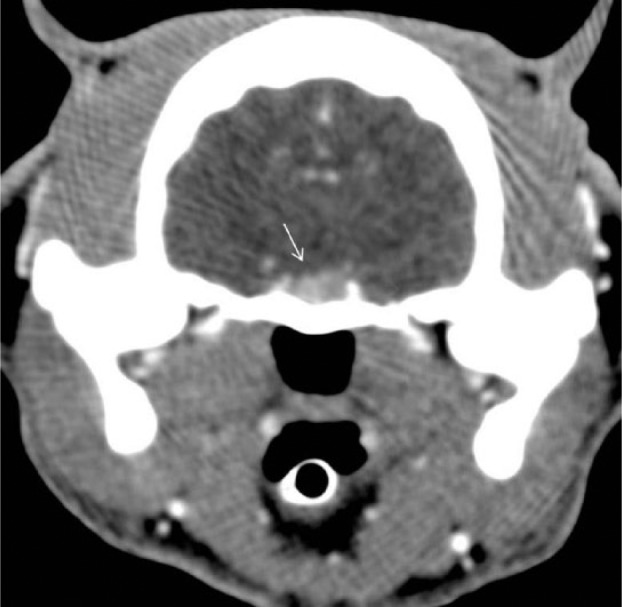
Transverse postcontrast CT image of the brain of a 14-year-old male European shorthair cat with acromegaly, showing an enlarged pituitary gland (arrow)
Figure 4.
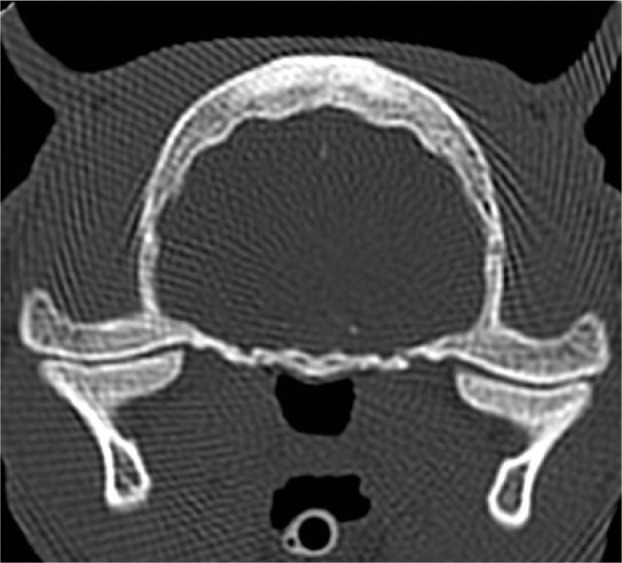
Transverse CT image of the skull of a 14-year-old male European shorthair cat with acromegaly, showing a thickened parietal bone and concave surface of the mandibular condyles
The final diagnosis was acromegaly without diabetes mellitus. Following diagnosis, blood glucose concentrations were measured at least twice a year and were always within the RI. Two years after the diagnosis the cat still did not have diabetes mellitus and was not receiving any treatment.
Discussion
In the cat presented herein, all basal serum glucose concentrations, measured on different occasions, were within the RI. Moreover, glucosuria was absent and serum fructosamine concentration was within the RI. These observations indicate that the cat did not have diabetes mellitus. However, the elevated serum insulin to glucose ratios and the strong rise in serum insulin concentration during the glucose tolerance test were consistent with insulin resistance.
The insulin resistance in this cat can be ascribed, at least partially, to acromegaly. The serum IGF-1 concentration was very high. However, an elevation of serum IGF-1 has been reported in apparently non-acromegalic diabetic cats,14,15 and therefore an elevation of serum IGF-1 concentration is not considered sufficient to provide a definitive diagnosis. The diagnosis in this cat was substantiated through the detection of consistent clinical signs, high serum GH concentrations that decreased only mildly after somatostatin administration and the finding of a pituitary mass and bone abnormalities on CT scan.
The intravenous administration of somatostatin caused a decrease in the serum GH concentration, which did not reach normal levels. Similar results were obtained in a population of cats with acromegaly, in which 5 µg/kg somatostatin was able to decrease but not normalise the plasma GH concentrations.12
CT documented the presence of a pituitary mass. In addition to pituitary morphology, feline acromegaly is associated with a number of CT abnormalities. The cat of this report showed the typical CT signs, such as thickening of the frontal and parietal bones, as described in previous studies.8,16
Conclusions
Feline acromegaly is not as rare as was thought in the past, and may be present in as many as 30% of poorly regulated or insulin-resistant diabetic cats.1,7 In line with this observation, the suspicion of feline acromegaly usually arises from cats with (insulin-resistant) diabetes mellitus. Furthermore, epidemiological studies concerning feline acromegaly have only evaluated populations of diabetic cats.
The present case demonstrates that acromegaly should not only be suspected in cats affected by diabetes mellitus, and that the prevalence of feline acromegaly may actually be higher if non-diabetic cats are included in future epidemiological studies.
Footnotes
Conflict of interest: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The authors received no financial support for the research, authorship, and/or publication of this article.
References
- 1. Niessen SJ, Petrie G, Gaudiano F, et al. Feline acromegaly: an underdiagnosed endocrinopathy? J Vet Intern Med 2007; 21: 899–905. [DOI] [PubMed] [Google Scholar]
- 2. Greco DS. Feline acromegaly. Top Companion Anim Med 2012; 27: 31–35. [DOI] [PubMed] [Google Scholar]
- 3. Peterson ME, Taylor RS, Greco DS, et al. Acromegaly in 14 cats. J Vet Intern Med 1990; 4: 192–201. [DOI] [PubMed] [Google Scholar]
- 4. Elliott DA, Feldman EC, Koblik PD, et al. Prevalence of pituitary tumors among diabetic cats with insulin resistance. J Am Vet Med Assoc 2000; 216: 1765–1768. [DOI] [PubMed] [Google Scholar]
- 5. Peterson ME. Acromegaly in cats: are we only diagnosing the tip of the iceberg? J Vet Intern Med 2007; 21: 889–891. [PubMed] [Google Scholar]
- 6. Berg RI, Nelson RW, Feldman EC, et al. Serum insulin-like growth factor-I concentration in cats with diabetes mellitus and acromegaly. J Vet Intern Med 2007; 21: 892–898. [DOI] [PubMed] [Google Scholar]
- 7. Niessen SJ. Feline acromegaly: an essential differential diagnosis for the difficult diabetic. J Feline Med Surg 2010; 12: 15–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Lamb CR, Ciasca TC, Mantis P, et al. Computed tomographic signs of acromegaly in 68 diabetic cats with hypersomatotropism. J Feline Med Surg 2014; 16: 99–108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Dreval AV, Trigolosova IV, Misnikova IV, et al. Prevalence of diabetes mellitus in patients with acromegaly. Endocr Connect 2014; 3: 93–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Feldman EC, Nelson RW. Disorders of growth hormone. In: Canine and feline endocrinology and reproduction. Feldman EC, Nelson RW. (eds). St Louis, MO: Saunders, 2004, pp 45–84. [Google Scholar]
- 11. Lewitt MS, Hazel SJ, Church DB, et al. Regulation of insulin-like growth factor-binding protein-3 ternary complex in feline diabetes mellitus. J Endocrinol 2000; 166: 21–27. [DOI] [PubMed] [Google Scholar]
- 12. Slingerland LI, Voorhout G, Rijnberk A, et al. Growth hormone excess and the effect of octreotide in cats with diabetes mellitus. Domest Anim Endocrinol 2008; 35: 352–361. [DOI] [PubMed] [Google Scholar]
- 13. Appleton DJ, Rand JS, Sunvold GD. Basal plasma insulin and homeostasis model assessment (HOMA) are indicators of insulin sensitivity in cats. J Feline Med Surg 2005; 7: 183–193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Starkey SR, Tan K, Church DB. Investigation of serum IGF-I levels amongst diabetic and non-diabetic cats. J Feline Med Surg 2004; 6: 149–155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Reusch CE, Kley S, Casella M, et al. Measurements of growth hormone and insulin-like growth factor 1 in cats with diabetes mellitus. Vet Rec 2006; 158: 195–200. [DOI] [PubMed] [Google Scholar]
- 16. Fischetti AJ, Gisselman K, Peterson ME. CT and MRI evaluation of skull bones and soft tissues in six cats with presumed acromegaly versus 12 unaffected cats. Vet Radiol Ultrasound 2012; 53: 535–539. [DOI] [PubMed] [Google Scholar]