

Abstract
Introduction
In the U.S., children from low-income families are more likely to be obese. The impact of parent modeling of physical activity (PA) and sedentary behaviors in low-income American ethnic minorities is unclear, and studies examining objective measures of preschooler and parent PA are sparse.
Methods
This cross-sectional study examined 1,003 parent–child pairs who were of low income, largely Latino and African American, and living in one of two geographically disparate metropolitan areas in the U.S. Parents and children wore GT3X/GT3X+ accelerometers for an average of >12 hours/day (7:00am–9:00pm) for 1 week (September 2012 to May 2014). Analysis occurred in 2015–2016.
Results
About 75% of children were Latino and >10% were African American. Mean child age was 3.9 years. The majority of children (60%) were normal weight (BMI ≥50th and <85th percentiles), with more than a third were overweight/obese. Children's total PA was 6.03 hours/day, with 1.5 hours spent in moderate to vigorous PA (MVPA). Covariate-adjusted models showed a monotonic, positive association between parent and child minutes of sedentary behavior (β=0.10, 95% CI=0.06, 0.15) and light PA (β=0.06; 95% CI=0.03, 0.09). Child and parent MVPA were positively associated up to 40 minutes/day of parent MVPA, but an inverse association was observed when parental MVPA was beyond 40 minutes/day (p=0.002).
Conclusions
Increasing parental PA and reducing sedentary behavior correlate with increased PA-related behaviors in children. However, more work is needed to understand the impact of high levels of parental MVPA on the MVPA levels of their children.
Introduction
Physical activity (PA) is a critical factor for the prevention of childhood obesity and the promotion of cardiovascular health.1-4 Moderate to vigorous PA (MVPA) is associated with lower odds of overweight in young children,5-8 but evidence is mixed concerning whether preschool children engage in sufficient amounts of MVPA.9-11 A recent report shows that less than half of preschoolers obtain the recommended ≥3 hours/day of total PA (light, moderate, and vigorous), with at least 1 of these hours in MVPA, recommended by leading international organizations.12,13 Some studies indicate that Latino and African American youth are at lower odds of meeting daily PA recommendations14,15 and higher odds of being overweight/obese.16 For example, nationally representative U.S. data of children aged 6–11 years show that Mexican Americans engage in less MVPA.17 However, other research suggests that children from lower-income households engage in more weekday MVPA18 than children from higher-income households. Identifying key determinants of PA in early childhood could contribute to the development of culturally appropriate, effective PA promotion strategies.
Data from Mexican American children aged 8–10 years found that increases in maternal BMI predicted decreases in children's MVPA and increases in sedentary behavior. Family lifestyles and shared environments are important,19,20 but it is unclear if parental PA contributes to preschool children's PA.21,22 Understanding how parents influence child PA is necessary for developing effective early childhood interventions.
In studies of preschool children in the United Kingdom23 and New Zealand,24 parental PA was significantly associated with child PA. However, because most prior studies had small sample sizes, did not represent underserved populations, and, in many cases, did not utilize clear minimum accelerometer wear time requirements, it is uncertain the extent to which the findings generalize to U.S. populations at high risk for pediatric obesity.25 The purpose of the present research was to examine the associations between accelerometer-measured parental and preschool child PA, among low-income black, white, and Latino families in the U.S. This study hypothesized that parental time in PA of varying intensities and sedentary behavior would be associated with their preschooler's PA and sedentary behavior.
Methods
Study Sample
Baseline data from two ongoing pediatric obesity prevention RCTs with the same data collection protocols for preschool child–parent pairs were examined.26,27 The Growing Right Onto Wellness Trial (NCT01316653) was conducted in Nashville, Tennessee, and the Now Everybody Together for Amazing and Healthful Kids Trial (NCT01606891) was conducted in Minneapolis/St. Paul, Minnesota. Parents were eligible if they had a preschool-aged child (2–5 years) with a BMI ≥50th percentile, no medical conditions preventing PA, received some type of federal assistance (e.g., Special Supplemental Nutrition Program for Women, Infants, and Children), and spoke either English or Spanish. Of eligible parent–preschool child pairs, 75% completed baseline data collection and were enrolled in the study. From the full sample of 1,143 parent–child pairs, 1,003 had valid accelerometer-measured PA data (defined below) for both parent and child; this constituted the analytic sample. This represents an 87.7% participation/response rate. The analytic sample compared to the full sample did not differ in child gender (p=1.00), child race/ethnicity (p=0.54), adult race/ethnicity (p=0.82), and adult education (p=0.79).
Measures
Study designs and data collection procedures have been published.26,27 Informed consent was delivered in the participant's language of choice (English or Spanish), in written and verbal form for parents. Participants received a monetary incentive of $50 at Minnesota and $40 at Vanderbilt for participating in all baseline data collection.26,27 Objective anthropometric measurements were obtained from both the parent and child before accelerometry data were collected.26,27 Data were collected from September 2012 to May 2014. Protocols were approved by Vanderbilt University (No. 120643) and the University of Minnesota (No. 1005S81634) IRBs.
Parent–preschool child participants were asked to wear an ActiGraph GT3X or GT3X+ accelerometer (ActiGraph LLC, Pensacola, FL), on the right hip for 7 days, including when sleeping. The accelerometry data were collected at a frequency of 40 Hz and were downloaded using ActiLife software, versions 6.1.1–6.9.2. The adherent wear time criterion was 4 days (3 weekdays and 1 weekend day) of at least 6 hours of wear time/day, but in most cases, parent–child pairs wore their accelerometry for >12 hours/day. Non-wear was defined by an interval of ≥90 consecutive minutes of zero counts. Any non-zero counts (except allowed short intervals of up to 2 minutes) were considered awake wear time.28 Accelerometry recordings from 7:00am to 8:59pm were used to capture the typical daily wake time cycle for young children.29,30
To explore total volume of PA, average counts/minute were assessed, followed by analysis of time spent in each category of PA and sedentary behavior, using vertical axis counts:
children: 0–25 counts/15 seconds=sedentary, 26–419 counts/15 seconds=light, 420–841 counts/15 seconds=moderate, and ≥842 counts/15 seconds=vigorous31; and
adults: 0–100 counts/minute=sedentary, 101–2,019 counts/minute=light, 2,020–5,998 counts/minute=moderate, and ≥5,999 counts/minute=vigorous.32-34
All analyses were repeated using the percentage wear time spent at different intensities instead of time to account for different durations of wear times; conclusions remained unchanged. Also, no differences were found in the associations between child and parent PA intensities on weekdays as compared to weekends; thus, PA was averaged over all days of the week. Lastly, to explore total volume of PA, average counts/minute were assessed.
Parents reported on age, gender, and race/ethnicity of children and parents; parent education; and country of origin.
Body weight was measured, after voiding and wearing light clothing and no shoes, to the nearest 0.1 kg on a calibrated digital scale. Height without shoes was measured to the nearest 0.1 cm using a standard stadiometer. BMI was calculated (weight [kg]/height [m2]) and weight classifications were assigned using the Centers for Disease Control and Prevention calculator and guidelines,35 respectively.
Statistical Analysis
All analyses were conducted in 2015–2016. To determine if combining data across the two trials was appropriate, the interaction between parent's total PA and study location on the outcome of child's total PA was tested. In addition, interactions between study location and both child and parent accelerometer wear time were examined. None of these interactions were statistically significant (p-values ranged from 0.07 to 0.46). Also explored were three-way interactions among parent's PA, study location, and alternatively child's age, gender, or race/ethnicity with child's total PA as an outcome. None of the interactions were significant (all p-values >0.10), leading to the conclusion that a pooled analysis was appropriate.
Descriptive statistics were calculated. Multiple linear regression analyses were conducted using parents' PA (minutes/day) spent in sedentary behavior, light, or MVPA as the main predictor variable and child's PA (minutes/day) spent at that same PA intensity level as the outcome variable, with parent and child accelerometer wear time as covariates. Additional covariates included child's age, gender, race/ethnicity, and BMI; parents' age and BMI; and study location. Parent's race/ethnicity, education, and employment did not contribute to any of the models (p>0.10 and had no impact on key associations); therefore, they were not included in final modeling. Analyses were conducted using SAS, version 9.3.
Results
The average child's age was 3.9 (SD=0.9) years (Table 1). Seventy-five percent of participating children were Latino, and >10% were African American. Most parents (56%) had at least a high school level education. The majority of children (60%) had normal weight (BMI <85% for gender and age), about 30% were overweight, and 10% obese. More than three quarters (76%) of participating parents were overweight/obese. Noted in Table 1 are the child demographic differences in the two participating sites that reflect the differences in their eligibility criteria.26,27 Appendix Table 1 provides parental demographic information.
Table 1. Characteristics of Index Children in the COPTR Study (N=1,003 Dyads).
| Variables | Minnesota (N=451)a | Vanderbilt (N=552)a | p-value |
|---|---|---|---|
| Socio-demographic characteristics | |||
| Age (years) | 3.3 (0.6) | 4.3 (0.9) | <0.0001 |
| Gender (% Male) | 48.3 | 48.4 | 0.9683 |
| Race/ethnicity (%) | |||
| Non-Hispanic white | 12.0 | 1.1 | <0.0001 |
| Non-Hispanic black | 18.4 | 6.0 | |
| Hispanic | 56.5 | 90.0 | |
| Others | 12.6 | 2.9 | |
| Anthropometric measures | |||
| Weight (kg) | 17.1 (3.1) | 17.8 (2.6) | <0.0001 |
| Height (cm) | 98.2 (6.4) | 103.3 (7.1) | <0.0001 |
| Waist circumference (cm) | 52.9 (5.2) | 53.0 (3.2) | 0.5591 |
| BMI (kg/m2) | 17.6 (1.8) | 16.6 (0.8) | <0.0001 |
| BMI percentile | 81.8 (14.2) | 76.9 (13.1) | <0.0001 |
| BMI categories (%) | |||
| ≥50th - <85th percentile | 51.7 | 65.2 | <0.0001 |
| ≥85th - <95th percentile | 25.0 | 33.9 | |
| ≥95th percentile | 23.1 | 0.9 |
Note: Boldface indicates statistical significance (p<0.05)
Values are either mean (SD) or %
COPTR, Childhood Obesity Prevention and Treatment Research
On average, parents and children wore accelerometers for >12 hours/day (Table 2), with a median wear time of 803.0 minutes/day for children and 801.3 minutes/day for adults. Children's total time spent in PA was 361.9 minutes/day; parents averaged 328.5 minutes/day. Children spent about 50% of their wear time in sedentary behavior (410.5 minutes/day), and their parents spent close to 60% in sedentary behavior (442.4 minutes/day). About 30% of children's wear time was spent in light PA; parents spent 40% in light PA. Almost 13% (98.2 minutes/day) of wear time among children was spent in MVPA, whereas parents spent 2.3% of wear time in MVPA (18.0 minutes/day). Mean MVPA minutes for boys was 113 minutes/day and 99 minutes/day for girls. The distributions of sedentary behavior and light PA minutes were approximately normal in parents and children, but the distribution of MVPA minutes was highly skewed in parents, with most parents having low minutes/day of MVPA and few parents having high minutes/day in MVPA.
Table 2.
| A. Mean (SD) of Baseline Physical Activity Levels in Index Children in the COPTR Study | |||
|---|---|---|---|
|
| |||
| Variables | Minnesota (N=451)a | Vanderbilt (N=552)a | p-value |
| Total physical activity (all types of PA combined in mean minutes/day) | |||
| Physical activity levels (minutes) | |||
| Wear minutes | 770.4 (81.1) | 774.1 (87.4) | 0.4942 |
| Light physical activity (minutes) | 261.1 (46.4) | 265.7 (53.7) | 0.1514 |
| Vigorous physical activity (minutes) | 26.4 (12.9) | 28.7 (14.5) | 0.0085 |
| Moderate to vigorous physical activity (minutes) | 96.9 (31.2) | 99.3 (33.9) | 0.2394 |
| Sedentary (minutes) | 412.4 (68.7) | 409.1 (67.3) | 0.4428 |
| Physical activity levels (percent time) | |||
| Light physical activity (% time) | 33.9 (4.8) | 34.1 (5.0) | 0.3848 |
| Vigorous physical activity (% time) | 3.4 (1.6) | 3.7 (1.8) | 0.0088 |
| Moderate to vigorous physical activity (% time) | 12.6 (3.8) | 12.8 (4.1) | 0.3143 |
| Sedentary (% time) | 53.6 (7.1) | 53.0 (7.6) | 0.2617 |
| Weekdays physical activity | |||
| Physical activity levels (minutes) | |||
| Wear minutes | 771.5 (87.7) | 777.7 (93.5) | 0.2837 |
| Light physical activity (minutes) | 261.4 (49.7) | 266.8 (56.2) | 0.1016 |
| Vigorous physical activity (minutes) | 26.4 (13.7) | 28.3 (14.6) | 0.0309 |
| Moderate to vigorous physical activity (minutes) | 96.7 (33.6) | 98.9 (34.3) | 0.3161 |
| Sedentary (minutes) | 413.4 (72.4) | 412.0 (71.8) | 0.7511 |
| Physical activity levels (percent time) | |||
| Light physical activity (% time) | 33.8 (5.1) | 34.1 (5.3) | 0.3634 |
| Vigorous physical activity (% time) | 3.4 (1.7) | 3.6 (1.8) | 0.0340 |
| Moderate to vigorous physical activity (% time) | 12.5 (4.0) | 12.7 (4.2) | 0.4571 |
| Sedentary (% time) | 53.6 (7.6) | 53.2 (8.0) | 0.3173 |
| Weekend days physical activity | |||
| Physical activity levels (minutes) | |||
| Wear minutes | 766.7 (107.4) | 765.3 (115.7) | 0.8467 |
| Light physical activity (minutes) | 260.2 (58.1) | 263.2 (67.1) | 0.4589 |
| Vigorous physical activity (minutes) | 26.5 (16.1) | 29.7 (19.2) | 0.0052 |
| Moderate to vigorous physical activity (minutes) | 97.1 (37.2) | 100.3 (44.6) | 0.2136 |
| Sedentary (minutes) | 409.4 (89.9) | 401.9 (86.7) | 0.1794 |
| Physical activity levels (percent time) | |||
| Light physical activity (% time) | 33.9 (6.2) | 34.1 (6.4) | 0.6754 |
| Vigorous physical activity (% time) | 3.5 (2.3) | 3.9 (2.4) | 0.0102 |
| Moderate to vigorous physical activity (% time) | 12.7 (4.7) | 13.0 (5.3) | 0.2814 |
| Sedentary (% time) | 53.4 (8.9) | 52.8 (9.8) | 0.3913 |
|
| |||
| Notes: Sedentary activity is defined as <25/15 s epoch. Light activity is defined as 26-419/15s epoch. MVPA is defined as ≥420/15 s epoch. Vigorous activity is defined as ≥842/15 s epoch. Total physical activity includes light, moderate, and vigorous PA combined. Each day of accelerometer data was considered valid if data were obtained for at least 360 minutes between 5:00am and 11:59pm. Participants PA data for this manuscript was considered valid if the parent-child dyad had 3 weekdays and 1 weekend day valid accelerometer data. | |||
| aValues are mean(SD) | |||
| COPTR, Childhood Obesity Prevention and Treatment Research; MVPA, moderate to vigorous physical activity; PA, physical activity | |||
| B. Mean (SD) of Baseline Physical Activity Levels in Index Parents in the COPTR Study | |||
|---|---|---|---|
|
| |||
| Variables | Minnesota (N=451)a | Vanderbilt (N=552)a | p-value |
| Total PA (all types of PA combined in mean/minutes/day) | |||
| Physical activity levels (minutes) | |||
| Wear minutes | 767.1 (82.1) | 774.1 (87.9) | 0.1935 |
| Light physical activity (minutes) | 302.5 (77.6) | 317.2 (81.3) | 0.0037 |
| Vigorous physical activity (minutes) | 0.6 (2.5) | 0.4 (1.5) | 0.1949 |
| Moderate to vigorous physical activity (minutes) | 18.2 (16.0) | 17.8 (18.0) | 0.7396 |
| Sedentary (minutes) | 446.4 (96.3) | 439.1 (93.4) | 0.2257 |
| Physical activity levels (percent time) | |||
| Light physical activity (% time) | 39.5 (9.5) | 40.9 (9.2) | 0.0215 |
| Vigorous physical activity (% time) | 0.07 (0.3) | 0.05 (0.2) | 0.1804 |
| Moderate to vigorous physical activity (% time) | 2.4 (2.1) | 2.3 (2.3) | 0.6097 |
| Sedentary (% time) | 58.1 (10.4) | 56.8 (10.3) | 0.0494 |
| Weekdays PA | |||
| Physical activity levels (minutes) | |||
| Wear minutes | 772.7 (84.0) | 781.8 (93.2) | 0.1038 |
| Light physical activity (minutes) | 307.8 (84.8) | 326.1 (89.9) | 0.0011 |
| Vigorous physical activity (minutes) | 0.6 (2.7) | 0.4 (1.6) | 0.1450 |
| Moderate to vigorous physical activity (minutes) | 18.9 (18.4) | 18.9 (19.7) | 0.9913 |
| Sedentary (minutes) | 445.9 (101.8) | 436.8 (98.4) | 0.1489 |
| Physical activity levels (percent time) | |||
| Light physical activity (% time) | 39.9 (10.2) | 41.5 (10.0) | 0.0106 |
| Vigorous physical activity (% time) | 0.08 (0.3) | 0.05 (0.2) | 0.1279 |
| Moderate to vigorous physical activity (% time) | 2.4 (2.4) | 2.4 (2.5) | 0.8587 |
| Sedentary (% time) | 57.6 (11.2) | 56.0 (11.1) | 0.0232 |
| Weekend days PA | |||
| Physical activity levels (minutes) | |||
| Wear minutes | 750.1 (131.5) | 754.9 (121.1) | 0.5574 |
| Light physical activity (minutes) | 287.7 (94.8) | 294.9 (95.1) | 0.2284 |
| Vigorous physical activity (minutes) | 0.4 (2.5) | 0.3 (2.5) | 0.5938 |
| Moderate to vigorous physical activity (minutes) | 16.1 (17.5) | 14.8 (20.9) | 0.3005 |
| Sedentary (minutes) | 446.4 (118.2) | 445.1 (112.4) | 0.8614 |
| Physical activity levels (percent time) | |||
| Light physical activity (% time) | 38.4 (11.1) | 39.0 (10.8) | 0.3971 |
| Vigorous physical activity (% time) | 0.05 (0.3) | 0.04 (0.3) | 0.5867 |
| Moderate to vigorous physical activity (% time) | 2.1 (2.3) | 2.0 (2.7) | 0.3192 |
| Sedentary (% time) | 59.5 (11.8) | 59.0 (12.0) | 0.5693 |
Notes: Sedentary is defined as <100 cpm; Light activity is defined as 101-2019 cpm; MVPA is defined as ≥2,020 cpm; Vigorous activity is defined as ≥5,999 cpm. Each day of accelerometer data was considered valid if data were obtained for at least 360 minutes between 5:00am and 11:59pm. Participants PA data for this manuscript was considered valid if the parent-child dyad had 3 weekdays and 1 weekend day valid accelerometer data.
Values are mean (SD)
COPTR, Childhood Obesity Prevention and Treatment Research; MVPA, moderate to vigorous physical activity; PA, physical activity
Associations of time spent by parents and their children in sedentary behavior and light PA were described using linear models, but quadratic terms were needed to describe the association for MVPA. Table 3 shows results from both unadjusted and adjusted linear models for sedentary behavior and light PA. In adjusted models, for every minute that a parent spent in sedentary behavior, child's sedentary behavior increased by 0.10 minutes (p<0.001). Similarly, for every minute a parent engaged in light PA, child's light PA increased by 0.06 minutes (p<0.001).
Table 3. Linear Associations of Parents' Daily Average Minutes Spent in Each PA Intensity Category With Child's.
| Child activity category/Models | Parent estimate | 95% CI | p-value |
|---|---|---|---|
| Sedentary behavior | |||
| Unadjusted | 0.22 | 0.18, 0.27 | <0.001 |
| Adjusted | 0.10 | 0.06, 0.15 | <0.001 |
| Light physical activity | |||
| Unadjusted | 0.17 | 0.13, 0.21 | <0.001 |
| Adjusted | 0.06 | 0.03, 0.09 | <0.001 |
Note: Boldface indicates statistical significance (p<0.05). Covariates in adjusted models include parent and child wear times; children's age, gender, race/ethnicity, and BMI; parent's age and BMI; and study location.
The relationship between parent's and child's daily time spent in MVPA is shown in Figure 1. As parent MVPA minutes go from 1 to 10 minutes, child's mean predicted MVPA minutes increases from 95 to 98.5, when the parent MVPA minutes go from 30 to 40 minutes, child's mean predicted MVPA minutes increases slightly, from 103 to 103.5, and when parent MVPA minutes go from 40 to 50 minutes, child's mean predicted MVPA minutes begin to decrease, from 103.5 to 102.5 minutes. The parent data are sparse (5.98%) above the MVPA level of 50 minutes. Nevertheless, the quadratic coefficient was negative and the overall quadratic association was significant (p=0.002, F-test).
Figure 1.
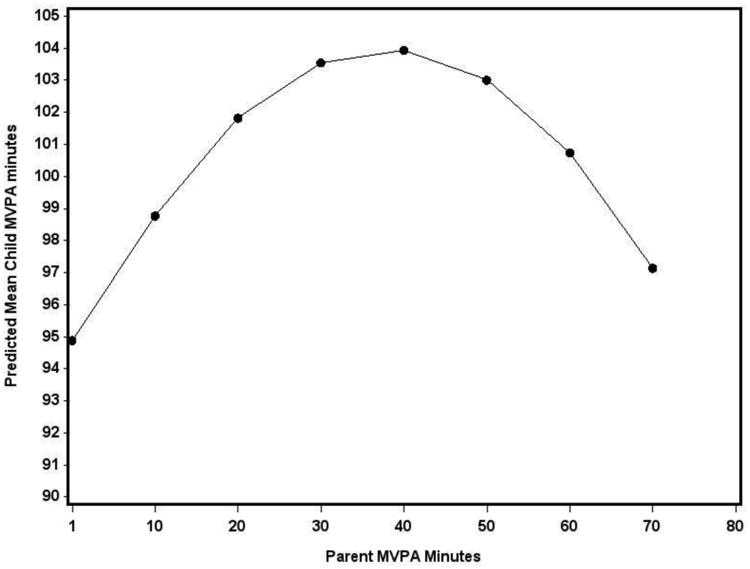
Parent MVPA minutes and predicted child MVPA minutes.
MVPA, moderate to vigorous physical activity
Discussion
Determinants of PA in underserved Latino and African American preschool-aged children have not been well studied, but are important to understand because of their elevated obesity risk.36 Several studies have linked parental PA to young children's PA.21,22 However, the present study is the first to examine the association using accelerometry in a large sample of underserved, mostly Latino parent–preschool child pairs. With a mean wear time of 12 hours/day for both parents and children, the current study better describes time spent in all types of PA and sedentary behavior.
This sample of more than 1,000 racially and ethnically diverse preschool-aged children spent an average of 98 minutes/day in MVPA daily. This amount is higher than previously reported37-40 and could reflect the benefit of collecting data with longer accelerometry wear times. In a study conducted by Ruiz et al.,41 Latino preschoolers took an average of 11 hours to achieve their full MVPA, highlighting the importance of longer wear times to collecting accurate measurements of MVPA in this population. Importantly, no gender differences in achieving MVPA recommendations (60 minutes/day)42 at these young ages were observed. In fact, both boys and girls achieved a mean of greater than 90 minutes of MVPA/day; however, boys had a mean average of 13 minutes more in MVPA/day than girls (p<0.001). Cross-sectional studies using older samples of children12,43-45 found that boys engaged in significantly greater amounts of accelerometry-assessed PA than girls. The present study's finding highlights the opportunity at this developmental period to enhance PA and reduce sedentary behaviors among all children before PA levels begin to decline as they reach adolescence, particularly among girls given this decline begins in early adolescence.46
These findings also indicate that, on average, low-income black, white, and Latino preschool-aged children achieve recommended levels of MVPA (mean of 98 minutes/day in MVPA daily) despite their parents' low mean levels of MVPA (mean of 18 minutes/day). The relationship between parent and preschool MVPA appears to be nuanced. A curvilinear relationship was noted: a positive association at fewer than 40 minutes/day of parent MVPA but an inverse relationship if parents spent longer periods in MVPA. This approximate inflection point exceeds the 30 minutes/day that is the recommended for adult MVPA.47 It may be that parents spending more than 40 minutes/day in MVPA are engaging in activities that cannot be sustained by young children developmentally (such as running long distances), that parents are exercising without their young children present (such as exercising at the gym or exercising when children are at daycare), or in workplace-related PA, which is higher among African American and Latino adults than among white adults.48,49 The present study was only able to examine the objective accelerometry results and not additional information about what type of activity and where the activity occurred for parents. Further examination of this complex association between parental MVPA and preschool child MVPA, using rigorous methods to assess the type and place of PA in this age group, is warranted given the importance of MVPA for obesity prevention/treatment and to improving health outcomes.50,51
Both parental sedentary behavior and light PA were also significantly associated with higher levels of these same types of behaviors in their young children. This suggests that one possible way to help young children be more physically active is to encourage their parents to reduce sedentary behavior. Given that light PA was common and associated between parent and child, perhaps beginning with shifting parental activity from sedentary behavior to light PA could be a point of initial focus. Including parent PA behaviors as part of child obesity prevention efforts could be a critical lever to improve PA patterns in children, as well as parental health outcomes. To date, there are limited interventions that target both parent and preschool child PA levels. Although most recommendations focus on MVPA and demonstrate strong associations with improved health gains, it remains unknown how decreasing sedentary behavior and increasing light PA could result in benefits for children, including obesity prevention. This is an area worthy of further study.
Limited research has examined the relationship between objectively measured parent and preschool child activity levels. However, this study's results can be compared with findings in older pediatric populations. For example, preliminary studies in older children have shown the relationships between parent and child activity vary based on time of day52 and location of activity.53 It has been shown that older children (aged 8–14 years) participated in only 2 minutes of MVPA with their parents on school days and more than 90 minutes of sedentary behavior together on school days.54 This could inform future research by examining the timing and location of PA and sedentary behavior in younger child–parent pairs.
Future research would benefit from the development of comprehensive PA guidelines for preschool-aged children (2–5 years), similar to the 2008 PA Guidelines for Americans aged 6 years and older.55 Ambiguity in PA guidelines for preschool children makes it difficult to accurately monitor PA behaviors and to identify determinants of preschooler PA and health. For example, compliance with PA guidelines for preschool-aged children developed by the National Association for Sport and Physical Education varies considerably depending on guideline interpretations.56 Similar concerns exist with a recent National Academy of Medicine recommendation that preschool children be provided with opportunities for light, moderate, and vigorous PA for at least 15 minutes/hour while in care,57 as measurement of compliance depend on characteristics and patterns of accelerometer wear and assumptions of child wake time. Additionally, it does not consider how or if patterns of PA differ based on location of care, in the home or in a preschool program. The development of PA guidelines for preschoolers with clear interpretations would be valuable to this field.
Limitations
There were some limitations. First, though the analysis was constrained to the typical wake time of young children, 7:00AM–8:59PM, for some of these children, this may have included sleep or naptime and may have overestimated awake sedentary behavior. Additionally, this analysis utilized validated cut points for preschool-aged children and adults; however, because estimates of MVPA are impacted by differences in cut points and epoch length,58-60 the results may not be comparable to other studies that used different cut points and epoch lengths. Also, children were aged between 2 and 5 years, and there is evidence of significant declines in PA within this age range61; but this cross-sectional analyses conducted on children aged 2–5 years showed no differential effects of parent PA on child PA according to child age. Finally, these data derive from a cross-sectional analysis and therefore temporality cannot be assessed.
There are also limits to the study's generalizability due to its focus on children who are of low income, largely Latino and African American, and preschool aged. However, BMI distributions in this study are similar to nationally representative data of U.S. preschool children62 and adults.63 Although the results may only generalize to Latino preschool children, Hispanic preschool children in the U.S. are an under-represented demographic with a greater prevalence of obesity (15.6%) than non-Hispanic white (5.2%), non-Hispanic black (10.4%), and non-Hispanic Asian (5.0%) U.S. preschoolers.62 Further, improved understanding Latino preschooler PA is important for developing effective interventions. Although the provision of monetary incentives for participation could affect generalizability, these incentives were modest and the high response rate suggests that the study sample is reflective of the general population.
Conclusions
Parental sedentary behavior and light PA patterns are monotonically related to preschool-aged children's sedentary behavior and light PA patterns; however, high levels of MVPA in parents were not associated with high levels of MVPA in their preschooler. Considering how to reduce parental sedentary behavior and increase PA behaviors could be a powerful point of intervention. Further, helping families identify MVPA activities that are appealing to parents and developmentally appropriate for children may help to promote recommended levels of PA to all family members. Moreover, given that in this study's sample more than a third of child PA was spent in light intensity and this was associated with parent light PA, the most common type of parental PA, it would be important to study the potential health benefits of this type of PA.
Supplementary Material
Acknowledgments
This research was supported by grants (U01 HL103561, U01 HL103620, U01 HD068890, and U01 HL103629) with additional support for the remaining members of the Childhood Obesity Prevention and Treatment Research Consortium (U01 HL103622) from the National Heart, Lung, and Blood Institute and the Eunice Kennedy Shriver National Institute of Child Health and Development and the Office of Behavioral and Social Sciences Research. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Heart, Lung, and Blood Institute, NIH, or the National Institute of Child Health and Development.
Drs. Barkin and French conceptualized and designed the studies and drafted the initial manuscript. Drs. Lamichhane, Stevens, Bangdiwala, Buchowski, and Evenson analyzed the data. Drs. Barkin, Stevens, Banda, Pratt, and Ms. JaKa critically reviewed, edited, and wrote the manuscript. All authors reviewed and approved the final manuscript as submitted. Study protocols were approved by the Vanderbilt University (No. 120643) and the University of Minnesota (No. 1005S81634) IRBs. Clinical Trial Registration Numbers for the Growing Right Onto Wellness Trial is NCT01316653 and the Now Everybody Together for Amazing and Healthful Kids Trial Trial is NCT01606891.
Footnotes
No financial disclosures were reported by the authors of this paper.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Lambourne K, Donnelly JE. The role of physical activity in pediatric obesity. Pediatr Clin North Am. 2011;58(6):1481–1491. doi: 10.1016/j.pcl.2011.09.004. http://dx.doi.org/10.1016/j.pcl.2011.09.004. [DOI] [PubMed] [Google Scholar]
- 2.Janssen I, Leblanc AG. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int J Behav Nutr Phys Act. 2010;7:40. doi: 10.1186/1479-5868-7-40. http://dx.doi.org/10.1186/1479-5868-7-40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Brambilla P, Pozzobon G, Pietrobelli A. Physical activity as the main therapeutic tool for metabolic syndrome in childhood. Int J Obes (Lond) 2011;35(1):16–28. doi: 10.1038/ijo.2010.255. http://dx.doi.org/10.1038/ijo.2010.255. [DOI] [PubMed] [Google Scholar]
- 4.Flynn MA, McNeil DA, Maloff B, et al. Reducing obesity and related chronic disease risk in children and youth: a synthesis of evidence with ‘best practice’ recommendations. Obes Rev. 2006;7(Suppl 1):7–66. doi: 10.1111/j.1467-789X.2006.00242.x. http://dx.doi.org/10.1111/j.1467-789X.2006.00242.x. [DOI] [PubMed] [Google Scholar]
- 5.Francis SL, Morrissey JL, Letuchy EM, Levy SM, Janz KF. Ten-year objective physical activity tracking: Iowa Bone Development Study. Med Sci Sports Exerc. 2013;45(8):1508–1514. doi: 10.1249/MSS.0b013e31828b2f3a. http://dx.doi.org/10.1249/MSS.0b013e31828b2f3a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Jones RA, Hinkley T, Okely AD, Salmon J. Tracking physical activity and sedentary behavior in childhood: a systematic review. Am J Prev Med. 2013;44(6):651–658. doi: 10.1016/j.amepre.2013.03.001. http://dx.doi.org/10.1016/j.amepre.2013.03.001. [DOI] [PubMed] [Google Scholar]
- 7.Edwards NM, Khoury PR, Kalkwarf HJ, Woo JG, Claytor RP, Daniels SR. Tracking of accelerometer-measured physical activity in early childhood. Pediatr Exerc Sci. 2013;25(3):487–501. doi: 10.1123/pes.25.3.487. http://dx.doi.org/10.1123/pes.25.3.487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Telama R, Yang X, Leskinen E, et al. Tracking of physical activity from early childhood through youth into adulthood. Med Sci Sports Exerc. 2014;46(5):955–962. doi: 10.1249/MSS.0000000000000181. http://dx.doi.org/10.1249/MSS.0000000000000181. [DOI] [PubMed] [Google Scholar]
- 9.Alhassan S, Sirard JR, Robinson TN. The effects of increasing outdoor play time on physical activity in Latino preschool children. Int J Pediatr Obes. 2007;2(3):153–158. doi: 10.1080/17477160701520108. http://dx.doi.org/10.1080/17477160701520108. [DOI] [PubMed] [Google Scholar]
- 10.Dowda M, Brown WH, McIver KL, et al. Policies and characteristics of the preschool environment and physical activity of young children. Pediatrics. 2009;123(2):e261–266. doi: 10.1542/peds.2008-2498. http://dx.doi.org/10.1542/peds.2008-2498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Trost SG, Fees B, Dzewaltowski D. Feasibility and efficacy of a “move and learn” physical activity curriculum in preschool children. J Phys Act Health. 2008;5(1):88–103. doi: 10.1123/jpah.5.1.88. http://dx.doi.org/10.1123/jpah.5.1.88. [DOI] [PubMed] [Google Scholar]
- 12.Pate RR, O'Neill JR, Brown WH, Pfeiffer KA, Dowda M, Addy CL. Prevalence of Compliance with a New Physical Activity Guideline for Preschool-Age Children. Child Obes. 2015;11(4):415–420. doi: 10.1089/chi.2014.0143. http://dx.doi.org/10.1089/chi.2014.0143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Physical Activity Guidelines Advisory Committee Report, 2008. Washington, DC: U.S. DHHS; 2008. Physical Activity Guidelines Advisory Committee. [Google Scholar]
- 14.Fakhouri TH, Hughes JP, Brody DJ, Kit BK, Ogden CL. Physical activity and screen-time viewing among elementary school-aged children in the United States from 2009 to 2010. JAMA Pediatr. 2013;167(3):223–229. doi: 10.1001/2013.jamapediatrics.122. http://dx.doi.org/10.1001/2013.jamapediatrics.122. [DOI] [PubMed] [Google Scholar]
- 15.Anderson SE, Economos CD, Must A. Active play and screen time in U.S. children aged 4 to 11 years in relation to sociodemographic and weight status characteristics: a nationally representative cross-sectional analysis. BMC Public Health. 2008;8:366. doi: 10.1186/1471-2458-8-366. http://dx.doi.org/10.1186/1471-2458-8-366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011-2012. JAMA. 2014;311(8):806–814. doi: 10.1001/jama.2014.732. http://dx.doi.org/10.1001/jama.2014.732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Belcher BR, Berrigan D, Dodd KW, Emken BA, Chou CP, Spruijt-Metz D. Physical activity in U.S. youth: effect of race/ethnicity, age, gender, and weight status. Med Sci Sports Exerc. 2010;42(12):2211–2221. doi: 10.1249/MSS.0b013e3181e1fba9. http://dx.doi.org/10.1249/MSS.0b013e3181e1fba9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Nader PR, Bradley RH, Houts RM, McRitchie SL, O'Brien M. Moderate-to-vigorous physical activity from ages 9 to 15 years. JAMA. 2008;300(3):295–305. doi: 10.1001/jama.300.3.295. http://dx.doi.org/10.1001/jama.300.3.295. [DOI] [PubMed] [Google Scholar]
- 19.Butte NF, Gregorich SE, Tschann JM, et al. Longitudinal effects of parental, child and neighborhood factors on moderate-vigorous physical activity and sedentary time in Latino children. Int J Behav Nutr Phys Act. 2014;11(1):108. doi: 10.1186/s12966-014-0108-x. http://dx.doi.org/10.1186/s12966-014-0108-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Tschann JM, Martinez SM, Penilla C, et al. Parental feeding practices and child weight status in Mexican American families: a longitudinal analysis. Int J Behav Nutr Phys Act. 2015;12:66. doi: 10.1186/s12966-015-0224-2. http://dx.doi.org/10.1186/s12966-015-0224-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.De Craemer M, De Decker E, De Bourdeaudhuij I, et al. Correlates of energy balance-related behaviours in preschool children: a systematic review. Obes Rev. 2012;13(Suppl 1):13–28. doi: 10.1111/j.1467-789X.2011.00941.x. http://dx.doi.org/10.1111/j.1467-789X.2011.00941.x. [DOI] [PubMed] [Google Scholar]
- 22.Hinkley T, Crawford D, Salmon J, Okely AD, Hesketh K. Preschool children and physical activity: a review of correlates. Am J Prev Med. 2008;34(5):435–441. doi: 10.1016/j.amepre.2008.02.001. http://dx.doi.org/10.1016/j.amepre.2008.02.001. [DOI] [PubMed] [Google Scholar]
- 23.O'Dwyer MV, Fairclough SJ, Knowles Z, Stratton G. Effect of a family focused active play intervention on sedentary time and physical activity in preschool children. Int J Behav Nutr Phys Act. 2012;9:117. doi: 10.1186/1479-5868-9-117. http://dx.doi.org/10.1186/1479-5868-9-117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Oliver M, Schofield GM, Schluter PJ. Parent influences on preschoolers' objectively assessed physical activity. J Sci Med Sport. 2010;13(4):403–409. doi: 10.1016/j.jsams.2009.05.008. http://dx.doi.org/10.1016/j.jsams.2009.05.008. [DOI] [PubMed] [Google Scholar]
- 25.Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of obesity and trends in body mass index among U.S. children and adolescents, 1999-2010. JAMA. 2012;307(5):483–490. doi: 10.1001/jama.2012.40. http://dx.doi.org/10.1001/jama.2012.40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Po'e EK, Heerman WJ, Mistry RS, Barkin SL. Growing Right Onto Wellness (GROW): a family-centered, community-based obesity prevention randomized controlled trial for preschool child-parent pairs. Contemp Clin Trials. 2013;36(2):436–449. doi: 10.1016/j.cct.2013.08.013. http://dx.doi.org/10.1016/j.cct.2013.08.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Sherwood NE, French SA, Veblen-Mortenson S, et al. NET-Works: Linking families, communities and primary care to prevent obesity in preschool-age children. Contemp Clin Trials. 2013;36(2):544–554. doi: 10.1016/j.cct.2013.09.015. http://dx.doi.org/10.1016/j.cct.2013.09.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Choi L, Liu Z, Matthews CE, Buchowski MS. Validation of accelerometer wear and nonwear time classification algorithm. Med Sci Sports Exerc. 2011;43(2):357–364. doi: 10.1249/MSS.0b013e3181ed61a3. http://dx.doi.org/10.1249/MSS.0b013e3181ed61a3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Goodlin-Jones BL, Tang K, Liu J, Anders TF. Sleep patterns in preschool-age children with autism, developmental delay, and typical development. J Am Acad Child Adolesc Psychiatry. 2008;47(8):930–938. doi: 10.1097/CHI.ObO13e3181799f7c. http://dx.doi.org/10.1097/CHI.0b013e3181799f7c. [DOI] [PubMed] [Google Scholar]
- 30.Anders TF, Iosif AM, Schwichtenberg AJ, Tang K, Goodlin-Jones BL. Six-month sleep-wake organization and stability in preschool-age children with autism, developmental delay, and typical development. Behav Sleep Med. 2011;9(2):92–106. doi: 10.1080/15402002.2011.557991. http://dx.doi.org/10.1080/15402002.2011.557991. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Pate RR, Almeida MJ, McIver KL, Pfeiffer KA, Dowda M. Validation and calibration of an accelerometer in preschool children. Obesity (Silver Spring) 2006;14(11):2000–2006. doi: 10.1038/oby.2006.234. http://dx.doi.org/10.1038/oby.2006.234. [DOI] [PubMed] [Google Scholar]
- 32.Matthews CE, Chen KY, Freedson PS, et al. Amount of time spent in sedentary behaviors in the United States, 2003-2004. Am J Epidemiol. 2008;167(7):875–881. doi: 10.1093/aje/kwm390. http://dx.doi.org/10.1093/aje/kwm390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Troiano RP, Berrigan D, Dodd KW, Masse LC, Tilert T, McDowell M. Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc. 2008;40(1):181–188. doi: 10.1249/mss.0b013e31815a51b3. http://dx.doi.org/10.1249/mss.0b013e31815a51b3. [DOI] [PubMed] [Google Scholar]
- 34.Matthew CE. Calibration of accelerometer output for adults. Med Sci Sports Exerc. 2005;37(11 Suppl):S512–522. doi: 10.1249/01.mss.0000185659.11982.3d. http://dx.doi.org/10.1249/01.mss.0000185659.11982.3d. [DOI] [PubMed] [Google Scholar]
- 35.CDC. BMI Calculator for Child and Teen: English Version. [Accessed November 11, 2016]; https://nccd.cdc.gov/dnpabmi/calculator.aspx.
- 36.Dawson-Hahn EE, Fesinmeyer MD, Mendoza JA. Correlates of Physical Activity in Latino Preschool Children Attending Head Start. Pediatr Exerc Sci. 2015;27(3):372–379. doi: 10.1123/pes.2014-0144. http://dx.doi.org/10.1123/pes.2014-0144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Senso MM, Trost SG, Crain AL, Seburg EM, Anderson JD, Sherwood NE. Activity Patterns of Preschool-Aged Children at Risk for Obesity. J Phys Act Health. 2015;12(6):861–868. doi: 10.1123/jpah.2013-0503. http://dx.doi.org/10.1123/jpah.2013-0503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Hnatiuk JA, Salmon J, Hinkley T, Okely AD, Trost S. A review of preschool children's physical activity and sedentary time using objective measures. Am J Prev Med. 2014;47(4):487–497. doi: 10.1016/j.amepre.2014.05.042. http://dx.doi.org/10.1016/j.amepre.2014.05.042. [DOI] [PubMed] [Google Scholar]
- 39.Bornstein DB, Beets MW, Byun W, McIver K. Accelerometer-derived physical activity levels of preschoolers: a meta-analysis. J Sci Med Sport. 2011;14(6):504–511. doi: 10.1016/j.jsams.2011.05.007. http://dx.doi.org/10.1016/j.jsams.2011.05.007. [DOI] [PubMed] [Google Scholar]
- 40.Colley RC, Garriguet D, Adamo KB, et al. Physical activity and sedentary behavior during the early years in Canada: a cross-sectional study. Int J Behav Nutr Phys Act. 2013;10:54. doi: 10.1186/1479-5868-10-54. http://dx.doi.org/10.1186/1479-5868-10-54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Ruiz RM, Tracy D, Sommer EC, Barkin SL. A novel approach to characterize physical activity patterns in preschool-aged children. Obesity (Silver Spring) 2013;21(11):2197–2203. doi: 10.1002/oby.20560. http://dx.doi.org/10.1002/oby.20560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.American Heart Association. The AHA's Recommendations for Physical Activity in Children. 2012. [Google Scholar]
- 43.Hesketh KR, McMinn AM, Ekelund U, et al. Objectively measured physical activity in four-year-old British children: a cross-sectional analysis of activity patterns segmented across the day. Int J Behav Nutr Phys Act. 2014;11:1. doi: 10.1186/1479-5868-11-1. http://dx.doi.org/10.1186/1479-5868-11-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Hinkley T, Salmon J, Okely AD, Crawford D, Hesketh K. Preschoolers' physical activity, screen time, and compliance with recommendations. Med Sci Sports Exerc. 2012;44(3):458–465. doi: 10.1249/MSS.0b013e318233763b. http://dx.doi.org/10.1249/MSS.0b013e318233763b. [DOI] [PubMed] [Google Scholar]
- 45.Trost SG, McCoy TA, Vander Veur SS, Mallya G, Duffy ML, Foster GD. Physical activity patterns of inner-city elementary schoolchildren. Med Sci Sports Exerc. 2013;45(3):470–474. doi: 10.1249/MSS.0b013e318275e40b. http://dx.doi.org/10.1249/MSS.0b013e318275e40b. [DOI] [PubMed] [Google Scholar]
- 46.Dumith SC, Gigante DP, Domingues MR, Kohl HW., 3rd Physical activity change during adolescence: a systematic review and a pooled analysis. Int J Epidemiol. 2011;40(3):685–698. doi: 10.1093/ije/dyq272. http://dx.doi.org/10.1093/ije/dyq272. [DOI] [PubMed] [Google Scholar]
- 47.Haskell WL, Lee IM, Pate RR, et al. Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med Sci Sports Exerc. 2007;39(8):1423–1434. doi: 10.1249/mss.0b013e3180616b27. http://dx.doi.org/10.1249/mss.0b013e3180616b27. [DOI] [PubMed] [Google Scholar]
- 48.He XZ, Baker DW. Differences in leisure-time, household, and work-related physical activity by race, ethnicity, and education. J Gen Intern Med. 2005;20(3):259–266. doi: 10.1111/j.1525-1497.2005.40198.x. http://dx.doi.org/10.1111/j.1525-1497.2005.40198.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Marquez DX, Neighbors CJ, Bustamante EE. Leisure time and occupational physical activity among racial or ethnic minorities. Med Sci Sports Exerc. 2010;42(6):1086–1093. doi: 10.1249/MSS.0b013e3181c5ec05. http://dx.doi.org/10.1249/MSS.0b013e3181c5ec05. [DOI] [PubMed] [Google Scholar]
- 50.Goldfield GS, Harvey A, Grattan K, Adamo KB. Physical activity promotion in the preschool years: a critical period to intervene. Int J Environ Res Public Health. 2012;9(4):1326–1342. doi: 10.3390/ijerph9041326. http://dx.doi.org/10.3390/ijerph9041326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Timmons BW, Leblanc AG, Carson V, et al. Systematic review of physical activity and health in the early years (aged 0-4 years) Appl Physiol Nutr Metab. 2012;37(4):773–792. doi: 10.1139/h2012-070. http://dx.doi.org/10.1139/h2012-070. [DOI] [PubMed] [Google Scholar]
- 52.Fuemmeler BF, Anderson CB, Masse LC. Parent-child relationship of directly measured physical activity. Int J Behav Nutr Phys Act. 2011;8:17. doi: 10.1186/1479-5868-8-17. http://dx.doi.org/10.1186/1479-5868-8-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Dunton GF, Liao Y, Almanza E, Jerrett M, Spruijt-Metz D, Pentz MA. Locations of joint physical activity in parent-child pairs based on accelerometer and GPS monitoring. Ann Behav Med. 2013;45(Suppl 1):S162–172. doi: 10.1007/s12160-012-9417-y. http://dx.doi.org/10.1007/s12160-012-9417-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Dunton GF, Liao Y, Almanza E, et al. Joint physical activity and sedentary behavior in parent-child pairs. Med Sci Sports Exerc. 2012;44(8):1473–1480. doi: 10.1249/MSS.0b013e31825148e9. http://dx.doi.org/10.1249/MSS.0b013e31825148e9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.U.S. DHHS. Physical Activity Guidelines for Americans. [Accessed July 20, 2009];2008 www.health.gov/paguidelines.
- 56.Beets MW, Bornstein D, Dowda M, Pate RR. Compliance with national guidelines for physical activity in U.S. preschoolers: measurement and interpretation. Pediatrics. 2011;127(4):658–664. doi: 10.1542/peds.2010-2021. http://dx.doi.org/10.1542/peds.2010-2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.IOM. Early Childhood Obesity Prevention Policies. IOM; 2011. [Google Scholar]
- 58.Ojiambo R, Cuthill R, Budd H, et al. Impact of methodological decisions on accelerometer outcome variables in young children. Int J Obes (Lond) 2011;35(Suppl 1):S98–103. doi: 10.1038/ijo.2011.40. http://dx.doi.org/10.1038/ijo.2011.40. [DOI] [PubMed] [Google Scholar]
- 59.Orme M, Wijndaele K, Sharp SJ, Westgate K, Ekelund U, Brage S. Combined influence of epoch length, cut-point and bout duration on accelerometry-derived physical activity. Int J Behav Nutr Phys Act. 2014;11(1):34. doi: 10.1186/1479-5868-11-34. http://dx.doi.org/10.1186/1479-5868-11-34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Sanders T, Cliff DP, Lonsdale C. Measuring adolescent boys' physical activity: bout length and the influence of accelerometer epoch length. PLoS One. 2014;9(3):e92040. doi: 10.1371/journal.pone.0092040. http://dx.doi.org/10.1371/journal.pone.0092040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Taylor RW, Williams SM, Farmer VL, Taylor BJ. Changes in physical activity over time in young children: a longitudinal study using accelerometers. PLoS One. 2013;8(11):e81567. doi: 10.1371/journal.pone.0081567. http://dx.doi.org/10.1371/journal.pone.0081567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Ogden CL, Carroll MD, Lawman HG, et al. Trends in Obesity Prevalence Among Children and Adolescents in the United States, 1988-1994 Through 2013-2014. JAMA. 2016;315(21):2292–2299. doi: 10.1001/jama.2016.6361. http://dx.doi.org/10.1001/jama.2016.6361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011-2012. JAMA. 2014;311(8):806–814. doi: 10.1001/jama.2014.732. http://dx.doi.org/10.1001/jama.2014.732. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.