

Abstract
Cough is one of the most common symptoms that doctor faces in working with pediatric population, and according to some characteristics of cough, doctors can often conclude localization, and sometimes even the nature of the disease that causes it. Cough is not only the physiological defense reaction, but a symptom of a disease. According to duration it can be acute, chronic and recidivist, recurrent and persistent, strong or discreet, caused by changes in body position and changes in outside temperature. Pathoanatomically it is divided into lobar, lobular, alveolar and interstitial, pathogenetically to bronchogenic and hematogenous, as well as in immuno competent and immunocompromised, and clinically on the local and inpatient (72 hours after hospital admission). Considering the contents, cough can be productive–with secretion from the respiratory tract, and unproductive-dry, without secretion. By auscultation bronchial breathing, rattle and crepitus can be heard. The primary diagnostics is radiological, posterior to anterior (P-A) and lateral footage of the chest. Laboratory findings in typical pneumonia, are characterized by leukocytosis, neutrophilia and shift of blood image to the left. Sedimentation is accelerated and C-reactive protein is elevated. The basic bacteriological diagnosis is sputum Gram’s stain and culture of sputum. In atypical pneumonia, leukocytes are usually in the normal range, and it is necessary to do serological tests (IgM and IgG antibodies). The role of doctors in primary health care is auscultation differentiation of murmurs with confirmation of doubt if there is pathological findings by laboratory tests and treatment, depending on the type of cough. Treatment is essentially pharmacological, with irrefutable importance of non-pharmacological measures.
Keywords: cough, pediatric population, primary health care system
1. INTRODUCTION
Cough is one of the most common symptoms that doctor faces in working with pediatric population, and according to some characteristics of cough, doctors can often conclude the localization, and sometimes even the nature of the disease that causes it (1). Cough is one of the most common symptoms for which patients seek medical attention from primary care physicians and pulmonologists (2). In children, it is the second symptom of respiratory disease after runny nose, with 46-56% representation depending on the age of the child. The literature states that the infant in a day inhales 1260, and schoolchild 6640 liters of air (3). It represents a protective reflex that wants to free the airways from pathological foreign content, from irritating substances, bronchial secretion, inflammatory products and products of circulatory congestion. Cough is, therefore, not only the physiological defense reaction, but a symptom of a disease.
Considering the contents, cough can be productive–with secretion from the respiratory tract, and unproductive-dry, without secretion. Wet cough is a specific feature of exudation phase, except in lower respiratory diseases it can be found as productive cough or sore throat lasting secretion of hypertrophic and chronically inflamed adenoid vegetations.
2. DIFFERENTIATION OF COUGH – THE IMPORTANCE OF AUSCULTATION
According to duration it can be acute, chronic and recidivist, recurrent and persistent, strong or discreet, caused by changes in body position and changes in outside temperature. Pediatric chronic cough (i.e., cough in children aged <15 years) is defined as a daily cough lasting for >4 weeks (5). Cough has three acts–first is a deep inspiration, second act is expiratory when glottis is closed and the third is a quick gasp of air when the glottis is open. Center for coordination is in the medulla oblongata, near the center of breathing.
Pharyngeal cough is usually dry and not particularly strong (dry cough). Outburst of convulsive dry cough in attacks that supplements strong sound inspiration, is a feature of whooping cough. Laryngeal cough is marked by hoarseness of voice. Two-part (bi-tonal) cough is rare but important sign of the stenosis of main bronchus and trachea by swollen lymph glands or by foreign body, and is marked by the simultaneous appearance of one deep hoarse tone and one high-pitched tone.
Restrained cough occurs in a child in difficult dyspnea or with pleural pain, and is identified by a distinct effort of a child to suppress cough reflex (pleuropneumonia). Productive cough suggests to lower respiratory diseases, asthma (bronchial asthma–mucoid mucus, purulent–a sign of bacterial superinfection and severe allergic reactions) or pneumonia, as well as chronic pulmonary disease like cystic fibrosis, bronchiectasis (purulent or very purulent) etc.
A productive cough in acute bronchitis, appears as serous. Smelly expectoration suggests anaerobic infection of the lungs, lung abscess, unlike cystic fibrosis, where the sputum, although purulent, rarely has unpleasant smell. Sometimes, for differentiation, culture of sputum is necessary, other than specific diagnostic tests of immune or alergology type, with X-ray diagnostics of respiratory and sometimes digestive system.
If there is a productive cough, it is usually caused by the presence of secretion in the respiratory system. In pediatric population pneumonia is the most common cause of productive cough. Pneumonia, is an acute inflammation of the lung parenchyma caused by various bacteria, viruses, fungi and parasites. Cause of pneumonia is not isolated in more than 40-50% of cases. The most common cause is Streptococcus pneumoniae, in 9-20% of cases.
Pathoanatomically it is divided into lobar, lobular, alveolar and interstitial, pathogenetically to bronchogenic and hematogenous, as well as in immuno competent and immunocompromised, and clinically on the local and inpatient (72 hours after hospital admission). Typical pneumonia is mostly bacterial and atypical is caused by mycoplasma, chlamydia, legionella and viruses.
In a typical pneumonia onset is sudden, it begins with temperature and fever (temperature suddenly rises above 39 degrees). Pain occurs in the chest on the side of inflammation, then tachypnea and cough. Cough is initially unproductive, and eventually, in three days, it becomes productive with purulent, sometimes bloody sputum. Atypical pneumonia, begins gradually, with general symptoms, poor dry and non-productive cough, accompanied by a temperature not exceeding 39 degrees.
3. ADDITIONAL DIAGNOSTIC TESTS IN DIFFERENTIATION OF COUGH
Sudden and turbulent start is in favor of typical pneumonia. By auscultation bronchial breathing, rattle and crepitus can be heard. The primary diagnostics is radiological, posterior to anterior (P-A) and lateral footage of the chest. Laboratory findings in typical pneumonia, are characterized by leukocytosis, neutrophilia and shift of blood image to the left.
Sedimentation is accelerated and C-reactive protein is elevated. The basic bacteriological diagnosis is sputum Gram’s stain and culture of sputum. In atypical pneumonia, leukocytes are usually in the normal range, and it is necessary to do serological tests (IgM and IgG antibodies).
The main symptom of bronchiectasis (permanent, irreversible enlargement of the bronchi) is cough with higher amounts of muco-purulent sputum (coughing with full mouth, which occurs with abundant secretion in the morning after waking up), hemoptysis, and recurrent pneumonia. The appearance and quantity of sputum depends on bacterial superinfection, and its cause. In bronchial asthma, in case that attack of obstruction is not suppressed relatively quickly, it usually leads to secretion in the bronchi, which often causes, other than productive cough, vomiting of thick, viscous mucus.
Figure 1.
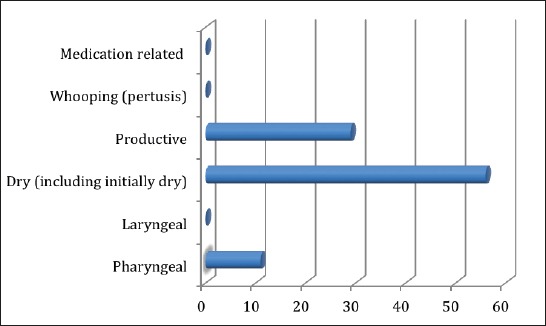
Distribution of cough according to type
In cystic fibrosis, an integral part of the clinical picture is the chronic cough with expectoration, which is usually firstly mucoid and later purulent. Clinically with exacerbations of the lung disease, by new strain of a pathogen or previous cause, intensifies the cough, with a change of color and consistency of the ejected content. In these stages, other than expectorants and secretolytic agents, intensive respiratory physical treatment is used (1).
4. TREATMENT OF COUGH
The role of doctors in primary health care is auscultation differentiation of murmurs with confirmation of doubt, if there is pathological findings by laboratory tests and treatment, depending on the type of cough. Treatment is essentially pharmacological, with irrefutable importance of non-pharmacological measures.
Productive cough can be treated with expectorants, secretolytic agents, having previously applied non-pharmacological measures, in the form of hydration, positioning drainage, physiotherapy and inhalation of water steam or aerosol. In smaller children in addition to secretolytic agents, mobilized secretion can be evacuated with implementation of mechanism like coughing, gasping (“huffing”) and suction.
Except bromhexine (bromhexine derivative–ambroxol hydrochloride) and acetylcysteine, for secretolytic agents as pharmacotherapeutic agents today no firm scientific evidence for clinical activity is available (3). In all cases of expectoration, other than expectorants, secretolytic agents, especially in children, it makes sense to make expectoration easier with extracts of plantain, primrose, thyme, in the form of large spectrum of syrups or making tea with the aforementioned extracts.
Footnotes
• Conflict of interest: none declared.
REFERENCES
- 1.Mardešić D. i sur. Pedijatrija. Zagreb: Školska knjiga Zagreb; 2003. pp. 768–773. [Google Scholar]
- 2.De Blasio F, Virchow JC, Polverino M, Zanasi A, Behrakis PK, Kilinç G, et al. Cough management: a practical approach. Cough. 2011;7:7–10. doi: 10.1186/1745-9974-7-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Von der Hardt H. Luftverschmutzung und bronchoplumonale Erkrankungen Im Kindersalter. Monatschr Kinderheilkd. 198(133):2. [PubMed] [Google Scholar]
- 4.Čemerlić-Zečević E, Zubčević S. Pedijatrija, Udžbenik za studente Medicinskog fakulteta. Sarajevo: Štamparija Fojnica; 2006. pp. 321–47. [Google Scholar]
- 5.Chang AB, Glomb WB. Guidelines for evaluating chronic cough in pediatrics: ACCP evidence-based clinical practice guidelines. Chest. 2006 Jan;129(1 Suppl):260S–283S. doi: 10.1378/chest.129.1_suppl.260S. [DOI] [PubMed] [Google Scholar]