

Abstract
Introduction
The majority of cases of lung cancer are still diagnosed at a late stage. At this stage, palliative therapeutic options including nonspecific cytotoxic drugs, targeted therapy, or immunotherapy can be utilized. In 2016, immunotherapy was approved in Europe for squamous cell carcinoma and adenocarcinoma. Moreover, afatinib was also approved as second-line therapy for squamous cell carcinoma.
Case report
This article presents a case of a 76-year-old male with squamous cell carcinoma who received nab-paclitaxel as first-line therapy, and his treatment was switched to the tyrosine kinase inhibitor afatinib (40 mg) after disease progression with left lung atelectasis. After receiving afatinib for only 28 days, the atelectasis resolved. No adverse effects were observed from the afatinib therapy.
Discussion
In this case, afatinib 40 mg proved to be an effective alternative treatment for an elderly patient. Treatment choice should be based on the performance status of the patient, cost-effectiveness, and drug treatment guidelines.
Keywords: lung cancer, EGFR, afatinib
Introduction
Lung cancer is most commonly diagnosed at a late stage because of the lack of early symptoms and no reliable screening markers. However, early detection is very important; hence, several authors have proposed specific target groups and techniques for lung cancer screening.1,2 Treatment for stage IV disease could be divided in four groups: 1) nonspecific cytotoxic agents, 2) tyrosine kinase inhibitors (TKIs), 3) immunotherapy, and 4) local therapy (eg, endoscopic debulking techniques, microwave, or radiofrequency).3–6 Nonspecific cytotoxic agents have a limitation because of the drug-related complications in the elderly and those with a compromised performance status. Therapies that target epidermal growth factor receptor (EGFR) and anaplastic lymphoma kinase are currently available. In order to identify these mutations, re-biopsy if indicated or liquid biopsy may be needed to identify a possible mutation.7–13 Immunotherapy was approved in Europe for both squamous cell carcinoma and adenocarcinoma.14 Immunotherapy utilized as maintenance therapy is actively being investigated.15 The novel immunotherapy pembrolizumab has been approved as first-line treatment for non-small cell lung cancer (NSCLC) based on the expression of anti-PD-1/PD-L1 antibodies.16 The major issue with immunotherapy is the cost; however, since immunotherapy is becoming a “targeted” therapy, it will certainly become a first choice of treatment for lung cancer. TKIs still remain the targeted therapy of choice where possible with novel agents being already on the market such as AZD9291 osimertinib. Further experimentation with TKIs has identified new treatment options such Giotrif® (afatinib), which is approved for second-line treatment without the patient expressing an EGFR mutation.17,18 Afatinib is a second-generation protein kinase inhibitor that irreversibly inhibits EGFR.19
Case report
A 76-year-old male was diagnosed with squamous cell carcinoma from a central mass in the left stem bronchus. The patient had 150 pack-years of tobacco abuse and no distant metastasis, but he could not undergo surgery because of the location of the central mass. He was offered and agreed to receive nab-paclitaxel as first-line treatment because of his age and performance status. After four cycles of therapy, atelectasis was observed consistent with disease progression on chest imaging and afatinib 40 mg was suggested to the patient, which he agreed upon and initiated. The patient performance status was Eastern Cooperative Oncology Group (ECOG) 0 upon initiation of afatinib 40 mg. The EGFR status was negative. No adverse effects were observed from the administration of nab-paclitaxel, nor afatinib 40 mg till date. After only 28 days of the afatinib 40 mg administration, a complete resolution of the atelectasis of the left lung was observed consistent with drug response (Figures 1–4). A written informed consent statement was obtained from the patient to have the case details and any accompanying images published by the authors.
Figure 1.
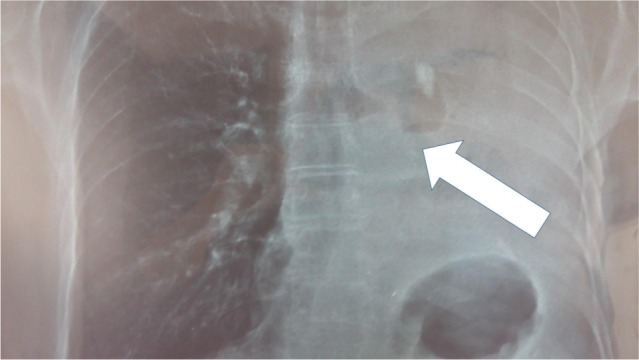
Left lung atelectasis (during abraxane, last therapy session); white arrow indicates the central mass to the left main bronchus.
Figure 2.
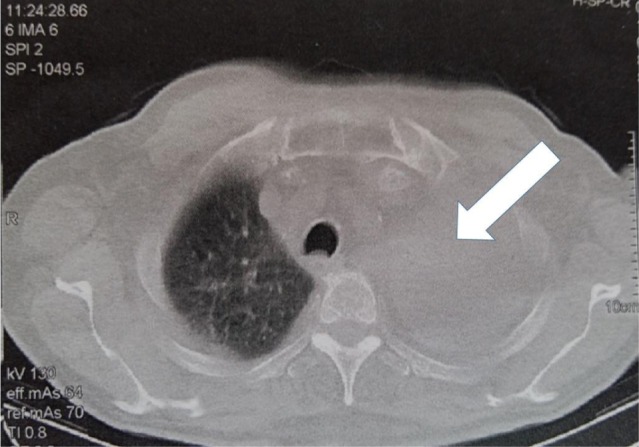
Computed tomography scan of the thorax (during abraxane); the left lung is totally collapsed (white arrow).
Figure 3.
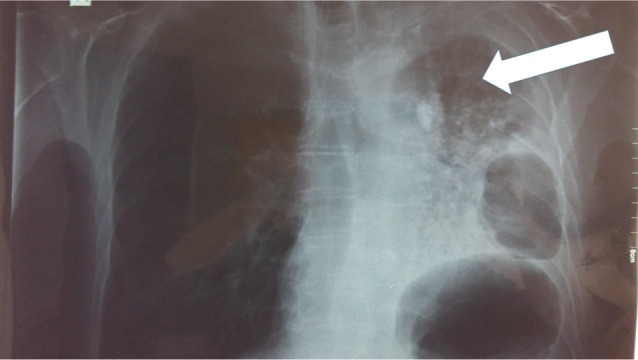
After 28 days under afatinib 40 mg (the mass has started to shrink and the left lung to inflate, white arrow).
Figure 4.
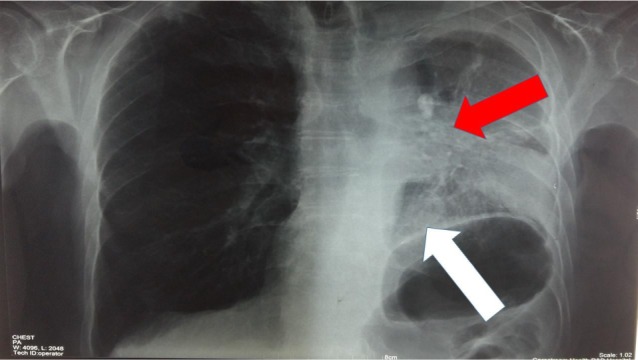
After 65 days from the afatinib 40 mg administration (white arrow indicates the part of the left lower lobe that has been inflated and red arrow indicates the central mass that used to totally block the left lung).
Discussion
There are several nonspecific cytotoxic agents that a treating physician can offer for squamous cell lung cancer.4 It is known that these drugs are given based on the performance status and age of the patient. Adverse effects are severe in several patients, and hospitalization is also necessary if these occur.20,21 In a recent study, it was proposed that a single agent or avoidance of platinum analogs for the elderly aged ≥70 years could be a solution.21 On the basis of the center experience and the patient characteristics, a single agent (nab-paclitaxel 150 mg) was chosen to be administered weekly on days 1, 8, and 15 with 2 weeks off based on the current institutional treatment algorithms. The patient did not have any adverse effects; however, there was radiographic evidence of disease progression for which afatinib 40 mg was chosen to be administered. In this case, the patient had a remarkable response with only 28 days of administration. Of note, in a recent study, the overexpression of secreted protein acidic and rich in cysteine (SPARC), which binds to albumin, was used as marker of treatment efficiency with afatinib.22 The patient did not have any adverse effects from the afatinib 40 mg administration. Immunotherapy is another potential choice that treating physicians could consider in elderly patients, since adverse effects are less frequent. Further studies are needed to determine efficacy and safety profiles in this patient population.
Acknowledgments
The authors would like to thank Dr Mina Gaga for the useful insights in the presentation of the case.
Footnotes
Disclosure
Paul Zarogoulidis is a member of the advisory board of Boehringer Ingelheim® Greece for Oncology agents. The authors report no other conflicts of interest in this work.
References
- 1.Kanodra NM, Pope C, Halbert CH, Silvestri GA, Rice LJ, Tanner NT. Primary care provider and patient perspectives on lung cancer screening. A qualitative study. Ann Am Thorac Soc. 2016;13(11):1977–1982. doi: 10.1513/AnnalsATS.201604-286OC. [DOI] [PubMed] [Google Scholar]
- 2.Henschke CI, Yip R, Smith JP, et al. CT screening for lung cancer: part-solid nodules in baseline and annual repeat rounds. AJR Am J Roentgenol. 2016;207(6):1176–1184. doi: 10.2214/AJR.16.16043. [DOI] [PubMed] [Google Scholar]
- 3.Domvri K, Zarogoulidis P, Darwiche K, et al. Molecular targeted drugs and biomarkers in NSCLC, the evolving role of individualized therapy. J Cancer. 2013;4(9):736–754. doi: 10.7150/jca.7734. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Zarogoulidis K, Zarogoulidis P, Darwiche K, et al. Treatment of non-small cell lung cancer (NSCLC) J Thorac Dis. 2013;5(Suppl 4):S389–S396. doi: 10.3978/j.issn.2072-1439.2013.07.10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Stratakos G, Gerovasili V, Dimitropoulos C, et al. Survival and quality of life benefit after endoscopic management of malignant central airway obstruction. J Cancer. 2016;7(7):794–802. doi: 10.7150/jca.15097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hohenforst-Schmidt W, Zarogoulidis P, Pitsiou G, et al. Drug eluting stents for malignant airway obstruction: a critical review of the literature. J Cancer. 2016;7(4):377–390. doi: 10.7150/jca.13611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Zarogoulidis P, Gaga M, Huang H, Darwiche K, Rapti A, Hohenforst-Schmidt W. Tissue is the issue and tissue competition. Re-biopsy for mutation T790: where and why? Clin Transl Med. 2017;6(1):6. doi: 10.1186/s40169-017-0135-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Papadopoulou E, Tsoulos N, Tsirigoti A, et al. Determination of EGFR and KRAS mutational status in Greek non-small-cell lung cancer patients. Oncol Lett. 2015;10(4):217–2184. doi: 10.3892/ol.2015.3600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Zaric B, Stojsic V, Kovacevic T, et al. Clinical characteristics, tumor, node, metastasis status, and mutation rate in domain of epidermal growth factor receptor gene in Serbian patients with lung adenocar-cinoma. J Thorac Oncol. 2014;9(9):1406–1410. doi: 10.1097/JTO.0000000000000242. [DOI] [PubMed] [Google Scholar]
- 10.Hohenforst-Schmidt W, Zarogoulidis P, Steinheimer M, et al. Tyrosine kinase inhibitors for the elderly. J Cancer. 2016;7(6):687–693. doi: 10.7150/jca.14819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Yarmus L, Akulian J, Gilbert C, et al. Optimizing endobronchial ultrasound for molecular analysis. How many passes are needed? Ann Am Thorac Soc. 2013;10(6):636–643. doi: 10.1513/AnnalsATS.201305-130OC. [DOI] [PubMed] [Google Scholar]
- 12.Soejima K, Yasuda H, Hirano T. Osimertinib for EGFR T790M mutation-positive non-small cell lung cancer. Expert Rev Clin Pharmacol. 2016;10(1):31–38. doi: 10.1080/17512433.2017.1265446. [DOI] [PubMed] [Google Scholar]
- 13.Speranza G, Cohen V, Agulnik JS, et al. Molecular changes in epidermal growth factor receptor (EGFR) in non-small cell lung cancer (NSCLC) biopsies at time of progression compared to initial biopsy. J Clin Oncol. 2009;27(15 Suppl):e22066. [Google Scholar]
- 14.Metro G, Ricciuti B, Brambilla M, et al. The safety of nivolumab for the treatment of advanced non-small cell lung cancer. Expert Opin Drug Saf. 2016;16(1):101–109. doi: 10.1080/14740338.2017.1267725. [DOI] [PubMed] [Google Scholar]
- 15.Blumenschein G, Jr, Chandler J, Garon EB, et al. PS01.59: CheckMate 370: a master protocol of phase 1/2 studies of nivolumab as maintenance or first-line +/− standard-of-care therapies in advanced NSCLC: Topic: Medical Oncology. J Thorac Oncol. 2016;11(11S):S307. [Google Scholar]
- 16.Valecha GK, Vennepureddy A, Ibrahim U, Safa F, Samra B, Atallah JP. Anti-PD-1/PD-L1 antibodies in non-small cell lung cancer: the era of immunotherapy. Expert Rev Anticancer Ther. 2017;17(1):47–59. doi: 10.1080/14737140.2017.1259574. [DOI] [PubMed] [Google Scholar]
- 17.Cobo M, Gutierrez V, Rodelo L, Lopez O, Ruiz M, Godoy A. Afatinib en pacientes con carcinoma de células escamosas de pulmón: contexto actual y la opción de tratamiento oral [Afatinib in patients with squamous cell carcinoma of the lung: current context and the option of oral treatment] Med Clin [Barc] 2016;146(Suppl 1):25–29. doi: 10.1016/S0025-7753(16)30260-3. Spanish. [DOI] [PubMed] [Google Scholar]
- 18.Keating GM. Afatinib: a review in advanced non-small cell lung cancer. Target Oncol. 2016;11(6):825–835. doi: 10.1007/s11523-016-0465-2. [DOI] [PubMed] [Google Scholar]
- 19.Diz Tain P, Gonzalez AL, Garcia-Palomo A. Mecanismo de acción y desarrollo preclínico de afatinib [Mechanism of action and preclinical development of afatinib] Med Clin [Barc] 2016;146(Suppl 1):7–11. doi: 10.1016/S0025-7753(16)30257-3. Spanish. [DOI] [PubMed] [Google Scholar]
- 20.Yang J, He J, Yu M, Li T, Luo L, Liu P. The efficacy and safety of platinum plus gemcitabine (PG) chemotherapy with or without molecular targeted agent (MTA) in first-line treatment of non-small cell lung cancer (NSCLC) Medicine. 2016;95(50):e5599. doi: 10.1097/MD.0000000000005599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Santos FN, Castria TB, Cruz MR, Riera R. Chemotherapy for advanced non-small cell lung cancer in the elderly population. Sao Paulo Med J. 2016;134(5):465–466. doi: 10.1590/1516-3180.20161345T1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Komiya K, Nakamura T, Nakashima C, et al. SPARC is a possible predictive marker for albumin-bound paclitaxel in non-small-cell lung cancer. OncoTargets Ther. 2016;9:6663–6668. doi: 10.2147/OTT.S114492. [DOI] [PMC free article] [PubMed] [Google Scholar]