

Abstract
Background
Despite the well-documented economic and psychosocial burden of Irritable Bowel Syndrome (IBS), few studies have focused on the impact of IBS on daily activities. The current study aims to quantify impairment in daily activities among IBS patients and to evaluate the relationship between impairment, IBS, quality of life, and psychiatric symptoms.
Methods
179 participants meeting ROME-III criteria for IBS completed an online research survey evaluating the following variables: 1) the impact of IBS on daily activities, 2) comorbid psychiatric diagnoses, 3) symptom severity, 4) quality of life, and 5) and symptom-specific cognitive affective factors related to IBS.
Key Results
This sample reported a high degree of impairment due to IBS, with 76% of the sample reporting some degree of IBS-related impairment in at least 5 different domains of daily life. Rates of impairment were significantly higher for participants who met criteria for anxiety, depression, and/or panic disorder.
Conclusions and inferences
This study contributes to existing literature by demonstrating a high level of daily impairment among patients with Irritable Bowel Syndrome, particularly those who meet criteria for anxiety, depression, and panic disorder. These findings support the importance of integrated psychosocial and medical care for IBS patients, and highlight the utility of evaluation and intervention for behavioral avoidance/impairment especially among those who exhibit signs or symptoms of psychiatric diagnoses.
Keywords: Irritable Bowel Syndrome, Quality of Life, Chronic Illness, Illness Burden
Abbreviated abstract
This study characterizes daily impairment in patients with IBS. The majority of respondents reported impairment in at least 5 domains of daily living. Rates of impairment were highest among participants who met questionnaire-based criteria for psychiatric diagnoses.
Irritable bowel syndrome is a common disorder of the gastrointestinal tract with a multifactorial etiology and no reliable biomarker. Similar to other functional disorders, medical treatments for IBS are suboptimal and illness burden is high1. Individuals with IBS often report high rates of psychopathology and low quality of life2,3. They also tend to miss more days of work, report decreased productivity at work, and use many healthcare resources4–6.
Despite the well-documented impact of IBS on quality of life, healthcare utilization, and work productivity, relatively few studies have evaluated the impact of IBS on overall daily functioning. With approximately 40–60% of individuals with IBS meeting criteria for a psychiatric disorder2 and with IBS accounting for 1.5–2.7 million physician visits a year4 (2–3 times more visits than the general population), it would make sense that individuals with IBS might experience increased difficulty engaging in daily activities and responsibilities.
Existing data on the impact of IBS on daily activities come primarily from large survey studies that have included 1–2 questions about overall daily functioning and quality of life. The results of these studies suggest that individuals with IBS report higher levels of difficulty in a broad range of daily activities when compared to healthy controls7; that IBS negatively affects both mental and physical functioning (as measured by quality of life questionnaires)8; and that the reported impact of IBS on daily living is almost as high as that of the flu (6.2/10 for IBS compared to 7/10 for the flu)9.
Although there are many published studies that thoroughly evaluate the impact of IBS on quality of life (a measure of perceived emotional, social, and physical problems), only one study to our knowledge has sought to systematically quantify and characterize impairment of daily activities in a sample of individuals with IBS10. In Corney and Stanton’s study, 42 patients completed questionnaires measuring IBS symptom severity and avoidance of daily activities. Avoidance was measured using an 8-point rating scale in the domains of exercise, sexual intercourse, work, household chores, socializing, traveling, leisure, and eating. The findings suggested high levels of avoidance in a range of daily activities, particularly when abdominal pain was present. This was especially evident in the domains of work, household chores, socializing, sexual intercourse, and leisure activities, with over 40% of the sample reporting avoidance of these activities due to abdominal pain.
The current study seeks to replicate and expand upon Corney and Stanton’s original findings by increasing the sample size and including measures to evaluate the relationships between functional impairment and other psychosocial and illness-related factors. Based on the findings mentioned above and clinical knowledge of the day-to-day impact of IBS, we hypothesized that the sample would report a high level of impairment due to IBS and that the level of impairment would be significantly associated with psychosocial and illness-related variables.
Materials and methods
Sample
This study was approved by an institutional review board in accordance with the provisions of the World Medical Association Declaration of Helsinki. Data was collected from 227 male and female participants with IBS ages 18–70. These participants were recruited as part of an online survey that was advertised on various IBS websites and weblogs. Data was collected using Adobe FormsCentral, an online data collection tool (www.acrobat.com/FormsCentral).
Participation in this survey was anonymous and respondents did not provide any identifying information. Diagnosis of IBS was confirmed through inclusion of the ROME-III questionnaire. Respondents were excluded from the final sample if they: 1. Did not meet criteria for IBS; 2. Were currently pregnant or had given birth in the last 12 weeks; or 3. Were diagnosed with crohn’s disease or ulcerative colitis
Functional impairment assessment
For the purposes of this study, functional impairment (our primary outcome variable) was operationalized as the behavioral outcome of being unable or unwilling to participate in daily activities due to IBS symptoms or fear of IBS symptoms.
Because there is no available validated measure of impairment in daily functioning for patients with chronic conditions such as IBS, functional impairment was evaluated using a questionnaire adapted from Corney and Stanton’s original study10. The questionnaire evaluated 10 domains of functional impairment: Job/school performance; Social activity; Physical activity; Physical Appearance; Household activities; Sexual activity; Leisure activity; Travel; Eating alone; and Eating in groups. Each domain had 2 questions: 1) from 0–10 rate your level of avoidance or inability to complete tasks in this domain in the past 2 weeks; and 2) was this related to IBS symptoms (yes/no)? See appendix 1
IBS symptom assessment
Participants completed the ROME-III diagnostic questionnaire to confirm IBS diagnosis 11,12. The ROME-III criteria are symptom-based and consist of 10 items. Diagnostic sensitivity is 87.8% when compared to clinician diagnosis, and test-retest agreement is 81.7% 13. Additionally, participants completed the IBS Symptom Severity Scale (IBS-SSS) to measure severity and frequency of IBS symptoms14. The IBS-SSS is 5-item scale and each item is measured on a 100 point scale with the total score for ranging from 0–500.
Psychological symptom assessment
Standardized questionnaires from the Patient Health Questionnaire (PHQ) modules (described below) were used to evaluate likely diagnoses of depression, anxiety, and panic. Depression was measured using the PHQ-8. This measure consists of 8 items on a 4 point scale over the past 2 weeks. The total score for the PHQ-8 ranges from 0–24 and cut points are 5 (mild), 10 (moderate), 15 (moderately severe), and 20 (severe). 15,16. A conservative cut-off score of 10 was used for this study.
Anxiety was measured using the Generalized Anxiety Disorder-7 (GAD-7), which is part of the PHQ modules. This measure consists of seven items on a 4 point scale rating symptoms of anxiety over the past 2 weeks. Scores range from 0–21 with cutpoints of 5 (mild), 10 (moderate), and 15 (severe). An overall cut point of 10 or greater yields sensitivity of .89 and specificity of .82 in identifying GAD 17. This measure has excellent internal consistency (Cronbach’s α=0.92) and good test-retest reliability (intraclass correlation=0.83)17.
Panic symptoms were measured using the PHQ-panic module. This measure includes 15 items rated “yes” or “no” over the past 4 weeks. If a patient endorses all of the first 4 items and endorses ≥4 somatic symptoms during an anxiety attack, a diagnosis of panic disorder is probable 18,19. Sensitivity and specificity of this algorithm have been found to be .75 and .96, respectively 20.
Symptom-specific anxiety assessment
Symptom-specific anxiety was measured using the Visceral Sensitivity Index (VSI)21. The VSI consists of 15 items with a 6-point Likert scale from 0 (strongly disagree) to 5 (strongly agree). The maximum score is 75 (severe GSA) and a score of 0 indicates no gastrointestinal specific anxiety (GSA). The VSI demonstrates good reliability (Cronbach’s α=0.93) and good content, convergent, divergent, and predictive validity in IBS patients.
Quality of life assessment
The SF-12 is a quality of life measure used to assess mental and physical functioning over the past 4 weeks22. This scale includes 12 items derived from the Short Form 36 health status questionnaire (SF-36)23,24. The SF-12 consists of 2 subscales: the Mental Component Summary (MCS) and the Physical Component Summary (PCS). Each subscale has a possible score of 0–100, with increasing scores indicating better quality of life. The SF-12 demonstrates good reliability and validity (Cronbach’s α for MCS = 0.76; PCS = 0.89).
Statistical methods
Data was stored and analyzed using SPSS v.21. Demographic and psychiatric data were summarized using descriptive and frequency analyses. Functional impairment was calculated in two ways: First, reported impairment due to IBS was calculated as a binary variable (yes/no) and then as a continuous variable (average impairment on a 0–10 scale) for each domain. Functional impairment was reported as percentage of the sample who avoided each domain of daily living and the average rate of impairment for each category. Finally, two composite functional impairment scores were calculated for each participant: 1) the “total rate of impairment”, calculated by averaging all reported impairment due to IBS across all categories (range = 0–10) and 2) the “total number of domains avoided due to IBS” calculated by adding all of the domains with a rating of 1 or higher and identified as avoided or impaired as a result of IBS (range = 0–10).
In our secondary analyses, T-tests were used to evaluate differences between participants who met criteria for a psychiatric diagnosis (based on the PHQ modules) and those who did not meet criteria.
Results
Demographics and clinical characteristics
A total of 227 respondents completed the online questionnaire. Of these, 179 met eligibility criteria for this study. Mean age in the sample of eligible respondents was 35.54 years old (SD=13.34 years, range 18–67). The majority of the sample was female (78%), Caucasian (89.4%), and not-Hispanic (94.4%, Table 1). IBS-M was the most common subtype in this sample (58.7%), followed by IBS-D (31.8%), and IBS-C (9.5%).
Table 1.
Sample (n=179) demographics
| Gender | |
| Female | 78% |
| Male | 22% |
| Race | |
| White/Caucasian | 89.40% |
| Black/African American | 3.40% |
| Asian | 2.80% |
| American Indian/Alaskan | |
| Native | 0.60% |
| Other | 1.10% |
| Declined | 2.80% |
| Ethnicity | |
| Hispanic | 4.50% |
| Not Hispanic | 94.40% |
| Declined | 1.10% |
| Marital Status | |
| Married/Life partner | 41.90% |
| Divorced/separated | 11.70% |
| Never married | 46.40% |
| Education | |
| No college | 10.60% |
| Some college | 34.10% |
| Completed college | 55.30% |
| Psych dx | |
| Any psych diagnosis | 58.00% |
| GAD | 38.00% |
| Depression | 49% |
| Panic | 22% |
Psychiatric diagnoses were determined using questionnaire-based criteria (PHQ modules).
Average reported symptom severity on the IBS-SSS was 279.5 (SD=101.7, Range 0–500). Average reported GI-specific anxiety measured by the VSI was 49.69 (SD=18.03, range 2–75). Average reported QoL measured by the SF12 PCS was 41.34 (SD=9.75, range 15–60) and the SF12 MCS was 31.08 (SD=10, range 8–58)
Fifty eight percent of the sample met criteria for at least one of the 3 psychiatric diagnoses evaluated with the Patient Health Questionnaire modules (table 1). Likely presence of psychiatric diagnosis, as measured by the study questionnaires (using conservative cut points of 10 for the PHQ-8 and the GAD-7) were all significantly correlated with the overall rate of functional impairment: depression (r=.430, p<.001); anxiety (r=.300, p<.001), panic (r=.303, p<.001), and any combination of the three diagnoses (r=.394, p<.001). As such, functional impairment was first evaluated in the entire sample and was later divided into two groups (presence/absence of psychiatric diagnosis).
Impairment of daily activities
Characterizing impairment in the entire sample
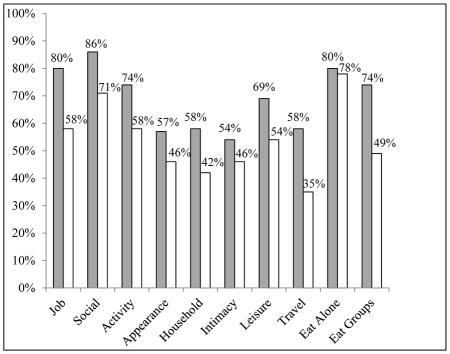
Functional impairment in the entire sample (n=179) is shown in figure 1. The average rate of impairment due to IBS (as measured on a 0–10 scale) in this sample was 5.33 (range 0–10, SD=2.15), and the average number of domains impaired due to IBS was 6.39 domains (range 0–10, SD=2.68). The majority (76.5%) of respondents reported IBS-related impairment in 5 or more domains of daily living.
Figure 1.

Percent reporting impairment due to IBS and average rates of impairment due to IBS in entire sample (with standard deviations)
Characterizing impairment by psychiatric diagnosis
Functional impairment by psychiatric diagnosis (as determined by PHQ module questionnaires) is shown in Figures 2–4. Overall rates of impairment were higher in patients who met criteria (using conservative cutpoints described above) for GAD (t(164)= −4.03, p=.000), depression (t(164)= −6.10, p=.000), panic disorder (t(164)= −4.07, p=.000), and any combination of the three diagnoses (t(164)= −5.49, p=.000) (Figure 2) when compared with those who did not meet criteria for any psychiatric diagnosis.
Figure 2.

Overall mean impairment by psychiatric diagnosis.
** indicates p<0.001. Psychiatric diagnoses were determined using questionnaire-based criteria (PHQ modules)
Figure 4.

Average rates of impairment due to IBS with vs. without psychiatric diagnoses.
Grey bars = pts who met criteria for psychiatric comorbidity.
** indicates p<0.001
Psychiatric diagnoses were determined using questionnaire-based criteria (PHQ modules)
Additionally, a higher percentage of participants who met criteria for a psychiatric diagnosis reported impairment in each domain of daily living when compared to participants who did not meet such criteria (Figure 3). On average, participants who met criteria for a psychiatric diagnosis reported impairment in 6.90 domains of daily living (SD=2.53), which was higher than those participants who did not meet criteria (mean=5.38, SD=2.62); t(164)= −3.76, p=.000. Participants who met criteria for a psychiatric diagnosis also reported higher rates of impairment in all domains of daily living except for dissatisfaction with appearance and eating alone (Figure 4).
Figure 3.

Percent reporting impairment due to IBS with vs. without psychiatric diagnoses.
Grey bars = pts who met criteria for psychiatric comorbidity.
Psychiatric diagnoses were determined using questionnaire-based criteria (PHQ modules)
Relationships among variables
The overall rate of functional impairment was significantly correlated with all measured psychosocial and symptom-related variables except for the Mental Component Subscale of the SF-12 (see Table 2). When the sample was divided into those who did and did not meet questionnaire-based criteria for a psychiatric comorbidity, functional impairment remained significantly correlated with the VSI, IBS-SSS, and SF-12 PCS, regardless of presence/absence of psychiatric diagnoses. However, there were statistically significant differences between respondents who did and did not meet criteria for psychiatric diagnoses. Respondents with psychiatric comorbidities scored significantly higher on the IBS-SSS (t(164)= 3.97, p=.000) and VSI (t(164)= 4.26, p=.000) and significantly lower on the SF-12 PCS (t(164)= 3.44, p=.001) and SF MCS (t(164)= 3.64, p=.000) compared to those who did not.
Table 2.
Correlations between psychosocial and illness-related variables and the total rate of impairment
| Variable | Entire sample | Yes psych dx | No psych dx |
|---|---|---|---|
|
| |||
| PHQ8 | .555** | .524** | 0.203 |
| GAD | .381** | 0.19 | 0.174 |
| Panic | .286** | 0.16 | 0.07 |
| VSI | .371** | .230* | .354** |
| IBS-SSS | .467** | .397** | .403** |
| SF12 PCS | −.436** | −.379** | −.373** |
| SF12 MCS | −0.120 | 0.01 | 0.031 |
Correlation is significant at the 0.01 level
Correlation is significant at the .05 level
Psychiatric diagnoses were determined using questionnaire-based criteria (PHQ modules: PHQ8 for depression; GAD-7 for anxiety; Panic module for panic disorder)
Discussion
In this study, we observed a high level of impairment and/or avoidance of daily activities associated with IBS. In addition, we found that the level of impairment was higher for subjects who met criteria for depression, anxiety, and/or panic disorder.
The majority of respondents in this study reported IBS-related impairment in daily living, with 76% of the sample reporting some degree of impairment in at least 5 different domains of daily life. Reported impairment was closely associated with symptom severity, GI-specific anxiety, and quality of life. To our knowledge, this is the first study since Corney and Stanton’s original study in 199010 to characterize and quantify the specific impact of IBS on daily functioning. This study contributes uniquely to the large body of research on the effect of IBS on overall quality of life by elucidating the specific behavioral impact of IBS on daily living. Existing quality of life research suggests that IBS is perceived to be as debilitating as the flu9 and that reported QoL is lower in IBS when compared to gastroesophageal reflux disease, inflammatory bowel diseases, diabetes, and end-stage renal disease25,26. Although reasons for such low QoL in IBS have not been clearly identified, it is apparent that the impact of IBS on a patient’s daily life should not be underestimated27.
Out of ten domains of daily living assessed in this study, social functioning, eating alone, and job functioning were reported to be the most affected by IBS. IBS-related impairments in social functioning and job functioning have been well-demonstrated in other quality of life research5. The impact of IBS on eating behavior (i.e. food choices), however, has not yet been well-researched28. The findings of this study suggest that individuals with IBS report more impairment when eating alone compared to when eating in groups. This finding is somewhat surprising, as eating in groups typically involves socializing and eating outside of the home, both of which could be potential stressors for an IBS patient. This finding may indicate that individuals with IBS are more likely to regulate or restrict their diets when they are eating alone. Accordingly, the “eating alone” category likely reflects food choices and dietary restrictions, while the “eating in groups” category reflects social eating situations. Moving forward, it may be best to change the title of these domains.
Interestingly, individuals who met questionnaire-based criteria for comorbid depression, anxiety, and/or panic disorder reported a higher degree of impairment/avoidance due to their IBS symptoms when compared to respondents without these psychiatric comorbidities. This is likely due in part to the nature of these diagnoses, all of which are characterized by some degree of impairment in functioning. However, our finding is striking in that the respondents attributed their impairment directly to IBS symptoms and not to depression, anxiety or other factors. The findings presented in this study support the importance of integrated psychosocial and medical care for IBS patients, and may support early evaluation and intervention for behavioral avoidance/impairment especially among those who exhibit signs or symptoms of psychiatric diagnoses.
As mentioned earlier, the current study contributes to the overall quality of life literature by providing specific data regarding the behavioral impact of IBS on daily functioning. The QoL construct is particularly important in chronic functional illnesses, like IBS, because it accounts for social and emotional consequences of a patient’s illness. Measuring these consequences in addition to physical symptoms provides a more accurate understanding of the overall illness impact. However, existing QoL measures do not parse out all of the domains of daily living that were assessed in the present study. Typically, QoL measures identify broad areas of emotional and physical functioning and assess general difficulty within these areas without assessing specific behavioral impairment or avoidance. Our finding that individuals with IBS report high levels of impairment and avoidance across a range of daily activities supports existing QoL research in IBS while providing specific information about how QoL is impaired on a day-to-day basis.
There were several limitations to this study. First, participants were part of an online survey study and, therefore, did not have clinician-verified IBS. Exclusion criteria included previous diagnosis of Inflammatory Bowel Diseases and current or recent (last 12 weeks) pregnancy. Other GI and non-GI comorbidities were not assessed, which reflects a limitation of this study’s sampling. However, given the high diagnostic sensitivity of the ROME-III criteria13 and the knowledge that a large portion of people suffering from IBS in the general population do not seek medical treatment for their symptoms29, this study sample was likely representative of the IBS population.
Second, we were inadequately powered to assess differences in daily functioning among IBS subtypes. Prevalence studies in western countries have revealed mixed results regarding prevalence rates of IBS-C and IBS-D, and rates of IBS subtypes appear to vary widely across cultures 30. Although there are no documented differences in quality of life between IBS-C and IBS-D, it appears that individuals with IBS-D are more likely to be referred to tertiary care clinics, and therefore may be more likely to seek medical attention or to connect with online resources 31,32. In our sample, the majority of respondents reported IBS Mixed Type (58.7%), followed by IBS-D (31.8%), and IBS-C (9.5%). Thus, we were unable to draw conclusions about differences in IBS-subtypes and our results may be most applicable to non-constipated IBS-patients.
Third, as in Corney and Stanton’s original study, we relied upon a non-validated measure of functional impairment. The measure was modeled after the original study as well as after other Quality of Life measures that have since been developed. The lack of an appropriate, validated measure for this construct reflects a significant gap in the literature. Despite a large body of research in physical impairment among chronic pain populations, available validated measures focus primarily on physical ability to perform tasks (e.g. self-care, household chores), which is not appropriate for this patient population. There are no available validated measures of avoidance and impairment in broad activities of daily living (e.g. socializing, traveling, exercising, leisure), which demonstrates the need for further research into the impact of chronic, functional illnesses on a patient’s ability to participate in daily activities. Of course, there are many existing measures of quality of life, which typically measure similar domains. However, QoL is a separate construct and does not provide clear data about avoidance/impairment of activities. Future directions will seek to validate this measure.
Conclusion
This study contributes to existing literature by quantifying the level of symptom-related impairment in a sample of participants with ROME-III IBS and by identifying particularly salient psychological and symptom-specific variables that might contribute to such impairment.
Key points.
The impact of IBS on daily functioning has not been adequately researched. This study characterizes daily impairment in patients with IBS.
The majority of respondents reported impairment in at least 5 domains of daily living. Rates of impairment were highest among participants who met questionnaire-based criteria for psychiatric diagnoses.
These results support the importance of integrated psychosocial and medical care for IBS and may support early evaluation and intervention among those with psychiatric diagnoses.
Acknowledgments
SB and LK designed the research study. SB performed the research and analyzed the data. SB and LK wrote the paper. This research was supported in part by an NIDDK training grant to the Division of Gastroenterology at Beth Israel Deaconness Medical Center (5T32DK007760-17).

References
- 1.Grundmann O, Yoon SL. Irritable bowel syndrome: epidemiology, diagnosis and treatment: an update for health-care practitioners. J Gastroenterol Hepatol. 2010 Apr;25(4):691–699. doi: 10.1111/j.1440-1746.2009.06120.x. [DOI] [PubMed] [Google Scholar]
- 2.Drossman DA, Camilleri M, Mayer EA, Whitehead WE. AGA technical review on irritable bowel syndrome. Gastroenterology. 2002 Dec;123(6):2108–2131. doi: 10.1053/gast.2002.37095. [DOI] [PubMed] [Google Scholar]
- 3.Kanuri N, Cassell B, Bruce SE, et al. The impact of abuse and mood on bowel symptoms and health-related quality of life in irritable bowel syndrome (IBS) Neurogastroenterol Motil. 2016 May 5; doi: 10.1111/nmo.12848. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Shih YC, Barghout VE, Sandler RS, et al. Resource utilization associated with irritable bowel syndrome in the United States 1987–1997. Dig Dis Sci. 2002 Aug;47(8):1705–1715. doi: 10.1023/a:1016471923384. [DOI] [PubMed] [Google Scholar]
- 5.Pare P, Gray J, Lam S, et al. Health-related quality of life, work productivity, and health care resource utilization of subjects with irritable bowel syndrome: baseline results from LOGIC (Longitudinal Outcomes Study of Gastrointestinal Symptoms in Canada), a naturalistic study. Clin Ther. 2006 Oct;28(10):1726–1735. doi: 10.1016/j.clinthera.2006.10.010. discussion 1710–1721. [DOI] [PubMed] [Google Scholar]
- 6.Dean BB, Aguilar D, Barghout V, et al. Impairment in work productivity and health-related quality of life in patients with IBS. Am J Manag Care. 2005 Apr;11(1 Suppl):S17–26. [PubMed] [Google Scholar]
- 7.Hungin AP, Whorwell PJ, Tack J, Mearin F. The prevalence, patterns and impact of irritable bowel syndrome: an international survey of 40,000 subjects. Alimentary Pharmacology and Therapeutics. 2003 Mar 1;17(5):643–650. doi: 10.1046/j.1365-2036.2003.01456.x. [DOI] [PubMed] [Google Scholar]
- 8.Koloski NA, Talley NJ, Boyce PM. The impact of functional gastrointestinal disorders on quality of life. Am J Gastroenterol. 2000 Jan;95(1):67–71. doi: 10.1111/j.1572-0241.2000.01735.x. [DOI] [PubMed] [Google Scholar]
- 9.Dapoigny M, Bellanger J, Bonaz B, et al. Irritable bowel syndrome in France: a common, debilitating and costly disorder. European Journal of Gastroenterology and Hepatology. 2004 Oct;16(10):995–1001. doi: 10.1097/00042737-200410000-00008. [DOI] [PubMed] [Google Scholar]
- 10.Corney RH, Stanton R. Physical symptom severity, psychological and social dysfunction in a series of outpatients with irritable bowel syndrome. J Psychosom Res. 1990;34(5):483–491. doi: 10.1016/0022-3999(90)90022-v. [DOI] [PubMed] [Google Scholar]
- 11.Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterology. 2006 Apr;130(5):1480–1491. doi: 10.1053/j.gastro.2005.11.061. [DOI] [PubMed] [Google Scholar]
- 12.Drossman DA, Dumitrascu DL. Rome III: New standard for functional gastrointestinal disorders. J Gastrointestin Liver Dis. 2006 Sep;15(3):237–241. [PubMed] [Google Scholar]
- 13.Whitehead WE, POS, Thiwan SIM, et al. Development and validation of the Rome III diagnostic questionnaire. In: Drossman DA, CE, Delvaux M, editors. Rome III: The Functional Gastrointestinal Disorders. 3. McLean, VA: Degnon Associates; 2006. pp. 835–853. [Google Scholar]
- 14.Francis CY, Duffy JN, Whorwell PJ, Morris J. High prevalence of irritable bowel syndrome in patients attending urological outpatient departments. Dig Dis Sci. 1997 Feb;42(2):404–407. doi: 10.1023/a:1018838507545. [DOI] [PubMed] [Google Scholar]
- 15.Kroenke K, Strine TW, Spitzer RL, Williams JB, Berry JT, Mokdad AH. The PHQ-8 as a measure of current depression in the general population. J Affect Disord. 2009 Apr;114(1–3):163–173. doi: 10.1016/j.jad.2008.06.026. [DOI] [PubMed] [Google Scholar]
- 16.Corson K, Gerrity MS, Dobscha SK. Screening for depression and suicidality in a VA primary care setting: 2 items are better than 1 item. Am J Manag Care. 2004 Nov;10(11 Pt 2):839–845. [PubMed] [Google Scholar]
- 17.Spitzer RL, Kroenke K, Williams JB, Lowe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006 May 22;166(10):1092–1097. doi: 10.1001/archinte.166.10.1092. [DOI] [PubMed] [Google Scholar]
- 18.Spitzer RL, Williams JB, Kroenke K, Hornyak R, McMurray J. Validity and utility of the PRIME-MD patient health questionnaire in assessment of 3000 obstetric-gynecologic patients: the PRIME-MD Patient Health Questionnaire Obstetrics-Gynecology Study. Am J Obstet Gynecol. 2000 Sep;183(3):759–769. doi: 10.1067/mob.2000.106580. [DOI] [PubMed] [Google Scholar]
- 19.Rief W, Nanke A, Klaiberg A, Braehler E. Base rates for panic and depression according to the Brief Patient Health Questionnaire: a population-based study. J Affect Disord. 2004 Oct 15;82(2):271–276. doi: 10.1016/j.jad.2003.11.006. [DOI] [PubMed] [Google Scholar]
- 20.Lowe B, Grafe K, Zipfel S, et al. Detecting panic disorder in medical and psychosomatic outpatients: comparative validation of the Hospital Anxiety and Depression Scale, the Patient Health Questionnaire, a screening question, and physicians’ diagnosis. J Psychosom Res. 2003 Dec;55(6):515–519. doi: 10.1016/s0022-3999(03)00072-2. [DOI] [PubMed] [Google Scholar]
- 21.Labus JS, Bolus R, Chang L, et al. The Visceral Sensitivity Index: development and validation of a gastrointestinal symptom-specific anxiety scale. Aliment Pharmacol Ther. 2004 Jul 1;20(1):89–97. doi: 10.1111/j.1365-2036.2004.02007.x. [DOI] [PubMed] [Google Scholar]
- 22.Ware JE, Kosinski M, Keller SD. A 12-item short-form health survey - Construction of scales and preliminary tests of reliability and validity. Medical care. 1996 Mar;34(3):220–233. doi: 10.1097/00005650-199603000-00003. [DOI] [PubMed] [Google Scholar]
- 23.Ware JE, Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Medical care. 1992 Jun;30(6):473–483. [PubMed] [Google Scholar]
- 24.McHorney CA, Ware JE, Jr, Raczek AE. The MOS 36-Item Short-Form Health Survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Medical care. 1993 Mar;31(3):247–263. doi: 10.1097/00005650-199303000-00006. [DOI] [PubMed] [Google Scholar]
- 25.Gralnek IM, Hays RD, Kilbourne A, Naliboff B, Mayer EA. The impact of irritable bowel syndrome on health-related quality of life. Gastroenterology. 2000 Sep;119(3):654–660. doi: 10.1053/gast.2000.16484. [DOI] [PubMed] [Google Scholar]
- 26.Cai Q, Buono JL, Spalding WM, et al. Health-Related Quality of Life, Work Productivity, and Daily Activity Among A Sample of Commercially Insured Patients With Irritable Bowel Syndrome With Constipation or Chronic Constipation In The United States. Value Health. 2015 Nov;18(7):A631. doi: 10.1016/j.jval.2014.08.839. [DOI] [PubMed] [Google Scholar]
- 27.Monnikes H. Quality of life in patients with irritable bowel syndrome. J Clin Gastroenterol. 2011 Aug;45( Suppl):S98–101. doi: 10.1097/MCG.0b013e31821fbf44. [DOI] [PubMed] [Google Scholar]
- 28.Fletcher PC, Schneider MA. Is there any food I can eat? Living with inflammatory bowel disease and/or irritable bowel syndrome. Clin Nurse Spec. 2006 Sep-Oct;20(5):241–247. doi: 10.1097/00002800-200609000-00011. [DOI] [PubMed] [Google Scholar]
- 29.Drossman DA, Li Z, Andruzzi E, et al. U.S. householder survey of functional gastrointestinal disorders. Prevalence, sociodemography, and health impact. Dig Dis Sci. 1993 Sep;38(9):1569–1580. doi: 10.1007/BF01303162. [DOI] [PubMed] [Google Scholar]
- 30.Ballou SK, Keefer L. Multicultural considerations in the diagnosis and management of irritable bowel syndrome: a selective summary. European journal of gastroenterology & hepatology. 2013 Oct;25(10):1127–1133. doi: 10.1097/MEG.0b013e3283632bf2. [DOI] [PubMed] [Google Scholar]
- 31.Schmulson M, Lee OY, Chang L, Naliboff B, Mayer EA. Symptom differences in moderate to severe IBS patients based on predominant bowel habit. The American journal of gastroenterology. 1999 Oct;94(10):2929–2935. doi: 10.1111/j.1572-0241.1999.01440.x. [DOI] [PubMed] [Google Scholar]
- 32.Simren M, Abrahamsson H, Svedlund J, Bjornsson ES. Quality of life in patients with irritable bowel syndrome seen in referral centers versus primary care: the impact of gender and predominant bowel pattern. Scandinavian journal of gastroenterology. 2001 May;36(5):545–552. doi: 10.1080/003655201750153476. [DOI] [PubMed] [Google Scholar]