

Abstract
Cerebral metastasis secondary to prostatic adenocarcinoma is rare and it is usually a late complication in patients with widespread distant metastases. Here, we report two unusual cases of such a rare condition. Our first case presented with a large frontal contrast-enhancing lesion-associated calcification and a large tumor cyst as shown on computed tomography and magnetic resonance imaging. This is the fifth reported case of prostatic metastasis manifesting as a cystic intraparenchymal tumor in the literature. The second case presented with a large soft tissue mass in the scalp and this lesion appeared to invade through the skull and into the middle cranial fossa. He was not known to have prostate cancer before his initial presentation and it was only diagnosed following histology results of the scalp lesion.
Keywords: cerebral metastasis, prostate cancer, brain tumors, prostatic adenocarcinoma
Introduction
Prostate cancer is a common condition amongst men and its prevalence has been increasing because of the aging population worldwide. Cerebral metastasis, however, is seldom seen amongst patients with prostate cancer. Even when present, it is only seen as a late complication in patients with widespread distant metastases in various organs. Here we report two unusual cases of such rare condition.
Case 1
P.H. is a 56-year-old male patient with a background history of metastatic castration-resistant prostatic adenocarcinoma (initial Gleason score of 5 + 4 = 9). He presented with 8 weeks history of worsening expressive dysphasia and his prostate-specific antigen (PSA) on admission was 1,472 μg/L (normal range: < 3.5 μg/L). Initial computed tomography (CT) brain demonstrated a contrast-enhancing mass measuring 47 mm × 21 mm × 47 mm associated with calcification and extensive vasogenic edema in the left frontal lobe (Fig. 1). Extending from the mass lesion is a cystic structure measuring 44 mm that appears to be compressing on the genu of the corpus callosum. Magnetic resonance imaging (MRI) subsequently showed six additional metastases throughout the supratentorial compartment. Near-total excision of the left frontal lesion was performed (Fig. 2) and histology confirmed metastatic adenocarcinoma of prostatic origin. He recovered postoperatively and was discharged 3 days later.
Fig. 1.
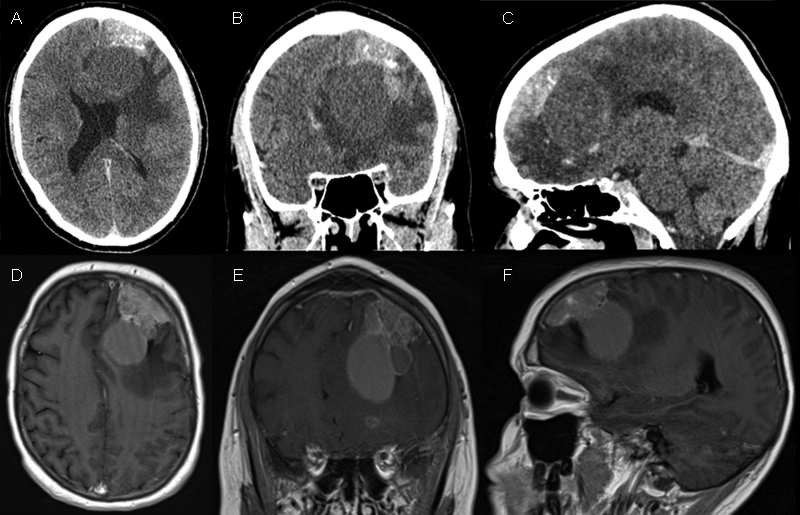
Preoperative CT brain with contrast in axial (A), coronal (B), and sagittal (C) section demonstrating the left frontal lesion with heterogeneous contrast enhancement, calcification and a tumor cyst compressing on the genu of corpus callosum. Preoperative MRI brain with gadolinium in axial (D), coronal (E), and sagittal (F) section demonstrating the same lesion. CT, computed tomography; MRI, magnetic resonance imaging.
Fig. 2.
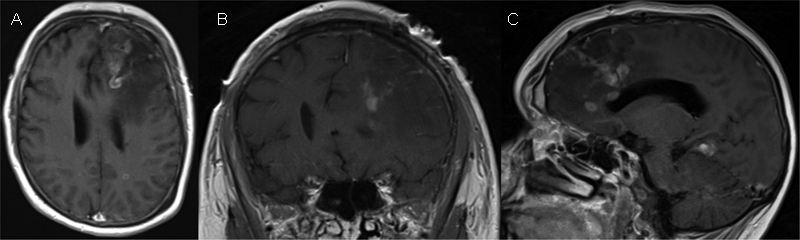
Postoperative MRI brain with gadolinium in axial (A), coronal (B), and sagittal (C) section demonstrating the postoperative changes following a partial debulking of the tumor and drainage of the tumor cyst with evidence of residual-enhancing lesion in the posteromedial margin. MRI, magnetic resonance imaging.
Case 2
U.S. is a 65-year-old male patient with no known history of malignancy, presented with a left temporal soft tissue mass that had been increasing in size over the preceding 2 months. This was associated with the 1-month history of worsening left eye ptosis. CT showed a contrast-enhancing mass measuring 91 mm × 62 mm × 96 mm extending from the left middle cranial fossa, through the temporal bone and into the subgaleal region (Fig. 3). The mass effect of the lesion results in a midline shift of 11 mm and the bone within the lesion has a sunburst type appearance. In addition, MRI showed prominent dural enhancement adjacent to the lesion. Staging CT demonstrated extensive sclerotic bony lesions throughout the axial skeleton and a moderately enlarged prostate associated with extensive internal and external iliac lymphadenopathy. PSA was found to be 645 μg/L (normal range: < 3.5 μg/L). Biopsy of the extracranial portion of the soft tissue mass was performed and histology confirmed metastatic adenocarcinoma of prostatic origin. He was subsequently referred to urology and oncology for ongoing management.
Fig. 3.

CT brain with contrast in axial (A) and coronal (B) section demonstrating the left frontotemporal mass with homogenous contrast enhancement invading through the skull and into the middle cranial fossa. The bone window of CT brain in axial (C) and coronal (D) shows the sunburst appearance of the skull. MRI brain with gadolinium in axial (E) and coronal (F) demonstrating the same lesion. CT, computed tomography; MRI, magnetic resonance imaging.
Discussion
Cerebral metastases are the most common intracranial neoplasms in adults, representing more than 50% of all the reported brain tumors.1 2 It is a frequent neurological complication that was reported in 10 to 40% of adults and 6 to 10% of children with malignant disease.2 3 4 With the advance of more targeted oncological treatment, and hence an improved survival and an increasing use of MRI, there has been a steady rise in the incidence of cerebral metastases over the last two decades.5 6 In particular, approximately 170,000 new cases cerebral metastasis is reported annually in the United States.7
Primary tumors that are commonly associated with cerebral metastasis include small cell lung cancer, nonsmall cell lung cancer, melanoma, renal cancer, breast cancer, and colorectal cancer.6 Prostate cancer, however, rarely metastasizes to the brain. Early autopsy study by Saitoh et al reported a 1.1% rate of cerebral metastasis amongst 1,885 patients with prostate cancer.8 Such rate of cerebral metastasis is noted to be even lower in clinical studies, with only 4 out of 3,732 patients with prostate cancer were found to have intracranial involvement.9 Despite the rarity of this condition, cerebral metastases from prostatic carcinoma are relatively well described in the literature. Several case reports have been published over the last few decades regarding prostatic metastases in the supratentorial region,10 11 posterior fossa,10 11 12 brain stem,13 and cerebellopontine angle.14 15
Here, we reported a rare case of metastatic prostate adenocarcinoma presented as a cystic and solitary intraparenchymal tumor with no evidence of systemic disease. Intracranial metastasis from prostate cancer is rare, and prostatic metastasis manifesting as a cystic intraparenchymal tumor is even rarer. Bland et al reported the first case of a large cystic intracranial metastasis from prostate cancer in 1992.16 Since then, three other similar cases were reported by a case report by Behrens et al and a case series by Tsai et al. in 2001.17 18 Therefore, to the best of our knowledge, this is the fifth reported case of prostatic metastasis manifesting as cystic intraparenchymal tumor in the literature.
Our second patient was not known to have prostate cancer before his initial presentation with a soft tissue mass in the scalp. Base on the radiological features of the lesion, osteosarcoma, and atypical meningioma were both considered as potential differential diagnoses. Adenocarcinoma of the prostate was only diagnosed following the biopsy results of the soft tissue mass in the scalp. Subsequent staging CT scan demonstrated an enlarged prostate with patchy enhancement and widespread sclerotic bony metastases throughout the axial skeleton. To the best of our knowledge, this is the first reported case of prostate adenocarcinoma with a solitary cerebral metastasis as the first manifestation.
Conclusion
Prostatic metastasis to the brain is considered a late complication and it is associated with a poor prognosis. Early diagnosis and treatment of prostate cancer plays an essential role in preventing the progression of the disease to the brain. With the current lack of funding to the National Health Service and the lack of a reliable test to implement a screening program for prostate cancer, the incidence of cerebral metastasis secondary to prostate cancer is likely to increase in the near future.
Funding
None.
Footnotes
Conflict of Interest None.
References
- 1.Posner J B.Management of brain metastases Rev Neurol (Paris) 1992148(6-7):477–487. [PubMed] [Google Scholar]
- 2.Soffietti R, Rudā R, Mutani R. Management of brain metastases. J Neurol. 2002;249(10):1357–1369. doi: 10.1007/s00415-002-0870-6. [DOI] [PubMed] [Google Scholar]
- 3.Gavrilovic I T, Posner J B. Brain metastases: epidemiology and pathophysiology. J Neurooncol. 2005;75(01):5–14. doi: 10.1007/s11060-004-8093-6. [DOI] [PubMed] [Google Scholar]
- 4.Graus F, Walker R W, Allen J C. Brain metastases in children. J Pediatr. 1983;103(04):558–561. doi: 10.1016/s0022-3476(83)80583-6. [DOI] [PubMed] [Google Scholar]
- 5.Smedby K E, Brandt L, Bäcklund M L, Blomqvist P. Brain metastases admissions in Sweden between 1987 and 2006. Br J Cancer. 2009;101(11):1919–1924. doi: 10.1038/sj.bjc.6605373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Nieder C, Spanne O, Mehta M P, Grosu A L, Geinitz H. Presentation, patterns of care, and survival in patients with brain metastases: what has changed in the last 20 years? Cancer. 2011;117(11):2505–2512. doi: 10.1002/cncr.25707. [DOI] [PubMed] [Google Scholar]
- 7.Langer C J, Mehta M P. Current management of brain metastases, with a focus on systemic options. J Clin Oncol. 2005;23(25):6207–6219. doi: 10.1200/JCO.2005.03.145. [DOI] [PubMed] [Google Scholar]
- 8.Saitoh H, Hida M, Shimbo T, Nakamura K, Yamagata J, Satoh T. Metastatic patterns of prostatic cancer. Correlation between sites and number of organs involved. Cancer. 1984;54(12):3078–3084. doi: 10.1002/1097-0142(19841215)54:12<3078::aid-cncr2820541245>3.0.co;2-u. [DOI] [PubMed] [Google Scholar]
- 9.Catane R, Kaufman J, West C, Merrin C, Tsukada Y, Murphy G P. Brain metastasis from prostatic carcinoma. Cancer. 1976;38(06):2583–2587. doi: 10.1002/1097-0142(197612)38:6<2583::aid-cncr2820380652>3.0.co;2-d. [DOI] [PubMed] [Google Scholar]
- 10.Lynes W L, Bostwick D G, Freiha F S, Stamey T A. Parenchymal brain metastases from adenocarcinoma of prostate. Urology. 1986;28(04):280–287. doi: 10.1016/0090-4295(86)90005-1. [DOI] [PubMed] [Google Scholar]
- 11.Sutton M A, Watkins H L, Green L K, Kadmon D. Intracranial metastases as the first manifestation of prostate cancer. Urology. 1996;48(05):789–793. doi: 10.1016/S0090-4295(96)00238-5. [DOI] [PubMed] [Google Scholar]
- 12.Lewis I. Cerebellar metastasis from prostatic carcinoma. A case report. Neurology. 1967;17(07):698–702. doi: 10.1212/wnl.17.7.698. [DOI] [PubMed] [Google Scholar]
- 13.Gupta A, Baidas S, Cumberlin R K. Brain stem metastasis as the only site of spread in prostate carcinoma. A case report. Cancer. 1994;74(09):2516–2519. doi: 10.1002/1097-0142(19941101)74:9<2516::aid-cncr2820740920>3.0.co;2-c. [DOI] [PubMed] [Google Scholar]
- 14.Flickinger F W, Yuh W T, Nichols R D, II, Kemp J D. Solitary prostatic metastasis to the cerebellopontine angle: MR and CT findings. J Comput Assist Tomogr. 1989;13(06):1088–1090. [PubMed] [Google Scholar]
- 15.Maiuri F, Corriero G, D'Amico L, Iaconetta G. Cerebellar metastasis from prostatic carcinoma simulating, on CT-scan, a cerebellopontine angle tumor. Case report. Acta Neurol (Napoli) 1989;11(01):21–24. [PubMed] [Google Scholar]
- 16.Bland L I, Welch W C, Okawara S H. Large cystic intraparenchymal brain metastasis from prostate cancer. Neuroradiology. 1992;34(01):70–72. doi: 10.1007/BF00588437. [DOI] [PubMed] [Google Scholar]
- 17.Tsai V, Kim S, Clatterbuck R E, Ewend M G, Olivi A. Cystic prostate metastases to the brain parenchyma: report of two cases and review of the literature. J Neurooncol. 2001;51(02):167–173. doi: 10.1023/a:1010606427945. [DOI] [PubMed] [Google Scholar]
- 18.Behrens B, Husain M M, Schmidley J W. Cystic solitary intracerebral metastasis from prostate adenocarcinoma. Neuroradiology. 2001;43(02):162–164. doi: 10.1007/s002340000509. [DOI] [PubMed] [Google Scholar]