

Abstract
Objective:
To determine the frequency of dyslipidemia in patients with Rheumatoid Arthritis.
Methods:
This is a prospective, cross-sectional, observational study, conducted at the ‘Rheumatology Clinic’ of Jinnah Postgraduate Medical Center (JPMC), Karachi, from November 2013 to May 2014. A total of 200 patients of Rheumatoid Arthritis (RA), diagnosed according to the ACR/EULAR criteria 2010, were included in the study. Laboratory investigations including creatinine, ALT, CBC, TSH and fasting lipid profile (LDL, HDL, and Total cholesterol) were done for all patients.
Results:
Out of 200 patients, 23 (11.5%) were male and 177 (88.5%) were female. The mean age was 36.31±10.46 years and the mean duration of disease was 3.82±3.03 years. A total of 107 (53.5%) patients had dyslipidemia, and the commonest abnormality was a low HDL, seen in 83 (41.5 %) patients.
Conclusion:
Dyslipidemia was frequently observed in Rheumatoid Arthritis. This may be considered as a secondary impact of chronic inflammatory state, seen in RA. Lipid abnormalities should be sought at regular intervals, and corrective actions taken to mitigate increased cardiovascular disease risk.
Keywords: Cholesterol, Dyslipidemia, Rheumatoid Arthritis
INTRODUCTION
Rheumatoid Arthritis (RA) is a chronic multisystem disease with heterogeneous presentation, variable disease progression and extra-articular manifestations. The estimated prevalence of RA has been reported from Northern Pakistan as 0.55%;1 while, the prevalence of RA in adult Indian population is reportedly 0.75%.2 It has been observed that RA patients have greater rates of cardiovascular (CV) morbidity and mortality.3,4 Studies indicate that the risk of incidental cardiovascular disease (CVD) is increased by 48% in patients with RA compared to the general population.5
Lipid metabolism is a complex process, especially when associated with chronic inflammatory states; therefore in many autoimmune diseases lipid abnormalities are frequently seen. The involvement of common pro-inflammatory cytokines, such as interleukin - 1 and 6, tumor necrosis factor-alpha (TNF-α), play a role in the development and progression of both RA and atherosclerosis. Variable degrees of heightened inflammatory state is seen in RA, which alters the properties of HDL cholesterol, hence, the HDL paradoxically assumes pro-inflammatory properties, thereby accelerating endothelial dysfunction and plaque formation.6
Many studies have previously reported lipid abnormalities in RA patients.7-9 The dyslipidemia observed in RA patients is paradoxical to the general population, comprising of low total cholesterol and low HDL.10,11 The disproportionate ratio between HDL and TC levels, results in an increased atherogenic index (TC:HDL ratio), which is an important prognostic marker for cardiovascular disease (CVD). Dyslipidemia is prevalent in our general population as well. Therefore, this study was designed to observe the pattern of abnormal lipid profile in relation to chronic inflammatory state seen in RA patients.
METHODS
Study Design
This was a cross-sectional observational study, conducted at the ‘Rheumatology Clinic’ of JPMC, Karachi, from November 2013 to May 2014.
Inclusion Criteria
A total of 200 patients with the diagnosis of RA of > 6 month duration, according to the ACR/EULAR criteria 2010,12 of either sex, between the ages of 20-60 years were included in the study.
Exclusion Criteria
Patients not consenting and those with chronic diseases like Diabetes Mellitus, Hypothyroidism, Chronic kidney disease, Chronic liver disease, smokers, patients taking oral contraceptive pills and statins were excluded.
Dyslipidemia
A total cholesterol of ≥200 mg/dl or HDL Cholesterol <40 mg/dlor LDL Cholesterol ≥160 mg/dl were used to define the cut-off values for dyslipidemia, according to the National Cholesterol Education Program- Adult Treatment Panel III (NCEP-ATP III) guidelines.13
Data Collection
All the patients who fulfilled the inclusion criteria were included in the study. Prior approval was obtained from the Institutional Ethical Review Committee. Informed consent was taken from all the patients before assigning them to the study. History and physical examination was recorded in all patients. Blood sample was collected in a sterile manner after an overnight fast for serum cholesterol, LDL, and HDL levels. Data was recorded in a pre-designed proforma. Complete blood count (CBC), creatinine, ALT and Thyroid stimulating hormone (TSH) were also checked in all patients.
Data Analysis
Data was analyzed by using SPSS Version 17. Demographic data was presented as simple descriptive statistics, giving mean and standard deviation for age and duration of disease. For qualitative variables, like gender and dyslipidemia, frequency and percentages were reported.
RESULTS
A total of 200 patients, with the diagnosis of RA, were analyzed; 23 (11.5%) were male and 177 (88.5%) were female. The mean age was 36.31±10.46 and mean duration of disease was 3.82±3.03 years. Most common age bracket was 4th decade of life, constituting 75 (37.5%) patients. (Fig.1). A total of 139 (69.5%) patients had duration of disease of 1-4 years.
Fig. 1.
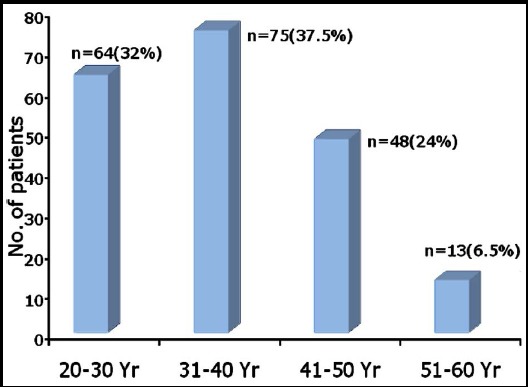
Age distribution among patients with RA.
Of all patients, 107 (53.5%) had dyslipidemia. The mean values for total cholesterol, HDL and LDL were 169.68±36.68 mg/dL, 40.02±10.23 mg/dL, and 93.29±26.17 mg/dL respectively (Table-I). Analysis of the lipid fractions in those who had dyslipidemia revealed that 83 patients (41.5%) had low HDL; 16 (8%) had high TC, whereas, 8 (4%) patients had combination of low HDL with high LDL and high TC(Fig.2). Majority of the patients with dyslipidemia were between 20-40 years of age, i.e. 139 (69.5%) patients.
Table-I.
Lipid levels in RA patients.
| Patients values Means±SD | Max-Min | |
|---|---|---|
| Total Cholesterol (mg/dl) | 169.68±36.68 | 65-321 |
| HDL (mg/dl) | 40.02±10.23 | 21-64 |
| LDL (mg/dl) | 93.29±26.17 | 54-182 |
Fig. 2.
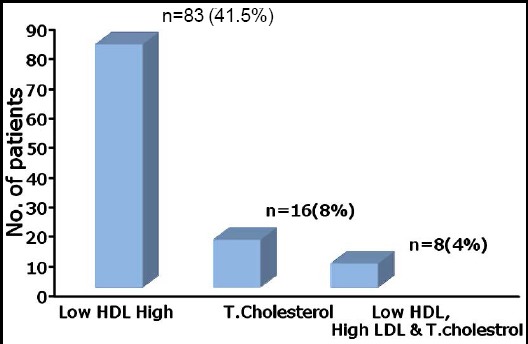
Distribution of lipid fractions in patients with dyslipidemia.
DISCUSSION
Dyslipidemia (DL) is frequently observed in patients with active RA.14 Systemic inflammation has a general effect in lowering circulating lipid levels.15 Moreover, patients with RA have an increased CVD risk at relatively low cholesterol levels, in contrast to that observed in the population without RA. These paradoxical changes in the lipid profiles of RA patients are still unclear, and the interactions between lipid fractions, inflammation and CVD risk in RA appears to be very complex. An Indian study, reported38.5% of dyslipidemia in a cohort of RA patients; commonest abnormality being low HDL.16 Another study from Pakistan reported an overall derangement of lipid profile in 44.87% of patients with different autoimmune diseases.17 The proportion of DL detected in our study is infact a little higher than that already reported in literature, commonest being low HDL. This is in contrast to that, reported by Nisar et al. where the commonest reported abnormality was high cholesterol.17 The commonest abnormality of low HDL may be a consequence of the unique pattern of lipid dysfunction that is seen in South-Asian population, which behaves differently in terms of accentuation of CVD risk. No population based study has been reported from Pakistan to reflect the exact prevalence of DL in our population. However, few studies have shown a prevalence of 40-87% of dyslipidemia in the context of metabolic syndrome and diabetes.18,19 As there is a strong association between metabolic syndrome and diabetes with dyslipidemia, hence it is not possible to relate these results to the entire population.
It has been reported that paradoxical lipid profile renders a patient to three fold increased CVD risk.20 Of note is that we need a more stringent control for DL, as ethnic variation in lipid profile is responsible for increased CVD risk and the high inflammatory state in RA patients, as this disease itself accentuates atherosclerosis. Patients with RA might benefit from being targeted with stricter than conventional CVD risk prevention and intervention.21,22 Evidence suggests that lipid lowering therapy may have beneficial effects in RA by virtue of their potent anti-inflammatory and immune-modulatory properties also.23 A vast majority of the patients with DL, in this study, were younger than 40 years, thus excluding aging as an exacerbating factor for occurrence of DL.
Despite there being an increased frequency of dyslipidemia in RA patients, it is unclear as to what extent these changes actually predispose an individual to increased CVD risk.24 Other studies have also reported the increased CVD risk even with marginally deranged traditional risk factors in RA patients compared to the healthy population.25,26
This is a small but systematic study to collate the estimates of lipid abnormalities in RA patients, and the results reflect the need of age-matched controlled comparable trials to observe the lipid profile in RA and control group and its relation, if any, to disease activity. Additional studies are needed to address the value of monitoring lipid profile, and to determine the effect of traditional CVD risk factors and inflammation and their impact on CV outcomes in RA patients. We also need to establish a strategy to monitor lipid profile at regular intervals in every individual with RA.
CONCLUSION
Dyslipidemia observed in RA is a frequent occurrence and may be considered as a secondary impact of chronic inflammatory state seen in RA patients. Identification and management of DL should be considered an integral part of RA therapeutic strategies to prevent CV morbidity and mortality in RA patients. Further studies are required to determine the interaction between DL and its impact on disease activity in RA patients.
Footnotes
Grant Support & Financial Disclosures: None.
Competing Interest: None
Authors’ Contributions
UE: Conception and design, acquisition, analysis and interpretation of data, drafting and revision of the article, final approval of the manuscript. Takes the responsibility for intellectual integrity of the study.
TA: Conception and design, drafting and revision of the article, final approval of the manuscript.
DK: Conception, acquisition and analysis and interpretation of data, drafting of the article, final approval of the manuscript.
REFERENCES
- 1.Farooqi A, Gibson T. Prevalence of the major rheumatic disorders in the adult population of Northern Pakistan. Br J Rheumatol. 1998;37:491–495. doi: 10.1093/rheumatology/37.5.491. [DOI] [PubMed] [Google Scholar]
- 2.Malaviya AN, Kapoor SK, Singh RR, Kumar A, Pande I. Prevalence of rheumatoid arthritis in the adult Indian population. Rheumatol Int. 1993;13(4):131–134. doi: 10.1007/BF00301258. doi:10.1007/BF00301258. [DOI] [PubMed] [Google Scholar]
- 3.Jacobsson LT, Knowler WC, Pillemer S, Hanson RL, Pettitt DJ, Nelson RG, et al. Rheumatoid arthritis and mortality. A longitudinal study in Pima Indians. Arthritis Rheum. 1993;36(8):1045–1053. doi: 10.1002/art.1780360804. [DOI] [PubMed] [Google Scholar]
- 4.Wolfe F, Mitchell DM, Sibley JT, Fries JF, Bloch DA, Williams CA, et al. The mortality of rheumatoid arthritis. Arthritis Rheum. 1994;37(4):481–494. doi: 10.1002/art.1780370408. [DOI] [PubMed] [Google Scholar]
- 5.Avina-Zubieta JA, Thomas J, Sadatsafavi M, Lehman AJ, Lacaille D. Risk of incident cardiovascular events in patients with rheumatoid arthritis: a meta-analysis of observational studies. Ann Rheum Dis. 2012;71(9):1524–1529. doi: 10.1136/annrheumdis-2011-200726. doi:10.1136/annrheumdis-2011-200726. [DOI] [PubMed] [Google Scholar]
- 6.Ansell BJ, Fonarow GC, Fogelman AM. The paradox of dysfunctional high density lipoprotein. Curr Opin Lipidol. 2007;18(4):427–434. doi: 10.1097/MOL.0b013e3282364a17. [DOI] [PubMed] [Google Scholar]
- 7.Gabriel SE, Crowson CS. Risk factors for cardiovascular disease in rheumatoid arthritis. Curr Opin Rheumatol. 2012;24(2):171–176. doi: 10.1097/BOR.0b013e32834ff2fd. doi:10.1097/BOR.0b013e32834ff2fd. [DOI] [PubMed] [Google Scholar]
- 8.Boyer JF, Gourraud PA, Cantagrel A, Davignon JL, Constantin A. Traditional cardiovascular risk factors in rheumatoid arthritis: a meta-analysis. Joint Bone Spine. 2011;78(2):179–183. doi: 10.1016/j.jbspin.2010.07.016. doi:10.1016/j.jbspin.2010.07.016. [DOI] [PubMed] [Google Scholar]
- 9.Choy E, Sattar N. Interpreting lipid levels in the context of high-grade inflammatory states with a focus on rheumatoid arthritis: a challenge to conventional cardiovascular risk actions. Ann Rheum Dis. 2009;68(4):460–469. doi: 10.1136/ard.2008.101964. doi:10.1136/ard.2008.101964. [DOI] [PubMed] [Google Scholar]
- 10.Steiner G, Urowitz MB. Lipid profiles in patients with rheumatoid arthritis: mechanisms and the impact of treatment. Semin Arthritis Rheum. 2008;38(5):372–381. doi: 10.1016/j.semarthrit.2008.01.015. doi:10.1016/j.semarthrit.2008.01.015. [DOI] [PubMed] [Google Scholar]
- 11.Amezaga UM, Suarez-Almazor ME. Lipid paradox in rheumatoid arthritis: changes with rheumatoid arthritis therapies. Curr Rheumatol Rep. 2012;14(5):428–437. doi: 10.1007/s11926-012-0269-z. doi:10.1007/s11926-012-0269-2. [DOI] [PubMed] [Google Scholar]
- 12.Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DJ, Bingham C, et al. Rheumatoid arthritis classification criteria. Arthritis Rheum. 2010;62(9):2569–2581. doi: 10.1002/art.27584. doi:10.1002/art.27584. [DOI] [PubMed] [Google Scholar]
- 13.Third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation and treatment of high blood cholesterol in adults (Adult Treatment Panel - ATP-III) IV- General Approach to treatment goals and thresholds. Circulation. 2002;106(25):3143–3421. [PubMed] [Google Scholar]
- 14.Park YB, Lee SK, Lee WK, Suh CH, Lee CW, Lee CH, et al. Lipid profiles in untreated patients with Rheumatoid arthritis. J Rheumatol. 1999;26(8):1701–1704. [PubMed] [Google Scholar]
- 15.Van Leuven SI, Franssen R, Kastelein JJ, Levi M, Stroes ESG, Tak PP. Systemic inflammation as a risk factor for atherothrombosis. Rheumatol. 2008;47(1):3–7. doi: 10.1093/rheumatology/kem202. [DOI] [PubMed] [Google Scholar]
- 16.Hadda V, Handa R, Aggarwal P, Lakshmy R, Umar UK, Pandey RM. Disease activity and lipids in rheumatoid arthritis: A prospective study. IJR. 2007;2(4):137–140. [Google Scholar]
- 17.Nisar A, Rasheed U, Aziz W, Farooqi A. Prevalence of dyslipidemia in autoimmune rheumatic diseases. J Coll Phys Surg Pak. 2012;22(4):235–239. doi:04.2012/jcpsp.235239. [PubMed] [Google Scholar]
- 18.Sarfraz M, Sajid S, Ashraf AM. Prevalence and pattern of dyslipidemia in hyperglycemic patients and its associated factors among Pakistani population. S J Bio Sci. 2016;23(6):761–766. doi: 10.1016/j.sjbs.2016.03.001. doi:10.1016/j.sjbs.2016.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Basit A, Shera SA. Prevalence of metabolic syndrome in Pakistan. Metab Syndr Relat Disord. 2008;6(3):171–175. doi: 10.1089/met.2008.0005. doi.10.1089/met.2008.005. [DOI] [PubMed] [Google Scholar]
- 20.Myasoedova E, Crowson CS, Kremers HM, Roger VL, Fitz-Gibbon PD, Therneau TM, et al. Lipid paradox in rheumatoid arthritis: the impact of serum lipid measures and systemic inflammation on the risk of cardiovascular disease. Ann Rheum Dis. 2011;70(3):482–487. doi: 10.1136/ard.2010.135871. doi:10.1136/ard.2010.135871. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Peters MJ, Symmons DP, McCarey D, Dijkmans BA, Nicola P, Kvien TK, et al. EULAR evidence-based recommendations for cardiovascular risk management in patients with rheumatoid arthritis and other forms of inflammatory arthritis. Ann Rheum Dis. 2010;69(2):325–331. doi: 10.1136/ard.2009.113696. doi:10.1136/ard.2009.113696. [DOI] [PubMed] [Google Scholar]
- 22.Van den Oever IA, van Sijl AM, Nurmohamed MT. Management of cardiovascular risk in patients with rheumatoid arthritis: evidence and expert opinion. Ther Adv Musculoskelet Dis. 2013;5(4):166–181. doi: 10.1177/1759720X13491025. doi:10.1177/1759720X13491025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.McCarey DW, McInnes IB, Madhok R, Hampson R, Scherbakov O, Ford I, et al. Trial of Atorvastatin in Rheumatoid Arthritis (TARA): double-blind, randomised placebo-controlled trial. Lancet. 2004;363(9426):2015–2021. doi: 10.1016/S0140-6736(04)16449-0. [DOI] [PubMed] [Google Scholar]
- 24.Kerola AM, Kauppi MJ, Kerola T, Nieminen TVM. How early in the course of rheumatoid arthritis does the excess cardiovascular risk appear? Ann Rheum Dis. 2012;71(10):1606–1615. doi: 10.1136/annrheumdis-2012-201334. doi:10.1136/annrheumdis-2012-201334. [DOI] [PubMed] [Google Scholar]
- 25.Haye-Salinas MJ, Bertoli AM, Lema L, Saucedo C, Rosa J, Quintana R, et al. Prevalence of dyslipidemia and elevated cardiovascular risk in patients with rheumatoid arthritis. Medicina (B Aires) 2013;73(1):26–30. [PubMed] [Google Scholar]
- 26.Curtis JR, John A, Baser O. Dyslipidemia and changes in lipid profiles associated with rheumatoid arthritis and initiation of anti-tumor necrosis factor therapy. Arthritis Care Res. 2012;64(9):1282–1291. doi: 10.1002/acr.21693. doi:10.1002/acr.21693. [DOI] [PMC free article] [PubMed] [Google Scholar]