

Introduction
Although surgical mitral valve repair or replacement is the treatment of choice for patients with severe mitral regurgitation (MR), up to 50% of these patients are denied surgery due to advanced age, poor left function, or comorbidities (1, 2). Percutaneous mitral valve repair using the MitraClip device (Abbott Laboratories, Abbott Park, IL, USA) has evolved as a less invasive therapeutic alternative for severe MR in patients who are inoperable or at a high risk for surgery (3, 4). Herein we report the case of a patient with severe MR who underwent percutaneous MitraClip implantation and suffered from embolization of one of the MitraClips in the right axillary artery during follow-up.
Case Report
A 29-year-old woman with a history of peripartum cardiomyopathy was referred to our clinic for heart failure and severe MR. Transthoracic echocardiography (TTE) demonstrated a dilated left ventricle with decreased systolic function (ejection fraction: 25%) and severe MR (vena contracta: 8 mm, effective regurgitant orifice area: 0.33 cm2, regurgitant volume: 52 mL, and regurgitant jet area: 12 cm2). Subsequent transesophageal echocardiography (TEE) confirmed the presence of severe MR between A2–P2 scallops and mild-to-moderate MR between A3–P3 scallops (Fig. 1). MitraClip procedure for severe MR was planned in order to improve her symptoms while waiting for a suitable donor.
Figure 1.
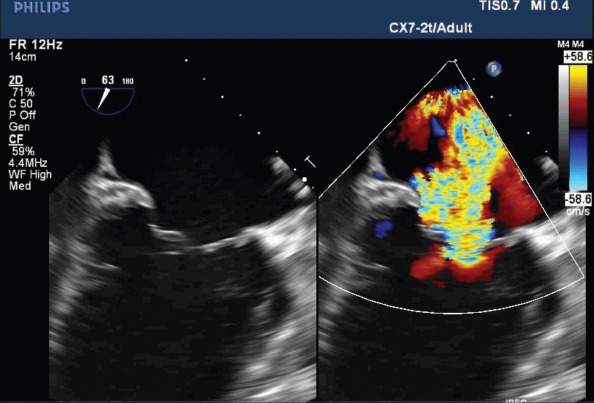
Transesophageal echocardiography demonstrates severe mitral regurgitation between A2–P2 scallops and mild-to-moderate regurgitation between A3–P3 scallops
A total of four MitraClip devices were implanted to reduce MR. The first MitraClip device was implanted in relation to the origin of the main regurgitant jet, between A2 and P2 scallops. Unfortunately, MR reduction was still not satisfactory after implantation of the second device. The third MitraClip device was implanted lateral to the first one with residual 2+ MR. We planned to terminate the procedure at that moment; however, after several minutes, TEE revealed severe MR due to detachment of the third MitraClip device from the posterior leaflet. Then, a fourth clip was implanted in order to stabilize the third clip. However, there was still a residual 3+ MR on the final control. Mean transmitral gradient was 6 mm Hg after implantation of the fourth MitraClip device. The patient refused to undergo further operation because of its high risk.
During follow-up periods at 1, 3, and 6 months after the procedure, TTE showed that three MitraClips were anchored to their site, whereas one MitraClip was solely attached to the anterior leaflet and MR remained to be 3+ (Fig. 2). After 1 year, she was admitted to our hospital with worsening heart failure symptoms. Chest X-ray showed an embolized MitraClip in her right axilla (Fig. 3). The patient reported no symptoms in the right upper extremity. Any vascular events related to embolized clip have not occurred since then.
Figure 2.
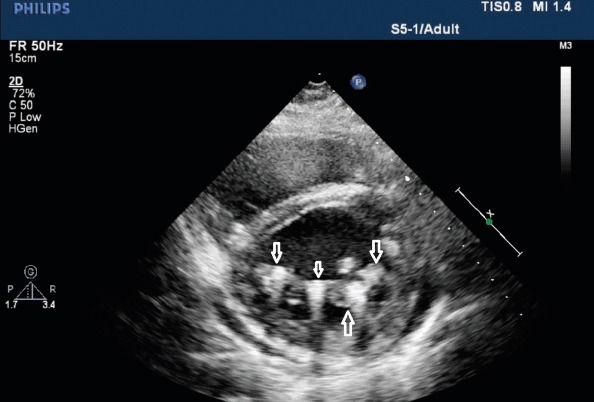
Parasternal short-axis view in transthoracic echocardiography demonstrates four MitraClips on the mitral valve position after 6 months (white arrows)
Figure 3.
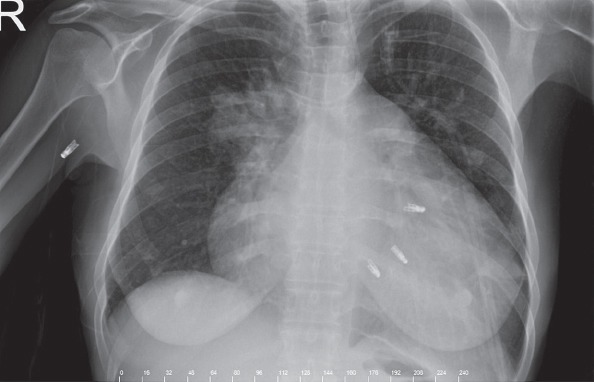
Chest X-ray demonstrates embolized MitraClip in the axillary artery and three MitraClips on the mitral valve position
Discussion
Partial clip detachment, embolization of clip, mitral valve stenosis, and clip entanglement in the chordae have been identified as potential complications specifically related to the MitraClip device (5). A total of nine patients (4.8%) were found to have partial detachment of the device within the first 12 months in the EVEREST II trial. After 12 months, one additional patient was found to have attachment of the device to a single leaflet (5). In ACCESS-EU study, single leaflet device detachment was reported in 4.8% of cases. There have been no reports of MitraClip device embolization in the ACCESS-EU study (6). Actually, only two cases of MitraClip embolization have been reported worldwide till date. One case with complete clip detachment and embolism has been reported in the study by Paranskaya et al. (7). The other case was that of a patient treated with surgery immediately after MitraClip implantation due to clip embolization. During surgery, one of the implanted MitraClips was not found on the valve and was detected in the renal artery (8).
During the procedure, one of the most important steps is imaging of proper grasping of the leaflets between the device arms. In our patient, the third implanted MitraClip detached from the posterior leaflet. We tried to stabilize this clip with a fourth MitraClip; unfortunately, we were not able to successfully reduce MR at the end. After 1 year, the detached MitraClip embolized to the axillary region.
Conclusion
Experience from our patient suggests that the use of multiple MitraClips may impose a higher risk for clip detachment, and embolization of the detached clip may occur at any time after the procedure.
References
- 1.Rossi A, Dini FL, Faggiano P, Agricola E, Cicoira M, Frattini S, et al. Independent prognostic value of functional mitral regurgitation in patients with heart failure. A quantitative analysis of 1256 patients with ischaemic and non-ischaemic dilated cardiomyopathy. Heart. 2011;97:1675–80. doi: 10.1136/hrt.2011.225789. [DOI] [PubMed] [Google Scholar]
- 2.Mirabel M, Iung B, Baron G, Messika-Zeitoun D, Détaint D, Vanoverschelde JL, et al. What are the characteristics of patients with severe, symptomatic, mitral regurgitation who are denied surgery? Eur Heart J. 2007;28:1358–65. doi: 10.1093/eurheartj/ehm001. [DOI] [PubMed] [Google Scholar]
- 3.Feldman T, Wasserman HS, Herrmann HC, Gray W, Block PC, Whitlow P, et al. Percutaneous mitral valve repair using the edge-to-edge technique:Six-month results of the EVEREST phase I clinical trial. J Am Coll Cardiol. 2005;46:2134–40. doi: 10.1016/j.jacc.2005.07.065. [DOI] [PubMed] [Google Scholar]
- 4.Franzen O, van der Heyden J, Baldus S, Schlüter M, Schillinger W, Butter C, et al. MitraClip thearpy in patients with end-stage systolic heart faliure. Eur J Heart Fail. 2011;13:569–76. doi: 10.1093/eurjhf/hfr029. [DOI] [PubMed] [Google Scholar]
- 5.Mauri L, Foster E, Glower DD, Apruzzese P, Massaro JM, Herrmann HC, et al. EVERST II investigators. 4 year results of a randomized controlled trial of percutaneous repair versus surgery for mitral regurgitation. J Am Coll Cardiol. 2013;62:317–28. doi: 10.1016/j.jacc.2013.04.030. [DOI] [PubMed] [Google Scholar]
- 6.Maisano F, Franzen O, Baldus S, Schäfer U, Hausleiter J, Butter C, et al. Percutaneous mitral valve interventions in the real world:early and 1-year results from the ACCESS-EU, a prospective, multicenter, nonrandomized post-approval study of the MitraClip therapy in Europe. J Am Coll Cardiol. 2013;62:1052–61. doi: 10.1016/j.jacc.2013.02.094. [DOI] [PubMed] [Google Scholar]
- 7.Paranskaya L, D’Ancona G, Bozdağ-Turan I, Akın I, Kische S, Turan GR, et al. Early and mid-term outcomes of percutaneous mitral valve repair with the MitraClip(R):Comparative analysis of different EuroSCORE strata. EuroIntervention. 2012;8:571–8. doi: 10.4244/EIJV8I5A88. [DOI] [PubMed] [Google Scholar]
- 8.Alozie A, Westphal B, Kische S, Kaminski A, Paranskaya L, Bozdağ-Turan I, et al. Surgical revision after percutaneous mitral valve repair by edge-to-edge device:when the strategy fails in the highest risk surgical population. Eur J Cardiothorac Surg. 2014;46:55–60. doi: 10.1093/ejcts/ezt535. [DOI] [PubMed] [Google Scholar]