

Abstract
We report two patients, one with congenital dystrophic medial rectus muscles and one with absence of the medial rectus muscles; in addition, one of them had absence of the lateral rectus muscles. While absence of the superior oblique and superior rectus has been more commonly reported in literature, especially with craniofacial syndromes, our patients were nonsyndromic. Considering the risk of anterior segment ischemia, correction of the large-angle exotropia was performed by horizontal rectus muscle surgery where possible, along with transfer of the superior oblique tendon to the superior part of the normal medial rectus muscle insertion area to create a tethering effect with a good outcome.
Keywords: Congenital absence, congenital dystrophy, lateral rectus, medial rectus, superior oblique tendon transfer
Congenital absence of the rectus muscles of the eye is rare. Most of these cases are associated with one of the craniofacial syndromes, the superior rectus or the superior oblique being commonly missing.[1] Absence of the inferior rectus muscle and its management has also been reported in literature.[2,3] We report two cases, one with congenital absence of the medial rectus muscle and one with congenital dystrophy of the medial rectus muscles with large-angle exotropia managed by superior oblique tendon transfer to the upper border of the normal medial rectus muscle insertion area with satisfactory results.
Case Reports
Case 1
A 19-year-old boy presented with large-angle exotropia noted since birth and an occasional right face turn. Vision was 6/6 in each eye. On examination, the anterior segment and fundus were within normal limits. Ocular examination revealed that he preferred fixation with the right eye. There was a face turn to the right of 15°. He had a large-angle exotropia (>100 PD) as measured by modified Krimsky test in all nine diagnostic positions of gaze [Fig. 1]. Ocular motility examination of both eyes revealed that he had absence of adduction (−4 on a scale of −4 to +4) beyond the midline while elevation, depression, and abduction were present. There was no fusion or stereopsis. Computed tomography scan showed the absence of medial rectus muscle in either eye in both the axial and coronal cuts [Fig. 2a and b]. He underwent surgery for the squint. Forced duction test on table did not reveal any tightness of muscles. The lateral rectus muscle in each eye was recessed by 10 mm. Exploration during surgery revealed complete absence of the medial rectus muscle [Fig. 3a]. Anterior ciliary vessels were absent. In both eyes, the superior oblique tendon was approached by a conjunctival incision lateral to the superior rectus. The superior oblique tendon was cut close to the insertion, resected by 7 mm, and placed at the superior part of the usual medial rectus scleral insertion with 5-0 polyester suture with the eye positioned in adduction on table. Good correction of the exotropia was obtained with the measurement in the primary position being 15 PD of exotropia at 3-year follow-up [Fig. 3b]. However, there was no remarkable improvement in the ductions, and fusion and stereopsis were not regained.
Figure 1.
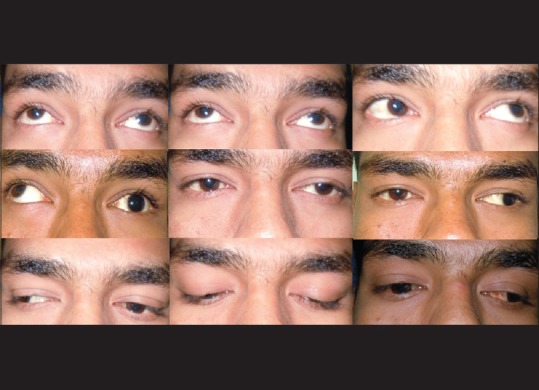
A 19-year-old boy with large-angle exotropia and limited ocular movements. Nine gaze pictures revealed absence of adduction in each eye
Figure 2.

Computed tomography scan of the orbits (a) axial sections revealed absence of medial rectus muscle in both eyes (arrow) and (b) coronal sections revealed absence of medial rectus muscle in both eyes (arrow)
Figure 3.
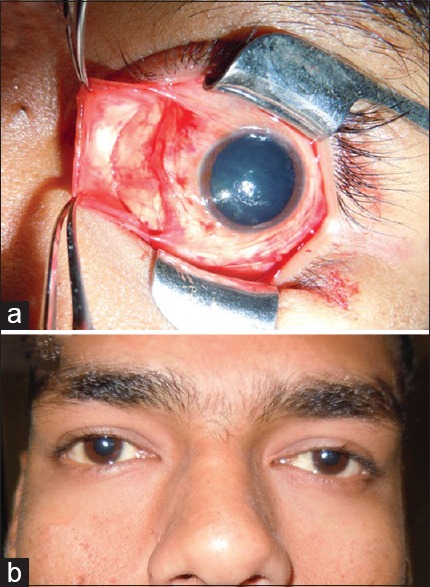
(a) During surgery, absence of the medial rectus muscle was noted (b) superior oblique tendon transfer was performed with satisfactory correction of the exotropia
Case 2
A 7-year-old girl presented with exotropia and limited ocular movements. She was noted by her parents to have divergent squint since birth. She needed to turn her face to look at objects on the sides. On examination, the vision was 6/9 in each eye with a refractive error of −1.50 DS in each eye. Anterior segment and fundus were within normal limits. There was moderate ptosis in both eyes. The lid crease was present in both eyes. Ocular examination revealed the presence of 70 PD of exotropia (on modified Krimsky test), with preference for right eye fixation though she could hold fixation well with each eye [Fig. 4a]. Ocular movements revealed marked limitation of abduction (−4 on a scale of −4 to + 4) and adduction (−4 on a scale of −4 to + 4) in each eye, while elevation and depression were present. There was no demonstrable fusion or stereopsis. During surgery, it was noted that there was no definite lateral or medial rectus muscles, and the anterior ciliary vessels were absent. On stretching the tissues in the medial rectus and lateral rectus muscle area on a muscle hook, it was noted to shred like Tenon's capsule [Fig. 4b and c]. To correct the exotropia, a superior oblique tendon transfer (with resection) to the superior part of the normal insertion area of the medial rectus was performed. Following surgery at the last 2-year follow-up, the residual exotropia was 15 PD. The ocular movements did not improve significantly.
Figure 4.
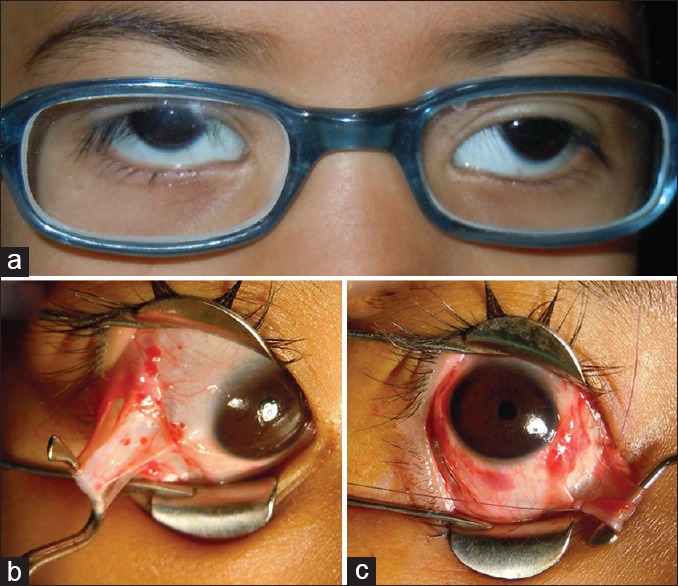
(a) A 7-year-old girl presented with exotropia and limited ocular movements (b) during surgery, the lateral rectus muscle and the (c) medial rectus muscle were dystrophic
Discussion
Absence of the rectus muscles has been reported in literature previously, but the absence of the medial or lateral rectus muscles is rare as usually the vertical recti or obliques are the missing muscles.[4,5] The extraocular muscles develop from the paraxial mesoderm in the orbit.[6] The superior rectus and oblique develop from the superior mesodermal complex and the inferior rectus and inferior oblique develop from the inferior mesodermal complex.[6] The medial and lateral rectus develop from both these complexes.[6] The cause for this anomaly is, however, unknown. The clinical presentation in these cases is complex, variable, and the incomitance is not explainable on clinical examination.
Imaging is useful in identifying these unusual anomalies, especially when the clinical examination of the strabismus does not follow routine patterns.[4] Planning surgery is difficult as there is a risk of anterior segment ischemia. The vertical anterior ciliary artery contribution is more important than the horizontal.[7] Even though the risk of anterior segment ischemia is less in children and the young, in cases with abnormal anatomy, it is not possible to predict the contributions of the anterior ciliary artery circulation. Vertical rectus muscle transposition is an option, but in our patients, superior oblique tendon transfer was performed to minimize this risk of anterior segment ischemia. This procedure has been performed in cases of third nerve palsy where the aim is only tethering of the eye in adduction and improvement of alignment.[8] Resection of the superior oblique tendon was performed to increase the tethering effect and ensure that the eye was placed in adduction on the operating table. Nonabsorbable 5-0 polyester suture was used to prevent chances of slippage of the superior oblique muscle. Good outcome was obtained in terms of alignment of the eyes with good correction of the exotropia. It is important to recognize and anticipate the absence or dystrophy of rectus muscles by performing an imaging. Counseling is a must to match the expectations of the patients as ocular motility cannot be improved with superior oblique tendon transfer. However, this procedure is safe and yields a good outcome in these complex cases.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Greenberg MF, Pollard ZF. Absence of multiple extraocular muscles in craniosynostosis. J AAPOS. 1998;2:307–9. doi: 10.1016/s1091-8531(98)90090-8. [DOI] [PubMed] [Google Scholar]
- 2.Muñoz M. Congenital absence of the inferior rectus muscle. Am J Ophthalmol. 1996;121:327–9. doi: 10.1016/s0002-9394(14)70287-9. [DOI] [PubMed] [Google Scholar]
- 3.Astle WF, Hill VE, Ells AL, Chi NT, Martinovic E. Congenital absence of the inferior rectus muscle – Diagnosis and management. J AAPOS. 2003;7:339–44. doi: 10.1016/s1091-8531(03)00214-3. [DOI] [PubMed] [Google Scholar]
- 4.Sa HS, Kyung SE, Oh SY. Extraocular muscle imaging in complex strabismus. Ophthalmic Surg Lasers Imaging. 2005;36:487–93. [PubMed] [Google Scholar]
- 5.Sandall GS, Morrison JW., Jr Congenital absence of lateral rectus muscle. J Pediatr Ophthalmol Strabismus. 1979;16:35–9. doi: 10.3928/0191-3913-19790101-10. [DOI] [PubMed] [Google Scholar]
- 6.Sevel D. A reappraisal of the origin of human extraocular muscles. Ophthalmology. 1981;88:1330–8. doi: 10.1016/s0161-6420(81)34856-8. [DOI] [PubMed] [Google Scholar]
- 7.Virdi PS, Hayreh SS. Anterior segment ischemia after recession of various recti. An experimental study. Ophthalmology. 1987;94:1258–71. doi: 10.1016/s0161-6420(87)80009-x. [DOI] [PubMed] [Google Scholar]
- 8.Young TL, Conahan BM, Summers CG, Egbert JE. Anterior transposition of the superior oblique tendon in the treatment of oculomotor nerve palsy and its influence on postoperative hypertropia. J Pediatr Ophthalmol Strabismus. 2000;37:149–55. doi: 10.3928/0191-3913-20000501-06. [DOI] [PubMed] [Google Scholar]