

Abstract
Background
Transnasal endoscopy (TNE) is performed with an ultrathin scope via the nasal passages and is increasingly used. This review covers the technical characteristics, tolerability, safety and acceptability of TNE and also diagnostic accuracy, use as a screening tool and therapeutic applications. It includes practical advice from an ear, nose, throat (ENT) specialist to optimise TNE practice, identify ENT pathology and manage complications.
Methods
A Medline search was performed using the terms “transnasal”, “ultrathin”, “small calibre”, “endoscopy”, “EGD” to identify relevant literature.
Results
There is increasing evidence that TNE is better tolerated than standard endoscopy as measured using visual analogue scales, and the main area of discomfort is nasal during insertion of the TN endoscope, which seems remediable with adequate topical anaesthesia. The diagnostic yield has been found to be similar for detection of Barrett's oesophagus, gastric cancer and GORD-associated diseases. There are some potential issues regarding the accuracy of TNE in detecting small early gastric malignant lesions, especially those in the proximal stomach. TNE is feasible and safe in a primary care population and is ideal for screening for upper gastrointestinal pathology. It has an advantage as a diagnostic tool in the elderly and those with multiple comorbidities due to fewer adverse effects on the cardiovascular system. It has significant advantages for therapeutic procedures, especially negotiating upper oesophageal strictures and insertion of nasoenteric feeding tubes.
Conclusions
TNE is well tolerated and a valuable diagnostic tool. Further evidence is required to establish its accuracy for the diagnosis of early and small gastric malignancies. There is an emerging role for TNE in therapeutic endoscopy, which needs further study.
Keywords: ENDOSCOPY, GASTRIC CANCER, BARRETT'S OESOPHAGUS, DIAGNOSTIC AND THERAPEUTIC ENDOSCOPY, OESOPHAGEAL VARICES
A gastrointestinal (GI) endoscopic procedure is the first-line tool for detecting GI pathology. Traditionally oesophagogastroduodenoscopy (OGD) is performed by the transoral route, often with the patient under conscious sedation; only 11% of procedures were performed without sedation in the a previous British Society of Gastroenterology (BSG) audit.1 Compared with local pharyngeal anaesthesia, sedation is associated with substantial cost and requires additional monitoring, nursing staff and a recovery area. Sedation is also associated with some risk; the incidence of cardiopulmonary events is estimated at 0.6%.2
Transnasal endoscopy (TNE) is performed with an ultrathin (UT) endoscope inserted via the nasal passages and is becoming increasingly available. It is performed unsedated so avoids sedation-related complications and there is emerging evidence that it also causes less sympathetic stimulation leading to milder cardiovascular stress.3 By virtue of its route it also reduces pharyngeal stimulation, which may be the reason for its superior tolerability and therefore patient satisfaction (see figure 1).
Figure 1.
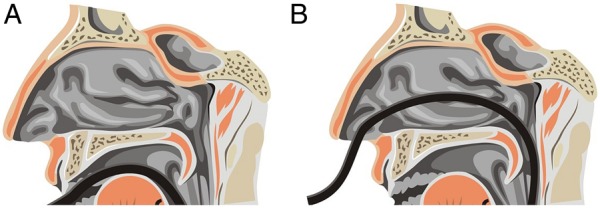
Differences in method of insertion between standard and transnasal approach (diagram courtesy of Dr S Inglis).
Thus, unsedated, TNE is an attractive diagnostic method as it offers efficient and accurate endoscopic assessment of the oesophagus, stomach and duodenum with less cost and fewer risks than sedated upper GI endoscopy.4–14 Its use has dramatically increased in Japan since its introduction, but uptake has been much slower in Europe.15
In this review, we elucidate the technical characteristics, tolerability, safety, side effects and acceptability of this method of upper gastrointestinal (UGI) endoscopy. We will cover the diagnostic accuracy of TNE and its possible use as a screening tool as well as therapeutic applications and future developments. We also offer practical advice including tips from an ear, nose, throat (ENT) specialist to optimise TNE practice.
Technical characteristics
UT endoscopes were initially designed for use in paediatrics and have a shaft diameter of 6 mm or less (range 4.9–6 mm), which allows them to be passed through the nose. They are similar in design to standard endoscopes, although the diameter of the accessory channel is only 2 mm (compared with 2.8 mm in a standard gastroscope) and the working length ranges from 1050 to 1100 mm. Some models, particularly those with the smallest shafts, have two-way (up and down) rather than conventional four-way tip deflection, but with the developments in CCD technology the latest models have not only conventional four-way tip deflection, but also a field of view of 120–140° and image enhancement (flexible spectral imaging colour enhancement (FICE)) capabilities. Due to a smaller working channel, the sizes of biopsy samples obtained with smaller diameter biopsy forceps are smaller (1.8 mm compared with 2.2 mm) but they are of comparable thickness; the smaller size has not been found to significantly affect their diagnostic performance.16 17 The new generation of TNE scopes now available offers a 2.4 mm channel allowing the passage of standard biopsy forceps. There is some evidence that using small diameter biopsy forceps for rapid urease test results in significantly lower positive rates although this can be eliminated by taking two samples, thus increasing the amount of tissue to be tested.17
There are some technical limitations of the UT endoscope; its narrow diameter results in a more floppy scope that can limit advancement especially in patients with unusual or tortuous anatomy, although a complete endoscopy is achieved by experienced users in all but the most complex cases. A smaller working channel also can result in limited suction, less effective screen washing and fewer available endoscopic accessories.
Pretreatment techniques
The technique of unsedated TNE involves the application of topical nasal anaesthesia and is performed with the patient in the upright seated or left lateral decubitus position (as for standard endoscopy). Once topical anaesthesia has been performed, the endoscope is lubricated and passed through the nasal cavity under direct visualisation into the posterior pharynx (see box 1). Once the instrument is beyond the upper oesophageal sphincter, endoscopy is performed in the standard fashion.
Box 1. Ear, nose, throat tips for negotiating the nasopharynx.
Passage through the nose can be disorientating so it is wise to have a set method.
Orientate the nasal passages vertically prior to starting.
Slow and careful passage through the nose should be either below or above the inferior turbinate.
Try and avoid contact with the nasal septum as this is the most sensitive part of the nose.
Ask the patient to breathe through the nose; this will depress the soft palate opening up the nasopharynx and making the correct line of passage more obvious.
TNE is generally recognised as a less painful endoscopic procedure,18–23 but the most commonly reported discomfort is during the nasal insertion phase of the procedure.20 24 Appropriate pretreatment is therefore important, but there are limited data regarding the optimal regimen and technique for reducing discomfort. Shaker published the earliest report on the use of 2% lidocaine gel delivered by a cotton-tipped applicator to perform nasal anaesthesia.25 Endoscopic-guided aerosolised spray (EGAS) has also been used, but in one study using 4% lidocaine nasal spray 33% of patients complained of nasal pain during the prolonged procedure.26–28 Lee recently reported a cotton pledget method of nasal anaesthesia and compared this with EGAS with no significant difference in visual analogue scores for pain during nasal anaesthesia.29 Pain scores during insertion were significantly lower in patients who received the cotton pledget method; they also experienced less throat pain after the examination, less gagging and had better overall tolerance. There were no cases of insertion failure, which may be due to more efficient turbinate shrinkage with this method.30 Topical nasal anaesthesia with local anaesthetic (LA) spray plus LA stick in the nasal cavity plus pharyngeal anaesthesia has been found to cause significantly less pain during insertion of the endoscope.31 There does not appear to be any additional benefit of adding a decongestant such as xylometazoline to topical anaesthetic to reduce discomfort, but does seem to improve nasal insertion and reduce procedure time, likely due to turbinate shrinkage.32 Optimal pretreatment therefore appears to be nasal and pharyngeal anaesthesia plus use of decongestant, which should result in optimum nasal anaesthesia and ease of endoscope passage, resulting in higher likelihood of successful transnasal examination (see boxes 2 and 3).
Box 2. Ear, nose, throat tips for assessing nasal patency.
Occlude one nostril at a time and ask patient to breathe through to see which is more patent.
Use an auroscope with nasal speculum attached to look up nose; this provides a rapid diagnosis of septal deviation, inferior turbinate enlargement or gross nasal polyposis.
It is then possible to ensure the correct nostril is prepared.
Box 3. Our practice for nasal preparation.
Lidocaine hydrochloride 5%, phenylephrine hydrochloride 0.5% spray is applied to both nostrils.
A flexible plastic catheter is then lubricated with 2% lidocaine gel (instillagel) and inserted into one nostril.
For ease of insertion, the patient’s head should be kept in a neutral position and the catheter is inserted aiming straight back towards the back of the head. If any resistance is felt to passage, the process is abandoned and attempted on the other side.
If it is not possible to insert the catheter, the procedure is carried out transorally.
Patient tolerability, side effects and safety
There are several studies comparing tolerance for unsedated TNE and conventional transoral OGD either with or without sedation. The majority of these found better patient tolerance rates in the TNE group based on patient tolerance questionnaires.8 18 20 22 33–36 Patients have greater satisfaction and acceptability4 8 9 20 34–36 and are to be more likely to undergo TNE in the future. They also report a significant reduction in gagging20 37 and in some studies discomfort22 34 (see table 1). One randomised study that reported better overall satisfaction with sedated conventional OGD also reported a significant level of pain during insertion of the endoscope during the transnasal procedure and also had a high failure rate of TNE procedure due to failure to pass through the nasal cavity at 22%.38 One comparative study demonstrated good tolerance of both routes but again found significantly more pain on insertion (1% phenylephrine, 4% lidocaine nasal spray) with TN route.39 Priess et al20 also found significantly more pain on insertion but significantly less gagging and significantly higher patient satisfaction. A recent study evaluating TNE in the elderly (>70 years) found it is safe and well accepted in this group.37
Table 1.
Tolerability of TNE versus conventional OGD
| Study | Outcome measure used | Reported outcome |
|---|---|---|
| Dean et al8 | VAS—choking, discomfort, acceptability | TNE more acceptable (p<0.05) |
| Campo et al18 | VAS—discomfort, retching, pain, tolerance | TNE better tolerated (p<0.05) |
| Dumortier et al21 | VAS—pain, nausea, choking | TNE less choking (p<0.05) |
| Garcia et al4 | VAS—satisfaction | No significant difference |
| Preiss et al20 | VAS—gagging, pain, tolerance | TNE less gagging (p<0.05) |
| Thota et al33 | Tolerance score | No significant difference |
| Murata et al22 | Pain score—tolerance, discomfort | TNE less discomfort (p=0.001) TNE better tolerated (p=0.002) |
| Trevisani et al34 | VAS—pain, discomfort Tolerance score |
TNE better tolerated |
| Zhang et al37 | VAS—pain, discomfort, choking | No significant difference |
| Choe et al67 | VAS—satisfaction and tolerance | TNE better tolerated (p=0.001) |
OGD, oesophagogastroduodenoscopy; TNE, transnasal endoscopy; VAS, visual analogue scale.
A recently published prospective randomised control trial has demonstrated that the high tolerance and acceptability reported mostly in trials from Southeast Asia is also applicable to the UK population.40
Due to the subjective nature of any assessment of patient tolerance and satisfaction, alternative methods for assessing safety and tolerability would be preferable. The assessment of cardiac function and oxygen saturation are both objective methods of evaluating safety and tolerability of endoscopic procedures. Previous studies have shown that TNE causes fewer adverse effects on cardiovascular function than transoral OGD.36 40 41 It is also less stressful to the cardiovascular system with reduced elevation of systolic blood pressure and less sympathetic stimulation than the oral procedure.41 This may well be an important factor as cardiovascular mortality has a significant relationship with autonomic nervous function.
As TNE is performed without sedation, this source of complications is eliminated. Rates of other complications are low and in the largest two series included self-limited epistaxis (0.85–2%) and vasovagal events (0.3%)34 42 A single oesophageal perforation was reported.39 The main difficulty in performing the procedure is the inability to pass the endoscope transnasally due to narrow nasal tracts or altered anatomy in 3–8% of patients,20 34 42 for which there can be multiple reasons (see box 4).
Box 4. Reasons for failure of passage of the endoscope.
Severe septal deviation will prevent passage of the endoscope; however, the opposite side will almost always be patent.
Nasal polyposis; this is relatively common. In gross disease, the patient will have obvious nasal obstruction and for less severe disease where polyps do not reach the nasal floor scope passage should be possible.
There are some rare pathologies that may prevent passage of the endoscope, which include Wegener's granulomatosis, neoplasms, meningoencephalocoeles and choanal atresia.
No definitive guidelines exist for indications or contraindications, but it is not usually performed in those with previous nasal trauma or surgery (although unless this is recent and the introducer is passed without problems, TNE should be possible) or a significant coagulopathy. From an ENT point of view, a history of frequent and problematic epistaxis would be the most likely reason to avoid TNE. In particular, patients with hereditary haemorrhagic telangiectasia (HHT) have delicate nasal mucosa, which will bleed on contact. If the nasal cavity otherwise looks straightforward for TNE passage, there should be no reason to avoid it in patients taking anticoagulants. If epistaxis does occur, this is usually a straightforward complication to manage (see box 5).
Box 5. What to do if epistaxis occurs.
The most frequent site for epistaxis is at Little's area, which is the anterior nasal septum; direct pressure over the lower third of nose for at least 5 min should control the majority of minor bleeds caused by transnasal endoscopy trauma.
For patients whose epistaxis does not settle with pressure, then either a tampon-type pack or a balloon-type pack should be inserted. The key is to insert it along the floor of the nose until the entire pack is within the nasal cavity. The tampon-type pack should be irrigated with 10 mL of water or saline to make it swell. The balloon-type pack should be inflated with air using the pilot balloon as a guide to its internal pressure. Packing can be performed bilaterally if unilateral packs do not control the bleeding.
In the rare event that bleeding is severe, appropriate resuscitation and liaison with ear, nose, throat is indicated.
For patients with minor epistaxis, controlled with pressure, the use of an antibiotic cream may prove beneficial. Naseptin cream (contains chlorhexidine and neomycin) is often prescribed for recurrent minor epistaxis and following nasal cauterisation. It should not be used in patients with peanut allergy. Other options include Bactroban or Vaseline. The cream should be sniffed off the patient's finger into the nostril and rubbed in by pressure from outside the nose. Patients should be warned from causing digital trauma.
Cost effectiveness
TNE has been shown to have shorter procedure times and lower procedure costs due to savings from avoiding sedation and minimising the patient observation period required post procedure.4 43 A shorter procedure means more efficient flow of patients through the endoscopy unit maximising cost efficiency. When TNE is compared with endoscopy under pharyngeal anaesthesia (throat spray), it has higher acceptance, thus less likely for a TNE procedure to fail. Its good safety profile means TNE does not require the presence of two nurses in the endoscopy room; the potential for fewer endoscopy nurses to support a TNE list reduces costs and increases the potential for out-of-hours lists increasing patient convenience and economic benefits resulting from a reduction in time taken out of work for patients.
Diagnostic capability
The diagnostic accuracy of TNE compared with standard gastroscopy has been examined in a variety of scenarios. In previous literature, the diagnostic yield had been found to be similar for the detection of Barrett's oesophagus (BO) and gastric cancer.5 44 45 It has been found to have better performance than oral OGD in the diagnosis of GORD-associated diseases in one paper.46 There has been increasing focus recently on the use of TNE as a screening tool especially for BO and early gastric and oesophageal malignancies. It use is also increasing for screening patients with documented aerodigestive tract tumours for coexisting oesophageal squamous cell carcinomas (SCCs).47 48
With the increasing incidence of oesophageal adenocarcinoma (increased sevenfold over the last 35 years)49 and poor survival rates,50 screening for BO has long been considered. Currently, screening of the general population in the UK is not recommended;51 52 however, the emergence of endoscopic therapies for BO may alter the economic viability of screening. Most previous studies into accuracy of diagnosis of BO with TNE were performed with the aim of looking at the accuracy of detection of any upper GI lesions; they consisted of very small numbers and were inconclusive as to whether smaller endoscope size does limit diagnostic ability.7 10 12 53 54 Only two studies used a randomised design and included BO as a randomised endpoint. Jobe et al5 found only moderate agreement (κ score=0.591); however, a more recent study showed almost perfect agreement between TN and standard OGD (κ score 0.94; 95% CI 0.85 to 1.00).45 It also found that dysplasia was detected by both modalities with similar accuracy.
Gastric cancer
In Japan, up to 60% of gastric cancers are diagnosed as early cancers.55 In Western countries, however, early disease is much less frequently detected accounting for between 10% and 20% of all gastric cancers.56 This difference can be partly explained by the mass screening programme that exists in Japan. It is recognised that there is a miss rate for gastric cancer with standard endoscopy, and false negative rates have been reported to be between 10% and 19%.57 It has also been shown that for those diagnosed with early gastric cancer endoscopically one out of six had had an endoscopy within the previous three years.58 In the UK, a recent abstract suggests that 14% of subjects with gastric cancer have had an endoscopy in the three years prior to their diagnosis.59 Early gastric cancer is not recognised on endoscopy with appearances being thought to be due to benign diagnoses such as inflammation with cancer being found on histology. It is also recognised that fewer years of endoscopic experience had an impact on the diagnosis of early gastric cancer and that early cancers in the gastric cardia, especially the lesser curve or posterior wall, are more likely to be overlooked.60
Various methods have been studied to attempt to improve accuracy of endoscopic diagnosis of gastric cancer with standard endoscopy. Magnifying endoscopy with narrow-band imaging (M-NBI) used in combination with conventional white-light endoscopy results in significantly enhanced performance in diagnostic yield of early gastric cancer when compared with white-light endoscopy alone. M-NBI is especially useful in making an accurate diagnosis from endoscopic findings alone even for small depressed gastric mucosa cancers.61
With regard to the use of TNE for the diagnosis of gastric cancer, the literature has raised some potential concerns especially relating to the accuracy of TNE in detecting small or superficial, gastric malignant lesions.5 34 50 An initial paper comparing the detection rate of early gastric cancer and adenoma with TNE and transoral endoscopy found no significant differences in diagnosis.44
Subsequent publications have revealed opposing findings. One paper62 looking at the performance of UT endoscopy for the diagnosis of superficial gastric neoplasia shows that the diagnostic accuracy for superficial gastric neoplasia is significantly lower for UT endoscopy than for high-resolution standard endoscopy with 25% of gastric neoplasia being missed by UT endoscopy.
A second paper looking at use of TNE in screening for early gastric cancer63 suggested that the diagnostic utility of UT endoscopy was inadequate for the diagnosis of early gastric cancer lesions (<20 mm), especially those located in the upper third of the stomach; the suggested explanation for this was lower resolution and lower light intensity of the UT scope. The authors also suggested that the diagnostic utility of UT endoscopy can be improved by indigo carmine dye spraying. Both trials included small numbers of patients, but both indicate that the location of pathology is important, with UT endoscopy being more likely to miss early pathology in the proximal stomach but no significant difference in the pick-up rate for pathology in the distal stomach. These studies only studied UT endoscopy with white light. In contrast, excellent detection rates for oesophageal and gastric cancers have previously been reported when using UT endoscopy in combination with chromoendoscopy using indigo carmine and iodine.64 It has also been suggested that if image enhancing techniques such as NBI (or FICE) can be applied through a UT endoscope, this may be useful in improving the detection of oesophageal premalignant lesions.65 This is now possible with the latest series of UT scopes.
In Asian populations, there have been two studies looking at the use of TNE to screen patients with head and neck cancers for oesophageal SCCs. One study looked at the yield of this procedure and found that 10% of patients had oesophageal SCC diagnosed by TNE and 7.3% had lesions with high-grade dysplasis. They used both NBI and Lugol chromoendoscopy and showed an increased pick-up rate when both NBI and Lugol chromoendoscopy were used compared with white light alone. Aiming for lesions that appeared brownish under NBI or unstained under Lugol chromoendoscopy had the highest sensitivity.47
A study on a similar patient population but comparing white endoscopy with FICE and Lugol staining did not show a significant difference between the two methods and diagnosed 12.5% of patients with oesophageal SCC.48
Oesophageal varices
TNE has been used to screen for oesophageal varices in patients with cirrhosis, the detection and grading of varices being equivalent to standard OGD in two papers66 67 Saeian et al66 included only 15 patients, those with a platelet count of <50 000 mm3 were excluded and epistaxis rate was 6%. Choe et al67 randomised 89 patients and had excellent concordance rates (κ score=0.87). They reported an epistaxis rate of 6%, and 28 patients had an international normalised ratio of 1.7–2.3 and platelets between 20 000 and 50 000 mm3; this group had an epistaxis rate of 14%. Concerns exist about performing TNE in patients with a coagulopathy, and this may be one of the reasons why TNE has not been adequately assessed as a screening tool for varices.
Diagnosis of ENT pathology
Infrequently, coincidental pathology may be noted within the upper aerodigestive system, so it is reasonable to expect TNE practitioners to have some knowledge of common ENT pathologies and pathways of management. Findings such as simple nasal polyps (see figure 2) would be appropriate to bring to the attention of the patient and inform them to consult their general practitioner. Suspected malignancies would require urgent referral to ENT. Common sites for aerodigestive tumours to be found with TNE are within the nose, larynx and hypopharynx (see figures 3 and 4); however, due to the swallowing motion required to aid passage of the TN scope, TNE is not an appropriate investigation for these areas as small pathology is likely to be missed. Also, tumours within the oropharynx are unlikely to be visualised. Nasal masses that look anything other than benign polyps warrant urgent ENT referral and likewise any suspicion of laryngeal and hypopharyngeal tumours. Laryngeal pathology is varied but is likely to ultimately require biopsy to confirm a diagnosis.
Figure 2.
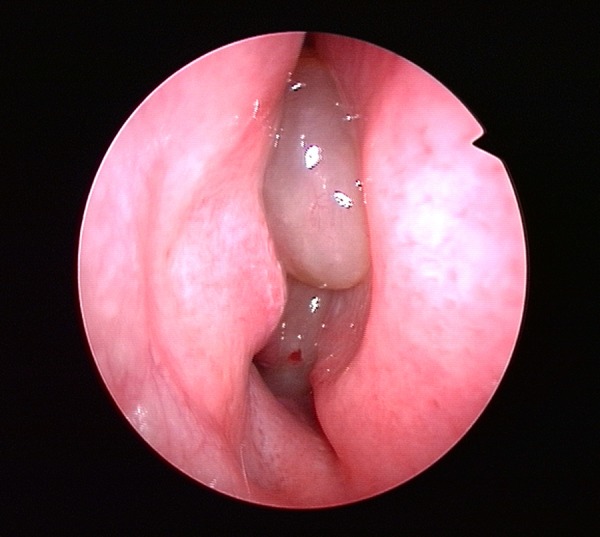
Rigid endoscope showing benign polyps within the right nasal cavity.
Figure 3.
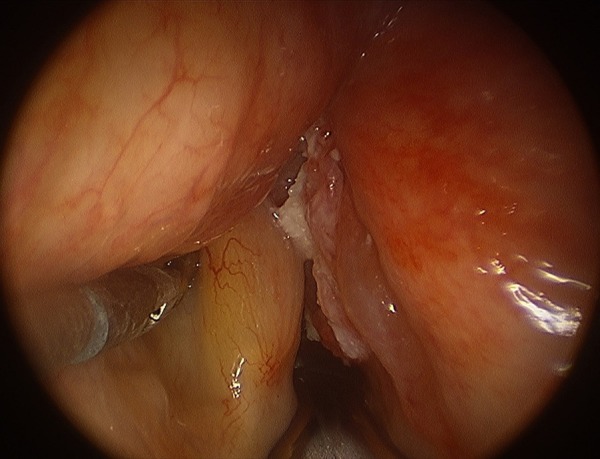
Right-sided glottic squamous carcinoma (viewed under general anaesthesia with rigid laryngoscope).
Figure 4.
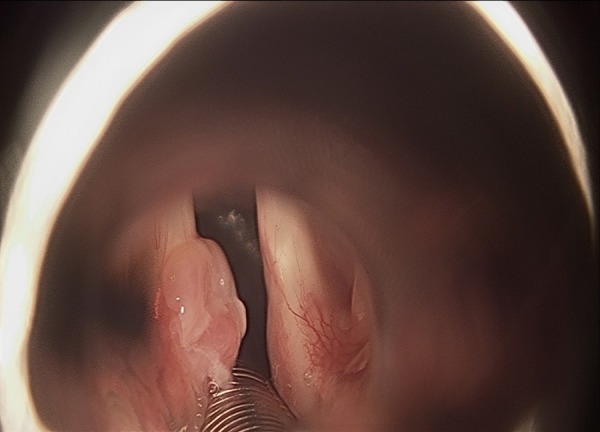
Left-sided glottic granuloma (viewed under general anaesthesia with rigid laryngoscope).
Feasibility and safety in the primary care population
A recent paper from 2012 demonstrated the feasibility and safety of TNE in a primary care population, achieving short procedure times, a high diagnostic yield and minimal anxiety. The findings suggested that TNE has a similar ability to standard OGD to identify upper GI pathology in this population, strengthening argument for its consideration for use as screening tool in the primary care population.68 The significant improvement of optics and field of view (from 120° to 140° similar to standard endoscopes) (see figures 5 and 6) of newer TNE endoscopes will most certainly reduce the probability of missing pathology compared with standard endoscopy, although comparative studies are necessary to confirm this in the future.
Figure 5.
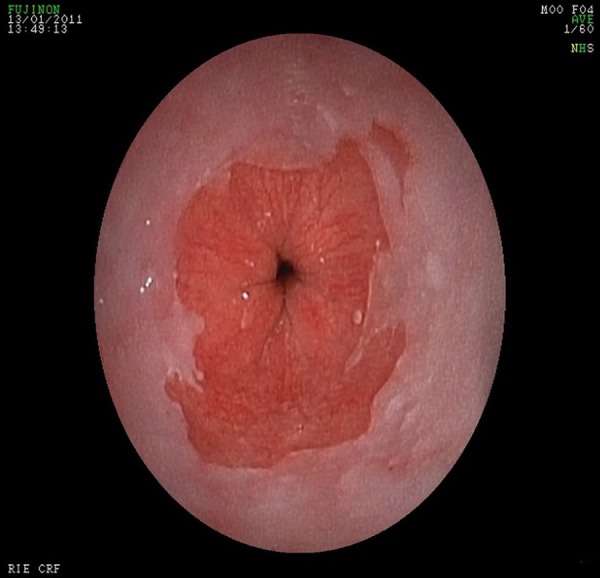
View of oesophagogastric junction for transnasal endoscopy.
Figure 6.
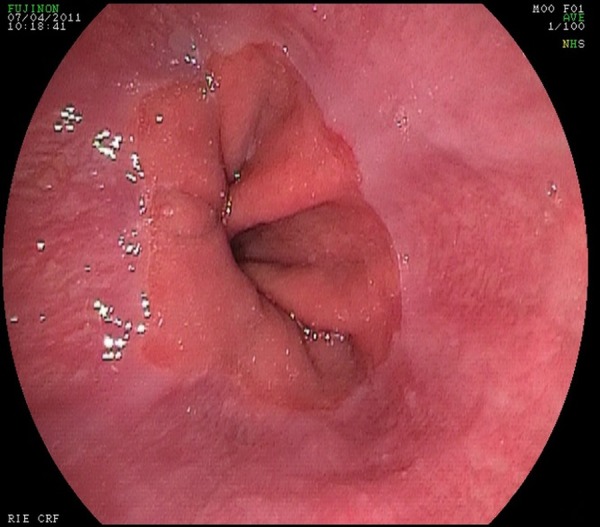
View of oesophagogastric junction for standard endoscopy.
Therapeutic applications of TNE
There is increasing literature on the use of UT scopes for various therapeutic indications including, most commonly, the insertion of feeding tubes. More recently, UT scopes have been used in the treatment of GI strictures (where the small diameter of the scope aids in the placement of a wire across the stricture) and to assist advanced endoscopic techniques such as endoscopic submucosal dissection (ESD) and endoscopic retrograde cholangiopancreatography (ERCP).
Insertion of NET/PEG tubes
TNE is ideal for the placement of nasoenteral feeding tubes (NET), especially nasojejunal (NJ) tubes (see box 6). It was first used to place NET in critically ill patients;69 its main benefits in this group are no requirement for additional sedation, ability to perform the procedure at the bedside and no radiation exposure compared with fluoroscopy-assisted insertions. In direct comparison to transoral endoscopic placement, TN placement is significantly faster and causes fewer cardiorespiratory complications.69
Box 6. Insertion of nasojejunal (NJ) tube with transnasal endoscopy (TNE).
TNE is performed in the usual manner.
A guidewire is then inserted under direct vision into the duodenum and advanced as far as possible into the small bowel as with standard technique for insertion of NJ tubes.
The endoscope is withdrawn, leaving the wire in situ and the NJ tube placed over the wire. In our experience, this makes the technique simpler with no awkward fiddling with the wire at the back of the mouth.
Post-pyloric placement of the feeding tube is then confirmed endoscopically. A thinner endoscope also seems to reduce the likelihood of pulling the feeding tube back as the endoscope is withdrawn.
When compared with fluoroscopic insertion in critically ill or severe pancreatitis patients, TN placement has equal success rates with a significantly shorter procedure time and less patient discomfort.70 71 It has been shown that using an endoscope with a longer working length 92 vs 133 cm significantly improves success rates of insertion of NET.72 TNE is very helpful in the placement of NET in a range of upper GI diseases such as malignant strictures, gastric outlet obstruction and gastroparesis,73 as well as nasogastric tube placement in patients with oesophageal cancer.74
TNE has also been used successfully for the insertion of percutaneous endoscopic gastrostomy (PEG) tubes (the bumper is compressed and then passed through the nose) and has a potentially important role due to less sedation requirements and less cardiovascular stress in patients likely to have significant comorbidities. However, further studies are necessary to establish its role and potential advantages over transoral PEG placement.75 Currently, TNE-assisted PEG insertions have been reserved for patients whom conventional PEG placement is difficult such as in cases of GI strictures or trismus (inability to fully open mouth).76
Management of upper GI strictures
UT scopes have been used in patients with upper GI strictures and can successfully traverse >80% of such strictures, resulting in higher endoscopy completion rates in such patients and enabling full characterisation of the stricture (diameter, length and enabling biopsies for histological diagnosis). Dilatation of such strictures can be done safely as endoscopic placement of a guidewire is possible in most cases via an UT endoscope even in tight strictures without the need for fluoroscopy.77 This is in line with the BSG guidelines that recommend using a wire-guided technique for performing oesophageal dilatations.78 Using the UT scope to place the wire reduces the numbers of repeat procedures and reduces the need for radiology support, therefore potentially reducing costs, and so on.
ESD is increasingly used for the treatment of early gastric cancer; however, difficulties can be encountered due to the location of the lesion. TNE has been used to enable easier access to lesions extending into the antrum/pylorus or duodenal bulb wherein the TN scope is used as an assistant scope to enable adequate retraction of tissue to allow en bloc resection.79 80 Transnasal scopes have also been used to perform ERCP; however, biliary cannulation has been found to be more difficult and the size of the channel will limit the availability of therapeutic accessories.81
Limitations of TNE
The thinner diameter of the TNE scope also produces limitations as well as benefits; it is more likely to be damaged than a standard endoscope. Due to its narrower channel and lesser washing and suction, there are limits to both visibility and available therapeutic accessories, which means its use is limited as a therapeutic tool, especially in the context of upper GI bleeding.
Conclusion
Although TNE has been available for more than a decade, the technique is widely used in Japan, but its use is variable in Europe and there are very little data on the extent of its use in the UK. It has been suggested from a previous European survey that reasons for reluctance in use are concerns about diagnostic accuracy and histological sampling as well as lack of training.82 There is an increasing body of evidence that TNE is a better tolerated procedure compared with standard endoscopy per os, and the main area of discomfort is nasal pain during insertion of the TNE endoscope, which seems remediable with adequate nasal and pharyngeal topical anaesthesia.
There are three areas where TNE has clear advantage compared with standard OGD:
its use as a screening tool for GI pathology;
first-line use as a diagnostic tool in the elderly and those with multiple comorbidities especially cardiovascular disease;
therapeutic procedures especially negotiating upper oesophageal strictures and for the insertion of nasoenteric feeding tubes.
The tolerability and cost effectiveness in comparison to oral OGD in a primary care population have been demonstrated. TNE is an ideal tool for screening and surveillance for UGI pathology such as Barrett's (in the Western world) or gastric cancer (in the East).
As discussed previously, there are miss rates for early gastric cancer with standard endoscopy and certainly there have been concerns raised from the literature about the use of TNE, especially in the diagnosis of early gastric cancer.
There are ways in which the technique of TNE may be enhanced to improve the pick-up of early gastric cancer. Adequate preparation of the gastric mucosa to ensure views are not impaired by mucus especially in TNE where views can potentially be a problem due to reduced suction; asking patients to drink a mucolytic and defoaming agent may be of use to improve views. During the procedure, meticulous examination of the gastric mucosa is required. Adequate insufflation is vital to ensure that all the gastric mucosa can be adequately visualised. To ensure all of the mucosa has been examined especially in the ‘high-risk’ miss areas, that is, the proximal stomach, the introduction of a technique to ‘map’ the entire stomach as has been developed in Japan83 may be helpful. This includes photomapping and requires multiple photographs to be taken; however, a variation of this from the European Society of Gastrointestinal Endoscopy requires only eight photographs and may be a more practical approach to adopt.84 There should be consideration given to procedure time as it has been established that endoscopists who have longer procedure times and take more than four pictures detect more pathology than those with shorter procedure times who take fewer pictures.85 Perhaps the consideration of a withdrawal time as for colonoscopy should be considered. That TNE is better tolerated makes it an ideal tool to ensure meticulous examination as longer procedures will be better tolerated. When abnormal areas are discovered, the use of indigo carmine and NBI may be helpful in characterising them. Many of the ways in which pick-up rates of early gastric cancer may be improved can be applied to both TNE and conventional upper GI endoscopy.
Further evidence is still required to establish the accuracy for TNE for the diagnosis of early and small gastric malignancies and ideally these would be studies performed in Western populations. Another factor that needs to be considered is the continuing evolution of technology with the availability of new endoscopes. These endoscopes now have an increased field of view at 140°, superior image quality and the routine use of image enhancing techniques such as NBI or FICE, as well as chromoendoscopy. They also have better suction and water jet and an increased size of biopsy channel. These technical improvements as well as changes in technique of examination should almost certainly help to improve the diagnostic accuracy of TNE for early gastric malignancies.
TNE can certainly be used in the diagnosis of oesophageal varices, although there are limited studies at present. Given the increasing incidence of chronic liver disease, TNE is a useful modality for variceal screening. More guidance regarding absolute contraindications with regard to levels of coagulopathy acceptable for performing TNE is currently lacking; it would be seen from ENT practice (although the ENT scope is thinner) that unless there is a history of recurrent epistaxis or HHT there is no reason for anticoagulation to be an absolute contraindication to TNE.
TNE has benefit in terms of cardiovascular stress, which translates to great advantages in patients with multiple comorbidities, particularly pre-existing cardiorespiratory disease, and in the elderly. There is also an emerging role for TNE in therapeutic endoscopy. Such use needs further study and development of appropriate accessories to increase its therapeutic potential. It is expected that the latest generation of TNE scopes in addition to better image definition and colour enhancement may also accommodate a larger biopsy channel (2.2 mm), which will increase the therapeutic ability of such scopes.
The reason for preventing widespread use of TNE may be the lack of formal training and accreditation for this technique in the UK, which may also contribute to the reluctance to use this technique.86 This raises the question of how endoscopists should be trained in the use of TNE. The authors would suggest the development of dedicated TNE training as part of existing upper GI basic skills courses or as a stand-alone course. ENT specialists should be involved to emphasise the important aspects of the anatomy of the nasopharynx and recognition of common but significant nasopharyngeal pathology, and finally, to advise on how to achieve successful nasal intubation as well as guidance on managing nasal complications. Guidelines for training and accreditation, as exist for standard endoscopy, should be developed for TNE.
Footnotes
Contributors: CP performed the literature review, gathered and reviewed the relevant literature and wrote the paper. EA assisted in writing the paper. JP supervised the work and assisted with writing and review of the paper. JO provided images and expertise for the ENT parts of the paper. SP supervised the work and assisted in writing and review of the paper.
Competing interests: CP was in an endoscopy fellow post financially supported by Imotech Medical UK. EA's previous fellowship and trial in Transnasal Endoscopy was supported by Fujifilm/Imotech Medical UK. JP was principal investigator for transnasal trial previously financially supported by Fujifil/Imotech Medical UK. SP is supervisor to endoscopy fellowship financially supported by Imotech Medical UK. JO, JP and SP have taught on TNE course supported by Imotech Medical UK.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Quine MA, Bell GD, McCloy RF, et al. . Prospective audit of upper gastrointestinal endoscopy in two regions of England: safety, staffing and sedation methods. Gut 1995;36:462–7. doi:10.1136/gut.36.3.462 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sharma VK, Nguyen CC, Crowell MD. A national study of cardiopulmonary unplanned events after GI endoscopy. Gastrointest Endosc 2007;66:27–34. doi:10.1016/j.gie.2006.12.040 [DOI] [PubMed] [Google Scholar]
- 3.Mori A, Ohashi N, Tatebe H. Autonomic nervous function in upper GI endoscopy: a prospective randomised comparison between transnasal and oral procedures. J Gastroenterol 2008;43:38–44. doi:10.1007/s00535-007-2124-y [DOI] [PubMed] [Google Scholar]
- 4.Garcia RT, Cello JP, Nguyen MH. Unsedated ultrathin EGD is well accepted when compared with conventional sedated EGD: a multicentre randomised trial. Gastroenterology 2003;125:1606–12. doi:10.1053/j.gastro.2003.08.034 [DOI] [PubMed] [Google Scholar]
- 5.Jobe BA, Hunter JG, Chang EY. Office-based unsedated small caliber endoscopy is equivalent to conventional sedated endoscopy in screening and sureveillance for Barretts esophagus: a randomised and blinded comparison. Am J Gastroenterol 2006;101:2693–703. doi:10.1111/j.1572-0241.2006.00890.x [DOI] [PubMed] [Google Scholar]
- 6.Saeian K, Staff DM, Vasilopoulos S. Unsedated transnasal endoscopy accurately detects Barretts metaplasia and dysplasia. Gastrointest Endosc 2002;56:472–8. doi:10.1016/S0016-5107(02)70429-X [DOI] [PubMed] [Google Scholar]
- 7.Mokhashi MS, Wildi SM, Glenn TF. A prospective, blinded study of diagnostic esophagoscopy with a superthin, stand-alone, batterypowered esophagoscope. Am J Gastroenterol 2003;98:2383–9. doi:10.1111/j.1572-0241.2003.08701.x [DOI] [PubMed] [Google Scholar]
- 8.Dean R, Dua K, Massey B. A comparative study of unsedated transnasal esophagogastroduodenoscopy and conventional EGD. Gastrointest Endosc 1996;44:422–4. doi:10.1016/S0016-5107(96)70092-5 [DOI] [PubMed] [Google Scholar]
- 9.Mori A, Ohashi N, Yoshida A. Unsedated transnasal esophagogastroduodenoscopy may provide better diagnostic performance on gastroesophageal reflux disease. Dis Esophagus 2011;24:92–8. doi:10.1111/j.1442-2050.2010.01098.x [DOI] [PubMed] [Google Scholar]
- 10.Catanzaro A, Faulx A, Pfau PR. Accuracy of a narrow-diameter battery-powered endoscope in sedated and unsedated patients. Gastrointest Endosc 2002;55:484–7. doi:10.1067/mge.2002.122576 [DOI] [PubMed] [Google Scholar]
- 11.Faulx AL, Catanzaro A, Zyzanski S. Patient tolerance and acceptance of unsedated ultrathin esophagoscopy. Gastrointest Endosc 2002;55:620–3. doi:10.1067/mge.2002.123274 [DOI] [PubMed] [Google Scholar]
- 12.Catanzaro A, Faulx A, Isenberg GA. Prospective evaluation of 4 mm diameter endoscopes for esophagoscopy in sedated and unsedated patients. Gastrointest Endosc 2003;57:300–4. doi:10.1067/mge.2003.113 [DOI] [PubMed] [Google Scholar]
- 13.Faulx A, Vela S, Das A. The changing landscape of practice patterns regarding unsedated endoscopy and propofol use: a national web survey. Gastrointest Endosc 2005;62:9–15. doi:10.1016/S0016-5107(05)00518-3 [DOI] [PubMed] [Google Scholar]
- 14.Boolchand V, Faulx A, Das A. Primary care physician attitudes toward endoscopic screening for GORD symptoms and unsedated esophagoscopy. Gastrointest Endosc 2006;63:228–33. doi:10.1016/j.gie.2005.06.044 [DOI] [PubMed] [Google Scholar]
- 15.Tatsumi Y, Harada A, Matsumoto T. Current status and evaluation of transnasal esophagogastroduodenoscopy. Dig Endosc 2009;21:141–6. doi:10.1111/j.1443-1661.2009.00891.x [DOI] [PubMed] [Google Scholar]
- 16.Walter T, Chesnay AL, Dumortier J. Biopsy specimens obtained with small caliber endoscopes have comparable diagnostic performances than those obtained with conventional endoscopes: a prospective study on 1335 specimens. J Clin Gastroenterol 2010;44:12–17. doi:10.1097/MCG.0b013e3181a1bebd [DOI] [PubMed] [Google Scholar]
- 17.Jeon SJ, Shin SJ, Lee KM. Can the 1.8 mm transnasal biopsy forceps instead of standard 2.2 mm alter rapid urease test and histological diagnosis?. J Gastroenterol Hepatol 2012;27:1384–7. doi:10.1111/j.1440-1746.2012.07152.x [DOI] [PubMed] [Google Scholar]
- 18.Campo R, Monserrat A, Brullet E. Transnasal gastroscopy compared to conventional gastroscopy: a randomised study of feasibility, safety and tolerance. Endoscopy 1998;30:448–52. doi:10.1055/s-2007-1001306 [DOI] [PubMed] [Google Scholar]
- 19.Miyawaki T, Nose M, Kouzu T. Transnasal upper GI endoscopy: safe and painless examination. Endosc Dig 2007;19:529–35. [Google Scholar]
- 20.Preiss C, Charlton JP, Schumacher B, et al. . A randomised trial of unsedated transnasal small caliber EGD versus peroral small-caliber EGD versus conventional EGD. Endoscopy 2003;35:641–6. doi:10.1055/s-2003-41513 [DOI] [PubMed] [Google Scholar]
- 21.Dumortier J, Ponchon T, Scoazec JY. Prospective evaluation of transnasal oesophagogastroduodenoscopy: feasibility and study on performance and tolerance. Gastrointest Endosc 1999;49:285–91. doi:10.1016/S0016-5107(99)70002-7 [DOI] [PubMed] [Google Scholar]
- 22.Murata A, Akahori K, Sumida Y. Prospective randomised trial of transnasal versus peroral endoscopy using ultrathin videoendoscope in unsedated patients. J Gastroenterol Hepatol 2007;22:482–5. doi:10.1111/j.1440-1746.2006.04730.x [DOI] [PubMed] [Google Scholar]
- 23.Yagi J, Adachi K, Arima N. A prospective comparative study on the safety and tolerability of transnasal EGD. Endoscopy 2005;37:1226–31. doi:10.1055/s-2005-921037 [DOI] [PubMed] [Google Scholar]
- 24.Cheung J, Bailey R, Veldhuyzen van Zanten S, et al. . Early experience with unsedated ultrathin 4.9 mm transnasal gastroscopy: a pilot study. Can J Gastroenterol 2008;22:917–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Shaker R. Unsedated trans-nasal pharyngoesophagogastroduodenoscopy (T-EGD) technique. Gastrointest Endosc 1994;40:346–8. doi:10.1016/S0016-5107(94)70068-0 [DOI] [PubMed] [Google Scholar]
- 26.Hu CT. Endoscopic guided versus cotton tipped applicator methods of nasal anaesthesia for transnasal EGD: a randomised, prospective controlled study. Am J Gastroenterol 2008;103:1114–21. doi:10.1111/j.1572-0241.2007.01769.x [DOI] [PubMed] [Google Scholar]
- 27.Maffei M, Dumonceau JM. Endoscopic guided versus cotton tipped applicator methods of nasal anaesthesia for transnasal EGD. Am J Gastroenterol 2008;103:3209; author reply 3209–10 doi:10.1111/j.1572-0241.2008.02161_8.x [DOI] [PubMed] [Google Scholar]
- 28.Itoi T, Kawai T, Sofuni A. Efficacy and safety of one-step transnasal endoscopic nasobiliary drainage for treatment of acute cholangitis in patients with previous endoscopic sphincterotomy. Gastrointest Endosc 2008;68:84–90. doi:10.1016/j.gie.2007.11.050 [DOI] [PubMed] [Google Scholar]
- 29.Lee YC, Wang CP. Cotton pledget method for nasal decongestive anaesthesia prior to transnasal endoscopy. Am J Gastroenterol 2008;103:3212–13. doi:10.1111/j.1572-0241.2008.02161_12.x [DOI] [PubMed] [Google Scholar]
- 30.Hu CT. Gauze pledgeting versus endoscopic-guided aerosolised spray for nasal anaesthesia before transnasal EGD: a prospective, randomised study. Gastrointest Endosc 2010;71:11–20. doi:10.1016/j.gie.2009.06.016 [DOI] [PubMed] [Google Scholar]
- 31.Iwamoto J, Mizokami Y, Shimokobe K. Pretreatment methods in transnasal endoscopy. Hepatogastroenterology 2011;58:842–5. [PubMed] [Google Scholar]
- 32.Cheung J, Goodman KJ, Veldhuyzen van Zanten S. CANHelp working group, a randomised trial of topical anaesthesia comparing lidocaine versus lidocaine plus xylometazoline for unsedated transnasal upper gastrointestinal endoscopy. Can J Gastroenterol 2010;24:317–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Thota PN, Zuccaro G, Vargo JJ. A randomised prospective trial comparing unsedated esophagoscopy via transnasal and transoral routes using a 4 mm video endoscope with conventional endoscopy with sedation. Endoscopy 2005;37:559–65. doi:10.1055/s-2005-861476 [DOI] [PubMed] [Google Scholar]
- 34.Trevisani L, Cifala V, Sartori S. Unsedated ultrathin upper endoscopy is better than conventional endoscopy in routine outpatient gastroenterology practice: a randomised trial. World J Gastroenterol 2007;13:906–11. doi:10.3748/wjg.v13.i6.906 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Stroppa I, Grasso E, Paoluzi O. Unsedated transnasal versus transoral sedated upper gastrointestinal endsocopy: a one-series prospective study on safety and patient acceptability. Dig Liver Dis 2008;40:767–75. doi:10.1016/j.dld.2008.02.033 [DOI] [PubMed] [Google Scholar]
- 36.Mori A, Ohashi N, Maruyama T, et al. . Cardiovascular tolerance in upper GI endoscopy using an ultrathin scope: prospective randomised comparison between transnasal and transoral procedures. Dig Endosc 2008;20:79–83. doi:10.1111/j.1443-1661.2008.00780.x [Google Scholar]
- 37.Zhang Q, Xioa AH, Tan XP. Ultrathin transnasal esophagogastroduodenoscopy in geriatric patients: a prospective evauation. Int J Gerontol 2011:217–21. doi:10.1016/j.ijge.2011.09.024 [Google Scholar]
- 38.Birkner B, Fritz N, Schatke W. A prospective randomised comparison of unsedated ultrathin versus standard esophagogastricduodenoscopy in routine outpatient gastroenterology practice: does it work better through the nose? Endoscopy 2003;35:647–51. doi:10.1055/s-2003-41523 [DOI] [PubMed] [Google Scholar]
- 39.Zaman A, Hahn M, Hapke R. A randomised trial of peroral versus transnasal unsedated endoscopy using an ultrathin videoendoscope. Gastrointest Endosc 1999;49:279–84. doi:10.1016/S0016-5107(99)70001-5 [DOI] [PubMed] [Google Scholar]
- 40.Alexandridis E, Inglis S, McAvoy NC, et al. . Randomised clinical study: comparison of acceptability, patient tolerance, cardiac stress and endoscopic views in transnasal and transoral endoscopy under local anaesthetic. Aliment Pharmacol Ther 2014;40:467–76. [DOI] [PubMed] [Google Scholar]
- 41.Mori A, Fushimi N, Asano T. Cardiovascular tolerance in unsedated upper GI endoscopy: prospective randomised comparison between transnasal and conventional oral procedures. Dig Endosc 2006;18:282–7. doi:10.1111/j.1443-1661.2006.00656.x [Google Scholar]
- 42.Dumortier J, Napoleon B, Hedelius F. Unsedated transnasal EGD in daily practice: results with 1100 consecutive patients. Gastrointest Endosc 2003;57:198–204. doi:10.1067/mge.2003.59 [DOI] [PubMed] [Google Scholar]
- 43.Gorelick AB, Inadomi JM, Barnett JL. Unsedated small caliber esophagogastroduodenoscopy (EGD): less expensive and less time consuming than conventional EGD. J Clin Gastroenterol 2001;33:210–14. doi:10.1097/00004836-200109000-00008 [DOI] [PubMed] [Google Scholar]
- 44.Yoshida Y, Hayami Y, Matuoka M. Comparison of detection rate of early gastric cancer and gastric adenoma using transnasal EGD and that of transoral EGD. Dig Endosc 2008;20:184–9. doi:10.1111/j.1443-1661.2008.00804.x [Google Scholar]
- 45.Shariff MK, Bird-Lieberman EL, O'Donovan M. Randomised crossover study comparing the efficacy of transnasal endoscopy with that of standard endoscopy to detect Barretts esophagus. Gastrointest Endosc 2012;75:954–61. doi:10.1016/j.gie.2012.01.029 [DOI] [PubMed] [Google Scholar]
- 46.Mori A, Ohashi N, Yoshida A. Unsedated transnasal ultrathin esophagogastroduodenoscopy may provide better diagnostic performance on gastroesophgeal reflux disease. Dis Esophagus 2011;24:92–8. [DOI] [PubMed] [Google Scholar]
- 47.Wang CH, Lee YC, Wang CP. Use of transnasal endoscopy for screening of esophageal squamous cell carcinoma in high risk patients: yield, completion rate and safety. Dig Endosc 2014;26:24–31. doi:10.1111/den.12053 [DOI] [PubMed] [Google Scholar]
- 48.Arantes V, Albuquerque W, Salles JM. Effectiveness of unsedated transnasal endoscopy with white light flexible spectral imaging and color enhancement and lugol staining for esophageal cancer screening in high risk patients. J Clin Gastroenterol 2013;47:314–21. doi:10.1097/MCG.0b013e3182617fc1 [DOI] [PubMed] [Google Scholar]
- 49.Pohl H, Sirovich B, Welsh HG. Esophgeal adenocarcinoma incidence: Are we reaching the peak? Cancer Epidemiol Biomarkers Prev 2010;19:1468–70. doi:10.1158/1055-9965.EPI-10-0012 [DOI] [PubMed] [Google Scholar]
- 50.Eloubeidi MA, Mason AC, Desmond RA. Temporal trends in survival of patients with esophageal adenocarcinoma in the US: a glimmer of hope? Am J Gastroenterol 2003;98:1627–33. [DOI] [PubMed] [Google Scholar]
- 51.Fitzgerald RC, Di Pietro M, Ragunath K, et al. . BSG guidelines of the diagnosis and management of Barretts oesophagus. Gut 2014;63:7–42. doi:10.1136/gutjnl-2013-305372 [DOI] [PubMed] [Google Scholar]
- 52.Wang KK, Sampliner RE. Updated guidelines 2008 for the diagnosis, surveillance and therapy of Barretts oesophagus. Gastroenterology 2011;140:1084–91. doi:10.1053/j.gastro.2011.01.030 [DOI] [PubMed] [Google Scholar]
- 53.Sorbi D, Gostout CJ, Henry J. Unsedated small calibre oesophagogastricduodenoscopy (EGD) versus conventional EGD: a comparative study. Gastroenterology 1999;117:1301–7. doi:10.1016/S0016-5085(99)70280-5 [DOI] [PubMed] [Google Scholar]
- 54.Wildi SM, Wallace MB, Glenn TF. Accuracy of esophagoscopy performed by a non-physician endoscopist with a 4 mm diameter battery-powered endoscope. Gastrointest Endosc 2002;56:472–8. [DOI] [PubMed] [Google Scholar]
- 55.Hisamichi S. Screening for gastric cancer. World J Surg 1989;13:31–7. doi:10.1007/BF01671151 [DOI] [PubMed] [Google Scholar]
- 56.Sue-Ling HM, Martin I, Griffith J, et al. . Early gastric cancer: 46 cases in one surgical department. Gut 1992;33:1318–22. doi:10.1136/gut.33.10.1318 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Hosokawa O, Tsuda S, Kidani E. Diagnosis of gastric cancer up to 3 years after negative upper gastrointestinal endoscopy. Endoscopy 1998;30:669–74. doi:10.1055/s-2007-1001386 [DOI] [PubMed] [Google Scholar]
- 58.Suvakovic Z, Bramble MG, Jones R, et al. . Improving the detection rate of early gastric cancer requires more than open access gastroscopy: a five year study. Gut 1997;41:308–13. doi:10.1136/gut.41.3.308 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Menon S, Dhar A, Hoare J, et al. . How commonly is gastric cancer missed at endoscopy: a UK primary care based study. Gut 2012;61:A43 doi:10.1136/gutjnl-2012-302514a.98 [Google Scholar]
- 60.Ren W, Yu J, Wang L. Missed diagnosis of early gastric cancer or high grade intraepithelial neoplasia. World J Gastroenterol 2013;19:2092–6. doi:10.3748/wjg.v19.i13.2092 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Ezoe Y, Muto M, Uedo N. Magnifying narrowband imaging is more accurate than conventional white-light imaging in diagnosis of gastric mucosal cancer. Gastroenterology 2011;141:2017–25. doi:10.1053/j.gastro.2011.08.007 [DOI] [PubMed] [Google Scholar]
- 62.Toyoizumi H, Kaise M, Arakawwa H. Ultrathin endoscopy versus high-resolution endoscopy for diagnosing superficial gastric neoplasia. Gastrointest Endosc 2009;70:240–5. doi:10.1016/j.gie.2008.10.064 [DOI] [PubMed] [Google Scholar]
- 63.Hayashi Y, Yamamoto Y, Suganuma T. Comparison of the diagnostic utility of teh ultrathin endoscope and the conventional endoscope in early gastric cancer screening. Dig Endosc 2009;21:116–21. doi:10.1111/j.1443-1661.2009.00840.x [DOI] [PubMed] [Google Scholar]
- 64.Kawai T, Yamagishi T, Moriyasu. Diagnosis of esophageal and gastric carcinoma using ultrathin esophagogastricduodenoscopy. In: Niwa, Tajiri, Nakajima, Yasuda, eds. New Challen in Gastrointestinal Endoscopy. Springer, 2008:79–86. [Google Scholar]
- 65.Kawai T, Takagi Y, Yamamoto K. Narrow-band imaging on screening of esophgeal lesions using an ultrathin transnasal endoscopy. J Gastroenterol Hepatol 2012;27:34–9. doi:10.1111/j.1440-1746.2012.07068.x [DOI] [PubMed] [Google Scholar]
- 66.Saeian K, Staff DM, Knox J. Unsedated transnasal endoscopy: a new technique for accurately detecting and grading esophageal varices in cirrhotic patients. Am J Gastroenterol 2002;97:2246–9. doi:10.1111/j.1572-0241.2002.05906.x [DOI] [PubMed] [Google Scholar]
- 67.Choe WH, Kim JH, Ko SY. Comparison of transnasal small-caliber versus peroral conventional esophagogastricduodenoscopy for evaluating varices in unsedated cirrhotic patients. Endoscopy 2011;43:649–56. doi:10.1055/s-0030-1256474 [DOI] [PubMed] [Google Scholar]
- 68.Peery A, Hoppo T, Garman K. Feasibility, safety, acceptability and yield of office-based screening transnasal endoscopy (with video). Gastrointest Endosc 2012;75:945–53. doi:10.1016/j.gie.2012.01.021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Kulling D, Bauerfeind P, Fried M. Transnasal versus transoral endoscopy for the placement of nasoenteral feeding tubes in critically ill patients. Gastrointest Endosc 2000;52:506–10. doi:10.1067/mge.2000.107729 [DOI] [PubMed] [Google Scholar]
- 70.Fang J, Hilden K, Holugkov R. Transnasal endoscopy versus fluroscopy for the placement of nasoenteric feeding tubes in critically ill patients. Gastrointest Endosc 2005;62:661–6. doi:10.1016/j.gie.2005.04.027 [DOI] [PubMed] [Google Scholar]
- 71.Zhihui T, Wenkui Y, Weiqin L. A randomised clincial trial of transnasal endoscopy versus fluroscopy for the placement of nasojejunal feeeding tubes in patients with severe acute pancreatitis. Postgrad Med J 2009;85:59–63. doi:10.1136/pgmj.2008.070326 [DOI] [PubMed] [Google Scholar]
- 72.Wildi SM, Gubler C, Vavricka S. Transnasal endoscopy for the placement of nasoenteral feeding tubes: does the working length of the endoscope matter? Gastrointest Endosc 2007;66:225–9. doi:10.1016/j.gie.2006.12.054 [DOI] [PubMed] [Google Scholar]
- 73.Zhang L, Huang Y, Yao W. Transnasal esophagogastricduodenoscopy for placement of nasenteric feeding tubes in patients with severe upper gastrointestinal diseases. J Dig Dis 2012;13:310–15. doi:10.1111/j.1751-2980.2012.00594.x [DOI] [PubMed] [Google Scholar]
- 74.Cheung-Hui I, Nai-Jen L, Ching-Song L. Nasogastric feeding tube placement in patients with esophageal cancer: application of ultrathin transnasal endoscopy. Gastrointest Endosc 2006;64:104–7. doi:10.1016/j.gie.2005.12.036 [DOI] [PubMed] [Google Scholar]
- 75.Dumortier J, Lapalus M, Pereira A. Unsedated transnasal PEG placement. Gastrointest Endosc 2004;59:54–7. doi:10.1016/S0016-5107(03)02526-4 [DOI] [PubMed] [Google Scholar]
- 76.Ogata T, Shimazu M, Sumi T. Percutaneous endoscopic gastrostomy using an ultra-thin transnasal endoscope for patients with trismus or GI stenosis. Dig Endosc 2009;21:A35. [Google Scholar]
- 77.Aydinli M, Koruk I, Dag MS. Ultrathin endoscopy for gastrointestinal strictures. Dig Endosc 2012;24:150–3. doi:10.1111/j.1443-1661.2011.01206.x [DOI] [PubMed] [Google Scholar]
- 78.Riley SA, Attwood SEA. Guidelines on the use of oesophageal dilatation in clinical practice. Gut 2004;53:i1–i16. doi:10.1136/gut.53.suppl_1.i1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Nakamura M, Shibata T, Tahara T. Usefulness of transnasal endoscopy where endoscopic submucosal dissection is difficult. Gastric Cancer 2011;14:378–84. doi:10.1007/s10120-011-0065-x [DOI] [PubMed] [Google Scholar]
- 80.Ahn JY, Choi KD, Lee JH. Is transnasal endoscope-assisted endoscopic submucosal dissection for gastric neoplasm useful in training beginners? Surg Endosc 2013;27:1158–65. doi:10.1007/s00464-012-2567-y [DOI] [PubMed] [Google Scholar]
- 81.Mori A, Ohashi N, Maruyama T. Transnasal endoscopic retrograde cholangiopancreatography using an ultrathin endoscope: a prospective comparison with a routine oral procedure. World J Gastroenterol 2008;14:1514–20. doi:10.3748/wjg.14.1514 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Dumonceau JM, Dumortier J, Deviere J, et al. . Transnasal OGD: practice survey and impact of a live video retransmission. Dig Liver Dis 2008;40:776–83. doi:10.1016/j.dld.2008.03.009 [DOI] [PubMed] [Google Scholar]
- 83.Yao K. The endoscopic diagnosis of early gastric cancer. Ann Gastroenterol 2013;26:11–22. [PMC free article] [PubMed] [Google Scholar]
- 84.Rey JF, Lambert R. ESGE recommendations for quality control in gastorintestinal endoscopy: guidelines for image documentation in upper and lower GI endoscopy. Endoscopy 2001;33:901–3. doi:10.1055/s-2001-42537 [DOI] [PubMed] [Google Scholar]
- 85.The J, Hartman M, Lau L. Duration of endoscopic examination significantly impacts detection rates of neoplastic lesions during diagnostic upper endoscopy. Gastrointest Endosc 2011;73:AB393. [Google Scholar]
- 86.Parker C, Panter S. Transnasal Endoscopy in the Northern REgion-Survey to assess availability and opinion of TNE. Gut 2013;62:A265–66. doi:10.1136/gutjnl-2013-304907.621 [Google Scholar]