

Abstract
Background and aims
Data on Internet addiction (IA) and its association with personality disorder are rare. Previous studies are largely restricted to clinical samples and insufficient measurement of IA.
Methods
Cross-sectional analysis data are based on a German sub-sample (n = 168; 86 males; 71 meeting criteria for IA) with increased levels of excessive Internet use derived from a general population sample (n = 15,023). IA was assessed with a comprehensive standardized interview using the structure of the Composite International Diagnostic Interview and the criteria of Internet Gaming Disorder as suggested in DSM-5. Impulsivity, attention deficit hyperactivity disorder, and self-esteem were assessed with the widely used questionnaires.
Results
Participants with IA showed higher frequencies of personality disorders (29.6%) compared to those without IA (9.3%; p < .001). In males with IA, Cluster C personality disorders were more prevalent than among non-addicted males. Compared to participants who had IA only, lower rates of remission of IA were found among participants with IA and additional cluster B personality disorder. Personality disorders were significantly associated with IA in multivariate analysis. Discussion and conclusion: Comorbidity of IA and personality disorders must be considered in prevention and treatment.
Keywords: IA, personality disorders, self-esteem, impulsivity, ADHD
Introduction
Since the Internet has become such an important tool in many different contexts, there is a rising interest in research on problematic Internet use. Internet-related disorders as such are still discussed from many different points of view. There is a debate on whether problematic Internet use could be defined as an addictive behavior per se, and if so, which kinds of Internet activities should be considered to determine a clinical diagnosis. Young (1998) described the cases of Internet addiction (IA) for the first time, proposing a classification of different Internet-related addictive behaviors. Major interest was given to online gaming, since recent studies have shown that playing the so-called Massive Multiplayer Online Role-Playing Games (MMORPGs) is associated with an enhanced risk of addictive use, namely, Internet Gaming Disorder (IGD; Muller, Beutel, Egloff, & Wolfling, 2014). Although problematic Internet use or IA might include different main activities, recently, growing research in IGD has contributed to its inclusion as a preliminary diagnosis in Section III of the DSM-5 (American Psychiatric Association, 2013).
The co-occurrence of psychiatric disorder with IA has been revealed by a body of patient studies. Mental disorders, at least Axis-I disorders, have been found to co-occur with pathological Internet use (Carli et al., 2013; Ko, Yen, Yen, Chen, & Chen, 2012). These studies reported the associations with attention deficit hyperactivity disorder (ADHD), depression, hostility or aggression, obsessive–compulsive symptoms, and anxiety disorders. Although there are some studies that discuss personality traits as risk factors for developing IA (Kuss, 2013; Muller et al., 2013, 2014; van der Aa et al., 2009), published data on personality disorders and its association with IA are rare. Black, Belsare, and Schlosser (1999) examined 21 participants who reported excessive computer use by word-of-mouth and psychiatric comorbidities, finding 52% of them having any personality disorder with the highest frequencies in borderline, narcissistic, and antisocial personality disorders. Bernardi and Pallanti (2009) assessed different comorbidities and dissociative symptoms among 15 outpatients of Internet addicts, finding 14% of the IA group having borderline, 7% having obsessive–compulsive, and 7% having avoidant personality disorders. Floros, Siomos, Stogiannidou, Giouzepas, and Garyfallos (2014) examined 50 college students who presented for the treatment of IA and found 38% of the clinical sample presenting any personality disorder (Floros et al., 2014). However, these three studies implicate conspicuous methodological limitations with samples consisting of a very few outpatients and moreover clinical subgroups. Another one issued a large sample consisting of 556 participants and focused on the association of IA and personality disorders with stratifying analyses by gender (Wu, Ko, & Lane, 2016). This study found higher rates of personality disorders in the group with IA (27.4%) than in the group without IA (13.9%; p < .01). In particular, it showed that the Internet-addicted group had higher frequencies of borderline, narcissistic, avoidant, and dependent personality disorders when compared to the non-addicted group. To our knowledge, this is the only representative study of the association between IA and personality disorders so far; however, the sample consisted of Taiwanese college students. According to latest information, Asian college students show the highest prevalence of IA (Cao, Sun, Wan, Hao, & Tao, 2011) indicating other mechanisms of pathogenesis than in non-Asian countries. Thus, findings might not be generalized. There are other methodological limitations: participants were not investigated with a DSM-5-based assessment but with the Chen IA Scale. Furthermore, there is a lack of control of further correlating conditions such as impulsivity.
To sum up, there is still a lack of studies investigating the co-occurrence of IA and personality disorders. The aim of this study was to analyze the associations between personality disorders and IA using a sample derived from the general population with a wide range of ages. It uses an extensive DSM-5-based assessment of IA criteria in a fully structured interview and takes inter-correlating factors into account. Furthermore, it analyzes the role of personality disorders in remitting from IA. On this basis, we assumed: (a) Among participants with IA, personality disorders are more prevalent than among participants without IA. (b) Because of the association between IA and low self-esteem (Ko et al., 2012; van der Aa et al., 2009), participants with IA have more often Cluster C personality disorders, covering anxious and fearful personality disorders such as avoidant, dependent, and obsessive–compulsive personality disorders. Because of the association between IA and high impulsiveness found in other studies (Gentile et al., 2011; Rehbein & Mößle, 2012; Rehbein, Kleimann, & Mössle, 2010), participants with IA have more often Cluster B personality disorders, covering dramatic and emotional personality disorders such as antisocial, borderline, histrionic, and narcissistic personality disorders (cf., Wu et al., 2016). Due to the ability to dose the social contact via online communication referring to the level of intimacy just as much as one would like, participants with IA show Cluster A personality disorders, covering eccentric personality disorders such as paranoid, schizoid, and schizotypal personality disorders. (c) Participants with personality disorders often have more Internet-related problems than participants without personality disorders. (d) Participants who remitted from IA have less often personality disorders than the participants who did not. (e) Finally, we will analyze the role of factors such as ADHD, impulsivity, and self-esteem to validate the association between IA and personality disorders, as suggested by Wu et al. (2016). Based on the characteristics of specific clusters, it might be suggested that individuals with Cluster B personality disorders develop IA due to impulsivity and Cluster C personality disorders develop IA due to low self-esteem.
Methods
Participants
The current sample is based on a large German general population-based sample of a previous study described in the following: The Pathological Gambling and Epidemiology (PAGE) study (n = 15,023) analyzed the prevalence and risk factors of pathological gambling (Meyer et al., 2015). Of the total sample, 55.2% were females whose mean age was 39.9 years (SD = 14.0) in which 4.4% were currently unemployed. Of the total sample of 15,023 participants, 8,132 reported to use the Internet for private (non-work) purposes at least 1 hr on a typical day of the week or at least 1 hr per day on the weekend. This subgroup was interviewed face-to-face with the Compulsive Internet Use Scale (CIUS; Meerkerk, Van Den Eijnden, Vermulst, & Garretsen, 2009). A total of 685 participants scored 21 or more points in the CIUS, which is the cutoff for problematic Internet use, and 307 of them consented to be contacted for future studies. In total, 196 were re-interviewed with reasons for non-participation detailed in Figure 1. A non-response analysis comparing the initial sample of 685 to those included in this study revealed that non-responders were more likely to have one of their parents born outside Germany (p < .001) and were more likely to have less than 10 years of schooling (p = .012). There were no differences in gender, age, unemployment status, and CIUS scores. Of the 196 participants interviewed, 168 participants aged 18 and older were included for the current analysis. Because of the fact that personality disorders should only be diagnosed in adults, 28 participants being under the age of 18 were excluded from the assessment of personality disorders. Of the 168 participants interviewed, 71 fulfilled five or more criteria according to the DSM-5-based diagnostic interview (see below). Among this sample, 25 specified computer games, 25 social networks, and 21 other applications (entertainment, downloads, buying or selling, eroticism and pornography, searching contemporary issues and news, and visiting dating sites) were their main activity when using the Internet.
Figure 1.
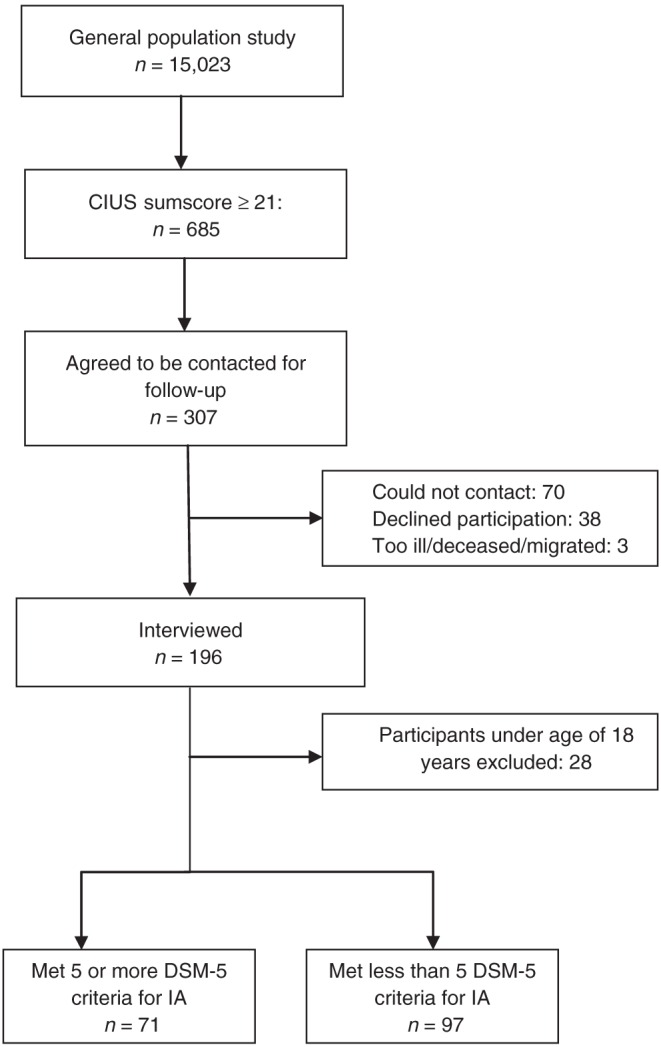
Flowchart of recruitment
Measures
Assessment of problematic Internet use
Participants scoring 21 points or more on the CIUS were defined as having elevated levels of Internet use and an increased risk of IA. The CIUS was used as a screener consisting of 14 items and representing the following five core criteria: salience, withdrawal, loss of control, conflict, and coping with unpleasant mood. Questions were answered on a 5-point Likert-type scale from “never” to “very often.” A stable one-factor solution was found across time and different samples, and Cronbach’s α ranging from .88 to .90 (Meerkerk et al., 2009), suggesting good validity and reliability.
Assessment of IA
For assessing the DSM-5 criteria proposed for IGD more broadly adapted to general Internet use, a personal diagnostic interview was used. This fully structured interview was based on the principles and structure of the Composite International Diagnostic Interview (CIDI; Wittchen, 1994). In the wording of the nine DSM-5 criteria, “Internet activities” replaced “gaming” to apply all probable forms of Internet use. All nine DSM-5 criteria were assessed by a total of 27 questions, with between one (for “loss of interest”) and nine (for “excessive use despite problems”) questions per criterion. Each symptom or criterion was assessed using dichotomous answers. Affirmative responses to any item related to the criterion constituted endorsement of the criterion. The structure and succession of questions relate to the original CIDI sections for substance use disorders and pathological gambling. The wording was kept as close as possible to these sections but was adapted to Internet use. Following recommendations in DSM-5, fulfilling five or more of the nine criteria was considered to meet Internet use disorder.
Overall, the diagnostic interview shows an excellent reliability for past year IA (Yule’s Y: .84) as well as lifetime diagnosis (Y = .86) in a sample of students (n = 66) from vocational schools (unpublished data). Students with elevated levels of Internet use (CIUS > 20) were interviewed twice within a period of 40 days (mean). In this study, lifetime as well as past year symptoms were assessed. According to the relationship of IA and personality disorders, lifetime diagnoses were analyzed. Remission of IA was defined as having fulfilled lifetime but no past year diagnosis.
Assessment of personality disorders
The following personality disorders were assessed in all subjects using the German version (Fydrich, Renneberg, Schmitz, & Wittchen, 1997) of the Structured Clinical Interview for DSM-IV Axis II Personality Disorders (SCID-II; First, Gibbon, Spitzer, Williams, & Benjamin, 1997): paranoid, schizoid, schizotypal, antisocial, borderline, histrionic, narcissistic, dependent, avoidant, and obsessive–compulsive personality disorders. SCID-II shows an excellent inter-rater reliability (Lobbestael, Leurgans, & Arntz, 2011). Interviews were conducted by clinically experienced psychologists via face-to-face sessions among participants aged 18 years and older. The psychologists involved had been trained in performing the SCID-II.
Assessment of ADHD
For measuring ADHD symptoms, a German translation of the Conners’ Adult ADHD Rating Scale (CAARS; Conners, Erhardt, & Sparrow, 1999) was used. It has proven to show a very high model fit in confirmative factor analysis with the established factors inattention and memory problems, hyperactivity and restlessness, impulsivity and emotional liability, and problems with self-concept. The CAARS has psychometric properties with Cronbach’s α ranging from .74 to .95 and test–retest reliability from .85 to .92 (Christiansen et al., 2012).
Assessment of impulsivity
A German version (Preuss et al., 2003) of the Barratt Impulsiveness Scale (BIS-11; Patton, Stanford, & Barratt, 1995) was used to measure the participants’ impulsivity. The questionnaire covers attention, motor, self-control, cognitive complexity, perseverance, and cognitive instability. It is one of the most widely used self-report measures. Data for both internal consistency and test–retest reliability were found to be .83 (Vasconcelos, Malloy-Diniz, & Correa, 2012).
Assessment of self-esteem
For measuring self-esteem, the Rosenberg’s self-esteem scale (Rosenberg, 1965) was used. It contains 10 items with half of them describing the positive aspects and the other half of them describing the negative aspects of one’s self-assessment. Items are answered on a 4-point Likert-type scale from “strongly disagree” to “completely agree.” The scale has an internal consistency ranging from .81 to .87 and a split-half reliability ranging from .82 to .84 (Ferring & Filipp, 1996).
Procedure
This study is based on a sample of the study “PAGE” (Meyer et al., 2015). The current follow-up study “Prevalence of Internet Use Disorder: Diagnoses and Risk profiles (PINTA-DIARI)” carried out personal interviews in a part of this sample for further assessment of Internet use disorder. The interviews were conducted nationwide at the homes of participants or at another convenient place in their hometown. They were performed by trained academic personnel experienced in clinical psychology. PAGE was funded by the German federal states; PINTA and PINTA-DIARI were funded by the German Federal Ministry of Health.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics 23. For analyzing associations between IA and any personality disorder, specific personality disorders as well as personality disorders in terms of the clusters, χ2-test was used. For analyzing the associations between personality disorders and the number of IA criteria, a non-parametric rank test (Mann–Whitney U test) was used. The association between personality disorders and the remission of IA was tested using the χ2-test. For the analysis of confounding factors such as ADHD, impulsivity, and self-esteem in the prediction of IA by personality disorders, binary logistic regression models were computed.
Ethics
The study procedures were carried out in accordance with the Declaration of Helsinki. The PAGE, PINTA, and PINTA-DIARI study were approved by the ethics committees of the University of Lübeck, Lübeck, Germany and the University of Greifswald, Greifswald, Germany. All subjects were informed about the study and all provided informed consent.
Results
Sample description
The total sample consisted of 168 participants with 71 fulfilling the criteria for IA and 97 not fulfilling the criteria. Of the total sample, 51.2% were males whose mean age was 32.9 years (SD = 12.4), 7.2% had 9 years or less of schooling, 57.5% had 10 years, and 35.3% had more than 10 years. Of the total sample, 7.1% were unemployed and 25.5% had a migration background. Of the 71 participants with IA, 35.2% reported online games, 35.2% social networks, and 29.6% other applications as their main activities when using the Internet (Table 1).
Table 1.
Sample description
| Feature | Total | IA | No IA | p value |
|---|---|---|---|---|
| n = 168 (%) | n = 71 (%) | n = 97 (%) | ||
| Age, M ± SD | 32.9 ± 12.4 | 31.1 ± 11.5 | 34.2 ± 13.0 | .12 n.s. |
| Gender | ||||
| Male | 86 (51.2) | 38 (53.5) | 48 (49.5) | .61 n.s. |
| Female | 82 (48.8) | 33 (46.5) | 49 (50.5) | |
| Years of schooling | ||||
| <10th class | 15 (8.9) | 4 (5.6) | 11 (11.3) | .20 n.s. |
| ≥10th class | 153 (91.1) | 67 (94.4) | 86 (88.7) | |
| Employment | ||||
| Employed | 156 (92.9) | 66 (93.0) | 90 (92.8) | .97 n.s. |
| Unemployed | 12 (7.1) | 5 (7.0) | 7 (7.2) | |
| Migration | ||||
| Migration background | 42 (25.5) | 19 (27.1) | 23 (24.2) | .67 n.s. |
| No migration background | 123 (74.5) | 51 (72.9) | 72 (75.8) | |
| Main activity | ||||
| Online games | 43 (25.6) | 25 (35.2) | 18 (18.6) | .01** |
| Social networks | 56 (33.3) | 25 (35.2) | 31 (32.0) | |
| Other applications | 69 (41.1) | 21 (29.6) | 48 (49.5) | |
Note. n: valid values (%); M: mean; SD: standard deviation; n.s.: not significant. **p ≤ .01.
The association between IA and personality disorders
Tables 2–4 show the differences in frequencies of personality disorders among participants with and without IA. In the total sample, clear differences were observed indicating that individuals with IA have more often personality disorders than individuals without IA (p ≤ .001). However, separating the sample by gender, differences were only observed in males (p < .01), but not in females. When analyzing having any personality disorder between the subgroups with different Internet main activities, no significant differences were observed (computer games 28.0%, social networks 28%, and others 33.3%; p = .90; not shown in the tables).
Table 2.
Occurrence of any personality disorder in participants with and without IA (χ2-test)
| Any personality | Total | IA | No IA | |
|---|---|---|---|---|
| disorder | n = 168 (%) | n = 71 (%) | n = 97 (%) | p value |
| All | 30 (17.9) | 21 (29.6) | 9 (9.3) | .001*** |
| Male | 17 (19.8) | 13 (34.2) | 4 (8.3) | .003** |
| Female | 13 (15.9) | 8 (24.2) | 5 (10.2) | .09 n.s. |
Note. n: valid values (%); n.s.: not significant. **p ≤ .01. ***p ≤ .001.
Table 4.
Occurrence of Clusters A, B, and C personality disorders in participants with and without IA (χ2-test)
| Total | No IA | |||
|---|---|---|---|---|
| Clusters | n = 168 (%) | IA n = 71 (%) | n = 97 (%) | p value |
| All | ||||
| Cluster A | 7 (4.2) | 6 (8.5) | 1 (1.0) | .043*a |
| Cluster B | 13 (7.7) | 10 (14.1) | 3 (3.1) | .008** |
| Cluster C | 22 (13.1) | 15 (21.1) | 7 (7.2) | .008** |
| Male | ||||
| Cluster A | 3 (3.5) | 3 (7.9) | 0 (0.0) | .08 n.s.a |
| Cluster B | 10 (11.6) | 7 (18.4) | 3 (6.3) | .10 n.s.a |
| Cluster C | 13 (15.1) | 11 (28.9) | 2 (4.2) | .001*** |
| Female | ||||
| Cluster A | 4 (4.9) | 3 (9.1) | 1 (2.0) | .30 n.s.a |
| Cluster B | 3 (3.7) | 3 (9.1) | 0 (0.0) | .06 n.s.a |
| Cluster C | 9 (11.0) | 4 (12.1) | 5 (10.2) | 1.00 n.s.a |
Note. n: valid values (%); n.s.: not significant.
Fisher’s exact test.
*p ≤ .05. **p ≤ .01. ***p ≤ .001.
Table 3.
Occurrence of single personality disorders in participants with and without IA (χ2-test)
| Specific personality disorder | Total | IA | No IA | |
|---|---|---|---|---|
| n = 168 (%) | n = 71 (%) | n = 97 (%) | p value | |
| Paranoid PD | 6 (3.6) | 5 (7.0) | 1 (1.0) | .08 n.s.a |
| Schizoid PD | 1 (0.6) | 1 (1.4) | 0 (0.0) | .42 n.s.a |
| Schizotype PD | 0 (0.0) | 0 (0.0) | 0 (0.0) | –b |
| Antisocial PD | 4 (2.4) | 2 (2.8) | 2 (2.8) | 1.00 n.s.a |
| Borderline PD | 6 (3.6) | 6 (8.5) | 0 (0.0) | .005**a |
| Histrionic PD | 1 (0.6) | 1 (1.4) | 0 (0.0) | .42 n.s.a |
| Narcissistic PD | 2 (1.2) | 1 (1.4) | 1 (1.0) | 1.00 n.s.a |
| Avoidant PD | 11 (6.5) | 8 (11.3) | 3 (3.1) | .06 n.s.a |
| Dependent PD | 1 (0.6) | 0 (0.0) | 1 (1.0) | 1.00 n.s.a |
| Compulsive–obsessive PD | 13 (6.6) | 8 (11.3) | 5 (5.2) | .14 n.s. |
Note. n: valid values (%); n.s.: not significant; PD: personality disorder.
Fisher’s exact test.
No statistics computed.
**p ≤ .01.
With regard to specific personality disorders, differences were observed only in borderline personality disorder among participants with IA showing more often borderline personality disorder (p < .01) than participants without IA.
In the total sample, differences with regard to the clusters of personality disorders are observed in all clusters, again, indicating that individuals with IA have more often personality disorders than individuals without IA. More specifically, the differences were found in Cluster C (p < .01) and Cluster B (p < .01) as well as in Cluster A (p < .05). Separating the sample by gender, significant differences were observed only in males with regard to Cluster C (p ≤ .001) indicating that especially male individuals with IA tend to have Cluster C personality disorders.
The association between personality disorders and the number of IA criteria
Table 4 presents the mean ranks of fulfilled DSM-5 criteria for IA among participants with and without personality disorders. With regard to any personality disorder, significant differences were observed in the total sample (p < .001) as well as in the separated groups of males (p < .001) and females (p < .05) indicating that individuals with personality disorders show higher levels of IA than individuals without personality disorders. With regard to the clusters, the same is true for Cluster B personality disorders (total sample: p < .001, males: p ≤ .001, females: p < .05), whereas in Cluster A, differences are only observed in the total sample (p < .01) and males (p < .01), but not in females (n.s.) and similar to Cluster C with differences in the total sample (p < .01) and, again, strong differences in males (p < .001), but not in females (n.s.) (Table 5).
Table 5.
Comparisons of mean ranks of fulfilled DSM-5-criteria for IA in participants with and without personality disorders
| Sample | Criteria fulfilled Mean ranks | Criteria not fulfilled Mean ranks | p value |
|---|---|---|---|
| Any personality disorder | |||
| All (n = 168) | 76.86 (n = 30) | 119.63 (n = 138) | .001*** |
| Male (n = 86) | 64.79 (n = 17) | 38.25 (n = 69) | .001*** |
| Female (n = 82) | 54.35 (n = 13) | 39.08 (n = 69) | .033* |
| Cluster A | |||
| All (n = 168) | 135.64 (n = 7) | 82.28 (n = 161) | .004** |
| Male (n = 86) | 83.00 (n = 3) | 42.07 (n = 83) | –a |
| Female (n = 82) | 56.75 (n = 4) | 40.72 (n = 78) | –a |
| Cluster B | |||
| All (n = 168) | 136.04 (n = 13) | 80.18 (n = 155) | .001*** |
| Male (n = 86) | 67.85 (n = 10) | 40.30 (n = 76) | .001*** |
| Female (n = 82) | 69.67 (n = 3) | 40.43 (n = 79) | –a |
| Cluster C | |||
| All (n = 168) | 114.52 (n = 22) | 79.98 (n = 146) | .002** |
| Male (n = 86) | 65.73 (n = 13) | 39.54 (n = 73) | .001*** |
| Female (n = 82) | 47.22 (n = 9) | 40.79 (n = 73) | .441 n.s |
Note. n.s.: not significant.
No statistics computed; cell counts <5.
*p ≤ .05. **p ≤ .01. ***p ≤ .001.
The association between personality disorders and remission of IA
Table 6 presents the frequencies of remission among participants with IA with regard to any personality disorder and clusters of personality disorders. Significant differences were found for Cluster B (p < .01) indicating that individuals with IA but no additional Cluster B personality disorders are more likely to remit from IA than individuals who fulfill criteria for Cluster B personality disorders additionally. Adjusting for basic variables such as age and gender was not considered, because no significant effects with remission status were found.
Table 6.
Comparison of remission of IA in participants with personality disorders
| IA | IA | ||
|---|---|---|---|
| Personality disorder | Remitted (n = 38) | Not remitted (n = 33) | p value |
| Any personality disorder | |||
| n = 21 (%) | 8 (38.1) | 13 (61.9) | .09 n.s. |
| Cluster A | |||
| n = 6 (%) | 1 (16.7) | 5 (83.3) | .09 n.s.a |
| Cluster B | |||
| n = 10 (%) | 1 (10.0) | 9 (90.0) | .004**a |
| Cluster C | |||
| n = 15 (%) | 7 (46.7) | 8 (53.3) | .55 n.s. |
Note. n: valid values (%); n.s.: not significant.
Fisher’s exact test.
**p ≤ .01.
Analysis of confounding factors
Based on the characteristics of Cluster C and Cluster B personality disorders, it might be suggested that Cluster C is associated with self-esteem and Cluster B is associated with impulsiveness. Therefore, possible inter-correlations were tested using logistic regression analysis. Table 7 presents the following confounding factors in the prediction of IA by personality disorders: ADHD, impulsivity, and self-esteem. With regard to impulsivity, the following subscales of the BIS-11 differentiated significantly between participants with and without IA and were included in the logistic model: persistence and cognitive instability. Binary logistic regression of all factors shows that in the prediction of IA only having any personality disorder was significant (p < .05).
Table 7.
Analysis of the confounding factors such as ADHD, impulsivity, and self-esteem with respect to the relationship between personality disorders and Internet addiction (binary logistic regression analysis)
| Factors | Odds ratio (95% CI) | p value |
|---|---|---|
| Any personality disorder | 1.72 (1.09–2.69) | .02* |
| CAARS | 1.16 (0.48–2.80) | .74 n.s. |
| BIS-11 (cognitive instability)a | 1.45 (0.67–3.13) | .35 n.s. |
| BIS-11 (persistence)a | 1.24 (0.56–2.73) | .59 n.s. |
| Rosenberg scale | 0.92 (0.84–1.02) | .11 n.s. |
| Cluster Cb | 1.67 (1.02–2.74) | .04* |
| Rosenberg scale | 0.90 (0.83–0.98) | .02* |
| Cluster Bc | 2.00 (1.01–3.96) | .05* |
| BIS-11 (cognitive instability)a | 1.50 (0.75–3.01) | .26 n.s. |
| BIS-11 (persistence)a | 1.35 (0.64–2.87) | .43 n.s. |
Note. CI: confidence interval; n.s.: not significant.
Only the subscales’ cognitive instability and persistence of the BIS-11 differentiated significantly between participants with and without IA and were included in the logistic regression model.
Based on theoretical considerations, possible inter-correlations between Cluster C and self-esteem were tested.
Based on theoretical considerations, possible inter-correlations between Cluster B and impulsivity were tested; no association of any of the assessed variables with Cluster A was assumed.
*p ≤ .05.
With regard to the regression model of Cluster C personality disorders and self-esteem, both variables are significant in the prediction of IA (Cluster C: p < .05, self-esteem: p < .05).
With regard to the regression model of Cluster B personality disorders and impulsivity, Cluster B is significant in the prediction of IA (p < .05), but not impulsivity.
Discussion
This study examined the association of IA and personality disorders in a general population-based sample of 168 male and female individuals with a wide range of ages. Of the total sample, 71 participants fulfilled the criteria for IA based on criteria suggested in DSM-5. The rate of personality disorders among participants with IA was found to be 29.6% and 9.3% among participants without IA.
We found that individuals with IA showed a higher frequency of personality disorders of all clusters. Particularly, males with IA were found to have much more frequent Cluster C personality disorders compared with the non-addicted males. Cluster C includes avoidant, dependent, and obsessive–compulsive personality disorders. Individuals with these disorders tend to appear anxious and fearful (American Psychiatric Association, 2013). The anonymity in online applications enables users to take part in communities without being exposed to the risk of interpersonal conflicts and personal criticism in face-to-face situations. Their low self-esteem might be compensated by a controlled extent of personal information presented in the Internet and rewards receiving in games. In addition, the opportunity to withdraw from interactions or going offline might increase security. Furthermore, self-referred information in social networks as well as in online games can be adapted to a more attractive or more self-confident manner. In MMORPGs, for example, users are able to create their avatars with a diversity of features and characteristic abilities, which do not depend on their real-life features. Individuals take part in online game communities and find “friends” with same interests without being forced to display themselves personally. Thus, the need for social contact and integration can be satisfied in online activities, whereas individuals with Cluster C personality disorders might not feel able to play part in real life interaction due to their shyness and insecurity. These findings are in line with the results of some studies analyzing the association between Internet-related disorders and big five personality traits. Those studies claimed increased neuroticism (Muller et al., 2014) as well as lower extraversion (Muller et al., 2013) in patients with IGD. Similar to our suggestions, they assumed gamers to tend to perceive the real world as more threatening.
In this study, higher mean ranks of DSM-5-criteria for IA were found in individuals with personality disorders compared to those without personality disorders. These findings might indicate that individuals with personality disorders are more likely to develop IA. Referring to this, our data are more pronounced for male participants with Cluster B and Cluster C personality disorders. Cluster B includes antisocial, borderline, histrionic, and narcissistic personality disorders. Individuals with these disorders tend to appear dramatic, emotional, and erratic (American Psychiatric Association, 2013). The essential feature of antisocial personality disorder is a pattern of disregard for and violation of the rights of others. Individuals with borderline personality disorder are distinguished by a pattern of chronic feelings of emptiness and interpersonal and affective instability. For histrionic personality disorder, a pattern of attention seeking is specified. The essential feature of narcissistic personality disorder is a pattern of grandiosity and need for admiration. Several reasons might make the online environment very attractive for individuals with Cluster B personality disorders: due to the ability to act out violent and criminal behavior with less risk of consequences, the online environment might be very attractive for individuals with antisocial personality disorder. Individuals with borderline personality disorder might escape from their unpleasant feelings of loneliness and boredom using social networking sites and chats. This explanation is roughly in agreement with other studies discussing online activities as a coping strategy for emotional or social difficulties (Ko et al., 2012). For individuals with histrionic and narcissistic personality disorders, online games and especially social network platforms might be an attractive opportunity for self-display. Our findings and listed interpretations of Cluster B personality disorders in Internet-addicted participants are roughly conform to prior research examining the association between personality traits and compulsive Internet use (CIU; van der Aa et al., 2009). The authors found that for low-agreeable and emotionally less-stable youth, daily Internet use is strongly associated with CIU and, in turn, CIU is strongly linked to feelings of loneliness.
Altogether, our findings are roughly in line with those found on the co-occurrence of IA and personality disorders in Taiwanese students (Wu et al., 2016). Similar to that study, we observed higher frequencies of Cluster B and Cluster C personality disorders in the IA group compared to the non-addicted group. However, in contrast to those findings showing higher frequencies of avoidant and dependent personality disorders in female participants with IA, the opposite is true with regard to our results showing higher frequencies of Cluster C personality disorders in males with IA.
In addition, our study shed light on the impact of personality disorders on remitting from IA. We found that among participants with IA those without additional personality disorders show a higher frequency of remission of IA compared to those who fulfill criteria for personality disorders additionally. However, data were found to be significant only for Cluster B personality disorders, but the sample size for analysis was small at this point; therefore, studies with larger sample sizes are needed in the future. Lower rates of remission of IA among individuals who have IA and personality disorders additionally indicate the importance of this issue for therapeutic indications. Further research is needed to evaluate whether personality disorders are a main factor for pathogenesis and maintenance of IA.
Furthermore, going beyond Wu et al.’s (2016) findings, this study examined the confounding factors such as ADHD, impulsivity, and self-esteem to validate the association between IA and personality disorders. Because ADHD is associated with IA in general (Carli et al., 2013), we included it as one factor to the logistic regression model. It might be suggested that Cluster B personality disorders are related to impulsivity and Cluster C personality disorders are related to self-esteem. It turned out that for all factors taken together, the association between IA and any personality disorder was not explained better by ADHD, impulsivity, or self-esteem, which underlines the validity of this association.
There are certain strengths in our presented research: This is one of a very few studies to examine personality disorders with the SCID-II instead of using a screening or Big Five criteria only when analyzing the association with IA. A clear advantage is the recruitment based on a nationally representative study. We examined 168 participants with different socio-demographic backgrounds. Another one is the diagnostic procedure of IA based on a CIDI-based interview on the grounds of the DSM-5-criteria for IGD. In addition to this, we also considered the moderating factors such as ADHD, impulsivity, and self-esteem. However, some limitations need to be mentioned as well.
Although our study is based on a representative survey, it has to be taken into account that the whole sample consisted of individuals showing a problematic extent of Internet usage, defined by a cutoff of 21 or more on the CIUS. Results would be more pronounced if we took a group without any distinctive features of Internet usage into account additionally. Furthermore, there are some socio-demographic inequalities. Non-responders in the in-depth interview were more likely to have less school education and more often a migration background. In addition, in some data analyses, sample sizes are quite small, wherefore some results might have missed significance or might be interpreted with caution. This is true for the analysis of the specific personality disorders, the analysis of remission, as well as the analysis in which gender was considered. Another limitation is that unfortunately Cluster A personality disorders were under-represented (n = 6). This might have its reasons in the characteristics of Cluster A personality disorders itself: Cluster A includes paranoid, schizoid, and schizotypal personality disorders. Individuals with these disorders show patterns of pervasive distrust, detachment from social relationships, or social deficits marked by acute discomfort in social situations or relationships (American Psychiatric Association, 2013). It may be less likely to get them acquired for psychological research.
Finally, it has to be mentioned that, because of small sample sizes at some points, results have an explorative quality. Furthermore, results have to be interpreted with caution, since they do not prove any causalities.
Overall, the results support our hypotheses about the association of IA and personality disorders. Individuals with personality disorders, especially with personality disorders associated with low self-esteem and high impulsivity, that are Cluster C and Cluster B personality disorders, might be at special risk for developing IA. Affected individuals might tend to use online applications in a maladaptive manner to cope with interpersonal and emotional difficulties in the real world. As a consequence, personality disorders might be a perpetuating factor for IA and vice versa. If social difficulties in the real world will not improve, individuals might receive and satisfy social motivation predominantly from the Internet, then the risk of becoming addicted to the Internet might increase and individuals might develop increased impairments in real-life situations. In this condition, treatment focusing only on IA might result in the failure of treatment.
Conclusion
This study contributes new findings referring to the linkages between IA and personality disorders and the other way round, finding that individuals with IA more often suffer from personality disorders, especially Cluster C and Cluster B personality disorders. It encourages further research for these interacting disorders in order to identify subgroups that are at special risk for the development of IA, to identify mechanisms for the perpetuation of IA, and to develop an adequate psychotherapeutic treatment. Finally, it would be desirable that further research would take different kinds of Internet applications into account. It might be suggested that associations of IA and personality disorders depend on the different applications in the Internet such as gaming, using social networks or other activities.
Authors’ contribution:
SZ: statistical analysis and interpretation of findings, preparation of manuscript draft. GB: study concept and design. BB: data gathering. AB: study concept and design, data gathering. CM, UJ: study concept and design, obtained funding. H-JR: study concept and design, obtained funding, statistical analysis and interpretation of findings. All authors had full access to all data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Conflict of interest:
The authors declare that they have no conflict of interest.
Funding Statement
Funding sources: This work was supported by German Federal States and German Federal Ministry of Health.
References
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed). Washington, DC: American Psychiatric Association. [Google Scholar]
- Bernardi S., Pallanti S. (2009). Internet addiction: A descriptive clinical study focusing on comorbidities and dissociative symptoms. Comprehensive Psychiatry, 50(6), 510–516. doi:10.1016/j.comppsych.2008.11.011 [DOI] [PubMed] [Google Scholar]
- Black D. W., Belsare G., Schlosser S. (1999). Clinical features, psychiatric comorbidity, and health-related quality of life in persons reporting compulsive computer use behavior. The Journal of Clinical Psychiatry, 60(12), 839–844. doi:10.4088/JCP.v60n1206 [DOI] [PubMed] [Google Scholar]
- Cao H., Sun Y., Wan Y. H., Hao J. H., Tao F. B. (2011). Problematic Internet use in Chinese adolescents and its relation to psychosomatic symptoms and life satisfaction. BMC Public Health, 11(1), 802. doi:10.1186/1471-2458-11-802 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carli V., Durkee T., Wasserman D., Hadlaczky G., Despalins R., Kramarz E., Wasserman C., Sarchiapone M., Hoven C. W., Brunner R., Kaess M. (2013). The association between pathological Internet use and comorbid psychopathology: A systematic review. Psychopathology, 46(1), 1–13. doi:10.1159/000337971 [DOI] [PubMed] [Google Scholar]
- Christiansen H., Kis B., Hirsch O., Matthies S., Hebebrand J., Uekermann J., Abdel-Hamid M., Kraemer M., Wiltfang J., Graf E., Colla M., Sobanski E., Alm B., Rosler M., Jacob C., Jans T., Huss M., Schimmelmann B. G., Philipsen A. (2012). German validation of the Conners Adult ADHD Rating Scales (CAARS) II: Reliability, validity, diagnostic sensitivity and specificity. European Psychiatry, 27(5), 321–328. doi:10.1016/j.eurpsy.2010.12.010 [DOI] [PubMed] [Google Scholar]
- Conners C. K., Erhardt D., Sparrow E. (1999). Conners’ Adult ADHD Rating Scales (CAARS). North Tonawanda, NY, USA: Multihealth Systems, Inc. [Google Scholar]
- Ferring D.Filipp S.-H. (1996). Messung des Selbstwertgefühls: Befunde zu Reliabilität, Validität und Stabilität der Rosenberg-Skala [Measurement of Self-Esteem: Results on Reliability, Validity and Stability of the Rosenberg-Scale]. Diagnostica, 42(3), 284–292. [Google Scholar]
- First M., Gibbon M., Spitzer R., Williams J., Benjamin L. (1997). Structured clinical interview for DSM-IV Axis II personality disorders (SCID-II). Washington, DC: American Psychiatric Press, Inc. [Google Scholar]
- Floros G., Siomos K., Stogiannidou A., Giouzepas I., Garyfallos G. (2014). Comorbidity of psychiatric disorders with Internet addiction in a clinical sample: The effect of personality, defense style and psychopathology. Addictive Behaviors, 39(12), 1839–1845. doi:10.1016/j.addbeh.2014.07.031 [DOI] [PubMed] [Google Scholar]
- Fydrich T., Renneberg B., Schmitz B., Wittchen H.-U. (1997). SKID-II – Strukturiertes klinisches interview für DSM-IV Achse II: Persönlichkeitsstörungen [SCID-II – Structured clinical interview for DSM-IV Axis II: Personality Disorders]. Göttingen, Germany: Hogrefe. [Google Scholar]
- Gentile D. A., Choo H., Liau A., Sim T., Li D., Fung D., Khoo A. (2011). Pathological video game use among youths: A two-year longitudinal study. Pediatrics, 127(2), e319–e329. doi:10.1542/peds.2010-1353 [DOI] [PubMed] [Google Scholar]
- Ko C. H., Yen J. Y., Yen C. F., Chen C. S., Chen C. C. (2012). The association between Internet addiction and psychiatric disorder: A review of the literature. European Psychiatry, 27(1), 1–8. doi:10.1016/j.eurpsy.2010.04.011 [DOI] [PubMed] [Google Scholar]
- Kuss D. J. (2013). Internet gaming addiction: Current perspectives. Psychology Research and Behavior Management, 6, 125–137. doi:10.2147/PRBM.S39476 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lobbestael J., Leurgans M., Arntz A. (2011). Inter-rater reliability of the structured clinical interview for DSM-IV Axis I Disorders (SCID I) and Axis II Disorders (SCID II). Clinical Psychology & Psychotherapy, 18(1), 75–79. doi:10.1002/cpp.693 [DOI] [PubMed] [Google Scholar]
- Meerkerk G. J., Van Den Eijnden R., Vermulst A. A., Garretsen H. F. (2009). The Compulsive Internet Use Scale (CIUS): Some psychometric properties. CyberPsychology & Behavior, 12(1), 1–6. doi:10.1089/cpb.2008.0181 [DOI] [PubMed] [Google Scholar]
- Meyer C., Bischof A., Westram A., Jeske C., de Brito S., Glorius S., Schön D., Porz S., Gürtler D., Kastirke N., Hayer T., Jacobi F., Lucht M., Premper V., Gilberg R., Hess D., Bischof G., John U., Rumpf H.-J. (2015). The “Pathological Gambling and Epidemiology” (PAGE) study program: Design and fieldwork. International Journal of Methods in Psychiatric Research, 24(1), 11–31. doi:10.1002/mpr.1458 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muller K. W., Beutel M. E., Egloff B., Wolfling K. (2014). Investigating risk factors for Internet gaming disorder: A comparison of patients with addictive gaming, pathological gamblers and healthy controls regarding the big five personality traits. European Addiction Research, 20(3), 129–136. doi:10.1159/000355832 [DOI] [PubMed] [Google Scholar]
- Muller K. W., Koch A., Dickenhorst U., Beutel M. E., Duven E., Wolfling K. (2013). Addressing the question of disorder-specific risk factors of Internet addiction: A comparison of personality traits in patients with addictive behaviors and comorbid Internet addiction. Biomed Research International, 2013, 1–7. doi:10.1155/2013/546342 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patton J. H., Stanford M. S., Barratt E. S. (1995). Factor structure of the Barratt impulsiveness scale. Journal of Clinical Psychology, 51(6), 768–774. doi:10.1002/1097-4679(199511)51:6<768::AID-JCLP2270510607>3.0.CO;2-1 [DOI] [PubMed] [Google Scholar]
- Preuss U. W., Rujescu D., Giegling I., Koller G., Bottlender M., Engel R. R., Moller H. J., Soyka M. (2003). Factor structure and validity of a German version of the Barratt impulsiveness scale. Fortschritte der Neurologie Psychiatrie, 71(10), 527–534. doi:10.1055/s-2003-42872 [DOI] [PubMed] [Google Scholar]
- Rehbein F., Kleimann M., Mössle T. (2010). Prevalence and risk factors of video game dependency in adolescence: Results of a German nationwide survey. Cyberpsychology, Behavior, and Social Networking, 13(3), 269–277. doi:10.1089/cyber.2009.0227 [DOI] [PubMed] [Google Scholar]
- Rehbein F., Mößle T. (2012). Risikofaktoren für Computerspielabhängigkeit: Wer ist gefährdet? [Risk factors for Computergame Addiction: Who is at risk?] Sucht, 58, 391–400. doi:10.1024/0939-5911.a000216 [Google Scholar]
- Rosenberg M. (1965). Society and the adolescent self-image. Princeton, NJ: Princeton University Press. [Google Scholar]
- van der Aa N., Overbeek G., Engels R. C., Scholte R. H., Meerkerk G. J., Van den Eijnden R. J. (2009). Daily and compulsive Internet use and well-being in adolescence: A diathesis-stress model based on big five personality traits. Journal of Youth and Adolescence, 38(6), 765–776. doi:10.1007/s10964-008-9298-3 [DOI] [PubMed] [Google Scholar]
- Vasconcelos A. G., Malloy-Diniz L., Correa H. (2012). Systematic review of psychometric properties of Barratt Impulsiveness Scale Version 11 (BIS-11). Clinical Neuropsychiatry: Journal of Treatment Evaluation, 9(2), 61–74. [Google Scholar]
- Wittchen H.-U. (1994). Reliability and validity studies of the WHO-Composite International Diagnostic Interview (CIDI): A critical review. Journal of Psychiatric Research, 28(1), 57–84. doi:10.1016/0022-3956(94)90036-1 [DOI] [PubMed] [Google Scholar]
- Wu J. Y., Ko H. C., Lane H. Y. (2016). Personality disorders in female and male college students with Internet addiction. The Journal of Nervous and Mental Disease, 204(3), 221–225. doi:10.1097/NMD.0000000000000452 [DOI] [PubMed] [Google Scholar]
- Young K. S. (1998). Internet addiction: The emergence of a new clinical disorder. CyberPsychology & Behavior, 1(3), 237–244. doi:10.1089/cpb.1998.1.237 [Google Scholar]