

Abstract
Background:
Use of a pedicle screw at the level of fracture, also known as an intermediate screw, has been shown to improve clinical results in managing thoracolumbar(TL) fractures, but there is a paucity of powerful evidence to support the claim. The aim of this study was to compare outcomes between pedicle screw fixation combined with intermediate screw at the fracture level and conventional pedicle screw fixation (one level above and one level below the fracture level) for thoracolumbar (TL) fractures.
Methods:
A meta-analysis of cohort studies was conducted between pedicle screw fixation combined with intermediate screw at the fracture level (combined screw group) and conventional pedicle screw fixation (conventional group) for the treatment of TL fractures from their inception to December 2015. An extensive search of studies was performed in PubMed, Medline, Embase, and the Cochrane library. The following outcome measures were extracted: visual analogue scale (VAS), operation time and intraoperative blood loss, Cobb angle and anterior vertebral height (AVH), and complications. Data analysis was conducted with RevMan 5.3.5.
Results:
From 10 relevant studies identified, 283 patients undergoing pedicle screw fixation combined with intermediate screw at the fracture level were compared with 285 conventional pedicle screw procedures. The pooled analysis showed that there was statistically significant difference in terms of postoperative Cobb angle (95% confidence interval (CI), −3.00, −0.75; P = 0.001) and AVH (95% CI, 0.04, 12.23; P = 0.05), correction loss (Cobb angle: P < 0.0001; AVH: P < 0.0001) and implant failure rate (95% CI, 0.06, 0.62; P = 0.006), and blood loss (W 95% CI, 2.22, 23.60; P = 0.02) between 2 groups. But in terms of other complications, there were no differences between 2 groups (95% CI, 0.23, 2.04; P = 0.50). No difference was found in operation time (95% CI, −5.36, 14.67; P = 0.36) and VAS scores (95% CI, −0.44, 0.01; P = 0.06).
Conclusions:
The combined screw fixation technique was associated with better reduction of the fractured vertebrae, less correction loss in the follow-up, and lower implant failure rate. Given the lack of robust clinical evidence, these findings warrant verification in large prospective registries and randomized trials with long-term follow-up.
Keywords: fracture level, intermediate screw, pedicle screw fixation, thoracolumbar fracture, trauma
1. Introduction
Almost 60% to 70% of traumatic spinal fractures are related to thoracolumbar (TL) region which ranges from T11 to L2.[1,2] In clinical practice, TL fractures are managed either nonsurgically (conservative treatment) or surgically. Surgical decompression is generally acceptable for neurologically compromised patients but is highly controversial in those without neurological damage. Although nonoperative treatment could provide promising clinical outcomes, some clinical reports have showed that surgical treatment achieved better fracture reduction and long-term results.[3,4]
Posterior short-segment pedicle screw fixation (one level above and one level below the fracture level) is most widely used for TL fractures around the world, which can provide immediate spinal stability, improved correction of kyphotic deformities, early painless mobilization, and indirect decompression of the spinal canal. However, many authors reported that short-segment pedicle screw instrumentation was not adequate to achieve and maintain the reduction of TL fractures and associated with an unacceptable rate of failure.[5–7]
Since a study of pedicle screw fixation at fractured vertebrae was first reported in 1994, a series of biomechanical studies[8–11] also showed that pedicle screw fixation combined with screws at the fractured vertebrae could significantly improve the spinal stability and decrease the stress of pedicle screws in the upper and lower normal vertebrae. The similar advantages have also been reported for treatment of TL fractures, however, the evidence is mainly limited to low-quality observational studies.[12–14] Furthermore, randomized controlled trials of high quality and long term follow-up on the pedicle screw fixation combined with the intermediate screw at the fracture level for TL fractures have not been well established, further limiting the evidence available for this technique.
Therefore, in the present study, we conducted a systematic meta-analysis from published studies to estimate the clinical, functional, and radiological outcomes of pedicle screw fixation combined with intermediate screw at the fractured vertebrae for TL fractures.
2. Methods
This meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Ethical approval was not necessary as our study did not involve any patient intervention or information.
2.1. Literature search strategy
We conducted electronic searches using PubMed, Medline, Embase, Cochrane Central Register of Controlled Trials (CCTR), and Cochrane Database of Systematic Reviews (CDSR), from their date of inception to December 2015. To achieve the maximum sensitivity of the search strategy, the following key words were used for search with various combinations of the operators “AND,” “NOT,” and “OR”: “thoracolumbar fracture,” “lumbar fracture,” “intermediate screw,” “additional screw,” “index level,” “fracture vertebrae,” “fracture level,” and “six screws.” In addition, the reference lists of all retrieved articles were reviewed for further identification of potentially relevant studies. We restricted the language to English.
2.2. Selection criteria
Studies were included in this meta-analysis only if they were comparative trials comparing pedicle screw fixation combined with intermediate screw at the fracture level versus conventional pedicle screw fixation for treatment of TL fractures. A manual search was conducted to acquire more relevant studies from original studies and reviews. All studies were included when they involved human subjects. Abstracts, case reports, conference presentations, editorials, reviews, and expert opinions were excluded. For repeated papers or literature containing the same population data, only the one with longest follow-up and most complete information was included.
2.3. Data extraction and critical appraisal
A standardized form was used to record name of first author, study period, country of study, sample size within each group, indication, and follow-up time. The postoperative Cobb angle and anterior vertebral height (AVH), correction loss of Cobb angle and AVH, and complication rate including implant failure were used as the primary outcomes. The secondary outcomes included operative time, blood loss, and clinical outcome. Visual analogue scale (VAS) for back pain was used to assess clinical outcome. Two researchers independently reviewed literature for data extraction. Any disagreement between the 2 reviewers was resolved by thorough discussions.
2.4. Quality evaluation
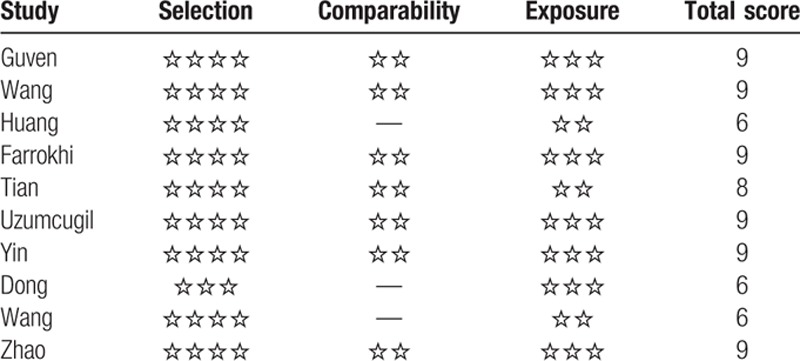
We evaluated the quality of the included studies using Newcastle–Ottawa Scale (NOS). Studies were graded according to the following 3 categories with 8 items: the selection of the study cases (4 items), the comparability of the study populations (1 item), and the ascertainment of either the exposure or outcome of interest (3 items). Nine stars were the highest value for quality assessment. Studies that had a score of 0 to 3, 4 to 6, and 7 or more stars were classified to be of poor, moderate, and high quality, respectively.[15]
2.5. Statistical analysis
Review Manager Version 5.3.5 (Cochrane Collaboration, Oxford, UK) was used for all data analysis. The odds ratio (OR) and weighted mean difference (WMD) were used as a summary statistic to analyze dichotomous and continuous variables, respectively. Both were reported with 95 % confidence intervals (CIs), and a P value lower than 0.05 or a 95% CI that did not contain unity was considered statistically significant. In the present meta-analysis, both fixed- and random-effect models were employed. Since similar results were obtained, only results of the random-effect model are presented. I2 test was used to evaluate the heterogeneity, where the values greater than 50% implied heterogeneity.
3. Results
3.1. Literature search
The literature search from electronic databases identified 287 articles. The literature search procedure is shown in Fig. 1. After application of the inclusion and exclusion criteria, 10 comparative studies were finally included in the present systematic review and meta-analysis, including 4 randomized controlled studies and 6 observational studies (Table 1). Of the 10 studies, there were 5 prospective studies[12,16–19] and 5 retrospective studies.[13,14,20–22] A total of 283 patients who underwent pedicle screw fixation combined with the intermediate screw at the fracture level were compared with 285 patients who underwent conventional pedicle screw fixation. In all studies, TL fractures were the primary indication for pedicle screw fixation. Follow-up for the included studies ranged from 6 to 84 months. As shown in Table 2, all of the included articles had high quality as they got 6 or more stars.
Figure 1.
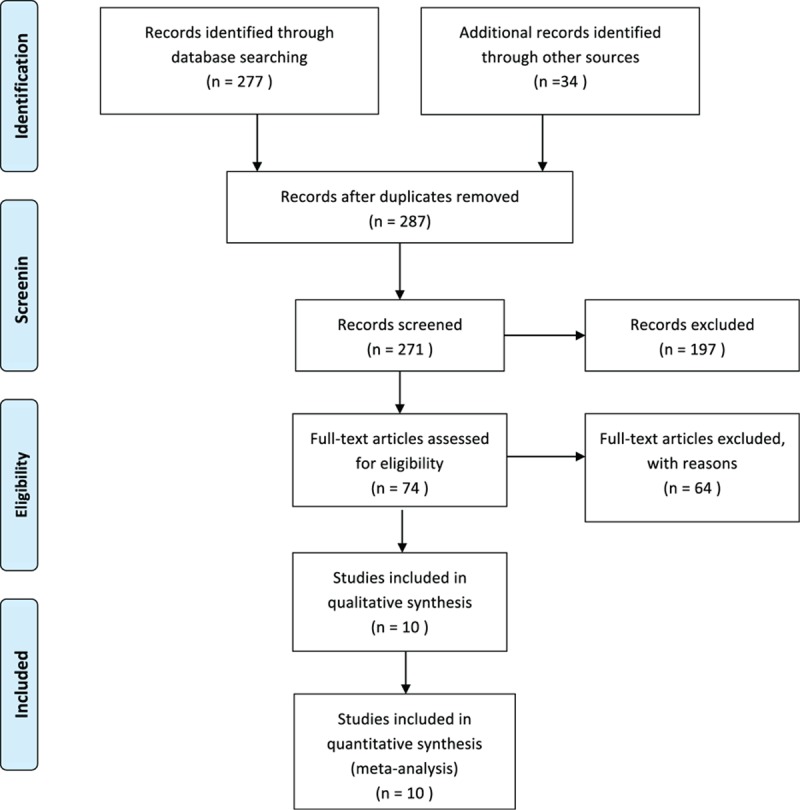
The procedure of literature search.
Table 1.
Study characteristics.
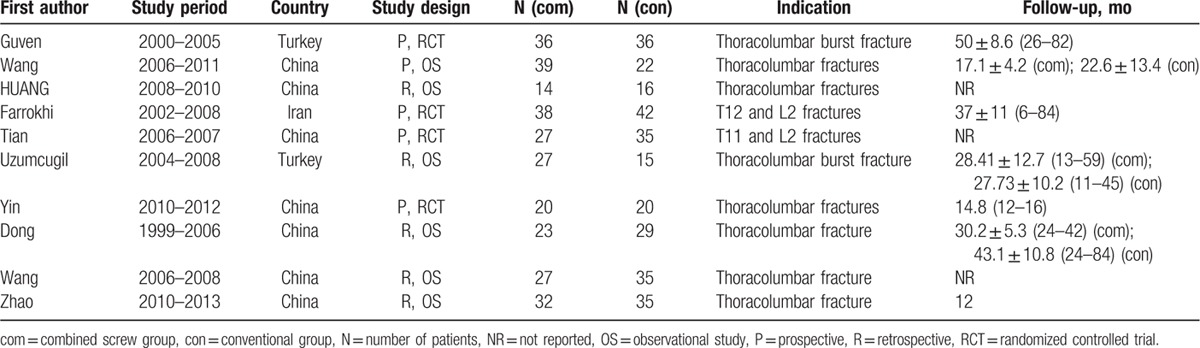
Table 2.
Methodological quality of included studies in the meta-analysis.
3.2. Operative parameters
Operation time for the combined screw and conventional groups was reported in 6 included studies. No difference was found in terms of operative duration between the combined and conventional cohorts (WMD, 4.65 minutes; 95% CI, −5.36, 14.67; I2 = 88%; P = 0.36). Significant heterogeneity was detected for this outcome (P < 0.00001; Fig. 2). Intraoperative blood loss was a little lower in the conventional fixation cohort versus combined screw fixation (WMD, 12.91 mL; 95% CI, 2.22, 23.60; I2 = 7%; P = 0.02; Fig. 3).
Figure 2.
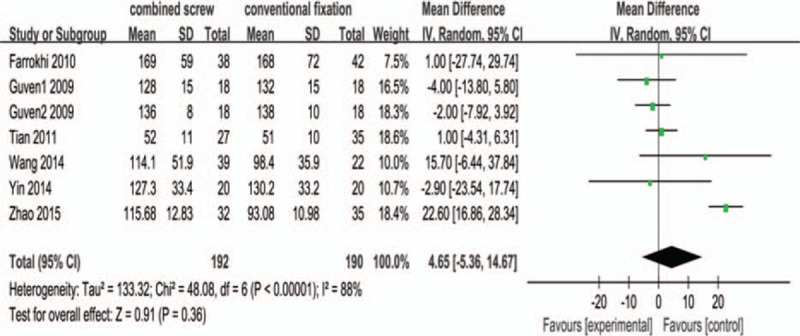
Forest plot comparing operation time for combined screw fixation versus conventional screw fixation. CI = confidence interval, IV = inverse variance, SD = standard deviation.
Figure 3.
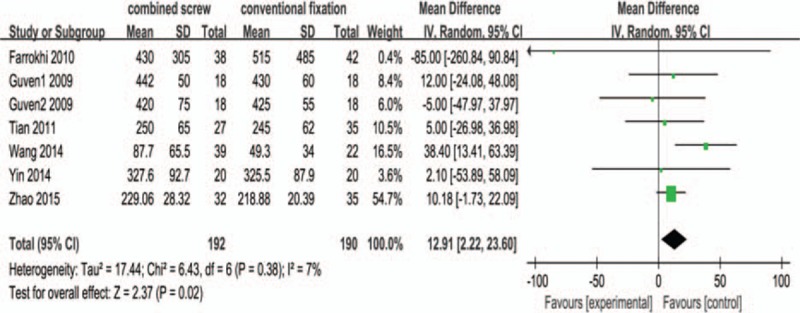
Forest plot comparing intraoperative blood loss for combined screw fixation versus conventional screw fixation. CI = confidence interval, IV = inverse variance, SD = standard deviation.
3.3. Clinical outcomes
Postoperative VAS outcomes for back pain were reported in 5 studies. Postoperative VAS scores were demonstrated to be equally better between the combined fixation cohort and the conventional fixation group (WMD, −0.21; 95% CI, −0.44, 0.01; I2 = 0%; P = 0.06). No heterogeneity was detected for this outcome (P = 0.44; Fig. 4).
Figure 4.

Forest plot comparing visual analogue scale (VAS) for combined screw fixation versus conventional screw fixation. CI = confidence interval, IV = inverse variance, SD = standard deviation.
3.4. Radiological outcomes
Similarly to previous studies, both combined screw fixation and conventional fixation techniques were able to significantly correct all monitored radiological parameters. Postoperative Cobb angle was demonstrated to be significantly better in the combine screw cohort compared with the conventional fixation group (WMD, −1.88; 95% CI, −3.00, −0.75; I2 = 77%; P = 0.001; Fig. 5).
Figure 5.
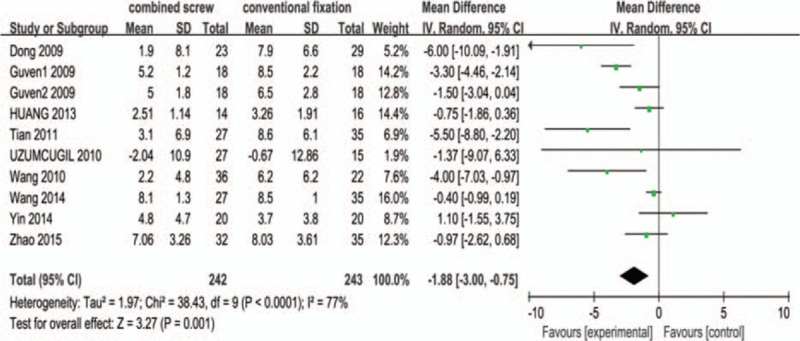
Forest plot comparing Cobb angle for combined screw fixation versus conventional screw fixation. CI = confidence interval, IV = inverse variance, SD = standard deviation.
Postoperative AVH was reported in 7 studies and postoperative anterior vertebrae height compression (AVHC) in the other 2 studies. Postoperative AVH was significantly better in the combined screw group versus conventional fixation (WMD, 6.14; 95% CI, 0.04, 12.23; I2 = 94%; P = 0.05). Similar trends were also seen for postoperative AVHC, which was significantly lower in the combined screw cohort (WMD, −2.48; 95% CI, −3.39, −1.58; I2 = 32%; P < 0.00001). The pooled analysis showed significant improvement in terms of AVH in the combined screw group compared with the conventional fixation (Fig. 6).
Figure 6.
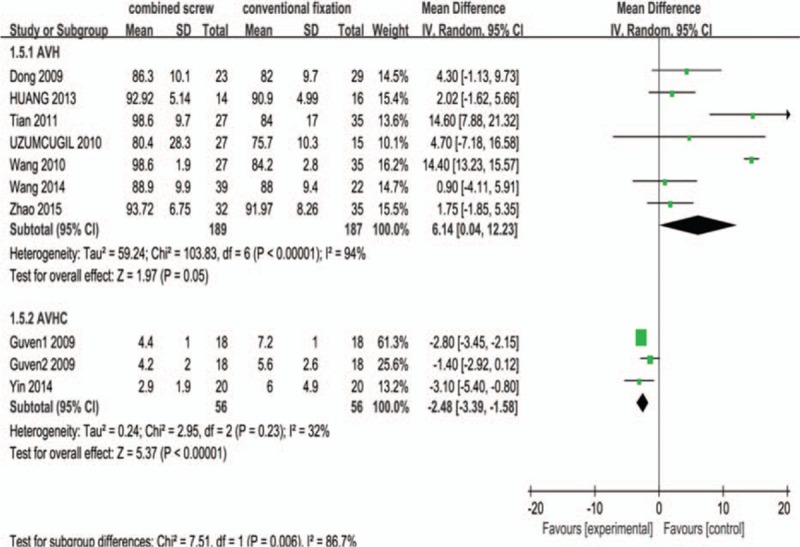
Forest plot comparing anterior vertebral height (AVH) and anterior vertebrae height compression (AVHC) for combined screw fixation versus conventional screw fixation. CI = confidence interval, IV = inverse variance, SD = standard deviation.
The correction losses of the Cobb angle and AVH in the last follow-up were provided in the 7 studies. Compared with the conventional fixation group, the correction loss of Cobb angle and AVH was demonstrated to be significantly less in the combined screw cohort (Cobb angle: WMD, −1.62; 95% CI, −2.39, −0.85; I2 = 51%; P < 0.0001. AVH: WMD, −2.38; 95% CI, −3.53, −1.24; I2 = 74%; P < 0.0001). However, these outcomes were heterogeneous (Cobb angle: P = 0.05; AVH: P = 0.0003; Figs. 7 and 8).
Figure 7.
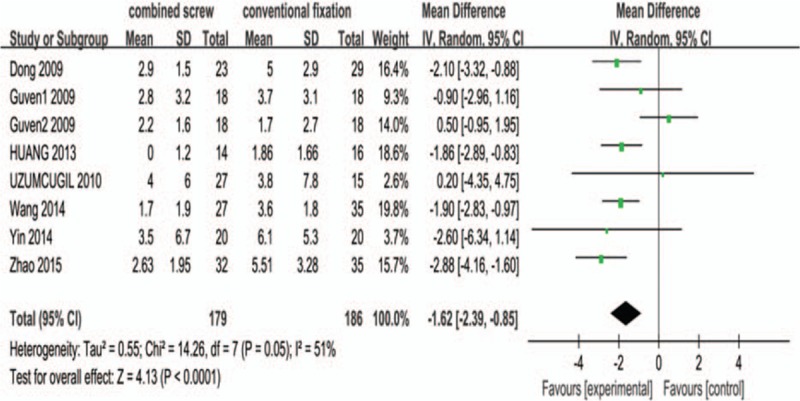
Forest plot comparing correction loss of Cobb angle for combined screw fixation versus conventional screw fixation. CI = confidence interval, IV = inverse variance, SD = standard deviation.
Figure 8.

Forest plot comparing correction loss of anterior vertebral height (AVH) for combined screw fixation versus conventional screw fixation. CI = confidence interval, IV = inverse variance, SD = standard deviation.
3.5. Complications
The primary complication reported commonly amongst the studies was limited to implant failure including breakage and loosening of the pedicle screws or the rods. Other complications included wound infection and thrombosis. Implant failure rates were reported in 4 included studies. Implant failure rates were demonstrated to be significantly lower in the combined screw fixation cohort, with 2 complications in the combined screw group versus 15 total failures in the conventional cohort (1.5% vs 11.7%; OR, 0.19; 95% CI, 0.06, 0.62; I2 = 0%; P = 0.006). There was no significant difference in other complications rate (6.0% vs 9.3%; OR, 0.69; 95% CI, 0.23, 2.04; I2 = 0%; P = 0.50; Fig. 9). No deaths and neurological complications attributed to pedicle screw fixation were reported in the included studies.
Figure 9.
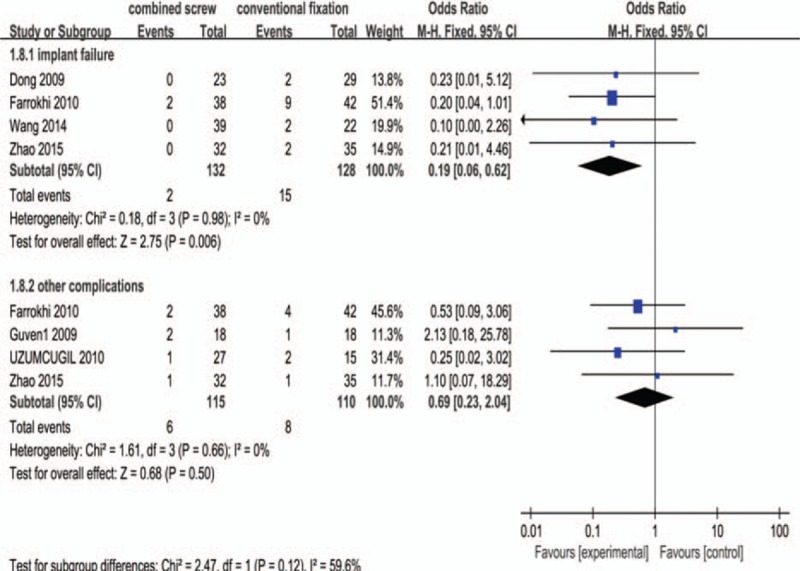
Forest plot comparing complication rates for combined screw fixation versus conventional screw fixation. CI = confidence interval, M–H = Mantel–Haenszel.
4. Discussion
As we know, this is the first meta-analysis of comparative studies on the pedicle screw combined with intermediate screw at the fracture level versus conventional pedicle screw fixation techniques for TL fractures. From the available data, this meta-analysis showed that the combined screw technique was associated with better reduction and less correction loss of fractured vertebrae, similar operation time, a little more intraoperative blood loss, and equal VAS clinical outcome when compared with the conventional fixation technique.
Since Dick et al[23] first conducted the biomechanical studies of pedicle screw fixation at fractured vertebrae in 1994, the technique has evolved, and it has been demonstrated that the addition of intermediate screws at the fractured vertebrae can achieve stronger fixation and less loss of reduction compared with conventional pedicle screw fixation. The clinical application of pedicle screw at the fractured vertebrae for TL fractures turns into a controversial issue due to the limited evidence available. Later, there were some in vitro biomechanical studies on the pedicle screw at the fracture level,[8,9,24] whose results showed that it could clearly improve the stability of pedicle screw fixation system and decrease the stress distribution on each pedicle screw. Some authors[17,25,26] also suggested that pedicle screw fixation combined with intermediate screw at the fractured vertebrae improved biomechanical stability and achieved better reduction, less correction loss, fewer instrument failures, and comparable or better clinical outcomes. Conversely, Hakalo and Wronski[27] considered that pedicle screw insertion into the fractured vertebra did not effectively increase the spinal axial bearing capacity and initial stability, thus it could not reduce the postoperative correction loss and failure rate of internal fixation. Therefore, we performed a meta-analysis to compare systematically the efficacy and safety between the 2 techniques.
VAS was used for evaluating clinical outcome in this study. Our review showed no difference in VAS scores between the 2 groups postoperatively. This indicated that addition of intermediate screws at the fractured vertebrae would not increase the postoperative pain of patients. However, it is noteworthy that the VAS scores evaluation is more dependent on the subjective experience of patients and the scores may be acquired variably by different investigators. Hence, the reliability of the results was investigated and the conclusions were consistent following sensitivity analysis.
The results of the present review confirm previously reported advantages of the combined screw fixation compared with conventional fixation technique. The pedicle screw fixation combined with the screw at the fractured vertebrae could achieve better correction of kyphotic angle and the height of the injured vertebrae postoperatively, and reduce the correction loss at the follow-up. The combined screw fixation technique requires insertion of 1 or 2 pedicle screws into the fractured vertebrae, which can produce a forward driving force to enhance the reduction and reshaping, and can be used to directly raise the end plate to assist in the restoration of the compressed vertebral height.[25,28] In previous studies, some authors[17,19] reported that placement of pedicle screws into the fractured vertebrae could lead to better kyphosis correction, and others[12] showed that it could more effectively restore the height of the fractured vertebrae. Whereas our study demonstrated that the combined screw fixation technique could both effectively correct the kyphotic deformity and restore the height of the fractured vertebrae.
Complication is a very important factor for assessing surgical safety and a low rate of complications was reported amongst the included studies. In the published literature, there has been inconsistent rate of pedicle screw breakage and loosening reported. Our review showed that the incidence of implant failure was significantly lower in the combined screw fixation group (combined screw fixation vs conventional fixation: 1.5% vs 11.7%), and statistical difference was detected between the 2 groups (P = 0.007). This is likely explained by the notion that the combined screw at the fractured vertebrae could significantly improve the stress distribution of screws, reduce screw load, and provide a fulcrum for the reduction to make it coincide with the mechanical mechanism, so as to significantly improve its antistress ability and enhance the stability of the fixation.[13,29] It is also important to note that implant failure rates may vary depending on their follow-up periods. Other complications rates were not significantly different between the 2 groups. This result is not surprising because of similar operation duration and surgical trauma in the 2 groups.
We also took the results of operation time and intraoperative blood loss for evaluating surgical trauma in this study. The results showed that there was no statistical difference in aspects of the operation time between the 2 groups, which suggested that the additional screws at the fracture level would not increase the operation time and surgical trauma. However, the intraoperative blood loss in the conventional fixation group was less compared with the combined screws fixation group, and significant difference was observed between the 2 groups. We consider that the insertion of pedicle screw caused outflow of the hematocele within the fractured vertebral body, and then increased the intraoperative blood loss. Additionally, only one minimally invasive study of the current review reported that significant difference in the intraoperative blood loss was observed between 2 groups. During the process of sensitivity analysis, I2 decreased to 0% from 7% and no significant difference in terms of intraoperative blood loss was observed between the 2 groups when this study was excluded. We concluded that our study was heterogeneous, and the heterogeneity derived from the percutaneous approach different from open approach.
Meta-analysis uses quantitative methods to combine the data collected from several independent researches and surveys on the same problem, pooling outcomes to arrive at a more unbiased and scientific conclusion.[30] There are some limitations to our meta-analysis. Firstly, of the 10 available studies, only 4 randomized controlled trials were included, which led to the data of low quality given the nonrandomized design of most studies. Secondly, the level and type of fracture and surgical approach adopted by different surgeon (i.e., percutaneous or open approach) may cause clinical heterogeneity in various treatment centers, and in most studies, results were combined together with no stratification. Thirdly, the patient sample was small, which may be unable to detect true complication rates. Finally, the data were limited to English-language articles and the majority of studies came from the same country, which may cause language and demography bias.
5. Conclusion
This study only concentrated on the operative parameters, clinical and radiological outcomes, and complications between the 2 groups. The combined screw fixation technique was associated with better reduction of the fractured vertebrae, less correction loss in the follow-up, and lower implant failure rate. Given the lack of robust clinical evidence, these findings warrant verification in large prospective registries and randomized trials with long-term follow-up.
Footnotes
Abbreviations: AVH = anterior vertebral height, AVHC = anterior vertebrae height compression, CCTR = Cochrane Central Register of Controlled Trials, CDSR = Cochrane Database of Systematic Reviews, CI = confidence interval, NOS = Newcastle–Ottawa Scale, OR = odds ratio, SD = standard deviation, TL = thoracolumbar, VAS = visual analogue scale, WMD = weighted mean difference.
The authors have no conflicts of interest to disclose.
References
- 1.Leucht P, Fischer K, Muhr G, et al. Epidemiology of traumatic spine fractures. Injury 2009; 40:166–172. [DOI] [PubMed] [Google Scholar]
- 2.Tian Y, Zhu Y, Yin B, et al. Age- and gender-specific clinical characteristics of acute adult spine fractures in China. Int Orthop 2016; 40:347–353. [DOI] [PubMed] [Google Scholar]
- 3.Siebenga J, Leferink VJ, Segers MJ, et al. Treatment of traumatic thoracolumbar spine fractures: a multicenter prospective randomized study of operative versus nonsurgical treatment. Spine 2006; 31:2881–2890. [DOI] [PubMed] [Google Scholar]
- 4.Ni WF, Huang YX, Chi YL, et al. Percutaneous pedicle screw fixation for neurologic intact thoracolumbar burst fractures. J Spinal Disord Tech 2010; 23:530–537. [DOI] [PubMed] [Google Scholar]
- 5.Wood KB, Bohn D, Mehbod A. Anterior versus posterior treatment of stable thoracolumbar burst fractures without neurologic deficit: a prospective, randomized study. J Spinal Disord Tech 2005; 18 (supp l):S15–S23. [DOI] [PubMed] [Google Scholar]
- 6.McLain RF, Sparling E, Benson DR. Early failure of short-segment pedicle instrumentation for thoracolumbar fractures. A preliminary report. J Bone Joint Surg Am 1993; 75:162–167. [DOI] [PubMed] [Google Scholar]
- 7.Scholl BM, Theiss SM, Kirkpatrick JS. Short segment fixation of thoracolumbar burst fractures. Orthopedics 2006; 29:703–708. [DOI] [PubMed] [Google Scholar]
- 8.Baaj AA, Reyes PM, Yaqoobi AS, et al. Biomechanical advantage of the index-level pedicle screw in unstable thoracolumbar junction fractures. J Neurosurg Spine 2011; 14:192–197. [DOI] [PubMed] [Google Scholar]
- 9.Norton RP, Milne EL, Kaimrajh DN, et al. Biomechanical analysis of four- versus six-screw constructs for short-segment pedicle screw and rod instrumentation of unstable thoracolumbar fractures. Spine J 2014; 14:1734–1739. [DOI] [PubMed] [Google Scholar]
- 10.Wang H, Li C, Liu T, et al. Biomechanical efficacy of monoaxial or polyaxial pedicle screw and additional screw insertion at the level of fracture, in lumbar burst fracture: an experimental study. Indian J Orthop 2012; 46:395–401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bolesta MJ, Caron T, Chinthakunta SR, et al. Pedicle screw instrumentation of thoracolumbar burst fractures: biomechanical evaluation of screw configuration with pedicle screws at the level of the fracture. Int J Spine Surg 2012; 6:200–205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Tian JW, Wang L, Xia T, et al. Posterior short-segmental fixation combined with intermediate screws vs conventional intersegmental fixation for monosegmental thoracolumbar fractures. Orthopedics 2011; 34:e389–e396. [DOI] [PubMed] [Google Scholar]
- 13.Huang W, Luo T. Efficacy analysis of pedicle screw internal fixation of fractured vertebrae in the treatment of thoracolumbar fractures. Exp Ther Med 2013; 5:678–682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Zhao QM, Gu XF, Yang HL, et al. Surgical outcome of posterior fixation, including fractured vertebra, for thoracolumbar fractures. Neurosciences (Riyadh) 2015; 20:362–367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ma Z, Guo F, Qi J, et al. Meta-analysis shows that obesity may be a significant risk factor for prosthetic joint infections. Int Orthop 2016; 40:659–667. [DOI] [PubMed] [Google Scholar]
- 16.Guven O, Kocaoglu B, Bezer M, et al. The use of screw at the fracture level in the treatment of thoracolumbar burst fractures. J Spinal Disord Tech 2009; 22:417–421. [DOI] [PubMed] [Google Scholar]
- 17.Farrokhi MR, Razmkon A, Maghami Z, et al. Inclusion of the fracture level in short segment fixation of thoracolumbar fractures. Eur Spine J 2010; 19:1651–1656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Yin F, Sun Z, Yin Q, et al. A comparative study on treatment of thoracolumbar fracture with injured vertebra pedicle instrumentation and cross segment pedicle instrumentation. Zhongguo xiu fu chong jian wai ke za zhi 2014; 28:227–232. [PubMed] [Google Scholar]
- 19.Wang H, Zhou Y, Li C, et al. Comparison of open versus percutaneous pedicle screw fixation using the sextant system in the treatment of traumatic thoracolumbar fractures. Clin Spine Surg 2014; [Epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- 20.Dong JW, Rong LM, Liu B, et al. [Additional screws fixation on fractured vertebrae versus only short-segment posterior instrumentation for thoracolumbar A3 fracture without neurologic deficit]. Zhonghua wai ke za zhi 2009; 47:1883–1887. [PubMed] [Google Scholar]
- 21.Uzumcugil O, Dogan A, Yetis M, et al. Results of ‘two above- one below approach’ with intermediate screws at the fracture site in the surgical treatment of thoracolumbar burst fractures. Kobe J Med Sci 2010; 56:E67–E78. [PubMed] [Google Scholar]
- 22.Wang L, Xia T, Tian JW, et al. [Treatment of thoracolumbar mono-segmental fracture with posterior short-segment fixation in combination with intermediate screws: a short-term outcome]. Zhonghua yi xue za zhi 2010; 90:886–889. [PubMed] [Google Scholar]
- 23.Dick JC, Jones MP, Zdeblick TA, et al. A biomechanical comparison evaluating the use of intermediate screws and cross-linkage in lumbar pedicle fixation. J Spinal Disord 1994; 7:402–407. [PubMed] [Google Scholar]
- 24.Anekstein Y, Brosh T, Mirovsky Y. Intermediate screws in short segment pedicular fixation for thoracic and lumbar fractures: a biomechanical study. J Spinal Disord Tech 2007; 20:72–77. [DOI] [PubMed] [Google Scholar]
- 25.Mahar A, Kim C, Wedemeyer M, et al. Short-segment fixation of lumbar burst fractures using pedicle fixation at the level of the fracture. Spine 2007; 32:1503–1507. [DOI] [PubMed] [Google Scholar]
- 26.Gelb D, Ludwig S, Karp JE, et al. Successful treatment of thoracolumbar fractures with short-segment pedicle instrumentation. J Spinal Disord Tech 2010; 23:293–301. [DOI] [PubMed] [Google Scholar]
- 27.Hakalo J, Wronski J. Complications of a transpedicular stabilization of thoraco-lumbar burst fractures. Neurologia i neurochirurgia polska 2006; 40:134–139. [PubMed] [Google Scholar]
- 28.Shen WJ, Liu TJ, Shen YS. Nonoperative treatment versus posterior fixation for thoracolumbar junction burst fractures without neurologic deficit. Spine 2001; 26:1038–1045. [DOI] [PubMed] [Google Scholar]
- 29.Lehman RA, Jr, Lenke LG, Keeler KA, et al. Computed tomography evaluation of pedicle screws placed in the pediatric deformed spine over an 8-year period. Spine 2007; 32:2679–2684. [DOI] [PubMed] [Google Scholar]
- 30.Xiao SW, Jiang H, Yang LJ, et al. Comparison of unilateral versus bilateral pedicle screw fixation with cage fusion in degenerative lumbar diseases: a meta-analysis. Eur Spine J 2015; 24:764–774. [DOI] [PubMed] [Google Scholar]