

Abstract
AIM
To examine the effects of cognitive remediation therapies on brain functioning through neuroimaging procedures in patients with schizophrenia.
METHODS
A systematic, computerised literature search was conducted in the PubMed/Medline and PsychInfo databases. The search was performed through February 2016 without any restrictions on language or publication date. The search was performed using the following search terms: [(“cogniti*” and “remediation” or “training” or “enhancement”) and (“fMRI” or “MRI” or “PET” or “SPECT”) and (schizophrenia or schiz*)]. The search was accompanied by a manual online search and a review of the references from each of the papers selected, and those papers fulfilling our inclusion criteria were also included.
RESULTS
A total of 101 studies were found, but only 18 of them fulfilled the inclusion criteria. These studies indicated that cognitive remediation improves brain activation in neuroimaging studies. The most commonly reported changes were those that involved the prefrontal and thalamic regions. Those findings are in agreement with the hypofrontality hypothesis, which proposes that frontal hypoactivation is the underlying mechanism of cognitive impairments in schizophrenia. Nonetheless, great heterogeneity among the studies was found. They presented different hypotheses, different results and different findings. The results of more recent studies interpreted cognitive recovery within broader frameworks, namely, as amelioration of the efficiency of different networks. Furthermore, advances in neuroimaging methodologies, such as the use of whole-brain analysis, tractography, graph analysis, and other sophisticated methodologies of data processing, might be conditioning the interpretation of results and generating new theoretical frameworks. Additionally, structural changes were described in both the grey and white matter, suggesting a neuroprotective effect of cognitive remediation. Cognitive, functional and structural improvements tended to be positively correlated.
CONCLUSION
Neuroimaging studies of cognitive remediation in patients with schizophrenia suggest a positive effect on brain functioning in terms of the functional reorganisation of neural networks.
Keywords: Cognitive remediation, Cognitive training, Neuroimaging, Cognition, Prefrontal cortex, Thalamus, Plasticity, Schizophrenia
Core tip: Cognitive remediation therapy for schizophrenia is an evidence-based psychological treatment that aims to improve cognitive dysfunction. However, its underlying neural mechanisms have not been established. Several neuroimaging studies have shown positive effects in terms of brain activation. However, the results have been heterogeneous and difficult to integrate. The primary aim of the present review was to analyse systematically all of the published trials that used neuroimaging procedures. Additionally, we performed a more qualitative analysis examining the possible influence of neuroimaging methods and the use of different theoretical frameworks.
INTRODUCTION
Cognitive remediation therapy for schizophrenia is a psychological treatment that proposes to ameliorate cognitive dysfunction. It has been defined as a behavioural training-based intervention that aims to improve cognitive processes (attention, memory, executive function, social cognition or metacognition) with the goal of durability and generalisation[1]. Although the described effects have been modest, several trials and two meta-analyses have established its efficacy, improving not only cognition but also daily functioning[1,2]. Nonetheless, the underlying neural mechanisms of this treatment have not yet been well established.
Over the past few years, several neuroimaging studies have been conducted with the intention of identifying the different brain mechanisms underlying cognitive recovery. Some positive effects in terms of brain activation have been described, although the results have been heterogeneous[3,4]. Owing to this heterogeneity among the studies presenting different hypotheses, different results and different findings, we understand the need to review systematically all of the published works to provide new insights that would help to generate a new hypothesis in the near future. Moreover, recent revisions in the field of neuroimaging have indicated the need to explore not only the results but also the methods and theoretical frameworks[5].
The objective of the present review was to analyse neuroimaging studies that have tested the effects of cognitive remediation on brain functioning in patients with schizophrenia. To do so, we systematically reviewed published trials that used a cognitive remediation treatment and neuroimaging procedures. Additionally, we performed a more qualitative analysis examining the possible influence of neuroimaging methods and the use of different theoretical frameworks.
MATERIALS AND METHODS
Literature search
A systematic, computerised literature search was conducted in different online scientific databases: PubMed/Medline and PsychInfo. The search was performed through February 2016 without any restrictions on language or publication date. The search was performed using the following search terms: [(“cogniti*” and “remediation” or “training” or “enhancement”) and (“fMRI” or “MRI” or “PET” or “SPECT”) and (schizophrenia or schiz*)]. This search was accompanied by a manual online search and review of the references from each of the papers selected, and those papers fulfilling our inclusion criteria were also included.
The following inclusion criteria were applied. Studies in which any imaging technique was used to assess the effect of cognitive training were selected. Assessments had to be conducted both at baseline and also after therapy. We excluded those articles that did not report any results, for instance, presentations or descriptions of interventions or study designs. Regarding the intervention, we only included studies in which patients were provided with multiple sessions of cognitive training, and programmes focusing only on social cognition were excluded.
RESULTS
In total 101, studies were obtained, and 18 of them fulfilled the inclusion criteria (Figure 1). In addition to the differences in neuroimaging variables that will be analysed in subsequent paragraphs, an important heterogeneity in the characteristics of the retrieved studies was found (Table 1). Cognitive intervention approaches frequently differed among the studies, ranging from paper and pencil tasks, computerised cognitive training, training delivered in group format or individualised sessions with a therapist, simple auditory training, multimodal training and so on. The duration of the therapies ranged from less than one week to two complete years, with the mean duration of the training being 12.47 wk and 11 studies (64.7%) being between 10 and 16 wk in length. In addition, the cognitive remediation approaches focused on a single cognitive function to others focusing on all cognitive aspects possible, including social cognition. Because of the heterogeneity of the methodologies, interventions and assessments, we decided to rely on a qualitative description rather than a quantitative analysis.
Figure 1.
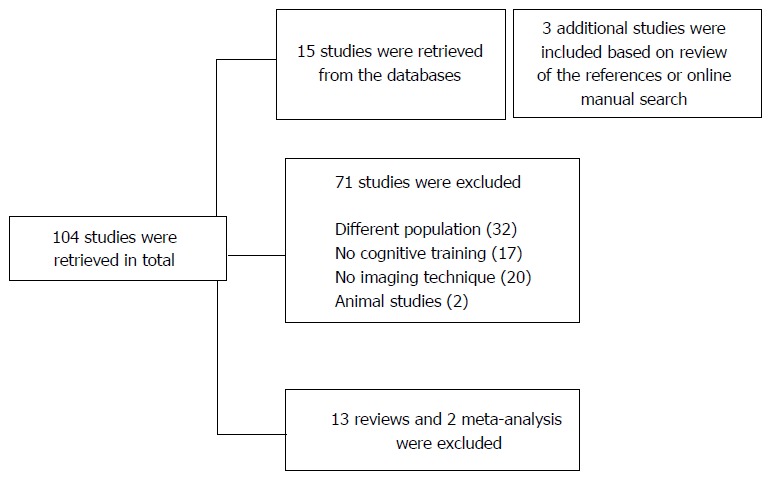
Diagram of literature search.
Table 1.
Studies included in the systematic review
| Ref. | Participants | Treatment | Treatment duration (wk) | Imaging method | Experimental task | Neural treatment effects | Direction of change |
| Cognitive remediation | |||||||
| Wykes et al[8] | SCH = 2 | CRT | 12 | SPECT | Verbal fluency | Bilateral frontal, temporal, parietal and occipital | ↑ |
| Penadés et al[9] | SCH = 2 | CRT | 12 | SPECT | Tower of London | Prefrontal activity | ↑ |
| Wexler et al[11] | SCH = 8 | CRT | 10 | fMRI | Auditory verbal memory | L inferior frontal | ↑ |
| Penadés et al[10] | SCH = 8 | CRT | 12 | SPECT | Tower of London | Prefrontal activity | ↑ |
| Wykes et al[12] | SCH = 12 HC =6 | CRT OC HC | 12 | fMRI | N-back | R inferior frontal gyrus and bilateral occipital activity | ↑ |
| Eack et al[20] | SCH = 53 | CET EST | 52 | MRI | - | Loss of GM in temporal cortex, including the L parahippocampal gyrus, L amygdala, bilateral anterior cingulate, and L hippocampus | ↓ |
| GM in L amygdala | ↑ | ||||||
| Haut et al[13] | SCH = 21 HC = 9 | CRT CBSST | 6 | fMRI | N-back, lexical task | L prefrontal activity | Case report series |
| Rowland et al[15] | SCH = 17 HC = 17 | CRT | < 1 | fMRI, VBM | L amygdala, bilateral inferior parietal regions | ↑ | |
| Controls also exhibited activation reductions in region and spatial extent with relational learning proficiency | ↓ | ||||||
| Edwards et al[14] | SCH = 22 HC = 14 | CRT | 22 | fMRI | Continuous performance task | R middle frontal R superior parietal cortex R inferior frontal junction R visual cortex Cerebellum | ↑↓ |
| Bor et al[16] | SCH = 20 HC = 15 | CRT | 8 | fMRI | N-back | L inferior/middle frontal gyrus, cingulate gyrus and inferior parietal lobule activity | ↑ |
| Subramaniam et al[19] | SCH = 31 HC = 16 | AT | 13 | fMRI | Word generation and recognition | Medial PFC activity | ↑ |
| Penadés et al[21] | SCH = 31 HC = 16 | CRT SST | 15 | fMRI, DTI | N-back | L superior parietal lobule and bilateral middle frontal gyri activity | ↑ |
| DMN activity in L precuneus and middle frontal gyrus | ↓ | ||||||
| FA in CC and R posterior thalamic radiations | ↑ | ||||||
| Vianin et al[22] | SCH = 16 | CRT | 8 | fMRI | Verbal fluency | Inferior parietal lobule, precentral gyrus, Broca’s area, middle occipital cortex, middle cingulate cortex, and superior parietal lobule activity | ↑ |
| Subramaniam et al[23] | HC = 15 SCH = 30 | AT | 15 | fMRI | N-back | Middle frontal and inferior frontal gyri activity | ↑ |
| Social-cognitive remediation | |||||||
| Haut et al[13] | SCH = 20 HC = 10 | TAR TAU | 10 | fMRI | Facial affect recognition | L middle and superior occipital lobe, R inferior and superior parietal cortex, and L and R inferior frontal cortex activity | ↑ |
| Combination of cognitive and social-cognitive remediation | |||||||
| Hooker et al[17] | SCH = 22 | AT + SCT | 11 | fMRI | Facial emotion recognition | Postcentral gyrus activity | ↑ |
| Hooker et al[18] | SCH = 22 | AT + SCT | 11 | fMRI | Facial emotion recognition | L and R amygdala, R putamen and R medial prefrontal cortex | ↑ |
SPECT: Single photon emission computed tomography; fMRI: Functional magnetic resonance imaging; GM: Grey matter; DMN: Default mode network; FA: Fractional anisotropy; CC: Corpus callosum; AT: Auditory-based cognitive training; SCT: Social cognitive training; SCH: Schizophrenia; HC: Healthy control.
First period: Improving brain activation
The first studies performed in the 1990s seemed to be inspired by the simple assumption that cognitive remediation would be able to cause some detectable effects on brain functioning. Thus, any visible changes in brain functioning would be considered a success. During that period, the use of functional neuroimaging techniques, such as positron emission tomography (PET) and single photon emission computed tomography (SPECT) procedures, were predominant. Both procedures helped to establish the hypothesis of hypofrontality. Hypofrontality was defined as a state of decreased cerebral blood flow or reduced utilisation of glucose in the prefrontal cortex of the brain[6,7]. Thus, testing cognitive remediation with PET or SPECT was the best option for researchers, more specifically in the context of the hypothesis of hypofrontality using analysis of regions of interest (ROIs), in this case, the prefrontal cortex. Thus, any detectable change in terms of brain activation indicating any sort of reduction of the hypofrontality would be proof that cognitive remediation was working well.
Thus, the first study to test the effects of cognitive remediation through SPECT procedures was performed by Wykes et al[8], who reported that two patients showed changes in frontal perfusion patterns after cognitive treatment. Penadés et al[9] found similar results, describing an increase in prefrontal blood flow during task performance following cognitive treatment in a case report study including two patients. These results were extended and confirmed in a later study with a small sample of eight patients[10]. However, two intriguing aspects from these studies raised questions that remain open. Firstly, not only increases but also decreases in the activation of some specific brain regions could be related to cognitive improvement. In the Wykes et al[8], not only increased but also decreased activity was found in the bilateral frontal, temporal, parietal and occipital regions. Secondly, another open question is the variables that could explain the intersubject variability, preventing the success of cognitive remediation in some patients. In a study by Penadés et al[9] with two patients, one had clearly improved prefrontal brain activation, while no significant changes were found in the other patient. Nonetheless, despite these and other possible open questions, this initial period offered promising results that were able to establish the idea that cognitive remediation is able to improve brain activation and eventually reduce hypofrontality. This line of thought was applied by Wexler et al[11] using a different methodology: Functional magnetic resonance imaging (fMRI). They described in a longitudinal study the progressive effects of cognitive remediation on brain functioning. In particular, they found increased task-related activation in the prefrontal cortex, which is the same brain region that was activated during memory tasks in healthy individuals. Improvement in brain activation was associated with cognitive changes, specifically verbal memory improvement.
In summary, in this initial period from 1998 to 2002, both SPECT and fMRI studies were able to detect changes in brain functioning after cognitive remediation. Data analyses were mainly based on particular regions of interest that were defined a priori and were mainly located in regions of the prefrontal cortex. Unfortunately, these studies had small samples and lacked control groups to exclude placebo effects. Nonetheless, during this period, no other treatment was able to show any changes in brain functioning related to cognitive improvement in schizophrenia.
Second period: Testing the hypofrontality hypothesis
Wykes et al[12] conducted a controlled study in which 12 patients were randomly assigned to control therapy or cognitive remediation. The effects of the intervention were tested with fMRI procedures using the n-back task during the scanning. The intervention was delivered on an individual basis and involved a therapist and paper and pencil tasks. Not surprisingly, only the group receiving cognitive remediation showed a significant increase in the activation of brain regions associated with working memory, particularly the inferior frontal gyrus. Although the sample size was still small, this study confirmed the insights from the previous period using a convincing methodology. It could be said that it was the first time that brain activation changes were clearly associated with the cognitive remediation intervention by applying a reliable and rigorous methodology. In conclusion, cognitive remediation acted as an active treatment to improve cognition, and it was also able to improve brain functioning in prefrontal regions in patients with schizophrenia. Thus, the need to replicate these results appeared to be the main target of successive studies.
Subsequent posterior studies showed similar results. Haut et al[13] conducted a quasi-randomised study involving nine patients receiving cognitive remediation, nine patients receiving a control therapy in the form of social skills training, and nine healthy control subjects. The authors showed that patients receiving cognitive remediation presented some increases in the activity of the left dorsolateral prefrontal cortex, left dorsal prefrontal cortex, anterior cingulate, right and left prefrontal cortex. The authors used fMRI procedures and visual n-back tasks containing words or pictures, as well as a lexical decision task. Patients receiving cognitive remediation improved on the word and picture 2-back tasks, showing more improvement than the control treatment group. Unfortunately, only regions of interest were examined. Edwards et al[14] used event-related fMRI to analyse brain activity associated with cognitive remediation. The sample comprised 22 patients with schizophrenia and a matched control group of 14 healthy participants. The training protocol emphasised direct encoding of contextual cues and updating of response selection goals in accordance with cue information. Following training, increased activation was observed in several areas involving anterior and posterior brain regions, such as right middle frontal, right superior parietal cortex, right inferior frontal junction, and left inferior frontal and visual cortex. These effects on brain activation seemed to be related to both clinical and cognitive improvements. Unfortunately, the analyses were also based on previously defined regions of interest.
Rowland et al[15] conducted an interesting study investigating the effects of cognitive training in the context of a relational learning task and using fMRI procedures. The sample comprised 17 patients with schizophrenia and 17 healthy control subjects. The most important innovations of this study were the use of whole-brain analysis and the fact that the healthy controls were also tested after having undergone cognitive training. Firstly, the authors found different patterns in both groups before and after treatment. The controls engaged regions including the frontal, parietal, and medial temporal lobes. After the training, the controls showed activation reductions in these regions and spatial extent in areas related to learning improvement. These findings are commonly observed phenomena in successful learning, but they were new in the context of cognitive training. Conversely, thee subjects with schizophrenia displayed bilateral inferior parietal region activation, as the authors had predicted.
Bor et al[16] conducted a study that explored the impact of cognitive remediation in a sample of 17 patients and 15 healthy volunteers. Throughout the study, all of the patients were on stable doses of atypical antipsychotics. The authors used fMRI and a visual 2-back test after 28 h of computerised cognitive remediation, comparing baseline with after treatment measurements in a randomised, controlled trial. Following treatment, patients in the group that received cognitive remediation exhibited higher levels of activation for the left inferior-middle frontal gyrus, cingulate gyrus, and inferior parietal cortex. These changes were related to improvement in measures of strategic efficiency and sustained attention. Hooker et al[17,18], in two studies with the same sample, tested the effects of a cognitive remediation programme plus a social cognitive intervention together in a sample of 22 schizophrenia patients. The authors used an fMRI task of positive and negative facial emotion recognition, showing improvements in postcentral gyrus activity, the left and right amygdala, the right putamen and the right medial prefrontal cortex. The particular choice of the fMRI task and the use of a combined treatment made it difficult to interpret whether these effects on brain functioning were the results of the cognitive treatment or the social cognitive treatment or even of the combination of both treatments.
Finally, Subramaniam et al[19] performed a controlled study with 31 schizophrenia patients and 16 healthy controls, but randomisation was not performed Almost all of the patients were taking atypical antipsychotics throughout the study. During fMRI scanning, tasks of word generation and recognition of words were used. Computerised cognitive training was used to examine its effects on regions related to reality monitoring. The authors found that patients exhibited less activation in the medial prefrontal cortex during word recognition for words at baseline. After cognitive remediation, the patients somewhat normalised their activation patterns, although they still had less activity than healthy controls. One important thing to note in this study was the use of a more complex theoretical framework of brain activation. However, owing to the use of the region of interest approach by the authors, the study precluded the detection of other possibly relevant changes in activity.
In summary, in this second period from 2002 to 2011, different studies consolidated that cognitive remediation acts by improving brain activation in the prefrontal lobes and other related regions. The use of fMRI totally replaced the use of other methods, such as SPECT or PET. Data analyses were still based mainly on predefined regions of interest, but whole-brain analysis opened a new pathway. The methodology was heterogeneous across the different studies, but some of them began to attain the highest standards. Moreover, hypofrontality is the current framework, and an increase of activity is always considered a success criterion. However, some studies have suggested going beyond the hypofrontality hypothesis because cognitive remediation may have some detectable effects in other brain areas. In addition, more brain activation does not necessarily indicate better brain functioning. At least in healthy people, a decrease in activation in some brain areas could be correlated with better cognitive performance.
Neuroprotection: Changes in brain morphology
Eack et al[20] conducted a study that was unique in many aspects, and it is probably one of the most influential works published in the field. The aim of the study was basically to test the option to detect changes in brain morphology after treatment by cognitive rehabilitation. A randomised, controlled trial was performed with a longitudinal design for 2 years, with annual assessments of cognition and structural MRI. Statistical analyses were based on a mixed effects model, while processing of the neuroimaging data was based on voxel-based morphometry methods. Volumetric analyses of regions of interest in different areas of the frontal and temporal regions were performed a posteriori. A sample of 53 patients with diagnoses of schizophrenia or schizoaffective disorder in the early course was included. They were symptomatically stable and, consequently, their doses of antipsychotics were also stable. Cognitive remediation was an integrated approach that combined cognitive computer training and group-based social cognitive exercises. A control group followed an active control based on supportive therapy to improve illness management. It provided psychoeducation and coping strategies training.
Astoundingly, patients who received cognitive remediation showed greater preservation of grey matter volume over 2 years. A main effect of time indicated loss of grey matter in some brain areas, such as the bilateral cerebellum, left medial and posterior cingulate. Additionally, an interactive effect of time and treatment suggested that patients showed less grey matter loss in the left parahippocampal and fusiform gyrus and even greater grey matter increases in the left amygdala following cognitive remediation. Interestingly, these changes were statistically related to cognition changes. The authors appealed to the possible neurobiologic protective effects of cognitive remediation, particularly in early schizophrenia. Unfortunately, this work has not yet been replicated.
Third period: Going beyond hypofrontality and testing connectivity changes
Penadés et al[21] conducted a trial using a whole-brain approach that combined fMRI and diffusion tensor imaging (DTI). They investigated the effect of cognitive remediation on brain functioning in a randomised, controlled trial with 30 schizophrenia outpatients with an experimental group and an active control group. Additionally, 15 healthy volunteers were also included as a second comparison group. Cognitive remediation consisted of an individual strategy-learning-based treatment implemented by a trained therapist, based on paper and pencil exercises. The control group used an active control with an identical duration based on an individual social skills training that provided information about illness management. Brain activation patterns were assessed during an n-back task using independent component analysis as implemented in multivariate exploratory linear decomposition into independent components. This analysis showed clear differences between schizophrenia patients and healthy participants. Despite having performed similarly on the n-back task, patients with schizophrenia showed two different networks that were overactive compared to the healthy participants: The central executive network and default mode network. After treatment, the activation pattern significantly changed only in the cognitive remediation group in the sense of normalising towards the patterns observed in healthy controls Thus, decreased activation was found in the left superior parietal lobule and bilateral middle frontal gyri. In addition, decreased activity in the default-mode network was found in the left precuneus and middle frontal gyrus, among other areas, allowing for activation of the central executive network and deactivating of the default mode network in a more proper manner, suggesting an improvement in the efficiency of both networks. Furthermore, analysis of white matter on DTI showed an increase in the fractional anisotropy index in the anterior part of the genu of the corpus callosum. Interestingly, after treatment, statistically significant correlations were found among cognitive, functional, and structural changes. Finally, the authors speculated that cognitive improvement could be based on an increase of interhemispheric information transfer between the bilateral prefrontal cortices via the corpus callosum.
Another interesting and innovative result was reported by Vianin et al[22]. The authors performed a single-blind, randomised trial with sixteen patients distributed into an experimental group of cognitive remediation and a treatment-as-usual control group. Cognitive remediation was based on executive function training lasting 14 wk. The authors tested brain activation patterns using a covert verbal fluency task during fMRI. In addition to cognitive improvements, the authors reported increased activation in many areas, such as the inferior parietal lobule, precentral gyrus, inferior frontal gyrus (Broca’s area), middle occipital cortex, middle cingulate cortex, and superior parietal lobule, in the cognitive remediation group compared to the control group after treatment. Particularly interesting was the increased activation in Broca’s area. The authors hypothesised that the use of metacognitive techniques of verbalisation might be the main factor underlying these brain changes.
Finally, Subramaniam et al[23] used n-back tasks in an fMRI study comparing computerised auditory and sociocognitive training based on a video game with an active control group and a group of healthy controls. They observed baseline hypoactivation in the middle frontal gyrus at baseline for the patient group. After treatment, the sociocognitive group showed a greater increase in activity in the middle frontal and inferior frontal gyri. One striking and interesting finding in this study was the correlation between the increase in right frontal activation on the verbal n-back task and the increase in the activation in left frontal regions. These results could suggest a process of increased connectivity after cognitive treatment.
Summarising the period since 2013 until today, the studies have definitively gone beyond the hypothesis of hypofrontality. A new and wider theoretical framework is emerging, and it includes more recent discoveries, such as the connectivity between different brain networks (Figure 2). Now, the focus is not only on task-related performance but also on rest-related brain functioning, which involves different interconnected regions that should be highly active at rest but that should be deactivated during the performance of cognitive tasks, such as the default mode network. For this reason, improvement can no longer be expressed only in terms of simple activation increases. Another feature of this period is the focus on other nonspecific prefrontal cortex areas such as the ventral regions or Broca’s area, which could be related to some aspects of the remediation process. These findings are changing the focus of neuroimaging studies and are possibly providing a more complex and accurate picture of the brain mechanisms underlying the effects of cognitive remediation.
Figure 2.
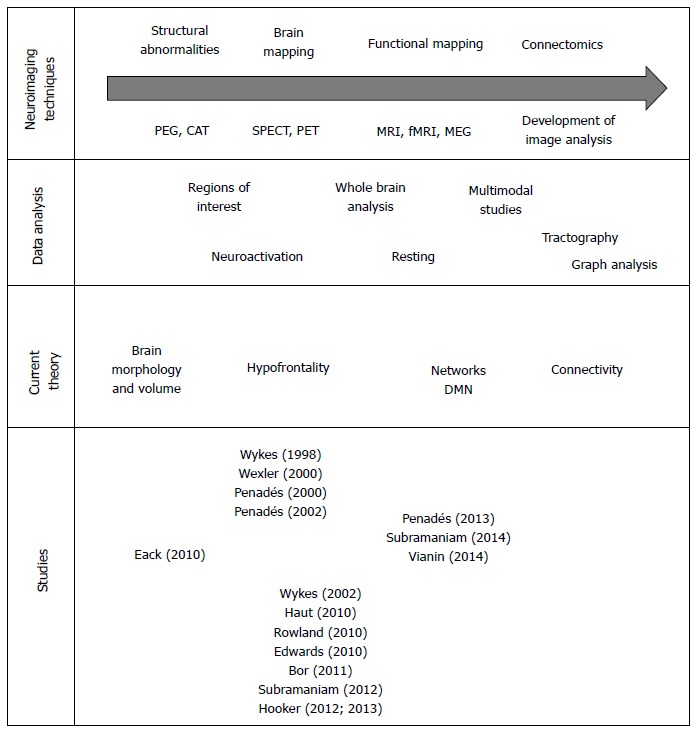
Evolution of neuroimaging studies, data analysis and theoretical frameworks. PEG: Pneumoencephalagraphy; CAT: Computed axial tomography; SPECT: Single-photon emission tomography; PET: Positron emission tomography; MRI: Magnetic resonance imaging; fMRI: Functional magnetic resonance imaging; MEG: Magneto encephalography; DMN: Default mode network.
Meta-analyses
Two meta-analyses have been performed. Ramsay et al[24] conducted an Activation Likelihood Estimation (ALE) meta-analysis. After a literature search, they identified 162 articles, but only 9 of them were included in the analysis. ALE analyses showed increased activity in several brain areas, such as the lateral and medial prefrontal cortex, parietal cortex, insula, and the caudate and thalamus. Wei et al[25], with the same number of studies, found similar but not identical results: Increased brain activation occurred in thee frontal and parietal lobes, including the left medial frontal gyrus, left inferior frontal gyrus, right middle frontal gyrus, right postcentral gyrus, and inferior parietal lobule. The main results of the meta-analyses confirmed the insights of previous studies. However, secondary analyses could add even more information to the state of art. For instance, an original secondary analysis in the Ramsay et al[24] study was performed to compare the brain areas involved in cognitive remediation with areas that had been previously associated with deficits in working memory and executive control in persons with schizophrenia. Surprisingly, they found that some areas, such as the left prefrontal cortex and thalamus, overlapped, but other areas did not, suggesting both restorative and compensatory mechanisms. Another interesting secondary analysis showed that cognitive remediation resulted in similar patterns of brain activation irrespective of the different treatment approaches.
Nonetheless, the results from these two meta-analytic studies should be interpreted with great caution. The number of the included studies (n = 9) was extraordinarily small. In addition, there was a risk of bias due to the heterogeneity among these nine studies. Beyond differences in remediation approach and neuroimaging methods, the studies used different types of control groups and different methods of randomisation, and also blinding was absent in some studies but not in others. Statistical analysis was performed using different methods, making the results difficult to compare because some studies used mixed models and others used a general lineal model; some used data substitution, and others did not; some used the intention-to-treat procedure, and others did not. In terms of neuroimaging processing, different software was used; some studies reported results in terms of interaction effects between time and treatment and others in terms of differences between baseline and posttreatment, and while some studies used whole-brain analysis, others were based on analysis of ROIs. Although Wei et al[25] found similar increased activation brain areas in analysis with or without ROI studies, they found that analysis including ROI studies yielded a higher ALE value. Future studies with larger numbers of studies and more homogenised methodologies will provide us with more consistent results.
DISCUSSION
Cognitive remediation seems to improve brain activation when it is tested by means of neuroimaging techniques. Changes involving the prefrontal and thalamic regions were the most commonly reported results in the reviewed studies as in other previous systematic reviews[3,4,26]. These findings were in agreement with the hypofrontality hypothesis, proposing frontal hypoactivation as the underlying mechanism of cognitive impairments in schizophrenia. Nonetheless, advances in neuroimaging methodology, such as the use of whole-brain analysis, tractography, graph analysis, and other sophisticated methodologies of data processing, might have conditioned the interpretation of results, generating new theoretical frameworks.
In fact, more complex theoretical frameworks are currently reinterpreting hypofrontality. Current theories are focusing on other aspects, such as the connectivity between different brain networks. In addition, not only task-related but also rest-related brain functioning is being considered. Consequently, different interconnected regions should be active at rest, but they should be deactivated during cognitive tasks. Improvement can no longer be expressed exclusively in terms of activation increases. Thus, the results of more recent studies are interpreting cognitive recovery within this framework, showing improvement in the efficiency of different networks. Additionally, structural changes have been described in both the grey and white matter suggesting a neuroprotective effect of cognitive remediation. Cognitive, functional and structural improvements have tended to appear positively correlated.
Results from meta-analytic studies have confirmed the active role of cognitive remediation in brain function involving the prefrontal and thalamic areas. However, other brain changes after treatment have been described. Consequently, cognitive recovery seems to be mediated by restoration and compensation mechanisms at the same time. Moreover, neuroimaging findings are not linked to a particular remediation approach, and all of the different cognitive remediation approaches act similarly in terms of brain functioning. Despite these findings, some limitations must be considered. Firstly, the evidence is tremendously incomplete because of the small number of studies and the lack of replicative studies. Secondly, different remediation approaches and different neuroimaging methods have made the comparison and generalisation of results problematic undertakings. Finally, the lack of a validated theoretical framework for the underlying neurobiological mechanisms of cognitive recovery has rendered the data difficult to interpret.
In conclusion, neuroimaging studies of cognitive remediation in patients with schizophrenia seem to have a positive effect on brain functioning in terms of the functional reorganisation of neural networks. Currently, the most commonly reported changes involve the prefrontal and thalamic regions. Structural changes in the grey and white matter have been described, suggesting a neuroprotective effect of cognitive remediation. Cognitive, functional and structural improvements appear to be positively correlated. Further randomised, controlled studies are needed to confirm and clarify these results, possibly in the context of more complex theoretical models, including different brain networks, aspects of connectivity, whole-brain analysis and multimodal neuroimaging.
COMMENTS
Background
Neuroimaging studies have been conducted by many authors with the intention of identifying the different brain mechanisms underlying cognitive recovery. Even though some positive effects in terms of brain activation have been described, results have been heterogeneous and difficult to integrate. Some studies have described increased brain activation and others have shown decreased activation patterns. The primary aim of this review was to examine systematically all the published trials using neuroimaging procedures. Furthermore, the analysis was intended following a qualitative analysis in order to investigate the influence of neuroimaging methodology and the use of different theoretical frameworks.
Research frontiers
Nowadays, a comprehensive theoretical framework for cognitive recovery is needed. In order to integrate all the studies that have already been published and to guide future research we need to reflect on how the hypothesis and results are evolving and how neuroimaging methodology has conditioned the results of the studies.
Innovations and breakthroughs
Nearly all the recruited neuroimaging studies testing cognitive remediation in patients with schizophrenia have been based on the hypothesis of hypofrontality. In addition, they were always performed using a task-related paradigm and using the “region of interest” methodology. Nowadays, the use of different methodologies such as the brain networks framework and the whole brain analysis has brought to light some new insights reconceptualising the previous findings. Thus, improving frontal activation is now understood in a broader framework that points to an improvement of the networks efficiency.
Applications
Beyond the necessary replicative studies, future research needs to explore different hypothesis such as the putative changes in connectivity patterns of the different brain networks.
Terminology
The efficiency of a network is described in network science as a measure of how efficiently it exchanges information. Brain networks are efficient when they are able to show enough but not excessive activation during cognitive and resting states.
Peer-review
In this systematic review, the authors have presented a qualitative and critical analysis of the neuroimaging studies paying close attention to the theory of the brain networks connectivity.
Footnotes
Supported by a grant from the Instituto de Salud Carlos III of Fondo de Investigaciones Sanitarias FIS, No. PI 11/09158 (to Penadés R).
Conflict-of-interest statement: All the authors declare that they have no competing interests for this article.
Manuscript source: Invited manuscript
Specialty type: Psychiatry
Country of origin: Spain
Peer-review report classification
Grade A (Excellent): 0
Grade B (Very good): B
Grade C (Good): C, C
Grade D (Fair): 0
Grade E (Poor): 0
Peer-review started: September 2, 2016
First decision: September 29, 2016
Article in press: December 14, 2016
P- Reviewer: Fakra E, Kapelski P, Müller MJ S- Editor: Qiu S L- Editor: A E- Editor: Wu HL
References
- 1.Wykes T, Huddy V, Cellard C, McGurk SR, Czobor P. A meta-analysis of cognitive remediation for schizophrenia: methodology and effect sizes. Am J Psychiatry. 2011;168:472–485. doi: 10.1176/appi.ajp.2010.10060855. [DOI] [PubMed] [Google Scholar]
- 2.McGurk SR, Twamley EW, Sitzer DI, McHugo GJ, Mueser KT. A meta-analysis of cognitive remediation in schizophrenia. Am J Psychiatry. 2007;164:1791–1802. doi: 10.1176/appi.ajp.2007.07060906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Thorsen AL, Johansson K, Løberg EM. Neurobiology of cognitive remediation therapy for schizophrenia: a systematic review. Front Psychiatry. 2014;5:103. doi: 10.3389/fpsyt.2014.00103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Isaac C, Januel D. Neural correlates of cognitive improvements following cognitive remediation in schizophrenia: a systematic review of randomized trials. Socioaffect Neurosci Psychol. 2016;6:30054. doi: 10.3402/snp.v6.30054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Eklund A, Nichols TE, Knutsson H. Cluster failure: Why fMRI inferences for spatial extent have inflated false-positive rates. Proc Natl Acad Sci USA. 2016;113:7900–7905. doi: 10.1073/pnas.1602413113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Andreasen NC, Rezai K, Alliger R, Swayze VW, Flaum M, Kirchner P, Cohen G, O’Leary DS. Hypofrontality in neuroleptic-naive patients and in patients with chronic schizophrenia. Assessment with xenon 133 single-photon emission computed tomography and the Tower of London. Arch Gen Psychiatry. 1992;49:943–958. doi: 10.1001/archpsyc.1992.01820120031006. [DOI] [PubMed] [Google Scholar]
- 7.Andreasen NC, O’Leary DS, Flaum M, Nopoulos P, Watkins GL, Boles Ponto L, Hichwa RD. Hypofrontality in schizophrenia: Distributed dysfunctional circuits in neuroleptic-naïve patients”. Lancet. 1997;349:1730–1734. doi: 10.1016/s0140-6736(96)08258-x. [DOI] [PubMed] [Google Scholar]
- 8.Wykes T. What are we changing with neurocognitive rehabilitation? Illustrations from two single cases of changes in neuropsychological performance and brain systems as measured by SPECT. Schizophr Res. 1998;34:77–86. doi: 10.1016/s0920-9964(98)00076-0. [DOI] [PubMed] [Google Scholar]
- 9.Penadés R, Boget T, Lomeña F, Bernardo M, Mateos JJ, Laterza C, Pavía J, Salamero M. Brain perfusion and neuropsychological changes in schizophrenic patients after cognitive rehabilitation. Psychiatry Res. 2000;98:127–132. doi: 10.1016/s0925-4927(99)00050-5. [DOI] [PubMed] [Google Scholar]
- 10.Penadés R, Boget T, Lomeña F, Mateos JJ, Catalán R, Gastó C, Salamero M. Could the hypofrontality pattern in schizophrenia be modified through neuropsychological rehabilitation? Acta Psychiatr Scand. 2002;105:202–208. doi: 10.1034/j.1600-0447.2002.1o421.x. [DOI] [PubMed] [Google Scholar]
- 11.Wexler BE, Anderson M, Fulbright RK, Gore JC. Preliminary evidence of improved verbal working memory performance and normalization of task-related frontal lobe activation in schizophrenia following cognitive exercises. Am J Psychiatry. 2000;157:1694–1697. doi: 10.1176/appi.ajp.157.10.1694. [DOI] [PubMed] [Google Scholar]
- 12.Wykes T, Brammer M, Mellers J, Bray P, Reeder C, Williams C, Corner J. Effects on the brain of a psychological treatment: cognitive remediation therapy: functional magnetic resonance imaging in schizophrenia. Br J Psychiatry. 2002;181:144–152. doi: 10.1017/s0007125000161872. [DOI] [PubMed] [Google Scholar]
- 13.Haut KM, Lim KO, MacDonald A. Prefrontal cortical changes following cognitive training in patients with chronic schizophrenia: effects of practice, generalization, and specificity. Neuropsychopharmacology. 2010;35:1850–1859. doi: 10.1038/npp.2010.52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Edwards BG, Barch DM, Braver TS. Improving prefrontal cortex function in schizophrenia through focused training of cognitive control. Front Hum Neurosci. 2010;4:32. doi: 10.3389/fnhum.2010.00032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rowland LM, Griego JA, Spieker EA, Cortes CR, Holcomb HH. Neural changes associated with relational learning in schizophrenia. Schizophr Bull. 2010;36:496–503. doi: 10.1093/schbul/sbq037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bor J, Brunelin J, d’Amato T, Costes N, Suaud-Chagny MF, Saoud M, Poulet E. How can cognitive remediation therapy modulate brain activations in schizophrenia? An fMRI study. Psychiatry Res. 2011;192:160–166. doi: 10.1016/j.pscychresns.2010.12.004. [DOI] [PubMed] [Google Scholar]
- 17.Hooker CI, Bruce L, Fisher M, Verosky SC, Miyakawa A, Vinogradov S. Neural activity during emotion recognition after combined cognitive plus social cognitive training in schizophrenia. Schizophr Res. 2012;139:53–59. doi: 10.1016/j.schres.2012.05.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hooker CI, Bruce L, Fisher M, Verosky SC, Miyakawa A, D’Esposito M, Vinogradov S. The influence of combined cognitive plus social-cognitive training on amygdala response during face emotion recognition in schizophrenia. Psychiatry Res. 2013;213:99–107. doi: 10.1016/j.pscychresns.2013.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Subramaniam K, Luks TL, Fisher M, Simpson GV, Nagarajan S, Vinogradov S. Computerized cognitive training restores neural activity within the reality monitoring network in schizophrenia. Neuron. 2012;73:842–853. doi: 10.1016/j.neuron.2011.12.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Eack SM, Hogarty GE, Cho RY, Prasad KM, Greenwald DP, Hogarty SS, Keshavan MS. Neuroprotective effects of cognitive enhancement therapy against gray matter loss in early schizophrenia: results from a 2-year randomized controlled trial. Arch Gen Psychiatry. 2010;67:674–682. doi: 10.1001/archgenpsychiatry.2010.63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Penadés R, Pujol N, Catalán R, Massana G, Rametti G, García-Rizo C, Bargalló N, Gastó C, Bernardo M, Junqué C. Brain effects of cognitive remediation therapy in schizophrenia: a structural and functional neuroimaging study. Biol Psychiatry. 2013;73:1015–1023. doi: 10.1016/j.biopsych.2013.01.017. [DOI] [PubMed] [Google Scholar]
- 22.Vianin P, Urben S, Magistretti P, Marquet P, Fornari E, Jaugey L. Increased activation in Broca’s area after cognitive remediation in schizophrenia. Psychiatry Res. 2014;221:204–209. doi: 10.1016/j.pscychresns.2014.01.004. [DOI] [PubMed] [Google Scholar]
- 23.Subramaniam K, Luks TL, Garrett C, Chung C, Fisher M, Nagarajan S, Vinogradov S. Intensive cognitive training in schizophrenia enhances working memory and associated prefrontal cortical efficiency in a manner that drives long-term functional gains. Neuroimage. 2014;99:281–292. doi: 10.1016/j.neuroimage.2014.05.057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ramsay IS, MacDonald AW. Brain Correlates of Cognitive Remediation in Schizophrenia: Activation Likelihood Analysis Shows Preliminary Evidence of Neural Target Engagement. Schizophr Bull. 2015;41:1276–1284. doi: 10.1093/schbul/sbv025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Wei YY, Wang JJ, Yan C, Li ZQ, Pan X, Cui Y, Su T, Liu TS, Tang YX. Correlation Between Brain Activation Changes and Cognitive Improvement Following Cognitive Remediation Therapy in Schizophrenia: An Activation Likelihood Estimation Meta-analysis. Chin Med J (Engl) 2016;129:578–585. doi: 10.4103/0366-6999.176983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kurtz MM. Cognitive remediation for schizophrenia: current status, biological correlates and predictors of response. Expert Rev Neurother. 2012;12:813–821. doi: 10.1586/ern.12.71. [DOI] [PubMed] [Google Scholar]