

Abstract
Rationale:
The great auricular nerve can be damaged by the neck surgery, tumor, and long-time pressure on the neck. But, great auricular neuralgia is very rare condition. It was managed by several medication and landmark-based great auricular nerve block with poor prognosis.
Patient concerns:
A 25-year-old man presented with a pain in the left lateral neck and auricle.
Diagnosis:
He was diagnosed with great auricular neuralgia.
Interventions:
His pain was not reduced by medication. Therefore, the great auricular nerve block with local anesthetics and steroid was performed under ultrasound guidance.
Outcomes:
Ultrasound guided great auricular nerve block alleviated great auricular neuralgia.
Lessons:
This medication-resistant great auricular neuralgia was treated by the ultrasound guided great auricular nerve block with local anesthetic agent and steroid. Therefore, great auricular nerve block can be a good treatment option of medication resistant great auricular neuralgia.
Keywords: cervical plexus, great auricular nerve, nerve block, neuralgia, ultrasonography
1. Introduction
The great auricular nerve is the largest sensory branch of superficial branches of the cervical plexus, arising from C2 and C3 spinal roots. It passes vertically upward over the sternocleidomastoid muscle (SCM) providing sensory innervations for the skin of auricle, lower face, and upper neck.[1] It can be damaged by the neck surgery,[2–4] tumor,[5] and prolonged pressure on the neck.[6,7] But, great auricular neuralgia rarely occurs.
We report the first description of great auricular neuralgia, which was treated successfully with the ultrasound guided great auricular nerve block using local anesthetic agent and steroid. A signed written consent was obtained from the patient for this case report.
2. Case report
A 25-year-old man was referred to our clinic with a 10-day history of pain in the left lateral neck and auricle. Ten days before his presentation, his pain suddenly developed after sleeping with the left side of his head against desk. His pain was characterized by constant burning or aching pain and intermittent sharp, lancinating pain over the left auricle and lateral neck area. His pain was rated at an intensity of 7 on the point numeric rating scale (NRS) from 0 (no pain) to 10 (worst pain imaginable). The pain was often provoked by rotation of his head to the right side and no trigger zone was found. General neurological and otorhinological examination showed no abnormal findings. In addition, there were no abnormalities in the magnetic resonance imaging of the neck and brain. His clinical diagnosis of great auricular neuralgia was made from the pain characteristics and painful region and he was treated with oral pregabalin (150 mg twice a day), amitriptyline (10 mg once a day), and tramadol (50 mg twice a day) for 9 days. But, despite this medication his pain did not reduce. Therefore, we decided to perform the great auricular nerve block. The great auricular nerve was identified at the level of the fourth cervical spine in the axial sonographic view using high-frequency linear array transducer (Fig. 1). The great auricular nerve was located at dorsal border of SCM. We inserted a 25-gauge block needle using in-plane approach and performed great auricular nerve block with 1% lidocaine 0.5 mL and triamcinolone 10 mg. One hour later, his pain was rated 2 on the NRS. Five days after the great auricular nerve block, his pain had completely disappeared and stopped taking pain medication. At 6 months follow-up after the great auricular nerve block, he remained symptom free.
Figure 1.
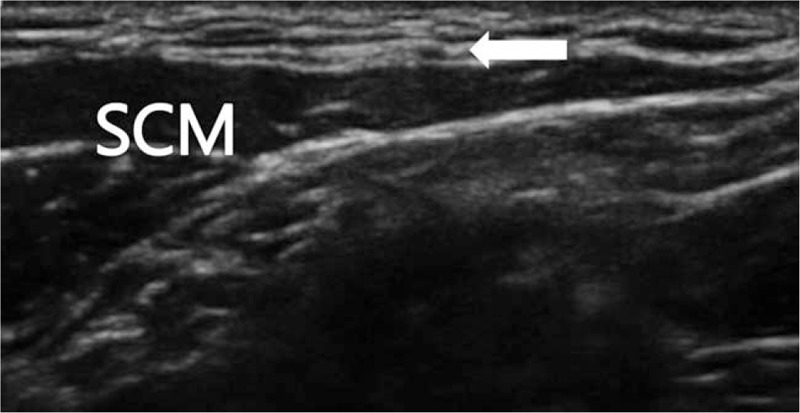
The axial sonographic view of the great auricular nerve (arrow) above the sternocleidomastoid muscle (SCM).
3. Discussion
The great auricular neuralgia is a very rare disorder. The pathogenesis of great auricular neuralgia remained unknown clearly. It may be idiopathic or secondary to surgery or trauma of head and neck or prolonged pressure on the neck. Diagnosis of great auricular neuralgia is based primarily on the history and physical findings—specifically, the specific pain characters including intermittent, electric shock-like, and distressing nature and well-localized cutaneous region of the pain.[8] Rotation of head to the opposite side often provokes the pain over the dermatome of great auricular nerve, which sometimes can radiate to upper neck, temporal, and occipital area.[9] In the present cases, definite causative factors of great auricular neuralgia were not identified but the great auricular neuralgia is presumed to be caused by compression of head and neck during sleep.
Numerous analgesics including anticonvulsants, antidepressants, and opioids are currently used for the treatment of neuropathic pain. However, neuropathic pain disorders including trigeminal neuralgia, glossopharyngeal neuralgia, postherpetic neuralgia, and occipital neuralgia are often difficult to treat with such drugs. It was reported that administration of gabapentin 1200 mg daily was effective to reduce great auricular neuralgia.[8] However, in the present case, treatment with pregabalin 300 mg, amitriptyline 10 mg, and tramadol 100 mg did not reduce the neuralgic pain. Nerve block is useful in the diagnosis and treatment of painful conditions. In the preclinical and clinical studies, it was shown that early application of nerve block can prevent or reduce neuropathic pain.[10,11] Therefore, we decided to turn our therapeutic focus toward nerve block.
Great auricular nerve block was achieved via superficial cervical plexus block using large volumes of local anesthetics. However, ultrasound visual guidance technique can identify target nerve, which allows highly selective block of the nerve with smaller volume of local anesthetics, leading to better efficacy for performing regional and peripheral nerve block.[12] In the present case, great auricular nerve block was performed with 1% lidocaine 0.5 mL and triamcinolone 10 mg. A combination of local anesthetics and steroid was found to be more effective than local anesthetics alone in the treatment of neuropathic symptoms and signs following nerve injury.[13] Administration of steroid around injured nerve may alleviate edema and provide analgesia through its anti-inflammatory and membrane stabilising actions, lead to hastening recovery of the damaged nerves.[14,15]
In conclusion, the great auricular neuralgia is a very rare disorder. In the present case, great auricular neuralgia was resistant to medications but was successfully treated by a real-time ultrasound-guided great auricular nerve block using local anesthetic agent and steroid. Therefore, great auricular nerve block can be a good treatment option of medication resistant great auricular neuralgia.
Footnotes
Abbreviations: NRS = numeric rating scale, SCM = sternocleidomastoid muscle.
The authors have no conflicts of interest to disclose.
References
- [1].Peuker ET, Filler TJ. The nerve supply of the human auricle. Clin Anat 2002;15:35–7. [DOI] [PubMed] [Google Scholar]
- [2].Lefkowitz T, Hazani R, Chowdhry S, et al. Anatomical landmarks to avoid injury to the great auricular nerve during rhytidectomy. Aesthet Surg J 2013;33:19–23. [DOI] [PubMed] [Google Scholar]
- [3].Moss CE, Johnston CJ, Whear NM. Amputation neuroma of the great auricular nerve after operations on the parotid gland. Br J Oral Maxillofac Surg 2000;38:537–8. [DOI] [PubMed] [Google Scholar]
- [4].Matarasso A, Elkwood A, Rankin M, et al. National plastic surgery survey: face lift techniques and complications. Plast Reconstr Surg 2000;106:1185–95. [DOI] [PubMed] [Google Scholar]
- [5].Ginsberg LE, Eicher SA. Great auricular nerve: anatomy and imaging in a case of perineural tumor spread. AJNR Am J Neuroradiol 2000;21:568–71. [PMC free article] [PubMed] [Google Scholar]
- [6].Arias M, Arias-Rivas S, Perez M, et al. Numb ears in resurrection: great auricular nerve injury in hanging attempt. Neurology 2005;64:2153–4. [DOI] [PubMed] [Google Scholar]
- [7].LaPrade CM, Foad A. Greater auricular nerve palsy after arthroscopic anterior-inferior and posterior-inferior labral tear repair using beach-chair positioning and a standard universal headrest. Am J Orthop (Belle Mead NJ) 2015;44:188–91. [PubMed] [Google Scholar]
- [8].Maimone-Baronello M, Piccoli F, La Bella V. Great auricular neuralgia: a case report. Headache 2003;43:1005–6. [DOI] [PubMed] [Google Scholar]
- [9].Robertson CE, Garza I. Great auricular neuralgia: case series. J Headache Pain 2013;14suppl 1:161–161. [DOI] [PubMed] [Google Scholar]
- [10].Xie W, Strong JA, Zhang JM. Early blockade of injured primary sensory afferents reduces glial cell activation in two rat neuropathic pain models. Neuroscience 2009;160:847–57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Yoo HS, Nahm FS, Lee PB, et al. Early thoracic sympathetic block improves the treatment effect for upper extremity neuropathic pain. Anesth Analg 2011;113:605–9. [DOI] [PubMed] [Google Scholar]
- [12].Jeon YH. Easier and safer regional anesthesia and peripheral nerve block under ultrasound guidance. Korean J Pain 2016;29:1–2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Eker HE, Cok OY, Aribogan A, et al. Management of neuropathic pain with methylprednisolone at the site of nerve injury. Pain Med 2012;13:443–51. [DOI] [PubMed] [Google Scholar]
- [14].Johansson A, Sjolund B. Nerve blocks with local anesthetics and corticosteroids in chronic pain: a clinical follow-up study. J Pain Symptom Manage 1996;11:181–7. [DOI] [PubMed] [Google Scholar]
- [15].Kim SY, Kim DG, Park YM, et al. Psoas compartment block for treatment of motor weakness and pain following herpes zoster. Korean J Pain 2017;30:62–5. [DOI] [PMC free article] [PubMed] [Google Scholar]