

A 35-year-old female presented with a giant hyperpigmented, light-brown colored macule with irregular margins measuring 38 × 19 cm extending from the left shoulder to the mid of forearm with overlying soft, nontender, gradually enlarging mass of size 25 × 10 cm with convoluted surface; on palpation, the mass felt like a “bag of worms,” extending from the shoulder to three-fourth of the left arm since childhood [Figure 1a–c]. Family history suggested autosomal dominant mode of inheritance; the patient had characteristic skin lesions such as multiple cafe-au-lait macules and neurofibromas over the trunk and extremities. Eye examination revealed characteristic Lisch nodules [Figure 1d], suggestive of Von Recklinghausen's disease. Histopathological examination of the mass revealed increased pigmentation of the basal layer due to increased proliferation of epidermal melanocytes, i.e., epidermal melanocytic hyperplasia with interlacing bundles of elongated spindle-shaped nerve cells with wavy nuclei along with intervening supportive fibro-collagenous stroma with few compressed blood vessels in dermis, suggestive of neurofibroma. Myxoid stroma was not appreciated [Figure 2a and b].
Figure 1.
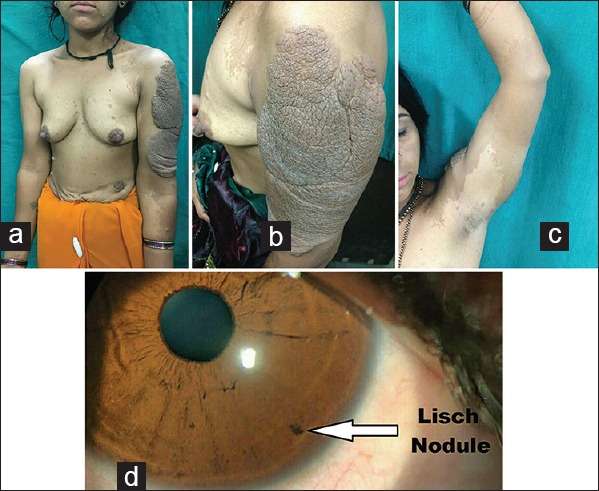
(a-c) Plexiform neurofibroma with convoluted surface and underlying giant café-au-lait macule extending from the shoulder to the middle of the left forearm. (d) 1–2 mm brown, dome-shaped solid lesions involving the iris between 4 to 6 o’clock position
Figure 2.
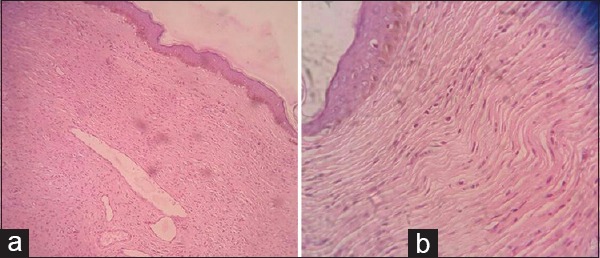
(a) Epidermis revealing increased pigmentation of the basal layer due to increased proliferation of epidermal melanocytes, i.e., epidermal melanocytic hyperplasia. (Hematoxylin and eosin; ×10) (b) Dermis revealing interlacing bundles of elongated, spindle-shaped nerve cells with wavy nuclei along with intervening supportive fibrocollagenous stroma with few compressed blood vessels. (Hematoxylin and eosin; ×40)
Neurofibromatosis type 1, also known as von Recklinghausen's disease, is an autosomal dominant disease due to the mutation of NF1 gene on chromosome 17q. 11.2.[1] Café-au-lait macules are commonly observed in childhood. They are of varying sizes ranging from 2 mm to 20 cm.[2] Plexiform neurofibroma is a benign proliferation of the neural element of peripheral nerve. Unlike cutaneous neurofibroma, plexiform neurofibroma may show malignant transformation, i.e., malignant peripheral nerve sheath tumor (MPNST).[3] Cross-sectional studies have demonstrated a 1–2% prevalence of MPNST among NF1 patients. Rapid enlargement should raise concern for malignant degeneration of a neurofibroma. Other clinical manifestations are radicular pain, paresthesias, and motor weakness. Clinically, these signs and symptoms of MPNST were not present in our case. The general histological appearance of MPNSTs is one of dense cellular fascicles, which alternate with myxoid regions, described as a marbleized pattern. Malignancy is suggested by features such as invasion of surrounding tissues, invasion of vascular structures, nuclear pleomorphism, necrosis, and mitotic activity. The disfigurement and malignant potential of plexiform neurofibroma is a cause of concern from both patient and physician's point of view. In our case, histopathological examination of the mass ruled out malignancy, and the patient was advised surgical correction for the large plexiform neurofibroma. To the best of our knowledge, plexiform neurofibroma with underlying giant café-au-lait macule has not been reported in literature.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
We acknowledge the sincere efforts of Dr Samarth Shukla, professor of pathology, for the histopathological evaluation of the skin biopsy.
References
- 1.Theos A, Korf BR. Pathophysiology of Neurofibromatosis Type 1. Ann Intern Med. 2006;144:842–9. doi: 10.7326/0003-4819-144-11-200606060-00010. [DOI] [PubMed] [Google Scholar]
- 2.Thappa DM, Jeevankumar B, Karthikeyan K. Giant café-au-lait macule in neurofibromatosis type 1. J Dermatol. 2001;28:60–1. doi: 10.1111/j.1346-8138.2001.tb00090.x. [DOI] [PubMed] [Google Scholar]
- 3.Korf BR. Plexiform neurofibromas. Am J Med Genet. 1999;89:31–7. doi: 10.1002/(sici)1096-8628(19990326)89:1<31::aid-ajmg7>3.0.co;2-w. [DOI] [PubMed] [Google Scholar]