

Abstract
Objective
To assess whether ever reporting depressive symptoms affects mortality in the modern HIV treatment era.
Design
Cohort study of HIV-infected adults in routine clinical care at 7 sites in the United States.
Methods
We examined the effect of ever reporting depressive symptoms on all-cause mortality using data from the Centers for AIDS Research Network of Integrated Clinical Systems cohort. We included individuals with at least one depression measure between 2005 and 2014. Depressive symptoms were measured with the Patient Health Questionnaire (PHQ)-9. We used weighted Kaplan-Meier curves and marginal structural Cox models with inverse probability weights to estimate the effect of ever reporting depressive symptoms (PHQ-9 > 10) on all-cause mortality.
Results
A total of 10,895 individuals were included. Participants were followed for a median of 3.1 years (35,621 total person-years [PY]). There were 491 (4.5%) deaths during the follow-up period (crude incidence rate 13.8/1,000 PY). At baseline, 28% of the population reported depressive symptoms. In the weighted analysis, there was no evidence that ever reporting depressive symptoms increased the hazard of all-cause mortality (HR 0.82, 95% CI 0.55, 1.24).
Conclusions
In a large cohort of HIV-infected adults in care in the modern treatment era, we observed no evidence that ever reporting depressive symptoms increased the likelihood of all-cause mortality, controlling for a range of time-varying factors. ART that is increasingly robust to moderate adherence and improved access to depression treatment may help to explain changes in the relationship between depressive symptoms and mortality in the modern treatment era.
Keywords: depression, depressive symptoms, HIV, mortality, mental health
Introduction
Depression affects 20–30% of people living with HIV (PLWH) and is the most commonly reported mental health condition among HIV-infected adults in care in the United States.[1, 2] For PLWH, depression is a debilitating condition that adversely affects quality of life,[3, 4] antiretroviral (ART) adherence,[5, 6] and viral suppression.[7–9] Depression has also been associated with higher mortality in the pre-combination ART (cART) and early cART eras.[7, 10–13]
Depression may affect mortality through two primary pathways, both of which may be altered in the modern HIV treatment era. First, depression is associated with suboptimal engagement in HIV care and ART adherence, which influences long-term survival.[14–16] However, as HIV treatment has become simpler, more tolerable and more potent, the negative consequences of missing ART doses have diminished.[17, 18] Second, depression has been hypothesized to adversely affect innate immunity among HIV-infected adults, which may translate into faster HIV progression and an increased risk of mortality.[19, 20] It is possible that the increasing recognition of the high prevalence of mental health conditions among PLWH,[21] has led to improved access to mental health treatment over time.[22–25]
Given these changes in both HIV and mental health treatment, there is a need to understand the relationship between depression and mortality in the modern HIV treatment era. The goal of this analysis was to estimate the effect of ever reporting depressive symptoms on all-cause mortality among HIV-infected adults in routine care in the United States in the cART-era.
Methods
Data for the present analysis come from the Centers for AIDS Research (CFAR) Network of Integrated Clinical Systems (CNICS) cohort. The CNICS cohort includes over 31,000 HIV-infected adults in routine HIV clinical care at 8 sites in the United States.[26] CNICS collects detailed information on demographic characteristics, ART, antidepressant medications, HIV/AIDS clinical events, co-morbid conditions, HIV-related laboratory values and vital status on patients who consent to participate (approximately 95% across sites).[27] Patients in CNICS also complete a battery of self-administered socio-behavioral questionnaires, called Patient-Reported Outcomes (PROs). HIV-infected patients complete PROs on touch-screen tablets during routine care visits approximately every 4–6 months, although frequency varies based on clinical follow-up. Participants provide written informed consent to participate in CNICS. Ethical approval for the use of routinely collected clinical data was provided by the institutional review board at each CNICS site.
Study Population and Design
The present analysis includes all HIV-infected individuals in CNICS with at least one PRO measure. PRO collection began between 2005 and 2011 at 7 of 8 CNICS sites; 1 site did not collect depression measures during their PRO assessment and was excluded. PRO assessments provided clinicians with routine assessments of patients’ depressive symptoms. A patient’s first PRO may capture either incident or prevalent depressive symptoms. Our study design is therefore analogous to a treatment decision design[28], where a participant’s depressive symptom severity at their first PRO represents a point where informed decisions about depression treatment may have been made, rather than onset of depressive symptoms exclusively. Participants were followed from the date of their first PRO until administrative censoring between June and November, 2014 (depending on site) or death; whichever date came first. Vital status is regularly ascertained for all CNICS participants, regardless of whether they are currently in care or not. Therefore we did not censor individuals at loss to follow-up (LTFU) from CNICS (≥12 months with no HIV appointment).[15] Person-time after a participant was LTFU was considered a period with missing exposure and covariate information and accounted for in the analysis (see below).
Measures
The outcome of interest was all-cause mortality. Deaths were ascertained from the United States Social Security Death Index or National Death Index for all CNICS participants. The exposure of interest was first report of moderate to severe depressive symptoms (hereafter “depressive symptoms”) within the study period, measured using the Patient Health Questionnaire-9 (PHQ-9) during the PRO assessment.[29] A PHQ-9 score of ≥ 10 has 88% sensitivity and specificity to detect a major depressive episode and was used to define depressive symptoms.[29]
As a part of the PRO assessment, CNICS also collects validated measures of panic disorder (Patient Health Questionnaire-5),[30] high risk alcohol use (Alcohol Use Disorders Identification Test (AUDIT) and defined as an AUDIT score ≥ 4 for males and ≥ 3 for females),[31] and current, past or no illicit drug use, including cocaine/crack, heroin/opiates, crystal/amphetamine use, but excluding marijuana (The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST)).[32, 33] For this analysis, we defined undetectable viral load as <50 copies/mL and ART adherence as no missed doses in the past week. Information on antidepressant prescription is available in CNICS. However, antidepressant use was not considered as a confounder in our analysis because it is unlikely to independently predict mortality and therefore does not represent a confounding pathway.
Statistical Analysis
The goal of our analysis was to estimate the effect of ever reporting depressive symptoms on mortality. We used weighted Kaplan-Meier curves and marginal structural Cox models with inverse probability weights [34] to approximate a randomized controlled trial intent-to-treat analysis in which individuals are considered to be randomized at baseline to ever report depressive symptoms over the study period or not. Inverse probability of treatment weights were estimated as the inverse probability of first reporting depressive symptoms at a given visit, conditional on time-fixed (site, gender, race/ethnicity, HIV acquisition risk group, and age at baseline) and time-varying variables (high alcohol use, drug use, panic disorder, ART use and adherence, CD4 count, and viral load suppression, and depressive symptoms score at the previous visit), as well as calendar year and length of time in CNICS care.[35] Depressive symptom scores were modeled using a linear term and age and CD4 count were modeled using restricted cubic splines. IPTWs were stabilized by baseline covariates and multiplied across visits to account for a participant’s exposure history.
Participants in CNICS present for care with varying frequency. Therefore, a report of depressive symptoms may be more common among individuals with more regular visits due to more frequent assessment. To account for the varying frequency of visits within CNICS, we used inverse probability of observation weights (IPOW), under the assumption that participants should complete a PRO at least once every 6 months.[36] We allowed all time-varying covariates to be valid (i.e. carried forward) for up to 6 months (182 days). After 182 days with no depressive symptoms, alcohol, drug, panic disorder or ART use and adherence measures participants were considered to have a missing PRO assessment. Multiple imputation (n=20 imputations) was used to fill in missing values for individual variables for all observed PRO assessments.[37] IPOW were estimated as the inverse probability of having an observed PRO within 6 months, conditional on time-fixed site, gender, race, HIV acquisition risk group, age at baseline, mental health diagnoses prior to baseline and time-varying history of having a previous PRO measurement, exposure status (binary), depressive symptoms score (continuous), alcohol use, drug use, panic disorder, being on an antidepressant, ART use and adherence, CD4 count and viral load suppression at the previous visit. Depressive symptoms scores and CD4 count were modeled using restricted cubic splines and age was modeled using a quadratic term. IPTW and IPOW were multiplied together to create a single combined set of weights. All weights were progressively truncated until the mean was 1.00 and the range was reasonable.[35]
We conducted two secondary analyses. First, we examined if the effect of ever reporting depressive symptoms on mortality differed by gender or baseline psychiatric comorbidities (defined as a history of a mental health diagnosis, panic symptoms or disorder). Second, to better understand which factors most strongly confounded the depressive symptoms and mortality relationship, we excluded time-varying measures of alcohol use, drug use and panic disorder from the estimation of the IPTW. For both the primary and secondary analyses, we compared unadjusted estimates, unweighted multivariable estimates adjusted for baseline covariates only, and weighted estimates adjusted for baseline and time-varying covariates. Analyses were conducted using Stata version 13 (StataCorp, College Station, Texas) and SAS version 9.4 (SAS Institute, Cary, North Carolina).
Results
A total of 10,895 individuals in CNICS had at least one PRO assessment between 2005 and 2014 and were included. Participants were followed for a median of 3.1 years (interquartile range 1.5–4.9) and contributed a total of 35,621 person-years. There were 491 (4.5%) deaths during the follow-up period (crude incidence rate 13.8 per 1,000 person-years). Depressive symptoms were reported by 28% of the population at baseline and at 39% of visits over the follow-up period (Table 1). Over 8 years, 59% of person-time was spent having “ever reported depressive symptoms”. (Figure 1). Among those who ever developed depressive symptoms, participants reported current depressive symptoms at 61% of subsequent PRO assessments.
Table 1.
Characteristics of 10,985 HIV-infected patients in routine care at CNICS sites in the United States at baseline and over follow-up: 2005–2014.
| Characteristic | Baseline (n=10,985) | Follow-up (over 99,040 observed PROs4, representing 35,621 person-years) |
|---|---|---|
|
| ||
| N(%) or Median (IQR) | N(%) or Median (IQR) | |
| Age | 44 (36, 50) | -- |
| Gender | ||
| Male | 9,324 (84.9) | -- |
| Female | 1,660 (15.1) | -- |
| Race/ethnicity | ||
| White, non-Hispanic | 5,546 (50.9) | -- |
| Black, non-Hispanic | 3,178 (29.2) | -- |
| Hispanic | 1,680 (15.4) | -- |
| Other | 488 (4.5) | -- |
| HIV acquisition risk group | ||
| IDU 1 | 1,538 (14.2) | -- |
| MSM 2 | 6,843 (63.0) | -- |
| Heterosexual | 2,313 (21.3) | -- |
| Other | 173 (1.6) | -- |
| Depressive symptoms | 5 (1,10) | 4 (0, 9) |
| No depressive symptoms (PHQ-9 <10) | 7,962 (72.5) | 60,334 (60.9) |
| Depressive symptoms (PHQ-9 ≥10) | 3,023 (27.5) | 38,706 (39.1) |
| On antidepressants | ||
| No | 8,255 (75.8) | 71,162 (72.0) |
| Yes | 2,643 (24.2) | 27,645 (28.0) |
| Alcohol use | ||
| Not high risk | 7,553 (72.3) | 73,217 (77.1) |
| High Risk | 2,893 (27.7) | 21,789 (22.9) |
| Drug use (excluding marijuana) | ||
| No use | 4,527 (43.9) | 47,638 (50.8) |
| Current use | 1,875 (18.2) | 12,377 (13.2) |
| Past use | 3,916 (38.0) | 33,718 (36.0) |
| Panic disorder | ||
| No panic symptoms | 7,544 (70.2) | 70,650 (72.9) |
| Some panic symptoms | 1,701 (15.8) | 13,657 (14.1) |
| Panic disorder | 1,503 (14.0) | 12,627 (13.0) |
| Mental health diagnosis prior to baseline | ||
| 0 | 10,342 (94.1) | -- |
| ≥ 1 | 643 (5.9) | -- |
| ART use/adherence 3 | ||
| ART, adherent | 6,996 (63.7) | 70,714 (77.5) |
| ART, not adherent | 1,358 (12.4) | 12,556 (13.8) |
| Not on ART | 2,631 (24.0) | 7,953 (8.7) |
| CD4 count | 479 (303, 684) | 495 (309, 699) |
| Viral load suppression (<50 copies/mL) | ||
| Undetectable | 5,506 (55.4) | 57,300 (64.9) |
| Detectable | 4,436 (44.6) | 31,044 (35.1) |
IDU = Intravenous drug users,
MSM = men who have sex with men,
adherence defined as no missed doses in the last week,
PRO = patient reported outcome. Missing baseline data: age n=1, race/ethnicity n=93, HIV acquisition risk group n=118, on antidepressants n=87, alcohol use n=539, drug use n=667, panic disorder n=237, viral load suppression n= 1,043.
Figure 1.
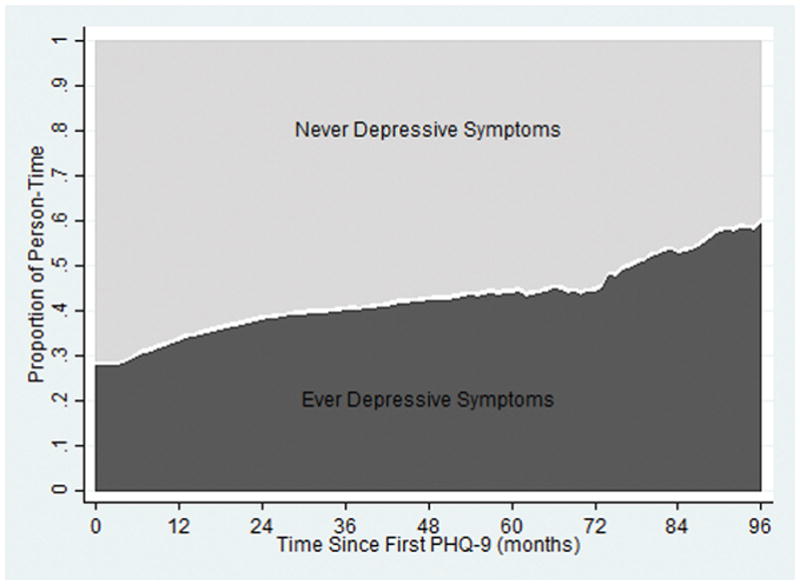
Proportion of person-time cumulatively spent ever with depressive symptoms versus never with depressive symptoms over 8 years of follow-up. The light gray area represents person time for those who never reported depressive symptoms and the dark gray represents person time for those who reported depressive symptoms at least once during the follow-up period.
The cohort was predominately male (85%), white non-Hispanic (51%) and self-reported contracting HIV through male-to-male sexual contact (63%) (Table 1). Mental health and substance abuse issues were common. Over a quarter (28%) of participants were high risk alcohol users, 56% were current or past drug users, and 30% had some panic symptoms or panic disorder. At baseline, 24% of participants were on antidepressants, of whom 43% had depressive symptoms. Mental health diagnoses recorded in CNICS prior to baseline were rare (6%). The majority of participants at baseline were on ART and adherent (64%). The median CD4 count at baseline was 479 (IQR 303–684) and overall 55% of participants had an undetectable viral load.
Of the 491 deaths that occurred, 232 occurred after reporting depressive symptoms over 13,071 person years (crude incidence rate 17.75 per 1,000 person-years) and 259 occurred among individuals who never reported depressive symptoms prior to death over 22,549.32 person years (crude incidence rate 11.49 per 1,000 person-years). Cause of death information was available for only 28% of participants.
In the unadjusted (crude) analysis, ever reporting depressive symptoms was associated with an increase in mortality (HR 1.33, 95% CI 1.11, 1.59; Table 2). When baseline factors only were accounted for, ever reporting depressive symptoms increased the hazard of mortality by 22% (HR 1.22, 95% CI 0.99, 1.49). After adjustment with a combined weight to account for both time-varying confounding and unobserved PRO assessments, there was no evidence that ever reporting depressive symptoms increased the hazard of all-cause mortality (HR 0.82, 95% CI 0.55, 1.24; Table 2, Figure 2). There was also no evidence that the effect of ever reporting depressive symptoms on all-cause mortality differed by gender (interaction p-value 0.35) or baseline psychiatric comorbidities (interaction p-value 0.21). In a secondary analysis when alcohol use, drug use and panic disorder were removed from the weights, effect estimates were also similar (HR 0.96, 95% CI 0.75, 1.25).
Table 2.
Unweighted and weighted estimates for the effect of ever reporting depressive symptoms on all-cause mortality among CNICS participants, 2005–2014.
|
|
||||||
|---|---|---|---|---|---|---|
| Events | Person-years | Incidence Rate1 | Unadjusted | Adjusted for baseline covariates3 | Weighted4 | |
| HR (95% CI)2 | HR (95% CI)2 | HR (95% CI)2 | ||||
|
| ||||||
| Never reported depressive symptoms | 232 | 13,071.37 | 17.7 | 1.00 | 1.00 | 1.00 |
| Ever reported depressive symptoms | 259 | 22,549.32 | 11.5 | 1.33 (1.11, 1.59) | 1.22 (0.99, 1.49) | 0.82 (0.55, 1.24) |
Incidence rate per 1,000 person years;
Estimated among kept visits only;
Adjusted for all time-fixed and time-varying covariates at baseline;
Weights include both time-fixed and time-varying covariates and are the product of inverse probability of treatment and inverse probability of observation weights; mean of combined weight 1.00, range 0.02 to 10.0. Truncated between 100th and 99th and 0 and 1st percentile.
Figure 2.
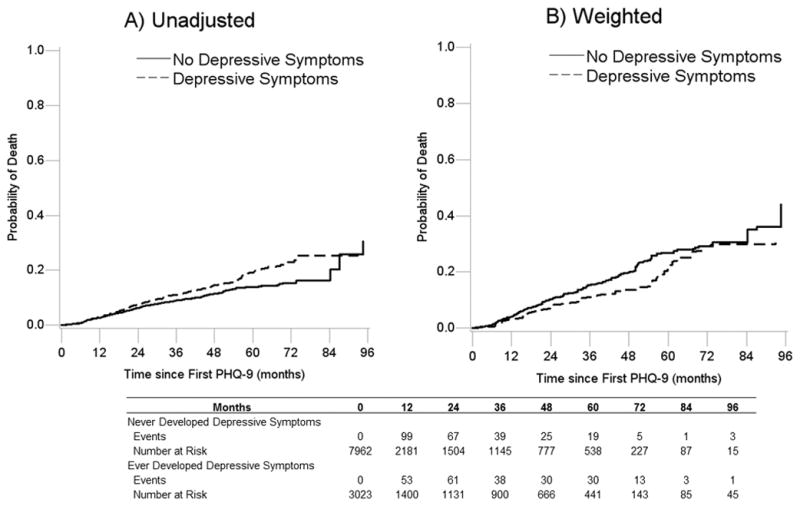
A) Unadjusted and B) Weighted Kaplan-Meier curves showing the cumulative probability of all-cause mortality for individuals who reported depressive symptoms and individuals who did not report depressive symptoms in care in CNICS between 2005 and 2014. Weighted estimates are weighted by the product of inverse probability of treatment weights to account for time-varying confounding and inverse probability of observation weights to account for not having an observed patient reported outcome assessment at least once within a 6-month period.
Not having a PRO measure at least once in a 6-month period was common over the follow-up period. Out of a possible 214,233 PRO measures (assuming a measurement at least once every 6 months) 115,193 (54%) were “missed” (i.e. not observed) and 99,040 (46%) visits were observed. Of the 99,040 observed PRO measures, 73,209 (74%) had complete data and 25,831 (26%) had at least 1 missing covariate value. The proportion of observed PRO measures among persons who ever reported depressive symptoms (48%), was similar to the proportion among those who never reported depressive symptoms (45%). Effect estimates were similar when only observed PRO measures were considered (e.g. complete case) and IPOW were not used (HR 0.98, 95% CI 0.65, 1.47).
Discussion
In our cohort of HIV-infected adults in routine care in the United States, depressive symptoms were experienced at 39% of visits over a 9-year period. Over the follow-up period, the crude mortality rate was 13.8 deaths per 1,000 person years. In unadjusted analyses, ever reporting depressive symptoms increased the hazard of all-cause mortality by 33%. After accounting for time-varying confounding and unobserved PRO assessments, there was no evidence that ever reporting depressive symptoms increased the hazard of all-cause mortality. These results did not differ by gender or baseline psychiatric comorbidities and remained consistent when alcohol use, drug use, and panic disorder were excluded as potential confounders.
Depression has been associated with an increased risk of mortality in a number of previous analyses.[7, 10–14, 38] There are several possible reasons why our results did not confirm previous findings. Depression status is affected by multiple factors including co-morbid mental and physical health conditions, social support, demographic factors and HIV status,[39] many of which may change over time. Time-varying factors, such as ART adherence, may influence the relationship between depression and mortality, and were not fully accounted for in several earlier analyses [7, 11, 13, 14] which did not use IPTWs to address time-varying confounding.
More efficacious ART and improved engagement in HIV care in the modern HIV treatment era may also help to explain a changing relationship between depression and mortality. ART’s efficacy has improved in recent years, making it more robust to moderate adherence. With ART more forgiving of adherence lapses, it is possible that the adverse effects of depression on adherence have become less clinically significant for survival.[17, 18] Depression has also been associated with increased LTFU from HIV care, which could affect access to treatment.[40–43] In our analysis, participants were not censored at LTFU, regardless of depressive symptoms, because mortality status was ascertained irrespective of in-care status. Further, missing PRO assessments were not more common among those who reported depressive symptoms, compared to those with no depressive symptoms.
Depression is also thought to affect mortality by harming elements of innate immunity.[19, 20] However, these negative effects are reversed once the depressive episode subsides.[44] While difficult to confirm, it is possible that access to depression treatment for PLWH has improved over time. Improved access to treatment may result in shorter depressive episodes, which in turn may minimize depression’s deleterious effect on innate immunity. A recent analysis of HIV-infected women, which began follow-up in 1998 (possibly when depression treatment was less common) and measured the effect of always being depressed (e.g. a persistent depression), found a strong effect on mortality (HR increased HR 3.23, 95% CI 1.61, 6.47) and lends support to this hypothesis.[45]
Depression may also affect mortality through its relationships with substance abuse and comorbid psychiatric conditions. Psychiatric illness and substance abuse have been linked to higher mortality among PLWH [46, 47], possibly due to their deleterious effect on ART adherence.[12, 14] In a secondary analysis that did not account for substance abuse (drug and alcohol use) and panic disorder, but did account for ART use and adherence, we observed no evidence of an effect of ever reporting depressive symptoms on all-cause mortality. However, measurement error of mental health comorbidities in our cohort is possible. Chart-documented mental health issues prior to baseline were rare (6% of the population) and PRO assessment of additional mental health issues in CNICS is limited to depression and panic disorder. Further, information on depressive symptoms prior to entering CNICS or counseling-based therapy while in CNICS is not available in our data.
Deaths in our cohort were rare compared to earlier reported estimates. The unadjusted mortality rate was 13.8 deaths per 1,000 person years over 9 years of follow-up. By contrast, the unadjusted mortality rate in a recent analysis of HIV-infected women was 28.9 per 1,000 person-years over 13 years of follow-up, with follow-up starting in 1998.[45] While death rates are declining for HIV-infected adults,[11] the lower death rate observed in our cohort may also reflect some under-counting of deaths. Vital status in CNICS is queried for all participants regardless of their LTFU status, but delays in reporting of vital status to national registries may result in an artificially low number of deaths among participants who are LTFU.[15] In our cohort, 72 deaths (15%) occurred among participants without a clinic visit for ≥ 12 months. Compared to those in care in CNICS, there was no evidence of a lower death rate among participants out of care, suggesting patients may have been engaged in care elsewhere.[15]
Depression is more common among HIV-infected women than men[48] and among persons with comorbid mental health conditions.[46, 47] In our analysis, there was no evidence that gender or psychiatric comorbidities at baseline modified the effect of ever reporting depressive symptoms on mortality. However, CNICS contains only 15% women, and while baseline psychiatric comorbidities were common (20%), deaths were rare (4.5%). Consequently, our analysis may have been underpowered to detect modification by gender or psychiatric comorbidities.
As with all observational studies, our findings rest on several assumptions. These assumptions are 1) no unmeasured confounding (exchangeability), 2) that depression could be eliminated from the population by a well-defined intervention (here conceptualized as antidepressant treatment) and any variation in how antidepressant treatment reduced depression would not change its effect on mortality (consistency and treatment-variation irrelevance) and 3) that conditional on all measured covariates all participants have a non-zero probability of being exposed (positivity).[49, 50] The assumptions of exchangeability and consistency are inherently unverifiable. Additionally, while an intervention that completely eliminates depression in a population is not realistic, antidepressant treatment could be expected to reduce depression through various means (e.g. different drugs or doses), all with the same probable effect on mortality. We note that there is likely some unmeasured confounding by comorbid mental health issues in our analysis, in the absence of observing an effect of ever reporting depressive symptoms on mortality, unmeasured confounding is unlikely to have induced appreciable bias.
Conclusions
In a large cohort of HIV-infected adults in care in the modern treatment era, we observed no evidence that ever reporting depressive symptoms increased the likelihood of all-cause mortality, controlling for a range of time-varying factors. As HIV treatment has become more effective and forgiving to moderate ART adherence, it is possible that depression’s effect on mortality through its role in adherence has diminished. It is also possible that increased clinical awareness about treating depression among PLWH and improved prognosis for survival has led to shorter depressive episodes, mitigating depression’s cumulative effect on innate immunity. Future analyses should consider examining the cumulative burden of depression’s effect on mortality. Finally, given the high burden of depression among HIV-infected adults, effectively treating depression among PLWH continues to be a public health priority.
Acknowledgments
Funding: This work was supported by the National Institutes of Mental Health [grant number R01MH100970] and the National Institute of Allergy and Infectious Diseases [grant number R24AI067039].
BWP, HMC, MJM contributed to the acquisition of the data; AMB, BWP designed the analysis; AMB drafted the manuscript; BWP RM, MMM, WCM, AH, BNG, SN, KC, HMC, MJM assisted with the interpretation of the data and critically revised the manuscript for important intellectual content. All authors take responsibility for and approve the final version of the manuscript. We thank the National Institutes of Mental Health [grant number R01MH100970] and the National Institute of Allergy and Infectious Diseases [grant number R24AI067039] for their support of this work.
Footnotes
Presentation: A version of this work was presented at the Conference on Retroviruses and Opportunistic Infections (CROI) in Boston, February, 2016.
Conflicts of Interest: The authors report no conflicts of interest.
References
- 1.Bing EG, Burnam MA, Longshore D, et al. Psychiatric disorders and drug use among human immunodeficiency virus-infected adults in the United States. Arch Gen Psychiatry. 2001;58(8):721–8. doi: 10.1001/archpsyc.58.8.721. [DOI] [PubMed] [Google Scholar]
- 2.Ciesla JA, Roberts JE. Meta-analysis of the relationship between HIV infection and risk for depressive disorders. Am J Psychiatry. 2001;158(5):725–30. doi: 10.1176/appi.ajp.158.5.725. [DOI] [PubMed] [Google Scholar]
- 3.Bengtson AM, Pence BW, O’Donnell J, et al. Improvements in depression and changes in quality of life among HIV-infected adults. AIDS Care. 2015;27(1):47–53. doi: 10.1080/09540121.2014.946386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Zimpel RR, Fleck MP. Depression as a major impact on the quality of life of HIV-positive Brazilians. Psychology, Health & Medicine. 2013 doi: 10.1080/13548506.2013.772302. [DOI] [PubMed] [Google Scholar]
- 5.Gonzalez JS, Batchelder AW, Psaros C, Safren SA. Depression and HIV/AIDS treatment nonadherence: a review and meta-analysis. J Acquir Immune Defic Syndr. 2011;58(2):181–7. doi: 10.1097/QAI.0b013e31822d490a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Horberg MA, Silverberg MJ, Hurley LB, et al. Effects of depression and selective serotonin reuptake inhibitor use on adherence to highly active antiretroviral therapy and on clinical outcomes in HIV-infected patients. J Acquir Immune Defic Syndr. 2008;47(3):384–90. doi: 10.1097/QAI.0b013e318160d53e. [DOI] [PubMed] [Google Scholar]
- 7.Ickovics JR, Hamburger ME, Vlahov D, et al. Mortality, CD4 cell count decline, and depressive symptoms among HIV-seropositive women: longitudinal analysis from the HIV Epidemiology Research Study. Jama. 2001;285(11):1466–74. doi: 10.1001/jama.285.11.1466. [DOI] [PubMed] [Google Scholar]
- 8.Ironson G, O’Cleirigh C, Fletcher MA, et al. Psychosocial factors predict CD4 and viral load change in men and women with human immunodeficiency virus in the era of highly active antiretroviral treatment. Psychosomatic medicine. 2005;67(6):1013–21. doi: 10.1097/01.psy.0000188569.58998.c8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Leserman J, Jackson ED, Petitto JM, et al. Progression to AIDS: the effects of stress, depressive symptoms, and social support. Psychosomatic medicine. 1999;61(3):397–406. doi: 10.1097/00006842-199905000-00021. [DOI] [PubMed] [Google Scholar]
- 10.Murphy K, Hoover DR, Shi Q, et al. Association of self-reported race with AIDS death in continuous HAART users in a cohort of HIV-infected women in the United States. Aids. 2013;27(15):2413–23. doi: 10.1097/01.aids.0000432537.92958.73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.French AL, Gawel SH, Hershow R, et al. Trends in mortality and causes of death among women with HIV in the United States: a 10-year study. J Acquir Immune Defic Syndr. 2009;51(4):399–406. doi: 10.1097/QAI.0b013e3181acb4e5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Villes V, Spire B, Lewden C, et al. The effect of depressive symptoms at ART initiation on HIV clinical progression and mortality: implications in clinical practice. Antivir Ther. 2007;12(7):1067–74. [PubMed] [Google Scholar]
- 13.Antelman G, Kaaya S, Wei R, et al. Depressive symptoms increase risk of HIV disease progression and mortality among women in Tanzania. J Acquir Immune Defic Syndr. 2007;44(4):470–7. doi: 10.1097/QAI.0b013e31802f1318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lima VD, Geller J, Bangsberg DR, et al. The effect of adherence on the association between depressive symptoms and mortality among HIV-infected individuals first initiating HAART. Aids. 2007;21(9):1175–83. doi: 10.1097/QAD.0b013e32811ebf57. [DOI] [PubMed] [Google Scholar]
- 15.Edwards JK, Cole SR, Westreich D, et al. Loss to clinic and five-year mortality among HIV-infected antiretroviral therapy initiators. PLoS One. 2014;9(7):e102305. doi: 10.1371/journal.pone.0102305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ojikutu B, Higgins-Biddle M, Greeson D, et al. The association between quality of HIV care, loss to follow-up and mortality in pediatric and adolescent patients receiving antiretroviral therapy in Nigeria. PLoS One. 2014;9(7):e100039. doi: 10.1371/journal.pone.0100039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Nelson M, Girard PM, Demasi R, et al. Suboptimal adherence to darunavir/ritonavir has minimal effect on efficacy compared with lopinavir/ritonavir in treatment-naive, HIV-infected patients: 96 week ARTEMIS data. The Journal of antimicrobial chemotherapy. 2010;65(7):1505–9. doi: 10.1093/jac/dkq150. [DOI] [PubMed] [Google Scholar]
- 18.Parienti JJ, Ragland K, Lucht F, et al. Average adherence to boosted protease inhibitor therapy, rather than the pattern of missed doses, as a predictor of HIV RNA replication. Clin Infect Dis. 2010;50(8):1192–7. doi: 10.1086/651419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Cruess DG, Douglas SD, Petitto JM, et al. Association of depression, CD8+ T lymphocytes, and natural killer cell activity: implications for morbidity and mortality in Human immunodeficiency virus disease. Curr Psychiatry Rep. 2003;5(6):445–50. doi: 10.1007/s11920-003-0083-4. [DOI] [PubMed] [Google Scholar]
- 20.Evans DL, Ten Have TR, Douglas SD, et al. Association of depression with viral load, CD8 T lymphocytes, and natural killer cells in women with HIV infection. Am J Psychiatry. 2002;159(10):1752–9. doi: 10.1176/appi.ajp.159.10.1752. [DOI] [PubMed] [Google Scholar]
- 21.Pence BW, O’Donnell JK, Gaynes BN. The depression treatment cascade in primary care: a public health perspective. Current psychiatry reports. 2012;14(4):328–35. doi: 10.1007/s11920-012-0274-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Burnam MA, Bing EG, Morton SC, et al. Use of mental health and substance abuse treatment services among adults with HIV in the United States. Arch Gen Psychiatry. 2001;58(8):729–36. doi: 10.1001/archpsyc.58.8.729. [DOI] [PubMed] [Google Scholar]
- 23.Himelhoch S, Josephs JS, Chander G, Korthuis PT, Gebo KA. Use of outpatient mental health services and psychotropic medications among HIV-infected patients in a multisite, multistate study. Gen Hosp Psychiatry. 2009;31(6):538–45. doi: 10.1016/j.genhosppsych.2009.05.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Taylor SL, Burnam MA, Sherbourne C, Andersen R, Cunningham WE. The relationship between type of mental health provider and met and unmet mental health needs in a nationally representative sample of HIV-positive patients. The journal of behavioral health services & research. 2004;31(2):149–63. doi: 10.1007/BF02287378. [DOI] [PubMed] [Google Scholar]
- 25.Weaver MR, Conover CJ, Proescholdbell RJ, Arno PS, Ang A, Ettner SL. Utilization of mental health and substance abuse care for people living with HIV/AIDS, chronic mental illness, and substance abuse disorders. J Acquir Immune Defic Syndr. 2008;47(4):449–58. doi: 10.1097/QAI.0b013e3181642244. [DOI] [PubMed] [Google Scholar]
- 26.Kitahata MM, Rodriguez B, Haubrich R, et al. Cohort profile: the Centers for AIDS Research Network of Integrated Clinical Systems. Int J Epidemiol. 2008;37(5):948–55. doi: 10.1093/ije/dym231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Saag Michael. Participation rate at CNICS sites. Personal email communication. 2016.
- 28.Brookhart MA. Counterpoint: the treatment decision design. Am J Epidemiol. 2015;182(10):840–5. doi: 10.1093/aje/kwv214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–13. doi: 10.1046/j.1525-1497.2001.016009606.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA. 1999;282(18):1737–44. doi: 10.1001/jama.282.18.1737. [DOI] [PubMed] [Google Scholar]
- 31.Babor TF, Higgins-Biddle JC, Saunders JB, Monteiro MG. Guidelines for Use in Primary Care. Geneva, Switzerland: World Health Organization; 2001. AUDIT, The Alcohol Use Disorders Identification Test. [Google Scholar]
- 32.The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST): development, reliability and feasibility. Addiction. 2002;97(9):1183–94. doi: 10.1046/j.1360-0443.2002.00185.x. [DOI] [PubMed] [Google Scholar]
- 33.Humeniuk R, Ali R, Babor TF, et al. Validation of the Alcohol, Smoking And Substance Involvement Screening Test (ASSIST) Addiction. 2008;103(6):1039–47. doi: 10.1111/j.1360-0443.2007.02114.x. [DOI] [PubMed] [Google Scholar]
- 34.Hernan MA, Brumback B, Robins JM. Marginal structural models to estimate the causal effect of zidovudine on the survival of HIV-positive men. Epidemiology (Cambridge, Mass) 2000;11(5):561–70. doi: 10.1097/00001648-200009000-00012. [DOI] [PubMed] [Google Scholar]
- 35.Cole SR, Hernan MA. Constructing inverse probability weights for marginal structural models. American Journal of Epidemiology. 2008;168(6):656–64. doi: 10.1093/aje/kwn164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Hernan MA, McAdams M, McGrath N, Lanoy E, Costagliola D. Observation plans in longitudinal studies with time-varying treatments. Stat Methods Med Res. 2009;18(1):27–52. doi: 10.1177/0962280208092345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Greenland S, Finkle WD. A critical look at methods for handling missing covariates in epidemiologic regression analyses. American Journal of Epidemiology. 1995;142(12):1255–64. doi: 10.1093/oxfordjournals.aje.a117592. [DOI] [PubMed] [Google Scholar]
- 38.Bouhnik AD, Preau M, Vincent E, et al. Depression and clinical progression in HIV-infected drug users treated with highly active antiretroviral therapy. Antivir Ther. 2005;10(1):53–61. [PubMed] [Google Scholar]
- 39.Hartzell JD, Janke IE, Weintrob AC. Impact of depression on HIV outcomes in the HAART era. The Journal of antimicrobial chemotherapy. 2008;62(2):246–55. doi: 10.1093/jac/dkn193. [DOI] [PubMed] [Google Scholar]
- 40.Traeger L, O’Cleirigh C, Skeer MR, Mayer KH, Safren SA. Risk factors for missed HIV primary care visits among men who have sex with men. J Behav Med. 2012;35(5):548–56. doi: 10.1007/s10865-011-9383-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Zuniga JA, Yoo-Jeong M, Dai T, Guo Y, Waldrop-Valverde D. The Role of Depression in Retention in Care for Persons Living with HIV. AIDS Patient Care STDS. 2016;30(1):34–8. doi: 10.1089/apc.2015.0214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Dombrowski JC, Simoni JM, Katz DA, Golden MR. Barriers to HIV Care and Treatment Among Participants in a Public Health HIV Care Relinkage Program. AIDS Patient Care STDS. 2015;29(5):279–87. doi: 10.1089/apc.2014.0346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Yehia BR, Stewart L, Momplaisir F, et al. Barriers and facilitators to patient retention in HIV care. BMC Infect Dis. 2015;15:246. doi: 10.1186/s12879-015-0990-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Cruess DG, Douglas SD, Petitto JM, et al. Association of resolution of major depression with increased natural killer cell activity among HIV-seropositive women. Am J Psychiatry. 2005;162(11):2125–30. doi: 10.1176/appi.ajp.162.11.2125. [DOI] [PubMed] [Google Scholar]
- 45.Todd JV, Cole SR, Pence BW, et al. Effects of antiretroviral therapy and depressive symptoms on all-cause mortality among HIV infected women. American Journal of Epidemiology. 2016 doi: 10.1093/aje/kww192. In press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.DeLorenze GN, Satre DD, Quesenberry CP, Tsai AL, Weisner CM. Mortality after diagnosis of psychiatric disorders and co-occurring substance use disorders among HIV-infected patients. AIDS Patient Care STDS. 2010;24(11):705–12. doi: 10.1089/apc.2010.0139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Nurutdinova D, Chrusciel T, Zeringue A, et al. Mental health disorders and the risk of AIDS-defining illness and death in HIV-infected veterans. Aids. 2012;26(2):229–34. doi: 10.1097/QAD.0b013e32834e1404. [DOI] [PubMed] [Google Scholar]
- 48.Bengtson AM, Pence PW, Crane HM, et al. Disparities in depression diagnosis and treatment by gender and race/ethnicity among HIV-infected adults in the United States. Under review. PLoS One. 2016 [Google Scholar]
- 49.Robins JM, Hernan MA, Brumback B. Marginal structural models and causal inference in epidemiology. Epidemiology. 2000;11(5):550–60. doi: 10.1097/00001648-200009000-00011. [DOI] [PubMed] [Google Scholar]
- 50.VanderWeele TJ. Concerning the consistency assumption in causal inference. Epidemiology. 2009;20(6):880–3. doi: 10.1097/EDE.0b013e3181bd5638. [DOI] [PubMed] [Google Scholar]