

Abstract
Growth and differentiation factor (GDF) 11 is a member of the transforming growth factor β superfamily recently identified as a potential therapeutic for age‐related cardiac and skeletal muscle decrements, despite high homology to myostatin (Mstn), a potent negative regulator of muscle mass. Though several reports have refuted these data, the in vivo effects of GDF11 on skeletal muscle mass have not been addressed. Using in vitro myoblast culture assays, we first demonstrate that GDF11 and Mstn have similar activities/potencies on activating p‐SMAD2/3 and induce comparable levels of differentiated myotube atrophy. We further demonstrate that adeno‐associated virus‐mediated systemic overexpression of GDF11 in C57BL/6 mice results in substantial atrophy of skeletal and cardiac muscle, inducing a cachexic phenotype not seen in mice expressing similar levels of Mstn. Greater cardiac expression of Tgfbr1 may explain this GDF11‐specific cardiac phenotype. These data indicate that bioactive GDF11 at supraphysiological levels cause wasting of both skeletal and cardiac muscle. Rather than a therapeutic agent, GDF11 should be viewed as a potential deleterious biomarker in muscle wasting diseases.
Keywords: activin receptor, cachexia, cardiac atrophy, muscle mass, myostatin
Subject Categories: Ageing, Musculoskeletal System
Introduction
The transforming growth factor (TGF)β superfamily of signaling proteins consists of a number of ligands having diverse effects. In mammals, there are more than 30 superfamily members that are currently classified into 4 subfamilies based on sequence similarities (Mueller & Nickel, 2012): TGFβs, the bone morphogenic proteins (BMPs)/growth and differentiation factors (GDFs), the activins/inhibins/nodals, and “others”, all having various roles in development, tissue maintenance, tissue repair, and disease. The GDF member, myostatin (Mstn; also known as GDF8), is of particular importance/interest in skeletal muscle as a potent negative regulator of muscle mass (McPherron et al, 1997), and strategies to inhibit its activity have received much focus for the treatment of degenerative and wasting diseases of skeletal muscle (Sumner et al, 2009; Morine et al, 2010a; Zhou et al, 2010). GDF11, which shares 90% homology with Mstn in its mature signaling peptide, has been the subject of recent reports proposing anti‐aging effects in heart (Loffredo et al, 2013), skeletal muscle (Sinha et al, 2014), and brain (Katsimpardi et al, 2014). These data have generated controversy about the physiological effects and therapeutic potential of GDF11, as highlighted in a recent pair of contending viewpoint articles (Harper et al, 2016; Walker et al, 2016).
Like many other members of the TGFβ superfamily, Mstn and GDF11 are both translated as a precursor protein with a secretion signal sequence, a propeptide domain, and a mature peptide domain, with a disulfide bond between two mature peptide domains (forming a dimer). The proteins are further processed by cleavage of the mature peptides from their respective propeptides, though they remain bound in a latent complex such that the propeptides prevent the mature dimer from becoming an active ligand. This latent complex is secreted and can be activated by proteolysis of the propeptides by BMP‐1/tolloid metalloproteinase (Wolfman et al, 2003; Ge et al, 2005), which releases the mature dimer to become a free ligand.
Cell signaling induced by TGFβ superfamily ligands is mediated though several type I and type II receptors that can dimerize in different combinations, based on affinities to the ligand and receptor expression by the cell (Mueller & Nickel, 2012). Mstn and GDF11 are ligands for the activin type II B receptor (ActRIIB; a TGFβ type II receptor). Their binding to ActRIIB recruits either activin‐like kinase (ALK) 4 or ALK5 type I receptors to the complex, activating the canonical ActRIIB signaling pathway through phosphorylation of SMAD2/3, dimerization with SMAD4, and activation of transcriptional activity (Derynck & Zhang, 2003). The TGFβ superfamily can also activate non‐canonical, less elucidated pathways that involve mitogen‐activated protein kinase (MAPKs), including p38 MAPK and extracellular regulated kinase (ERK) pathways (Derynck & Zhang, 2003).
While it is well known that Mstn, through activation of the canonical SMAD2/3 pathway, negatively affects skeletal muscle mass in vitro and in vivo (McPherron et al, 1997; Trendelenburg et al, 2009), the effects of GDF11 on muscle have been less clear, despite the highly similar structure and signaling activation. Unlike the highly muscular Mstn knockout mouse (McPherron et al, 1997), ablation of GDF11 is perinatal lethal and results in skeletal patterning defects (McPherron et al, 1999). Additionally, disruption of GDF11 in skeletal muscle results in no change in phenotype (McPherron et al, 2009), suggesting muscle‐derived GDF11 has a minor, if any, physiological role. This ambiguity of GDF11 function in striated muscle has led to controversy over whether recombinant GDF11 therapy can reverse age‐related cardiac hypertrophy (Loffredo et al, 2013) or skeletal muscle regenerative defects (Sinha et al, 2014). Indeed, several reports have emerged in response to these data, indicating non‐specific GDF11 detection methods (Egerman et al, 2015; Rodgers & Eldridge, 2015; Smith et al, 2015), irreproducibility of GDF11 decline with age (Egerman et al, 2015; Rodgers & Eldridge, 2015), prevention of cardiac hypertrophy (Smith et al, 2015), and the enhancement of muscle regeneration (Egerman et al, 2015; Hinken et al, 2016).
From this controversy, it is clear that the biological effects of GDF11 are not yet clearly delineated. The aim of the present report is to characterize the effects of bioactive GDF11 on differentiated striated muscle tissue. We demonstrate that recombinant GDF11 is a more potent activator of SMAD2/3 than Mstn and induces atrophy in differentiated myotubes. In addition, we report that systemic overexpression of full‐length GDF11 in C57BL/6 mice promotes a severe wasting phenotype in both skeletal and cardiac muscle. While Mstn and GDF11 similarly affect skeletal muscle mass in vivo, GDF11 overexpression leads to lethality.
Results
Recombinant GDF11 induces SMAD2/3 activation and atrophy in C2C12 myotubes
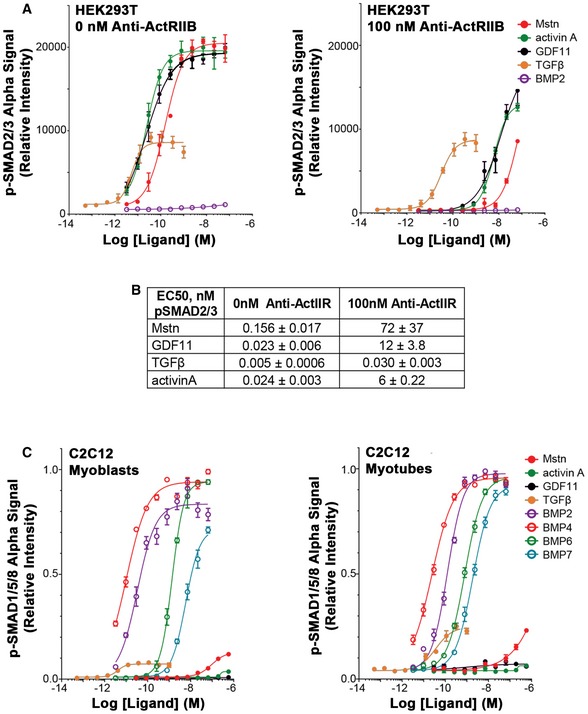
To assess relative potencies of TGFβ superfamily ligands on SMAD activation in vitro, we evaluated canonical signaling for several ligands, including Mstn and GDF11. In HEK293T cells, phosphorylation of SMAD2/3 (p‐SMAD2/3) is potently stimulated by Mstn, GDF11, activin A, and TGFβ (Fig 1A left), while phosphorylation of SMAD1/5/8 (p‐SMAD1/5/8) shows relatively modest stimulation by only activin A (Fig 1A right), especially in comparison with known stimulators of this pathway, such as BMP2 (a BMP type II receptor ligand). We also verified the involvement of the ActRIIB in the responses of Mstn, GDF11, and activin A using a murinized version of the BYM338 antibody that targets ActRIIB (Fig EV1A and B). In the presence of antibody, stimulation of HEK293T cells with GDF11, Mstn, or activin A resulted in > 100‐fold reduced potencies for all three ligands. By comparison, the potency and amplitude of TGFβ stimulation remained unchanged, thus verifying the requirement of ActRIIB for the potencies of affected ligands.
Figure 1. Activation of SMAD pathways by TGFβ superfamily ligands in vitro .
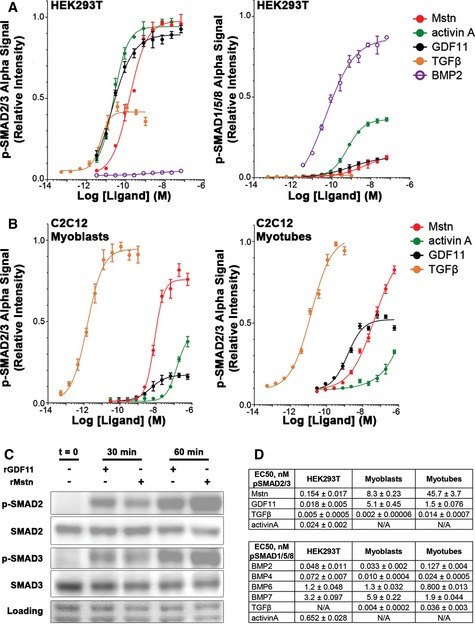
- Relative p‐SMAD2/3 (left) and p‐SMAD1/5/8 (right) response, evaluated by AlphaLISA signal, of HEK293T cells after 1‐h exposure to recombinant myostatin (Mstn), activin A, GDF11, TGFβ, and BMP2.
- Relative p‐SMAD2/3 response of C2C12 myoblasts (left) and myotubes (right) after 1‐h exposure to Mstn, activin A, GDF11, and TGFβ.
- Phosphorylation of SMAD2 and SMAD3 in differentiated C2C12 myotubes following stimulation with recombinant Mstn or GDF11 for 30 and 60 min, as detected by immunoblotting. Equal loading is verified by Ponceau Red staining.
- EC50 values (in nM) for p‐SMAD2/3 and p‐SMAD1/5/8 responses of HEK293T, C2C12 myoblasts, and C2C12 myotubes to the above listed ligands, as well as p‐SMAD1/5/8 response to BMP4, BMP6, and BMP7.
Figure EV1. Additional SMAD response assays to TGFβ ligands.
-
A, BSignificant shifts in the response of HEK293T cells to Mstn, GDF11, and activin A are observed with the addition of ActRIIB antibody (anti‐ActRIIB), when 0 or 100 nM anti‐ActRIIB was applied to HEK293T cells overnight prior to ligand addition and AlphaLISA evaluation. Note that the 0 nM antibody treatment panel is the un‐normalized form of Fig 1A left. EC50 values (in nM) are listed for the antibody data in (B).
-
Cp‐SMAD1/5/8 response of C2C12 myoblasts (left) and myotubes (right) in response to TGFβ family member ligands. All cells were stimulated with ligand 1 h prior to lysis and evaluation by AlphaLISA.
In differentiated C2C12 myotubes (Fig 1B right), TGFβ is a potent stimulator of p‐SMAD2/3, while Mstn and GDF11 demonstrate less potency (~103 less potent than TGFβ), with GDF11 being more potent than Mstn (~30‐fold), and activin A showing even less potency. The maximum level of p‐SMAD2/3, however, is much reduced for GDF11 compared to Mstn. C2C12 myoblasts demonstrate a similar response to these ligands (Fig 1B left), though the relative amplitude of p‐SMAD2/3 in response to GDF11 stimulation over differentiated cells is significantly decreased, while the potency is similar to that observed in myotubes. Effective induction of p‐SMAD2 and p‐SMAD3 in myotubes after 30 and 60 min of exposure to Mstn or GDF11 was also demonstrated by immunoblotting (Fig 1C). Phosphorylation of SMAD1/5/8 in C2C12 myoblasts or myotubes is not affected by GDF11 or Mstn, though BMP ligands potently stimulate this pathway (Fig EV1C). The measureable EC50s of ligands in these experiments are shown in Fig 1D.
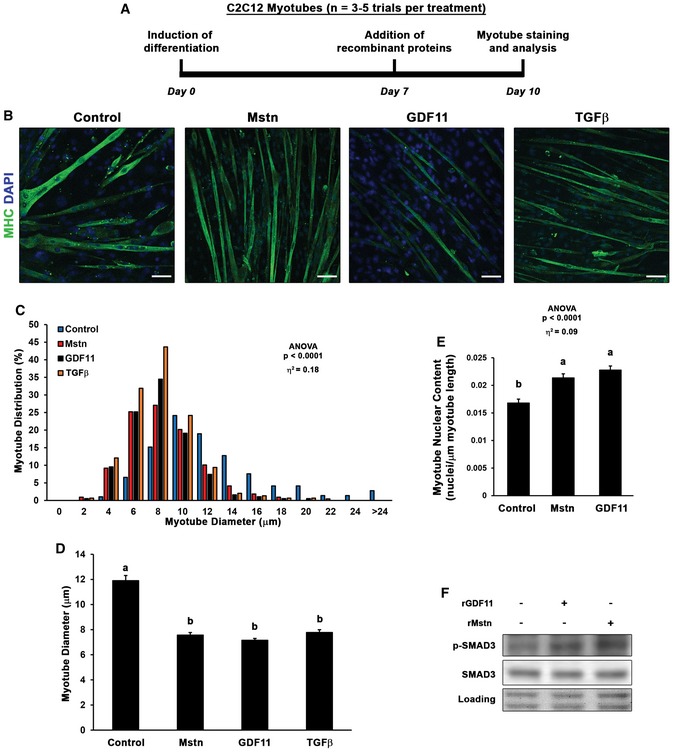
As it has been previously demonstrated that recombinant GDF11 can inhibit myoblast differentiation in vitro (Trendelenburg et al, 2009; Egerman et al, 2015), we sought to determine whether sustained exposure of GDF11 induces atrophy in differentiated myotubes. Thus, at seven days following induction of differentiation of C2C12 myoblasts, we added media supplemented with no ligand, of recombinant (r)Mstn, rGDF11, or rTGFβ (50 ng/ml; depicted in Fig 2A), and analyzed myotube diameter after 3 days of treatment to ensure steady‐state effects of ligand exposure are observed. GDF11‐treated myotube diameter (−40%) was nearly identical in size as Mstn (−36%) and TGFβ‐treated myotubes (−34%), compared to control myotubes (Fig 2B–D). The observed myotube atrophy induced by Mstn and GDF11 does not appear to be due to loss of myonuclei, as myotube nuclear content (normalized to length of myotubes) is actually increased by treatment (Fig 2E). Phosphorylation of SMAD3 via Mstn and GDF11 can also be found in these myotubes (Fig 2F), albeit to a lower degree than the acute stimulation shown in Fig 1C, as is typical for cellular responses to chronic stimuli. Therefore, we conclude that exposure of GDF11 does negatively affect myotube size in vitro in response to the potent activation of p‐SMAD2/3.
Figure 2. GDF11 induces myotube atrophy in vitro .
-
A, BC2C12 myoblasts were differentiated for seven days, then control (n = 5), myostatin (Mstn; n = 4), growth differentiation factor 11 (GDF11; n = 5), or transforming growth factor β (TGFβ; n = 3) supplemented media (50 ng/ml) was added for 3 days (depicted in A) before PFA fixation and staining with myosin heavy chain (MHC) to evaluate myotube diameter (B). The scale bars represent 50 μm.
-
C, DMyotube diameter data (n = 200–400 myotubes from 3 to 5 different trials) are depicted as a histogram of diameter distribution (C) and as mean diameter (mean ± SEM; D) by treatment.
-
EMyotube nuclear content was quantified as DAPI‐positive nuclei per μm of myotube length for control, Mstn, and GDF11 treatment groups.
-
FPhosphorylation of SMAD3 in control, Mstn, and GDF11 treatment groups, as detected by immunoblotting. Equal loading is verified by Ponceau Red staining.
Systemic GDF11 overexpression induces skeletal and cardiac muscle atrophy in vivo
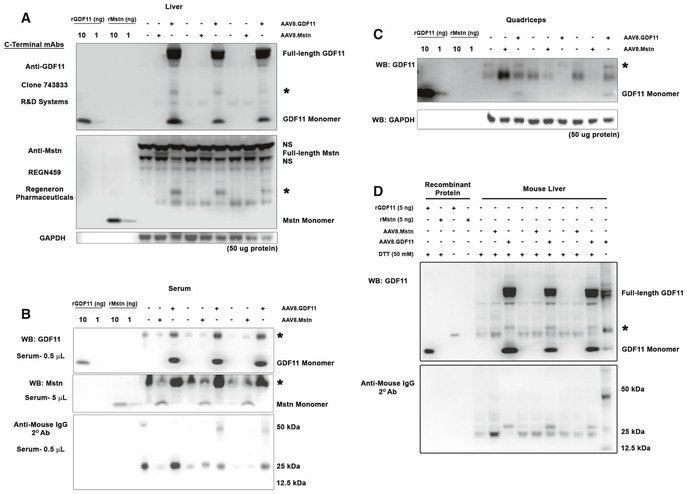
The effects of supraphysiological GDF11 were tested in vivo (scheme depicted in Fig 3A) by treating 12‐week‐old C57BL/6 male mice with full‐length murine GDF11 expressed in the liver using the liver‐specific α1‐anti‐trypsin promoter (with ApoE enhancer) packaged into AAV2/8 (referred hereafter as AAV8.GDF11). Robust expression of the transgene was evident within days, as AAV8.GDF11‐treated mice required euthanasia 7 days following treatment after losing over 35% of their body mass (Fig 3E). The liver exhibited clear expression of full‐length and monomeric GDF11 [Fig 3B; analyzed using R&D Systems' clone 743833 mouse mAb (Egerman et al, 2015; Smith et al, 2015)]. Serum levels of ~60 μg/ml were estimated from the monomeric band [equating to ~3.3 mg/kg for a 23 g mouse (using the standard mouse blood volume of 0.055 ml/g bwt); Fig 3C], while in the quadriceps, monomeric GDF11 content was in the order of 0.001% of the total muscle protein (Fig 3D). Interestingly, each AAV8.GDF11 sample exhibits a ~25 kDa immunoreactive band (denoted with * in Figs 3 and EV2) that is particularly prominent in the serum (immunoreactive with anti‐mouse IgG, yet cannot be depleted by a combination of protein A/G and protein L‐coated agarose beads; Fig EV2D). Also included in these experiments was a group of mice treated with an identical AAV2/8 dose of a construct containing full‐length murine Mstn (AAV8.Mstn). However, due to substantial disparity in expression (detected using anti‐Mstn C‐terminal REGN459 mouse mAb; Fig EV2) between these two viral treatments, AAV8.Mstn data from this seven‐day treatment cohort are only included in the Expanded View data.
Figure 3. Supraphysiological levels of GDF11 cause atrophy of striated muscle in vivo .

-
ATwelve‐week‐old male C57BL/6 mice (n = 3) were injected i.p. with PBS (control) or 1 × 1012 gc of a liver‐specific GDF11 packaged in AAV2/8 (AAV8.GDF11), and were euthanized seven days after treatment.
-
B–DImmunoblotting of IgG‐reduced samples (see Materials and Methods) reveals an increase in GDF11 content in AAV8.GDF11‐treated liver (B), serum (C), and quadriceps (D), as detected by the R&D Systems GDF11 mouse mAb under reducing (50 mM DTT) conditions. The identifiable bands of full‐length GDF11 and monomeric GDF11 in the immunoblots are labeled, while an ambiguous 25 kDa band is marked with a star (*). GAPDH immunoblotting is shown to demonstrate equal loading among lanes.
-
E, FSeven days after, AAV8.GDF11 treatment resulted in substantial losses in body weight (E), and muscle mass of the soleus (Sol), extensor digitorum longus (EDL), tibialis anterior (TA), gastrocnemius (Gas), quadriceps (Quad), and heart (F). Values depicted are mean ± SEM. Statistical analysis was performed using two‐tailed Student's t‐test with effect size presented as Cohen's d (d).
Figure EV2. Antibody validation and overexpression verification.
-
A–CTwelve‐week‐old C57BL/6 male mice were injected i.p. with PBS, a liver‐specific myostatin (Mstn) construct packaged into AAV2/8 (AAV8.Mstn), or a liver‐specific GDF11 construct packaged into AAV2/8 (AAV8.GDF11; n = 3). Verification of GDF11 and Mstn overexpression in the liver (A), serum (B), and quadriceps (C) of treated mice using clone 743833 anti‐GDF11 (R&D Systems #MAB19581) and REGN459 anti‐Mstn (Regeneron Pharmaceuticals) mouse monoclonal antibodies using samples pre‐incubated with protein A/G‐coated agarose beads, to reduce endogenous IgGs, and prepared in reducing conditions. The star (*) represents a 25 kDa band that is specifically prominent in AAV8.GDF11‐treated samples, however, is detected by anti‐mouse IgG secondary antibodies. Note that these are the full immunoblot images for those found in Fig 3B–D.
-
DImmunoblotting for GDF11 (using R&D #MAB19581) with reduced (50 mM DTT) and non‐reduced (no DTT) forms of recombinant GDF11 and Mstn, and liver samples from control, AAV8.Mstn, and AAV8.GDF11 mice subjected to IgG depletion with both protein A/G (targets IgG heavy chains) and protein L (targets IgG light chains)‐coated agarose beads. The differential detection of anti‐mouse IgG immunoreactive bands between AAV8.GDF11‐treated samples and the other groups indicates that GDF11 modifies anti‐mouse IgG immunoreactive species which do not appear to be depletable by incubation with protein A/G or L. The non‐reduced AAV8.GDF11 sample (lane 14) demonstrates both 25 and 12.5 kDa bands immunoreactive with anti‐mouse IgG secondary antibodies, as well. The star (*) represents the ambiguous 25 kDa band mentioned above.
The severe wasting phenotype caused by this robust systemic increase in GDF11 includes skeletal muscle mass loss of 21% in the soleus, 30% in the extensor digitorum longus, 23% in the tibialis anterior (TA), 23% in the gastrocnemius, and 26% in the quadriceps, as well as a 29% loss of heart mass (Fig 3F). This atrophy is evident at the myocyte level, as TA fiber and cardiomyocyte size is decreased by AAV8.GDF11 (Fig 4A and B). Interestingly, long‐term experiments involving manipulations of Mstn/GDF11 (Fig EV3) substantially affect skeletal muscle mass, but not heart mass. For instance, a 12‐week treatment cohort with an equal dose of AAV8.Mstn demonstrates similar muscle mass decrements (relative to respective controls) as the seven‐day AAV8.GDF11 group, though no effects on cardiac mass are seen (Fig EV3A). Additionally, inhibition of either Mstn or GDF11 in the same 12‐week trial by liver targeted overexpression of BMP‐1/tolloid metalloproteinase‐resistant mutations either of Mstn (D76A) or GDF11 (D120A) propeptides (dnMstn and dnGDF11, respectively) results in substantial increases in muscle mass without affecting heart mass (Fig EV3A). Likewise, Mstn knockout mice demonstrate this same trend (Cohn et al, 2007) (Fig EV3B). These data demonstrate that GDF11 causes atrophy in both skeletal and cardiac muscle, but only skeletal muscle atrophy is seen by overexpression of Mstn.
Figure 4. Myofiber and cardiomyocyte atrophy induced by GDF11.
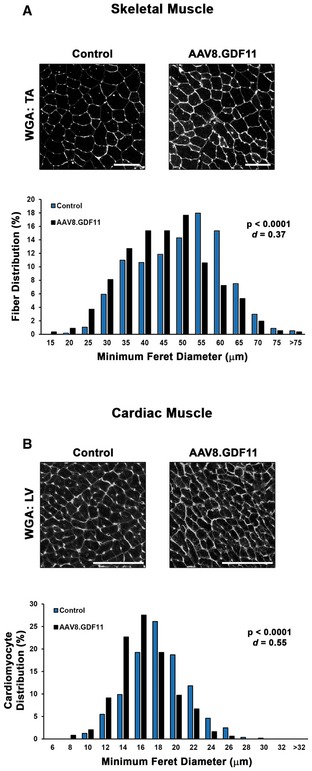
-
A, BWheat germ agglutinin (WGA; Texas Red‐conjugated) stained sections of the tibialis anterior (TA; A) and left ventricle (LV; B) from PBS (control) and liver‐specific GDF11 (AAV8.GDF11)‐treated mice (n = 3) were evaluated for minimum Feret diameter of the individual myocytes (n = 500–600 cells/group). The scale bars represent 100 μm. Myocyte size data are presented as a histogram of minimum Feret diameter distribution. Statistical analysis was performed using two‐tailed Student's t‐test with effect size presented as Cohen's d (d).
Figure EV3. Long‐term Mstn/GDF11 manipulation in vivo .

- Four‐week‐old C57BL/6 male mice were injected IP with PBS (control; n = 6) or 1 × 1012 gc of AAV2/8 packaged liver‐specific constructs of full‐length Mstn (AAV8.Mstn; n = 7), Mstn D76A propeptide (AAV8.dnMstn; n = 3), or GDF11 D120A propeptide (AAV8.dnGDF11; n = 4) and euthanized at 16 weeks of age (84 day treatments).
- Body weights and muscle masses of 12‐week‐old MstnWT/WT (n = 6), MstnWT/KO (n = 6), and MstnKO/KO (n = 4) mice congenic on a C57BL/6 background.
Consistent with previous reports (Egerman et al, 2015) and the in vitro reporter assays described above, systemic elevation by AAV8.GDF11 induced strong phosphorylation of SMAD3 in quadriceps muscle (Fig 5A), suggesting the atrophic effects of GDF11 in skeletal muscle involve the canonical signaling pathway. GDF11 also showed a negative physiological effect on the opposing p‐SMAD1/5/8 pathway (Fig EV4A), while SMAD4 content is variable upon GDF11 stimulation (Fig EV4A). GDF11 also increases Akt content without consistently affecting p‐Akt (Fig 5A), which may be a compensatory response to the atrophy. The systemic overexpression of GDF11 also affects the phosphorylation of p38 MAPK (Fig 5A), suggesting non‐canonical signaling may play a secondary role to the strongly elevated canonical pathway in skeletal muscle. NOX4 content, which was recently shown to have a major role in TGFβ‐mediated muscle dysfunction (Waning et al, 2015), does not appear to be affected by GDF11 (Fig EV4A).
Figure 5. GDF11‐induced signaling and atrogene expression in skeletal and cardiac muscle.
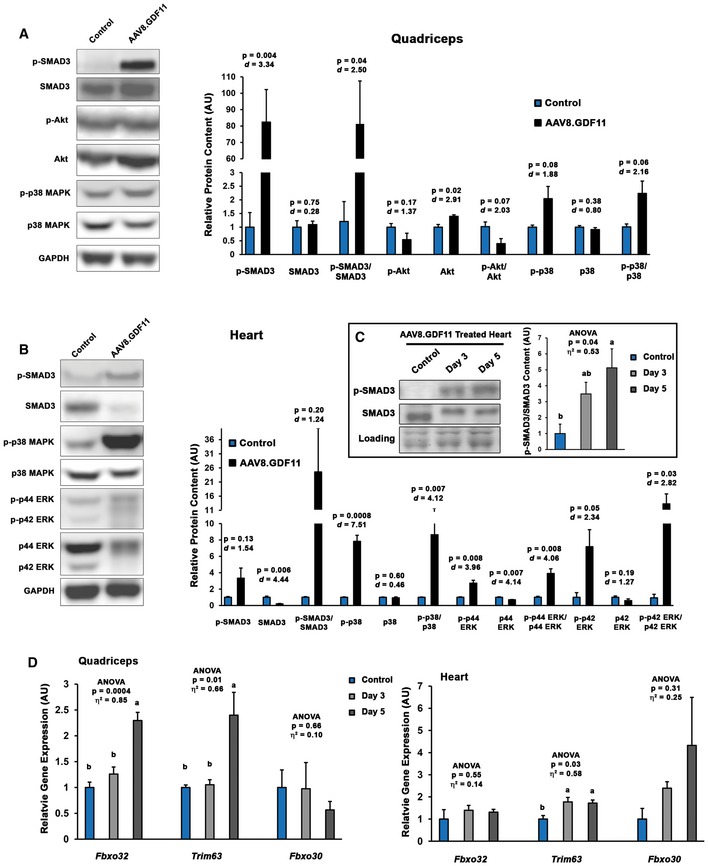
- Immunoblotting data from quadriceps of PBS (control; n = 3) and liver‐specific GDF11 (AAV8.GDF11; n = 3)‐treated male C57BL/6 mice for phosphorylated and total forms of SMAD3, Akt, and p38 MAPK. Loading is normalized by GAPDH content and quantified relative to control values.
- Immunoblotting data for phosphorylated and total forms of SMAD3, p38 MAPK, and p42/p44 ERK in the hearts of control and AAV8.GDF11‐treated male C57BL/6 mice. Loading is normalized by GAPDH content and quantified relative to control values.
- Phosphorylation status of SMAD3 in the hearts of control (n = 3) and AAV8.GDF11‐treated male C57BL/6 mice at 3 days (n = 4) and 5 days (n = 4) following injection. Loading is normalized by Ponceau Red staining and quantified relative to control values.
- Gene expression of Fbxo32 (MAFbx gene), Trim63 (MuRF1 gene), and Fbxo30 (MUSA‐1 gene) in the quadriceps (left) and heart (right) of control (n = 3) and AAV8.GDF11‐treated male C57BL/6 mice at 3 days (n = 4) and 5 days (n = 4) following injection. Relative gene expression values were calculated by the ΔΔCt method using Gapdh as the reference gene.
Figure EV4. Full immunoblots from AAV8.Mstn‐ and AAV8.GDF11‐treated mice.
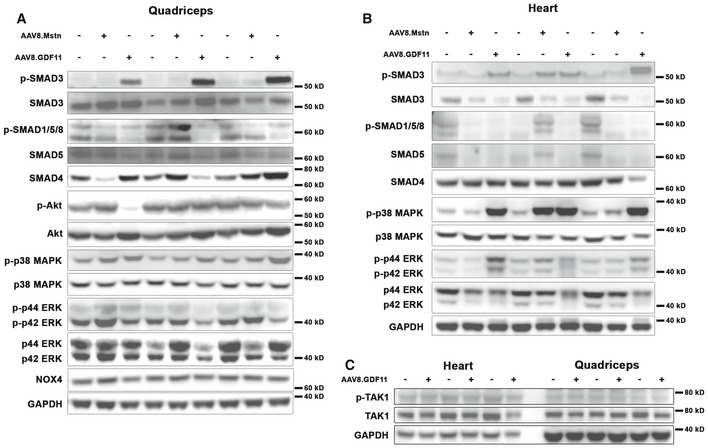
-
A, BQuadriceps (A) and heart (B) lysates from mice described in Figs 2 and EV2 were immunoblotted for phosphorylated and total content of SMAD3, SMAD1/5/8, Akt, p38 MAPK, ERK1/2, total SMAD4, and total NOX4. GAPDH content was used as a loading control and normalization standard. Note that the cropped version of many of these images is found in Fig 5A and B.
-
CPhosphorylation of TAK1 is not different between control and AAV8.GDF11‐treated hearts or quadriceps.
In the heart, the p‐SMAD3 response to AAV8.GDF11 is not as prominent as in skeletal muscle at 7 days following treatment, which coincides with substantial loss of SMAD3 protein in the AAV8.GDF11 group (Fig 5B). Elevated phosphorylation of SMAD3 in the heart is seen at the earlier time points of 3 and 5 days post‐treatment (Fig 5C), suggesting that cardiac muscle may differ at regulating SMAD3 signaling following chronic stimulation than skeletal muscle. As in skeletal muscle, the SMAD1/5/8 pathway is decreased, while SMAD4 content is unchanged (Fig EV4B). Contrary to skeletal muscle, non‐canonical signaling, as evidenced by large increases in the phosphorylation of p38 MAPK and ERK1/2 (Fig 5B), is more highly elevated than the canonical pathway. This activation does not appear to be mediated through stimulation of TGFβ‐activated kinase (TAK) 1 signaling (Fig EV4C).
To determine whether this cachexic phenotype is accompanied by increased expression of muscle “atrogenes”, gene expression of the muscle‐specific E3 ubiquitin ligases Fbxo32 (MAFbx/atrogin‐1 gene), Trim63 (MuRF1 gene), and Fbxo30 (MUSA1 gene) (Bodine et al, 2001; Sartori et al, 2013) was measured in the quadriceps and hearts of mice treated with AAV8.GDF11 for 3 and 5 days (Fig 5D). At 5 days of exposure, modest ~2.5‐fold upregulations of Fbxo32 and Trim63 were found in the quadriceps, while Fbxo30 expression remained unchanged. Trim63 expression in the heart was elevated ~twofold at both days 3 and 5, while Fbxo32 expression was unchanged and Fbxo30 expression became highly variable. These data suggest the striated muscle “atrogene” program is activated by systemic GDF11 overexpression; however, this activation is very modest in comparison with those shown by other atrophy models (Bodine et al, 2001; Sacheck et al, 2007).
Pharmacological levels of full‐length GDF11 uniquely induce cachexia and cardiac atrophy
To determine whether exposure levels similar to those reported to have pharmacological benefit also induce such a degree of muscle atrophy, a dose de‐escalation study was performed using 1 × 1011 gc (hereafter referred to as “mid dose”) and 5 × 1010 gc (low dose) of AAV8.GDF11 in 12‐week‐old mice (Fig EV5A). Similar to the high dose (1 × 1012 gc; described above), AAV‐mediated GDF11 expression was evident within 10 days post‐injection (Fig EV5B), resulting in estimated levels of 0.03–0.09 mg/kg and 0.01–0.02 mg/kg for the mid‐ and low‐dose groups, respectively (based on the above‐mentioned calculations for a 23 g mouse from serum levels of 0.5–1.6 ng/μl and 0.26–0.34 ng/μl, respectively). These levels are below those administered in recent pharmacological studies. The study was terminated at this 10‐day time point due to substantial wasting (~25% loss of body weight) and mobility issues from the mid dose, requiring immediate euthanasia (Fig EV5C). At this time point, the low‐dose group displayed ~10% loss of body weight, though no overt pathology was evident. While mid‐dose mice displayed both skeletal and cardiac muscle atrophy at this time point, the low‐dose group only began to exhibit a cardiac phenotype (Fig EV5D).
Figure EV5. Lower expression levels of GDF11 induce loss of body weight and muscle atrophy.
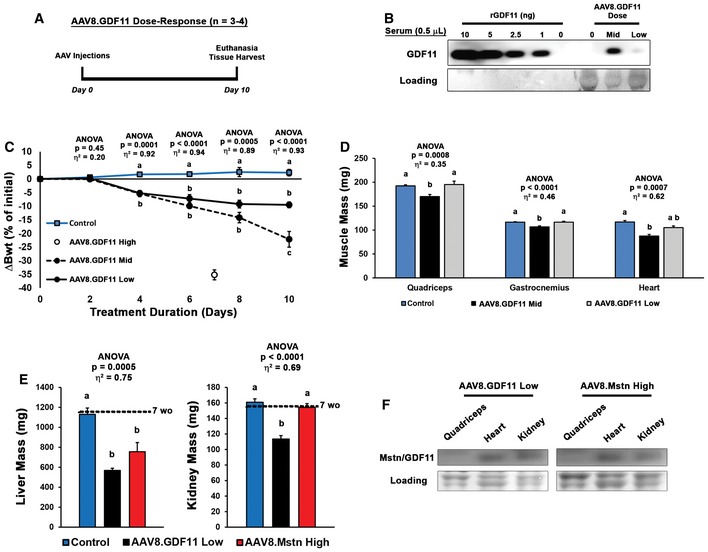
- Eleven‐week‐old C57BL/6 male mice received i.p. injections of PBS (control; n = 4), 1 × 1011 gc of AAV8.GDF11 (mid dose; n = 3), or 5 × 1010 gc of AAV8.GDF11 (low dose; n = 3), and their body weights were monitored every other day until the 1 × 1011 gc AAV8.GDF11 group required euthanasia on day 10.
- Immunoblotting of serum samples for GDF11 demonstrates expression levels of 0.5–1.6 ng/μl and 0.26–0.43 ng/μl for the mid‐ and low‐dose groups, respectively.
- Change in mouse body weights (Bwt) across the 10‐day study by the AAV8.GDF11 treatment groups, including terminal values for the previous 7‐day cohort treated with 1 × 1012 gc of AAV8.GDF11 (high dose).
- Mass of the quadriceps, gastrocnemius, and heart of the 10‐day study mice (n = 12 for control mice by the inclusion of untreated age‐matched mice, resulting in a larger, homogenous data set).
- Liver and kidney mass of 7‐week‐old C57BL/6 male mice were treated with PBS (control; n = 5), AAV8.GDF11 low dose (n = 4), or AAV8.Mstn high dose (n = 5) for 16 days (see Fig 6B). The mean values for 7‐week‐old mice from this colony (n = 5) are indicated by the dotted line to show starting masses.
- Immunoblotting comparison of monomeric GDF11 and Mstn levels in quadriceps, heart, and kidney demonstrate that differential effects are not due to differential accumulation of the ligands in tissue.
From the above data, we hypothesized that Mstn and GDF11 would induce similar phenotypes if expressed at similar levels. As the low dose of AAV8.GDF11 and a high dose (2 × 1012 gc) of AAV8.Mstn demonstrate comparable serum exposures at 10 days post‐injection (Fig 6A), we tested this hypothesis in 7‐week‐old male C57BL/6 mice (experiment depicted in Fig 6B). As displayed in Fig 6C, both Mstn and GDF11 groups lost body mass after treatment, while control mice continued to grow. The GDF11 group began exhibiting signs of severe cachexia beginning at day 14, and the study was terminated following the death of a mouse at day 16 (21% loss of initial body mass by the group). While the Mstn‐treated mice lost ~8% of their initial body mass at this time point, they otherwise appeared healthy and demonstrated normal activity.
Figure 6. Myostatin and GDF11 have differential effects in vivo .

-
ANearly equivalent serum exposure of myostatin (Mstn) and GDF11 can be obtained by treatment with 2 × 1012 gc of AAV8.Mstn (high dose) or 5 × 1010 gc of AAV8.GDF11 (low dose) 10 days following injection.
-
B, CSeven‐week‐old C57BL/6 male mice were treated with PBS (control; n = 5), AAV8.GDF11 low dose (n = 5), or AAV8.Mstn high dose (n = 5) and monitored for 16 days until experiment was terminated due to the death of an AAV8.GDF11‐treated mouse to severe cachexia (depicted in B). The change in body weight (Bwt) in these groups across the 16 days is displayed in (C).
-
D–GMorphological measurements of surviving mice (thus n = 4 for AAV8.GDF11 group) collected at tissue harvest, including Bwt (D), muscle mass of soleus and extensor digitorum longus (EDL), tibialis anterior (TA), gastrocnemius (Gastroc), quadriceps (Quad), and heart (E–F). Heart mass normalized to both Bwt (in g) and tibia length (TL; in mm; G). Mean values for 7‐week‐old mice from this colony (n = 5) are indicated by the dotted lines to show starting masses.
At time of euthanasia, there were no significant differences in absolute body weight or skeletal muscle mass between the Mstn and GDF11 groups (Fig 6D–F); however, the hearts of Mstn‐treated mice did not show the atrophic effects seen in those treated with GDF11. Even when normalized to either body weight or tibia length, Mstn‐treated hearts were larger than those with GDF11 treatment (Fig 6G). Stomach contents were comparable between the treatment groups, suggesting anorexia was not responsible for this wasting phenotype. Likewise, the observed differences in mass are due to atrophy of the tissues, not failure to grow, as the values for 7‐week‐old mice from this colony are similar to control treatment values. Interestingly, both Mstn‐ and GDF11‐affected liver mass, while only GDF11 atrophied the kidneys (Fig EV5E). These divergent effects of the ligands on heart and kidney mass are not due to differential accumulation of GDF11 and Mstn in the tissue (Fig EV5F), which appears, as one would expect, to be proportional to tissue vascularity.
Receptor expression patterns differ between skeletal and cardiac muscle
As Mstn and GDF11 affect skeletal muscle mass similarly and only GDF11 affects the heart, it is possible differential receptor utilization may occur in a tissue‐specific context, resulting in divergent effects of the ligands on cardiomyocytes at the levels expressed in this study. We thus investigated associated receptor levels/expression in skeletal muscle and heart. The heart contains nearly twofold the content of the common type II receptor, ActRIIB, as quadriceps, which was unchanged in either tissue by ligand manipulation (Fig 7A and B). Though gene expression of Acvr1b (ALK4 gene) is comparable between heart and quadriceps (Fig 7C), the expression of Tgfbr1 (ALK5 gene) is nearly twofold higher in the heart (Fig 7D). When normalized to Acvr1b, the heart contains ~60% more Tgfbr1 than the quadriceps (Fig 7E), which suggests that signaling induced by either GDF11 or Mstn in the heart is more likely to be mediated by ALK5 than ALK4, the primary mediator of Mstn signaling in myoblasts (Kemaladewi et al, 2012) and possibly mature muscle. At these expression levels, it is possible that GDF11 binding to ActRIIB may preferentially recruit ALK5 more so than Mstn, explaining the differential effects of the two ligands in the heart. The heightened Tgfbr1 expression in the heart is likely linked to the 5.5‐fold higher gene expression of Tgfb1 in the heart than skeletal muscle (Fig 7F), as TGFβ signals through dimerization of ALK5 with TGFβ type II receptor (TβRII) and is a positive regulator of cardiomyocyte size (Rosenkranz, 2004). Thus, differential receptor profiles between skeletal and cardiac muscle offer a potential explanation for the potent effects of GDF11 on cardiac mass in comparison with Mstn. Marked elevation of Tgfb1 expression in the heart following 3 and 5 days of exposure to high‐dose AAV8.GDF11 (Fig 7G) supports this hypothesis, as it appears the heart is upregulating Tgfb1 to compensate for the loss of cardiomyocyte mass.
Figure 7. Differential activin receptor levels in skeletal muscle and heart.

-
A, BRelative muscle content of the activin type IIB receptor (ActRIIB) in quadriceps (n = 6) and hearts (n = 4) from multiple treatment groups, as determined by immunoblotting (normalized to Ponceau‐visualized loading).
-
C–FGene expression of Acvr1b (ALK4 gene; C), Tgfbr1 (ALK5 gene; D and E), and Tgfb1 (F) in quadriceps and heart of untreated 7‐week‐old C57BL/6 mice (n = 3), as measured by real‐time PCR. Relative gene expression values were calculated by the ΔΔCt method using Gapdh (C, D and F) or Acvr1b (E) as reference genes.
-
GCardiac gene expression of Tgfb1 in control (n = 3), day 3 (n = 4), and day 5 (n = 4) high‐dose (1 × 1012 gc) AAV8.GDF11‐treated C57BL/6 mice. Relative gene expression values were calculated by the ΔΔCt method using Gapdh as the reference gene.
Discussion
Given the recent controversy surrounding GDF11 as an anti‐aging therapy (Harper et al, 2016; Walker et al, 2016), it is clear that additional mechanistic studies on this TGFβ superfamily member are required. While the physiological role of endogenous GDF11 in postnatal striated muscle remains ambiguous, the biomedical importance of this ligand is exemplified by the recent demonstration that elevated GDF11 levels associate with patient frailty and problematic recovery following cardiovascular disease (CVD) intervention (Schafer et al, 2016). In the current report, we demonstrate that recombinant GDF11 and Mstn similarly act through the canonical SMAD2/3 pathway and reduce myotube diameter in vitro. Additionally, we provide evidence that overexpression of full‐length, bioactive GDF11 is a powerful inducer of atrophy in both skeletal and cardiac muscle and induces a severe cachexic phenotype in vivo. Thus, it is not likely a candidate for an “anti‐aging” therapeutic.
TGFβ superfamily ligands can have substantial influence on skeletal muscle mass. In addition to the muscle effects of Mstn (described and demonstrated above), activin A, also an ActRIIB ligand, induces muscle atrophy (Chen et al, 2014) and has been implicated (along with Mstn) in cancer‐induced muscle wasting (Zhou et al, 2010). Soluble ActRIIB or anti‐ActRIIB antibodies, which can block activity of Mstn, GDF11, and activin A, substantially increase muscle mass and improve muscle wasting phenotypes (Morine et al, 2010b; Zhou et al, 2010). TGFβ1, signaling through ALK5 and TβRII to activate SMAD2/3, also induces a muscle atrophy phenotype (Mendias et al, 2012; Narola et al, 2013). Conversely, activation of the SMAD1/5/8 pathway via BMP receptor signaling promotes muscle hypertrophy (Sartori et al, 2013; Winbanks et al, 2013). It is therefore not surprising that GDF11, which similarly ligates to ActRIIB and activates SMAD2/3 as Mstn, induces skeletal muscle atrophy in vitro and in vivo.
In the current study, an estimated dose of 0.01 mg/kg (based on 0.055 ml/g bwt of blood volume for a 23 g mouse; http://www.informatics.jax.org/mgihome/other/mouse_facts1.shtml) of bioactive GDF11 is enough to induce substantial cachexia in male C57BL/6 mice in < 3 weeks of treatment. As none of the recent studies involving rGDF11 treatments (ranging from 0.1 mg/kg; Loffredo et al, 2013; Sinha et al, 2014; Egerman et al, 2015; Smith et al, 2015; to 1 mg/kg; Poggioli et al, 2016; daily) clearly provide skeletal muscle mass data, it is uncertain whether skeletal muscle atrophy occurred as a result of GDF11 administration in these studies. This is a critical omission for proposals of anti‐aging effects of GDF11, as further loss of skeletal muscle mass will severely decrease the quality of life for the elderly and CVD patients, which will result from elevating GDF11. Indeed, the recent report by Schafer et al (2016) depicts elevations in endogenous GDF11 as being major detriment to patients with co‐morbidities. While it is possible that the ligands used in the aforementioned studies (i.e., mature GDF11 dimer produced in bacteria) are either less potent or have different biological effects as those produced in vivo, thus contributing to the discrepancy in reported results, in vitro data reported in this work suggest the recombinant protein does display high, ActRIIB‐dependent potency when administered in cell culture.
An interesting and unexpected finding of the current work is the increased susceptibility of cardiac muscle to GDF11‐induced atrophy. While systemic manipulation (whether Mstn or dnMstn) and genetic deletion of Mstn display minimal effects in the heart despite dramatic changes to skeletal muscle, cardiac‐specific expression of Mstn or dnMstn does affect cardiomyocyte size (Bish et al, 2010; Heineke et al, 2010). This demonstrates Mstn can affect cardiac mass and suggests Mstn is more effective in autocrine fashion in the heart, while systemic levels (even at the levels expressed in the current study) are inadequate to affect cardiac muscle size. We propose a possible explanation for this phenomenon to be differential receptor profiles and utilization between heart and skeletal muscle, as evidenced by increased ActRIIB content and Tgfbr1:Acvr1b expression in the heart. As ALK4 is the primary mediator of Mstn signaling in myoblasts (Kemaladewi et al, 2012), is it reasonable to suspect that Mstn binding to ActRIIB preferentially recruits ALK4 as the type I receptor to initiate signaling. Likewise, GDF11 binding may preferentially recruit ALK5, explaining the differential effects of the two ligands in the heart. Additionally, the heart expresses more Tgfb1 than skeletal muscle; therefore, it is also possible that the atrophic effects of GDF11 of on the heart could additionally involve ActRIIB out‐competing TβRII for ALK5. We cannot, however, rule out the possibility of signaling modulators, such as the co‐receptor cripto (Kemaladewi et al, 2012), or receptor post‐translational modifications, such as SUMOylation (Miyazono et al, 2008), being involved in these divergent effects of Mstn and GDF11 on cardiac muscle, as well.
Another element of the existing GDF11 debate concerns proper reagents for the detection of GDF11 (Egerman et al, 2015; Rodgers & Eldridge, 2015; Poggioli et al, 2016). As shown by Egerman et al (2015), both the SOMAmer and the anti‐GDF11 antibody (Abcam #ab124721; now labeled as anti‐GDF8/11) used in the initial report by Loffredo et al (2013) detect Mstn and GDF11 to similar extents. In this study, an assay utilizing the GDF11‐specific clone 743833 [R&D Systems; specificity replicated previously (Smith et al, 2015) and in the current report] suggests GDF11 immunoreactivity is increased with age in both rat and human serum. In the present study, we used antibodies verified to be specific for both full‐length and monomeric GDF11 and Mstn (clone 743833 and REGN459, respectively; Fig EV2), allowing us to reliably detect either species in IgG‐reduced tissue lysate and serum.
As Poggioli et al (2016) attribute some of the immunoreactivity of ab124721 to be IgG light chains (hence appearing as Mstn/GDF11 dimer at ~25 kDa), we find an ambiguous 25 kDa anti‐mouse IgG immunoreactive band detected in AAV8.GDF11‐treated samples, which cannot be removed with pre‐treatment of samples with protein A/G and/or protein L‐coated agarose beads (Fig EV2D). Furthermore, purified rGDF11 does not react with anti‐mouse IgG in either reduced or non‐reduced forms (Fig EV2D). These observations suggest the detection of dimeric GDF11 from biological samples (both reducing and non‐reducing) may be further complicated by anti‐mouse IgG immunoreactive species that appear to be induced by increasing GDF11 levels, and is perhaps the same species detected by Abcam's ab124721.
With the current debate over the therapeutic potential of GDF11 for age‐related phenomena, a greater understanding of the role of this protein in physiological and pathological processes is needed. In the current report, it is shown that GDF11 is a potent negative regulator of striated muscle mass when expressed at supraphysiological levels. While it is still unclear what role, if any, that GDF11 plays in normal striated muscle physiology, it clearly activates similar pathways as its close relative, Mstn, and can induce pronounced muscle wasting and cachexia when elevated systemically. In fact, the degree of atrophy in skeletal and cardiac muscle demonstrated by this ligand is very reminiscent of that found in a severe murine model of cancer cachexia, which is ameliorated by anti‐ActRIIB treatment (Zhou et al, 2010). Interestingly, GDF11 has been suggested to be expressed by human cancers (Yokoe et al, 2007). This suggests caution should be used when considering the therapeutic potential of GDF11, as the presently described data suggest its true biological actions would greatly exacerbate muscle loss in already susceptible populations. In light of recent reports (Schafer et al, 2016) and the currently described data, we suggest that the biomedical focus of GDF11 to shift away from therapeutic potential and toward its potential role as a pathological effector/biomarker, particularly in conditions of muscle wasting.
Materials and Methods
AlphaLISA assays
To assess the phosphorylation of SMAD in response to TGFβ superfamily members in undifferentiated cells, C2C12 myoblasts (ATTC CRL‐1772; passage 14) and HEK293T cells (ATCC CRL‐11268; passage 13) were plated on 96‐well tissue culture‐treated plates (Greiner‐Bio‐One 655098) in growth medium [high glucose Dulbecco's modified Eagle's medium (DMEM) + 10% fetal bovine serum (FBS) + 1% penicillin streptomycin (PS)], grown to confluency, and were treated with various doses of the following recombinant ligands for 1 h (n = 4): Mstn (R&D Systems #788‐G8), GDF11 (R&D Systems # 1958‐GD), TGFβ (R&D Systems #240‐B), activin A (R&D Systems # 338‐AC), BMP‐2 (R&D Systems # 355‐BM), BMP‐4 (R&D Systems # 314‐BP), BMP‐6 (R&D Systems # 507‐BP), or BMP‐7 (R&D Systems # 354‐BP). All recombinant proteins were reconstituted according to the manufacturer's instructions. Cells were lysed using Phosphosafe Buffer (VWR EM71296‐4) for 45 min, and phosphorylation of SMAD2/3 or SMAD1/5/8 was determined using AlphaLISA Surefire Ultra kits (PerkinElmer ALSU‐PSM3 or ALSU‐PSM1, respectively) read on a PerkinElmer EnVision 2103 Multilabel reader. The Alpha signal was normalized to the maximum signal measured for that cell type and readout (either p‐SMAD2/3 or p‐SMAD1/5/8), so that relative contributions of each ligand to the p‐SMAD signal could be evaluated.
To assay ligand response in differentiated myotubes, C2C12 myoblasts were plated on in growth medium until confluency (~24 h), after which were switched to differentiation medium (DMEM + 2% horse serum + 1% PS) to induce differentiation to myotubes (day 0). Media was exchanged on day 2. At day 6, myotube cultures were treated with various doses of the recombinant ligands (listed above) for 1 h (n = 4), and SMAD phosphorylation was assayed as mentioned above. For ActRIIB antibody (anti‐ActRIIB) assays, HEK293T cells were treated with 0 or 100 nM anti‐ActRIIB (Creative BioMart, murinized version of BYM338 antibody; Lach‐Trifilieff et al, 2014) overnight prior to ligand addition, lysing, and AlphaLISA evaluation, as described above.
Myotube diameter assay
C2C12 myoblasts (ATTC CRL‐1772; maintained between passages 3 and 7) were cultured in growth medium until confluency, after which were switched to differentiation medium (low glucose DMEM + 2% FBS + 1% PS) to induce differentiation to myotubes (day 0, as depicted in Fig 2A). At day 7 of differentiation, myotube cultures were separated into control (n = 5), 50 ng/ml recombinant Mstn (R&D Systems #788‐G8; n = 4), 50 ng/ml recombinant GDF11 (R&D Systems #1958‐GD; n = 5), or 50 ng/ml recombinant TGFβ (R&D Systems #240‐B; n = 3) enriched differentiation media for 72 h. All recombinant proteins were reconstituted according to the manufacturer's instruction in 4 mM HCl with 0.1% bovine serum albumin (BSA).
At day 10, cultures were fixed in 4% paraformaldehyde (PFA), permeabilized in 0.1% Triton X‐100, and blocked in 0.2% BSA for 1 h. Myotubes were stained with anti‐myosin heavy chain (clone MY‐32; Sigma‐Aldrich #M1570; St. Louis, MO) overnight, incubated with Alexa‐568‐conjugated goat anti‐mouse secondary antibody (Life Technologies #A11031; Grand Island, NY) for 1 h, and counter stained with DAPI (Sigma‐Aldrich). Images were acquired with a Leica TSC‐SP8 confocal microscope and analyzed by Leica LAS X software (200–400 myotubes per condition).
Animals
All procedures and experiments were approved by and conducted in accordance of the University of Pennsylvania IACUC and the University of Florida IACUC. This study used male C57BL/6J mice from colonies originally obtained from Jackson Laboratory (Stock #000664). MstnKO/KO, wild‐type, and heterozygous littermates are congenic on the C57BL/6 background. Mice were housed 3–5 mice per cage, randomly assigned into treatment groups, provided ad libitum access to food and water with enrichment, and maintained on a 12‐h light/dark system. Following allotted time, mice were euthanized. Muscles were quickly dissected, weighed, and either snap‐frozen in liquid N2 or embedded in OCT and frozen in melting isopentane. The apical half of the heart was snap‐frozen, while the rest was frozen in OCT. Frozen tissue was stored at −80°C until analysis. Sample sizes were determined based on power analyses of primary measures from previous studies. Mice were randomized prior to treatment protocols.
Adeno‐associated virus production and treatment
Codon optimized cDNA encoding full‐length mouse GDF11 (NP_034402) and the D120A GDF11 propeptide (Ge et al, 2005; dnGDF11) were synthesized (Integrated DNA Technologies; Coralville, IA). These constructs, full‐length Mstn, and the D76A Mstn propeptide (Morine et al, 2010a) (dnMstn) were cloned behind the liver‐specific α1‐antitrypsin promoter with ApoE enhancer in the pLSP AAV shuttle vector (Morine et al, 2010a), and were packaged into adeno‐associated virus (AAV) pseudotype 2/8 by the University of Pennsylvania vector core. Mice were injected i.p. with the specified genome content (gc) of virus diluted to 50 μl in sterile PBS. Control animals received 50 μl of PBS.
Immunoblotting
Snap‐frozen samples were finely crushed and homogenized in T‐PER buffer (Thermo Scientific; Waltham, MA) supplemented with protease and phosphatase inhibitors (Thermo Scientific). Protein concentration of resulting supernatant was determined using Bio‐Rad Protein Assay (Bio‐Rad; Hercules, CA). Serum samples were diluted to the indicated concentration in PBS. Endogenous mouse IgGs were reduced from samples intended for analysis with mouse monoclonal antibodies by two 1‐h incubations with protein A/G‐coated agarose beads (Santa Cruz Biotechnology #sc‐2003; Dallas, TX; pre‐cleaned with homogenization buffer) at 4°C. Protein L‐coated agarose beads (Santa Cruz #sc‐2336) were used where indicated to remove IgG light chains. Lysates were removed from beads following each incubation by centrifugation at 1,000 g and removing the supernatant.
Protein samples were boiled for 10 min in 4× sample buffer containing 50 mM DTT (unless under non‐reducing conditions), subjected to SDS–PAGE using 4–12% SDS–polyacrylamide gels (Life Technologies), and transferred to nitrocellulose membranes using the iBlot system (Life Technologies). Unless otherwise noted, 50 μg of tissue homogenates was loaded per lane. Membranes were blocked in 5% milk‐TBST or 5% BSA‐TBST, and incubated with primary antibody overnight at 4°C. Following TBST washes, membranes were incubated in the appropriate HRP‐conjugated anti‐rabbit (Cell Signaling #7074; Danvers, MA) or anti‐mouse (Cell Signaling #7076) secondary antibody for 1 h at room temperature, washed, incubated for 5 min in ECL reagent (Thermo Scientific), and imaged using the LI‐COR C‐DiGit (LI‐COR Biosciences; Lincoln, NE) imaging system. Blots for phosphorylated proteins were stripped and re‐probed for total protein, unless initial signal was too strong to be reliably removed by stripping buffer. All membranes underwent a final probe for GAPDH (Santa Cruz Biotechnology #sc‐25778) and were stained with Ponceau Red for equal loading verification. Band signal intensities were measured using Image Studio Lite software (LI‐COR Biosciences), normalized to sample loading, and reported relative to respective control samples. Primary antibodies used for this study include the following: GDF11 (R&D Systems #MAB19581; Minneapolis, MN), Mstn (C‐terminal; kind gift from Regeneron Pharmaceuticals), p‐SMAD2 (S465/467; Cell Signaling #3108), SMAD2 (Cell Signaling #5339), p‐SMAD3 (S423/425; Cell Signaling #9520), SMAD3 (Cell Signaling #9523), p‐SMAD1/5/8 (S463/465; Cell Signaling #9511), SMAD5 (Cell Signaling #12534), SMAD4 (Cell Signaling #9515), p‐Akt (S473; Cell Signaling #9271), Akt (Cell Signaling #9272), p‐p38 MAPK (T180/Y182; Cell Signaling #9211), p38 MAPK (Cell Signaling #9212), p‐ERK1/2 (T204/Y204; Cell Signaling #9101), ERK1/2 (Cell Signaling #9102), NOX4 (Abcam #ab133303; Cambridge, MA), p‐TAK1 (T184/187; Cell Signaling #4531), TAK1 (Cell Signaling #4505), ActRIIB (Sigma‐Aldrich #A0457), and Mstn/GDF11 (Abcam #ab124721).
Muscle fiber and cardiomyocyte size
OCT‐embedded tibialis anterior and heart samples were sectioned at 10 μm, fixed in ice‐cold acetone for 10 min, and stained with Texas Red‐conjugated WGA (Life Technologies) diluted 1:500 in PBS for 1 h. Following incubation, slides were washed with PBS, coversliped with Vectashield (Vector Labs; Burlingame, CA) mounting medium, and imaged using a Leitz DMRBE microscope equipped with a Leica DCF480 digital camera. Myocyte size analysis (n = 500–600 cells/group) was performed using ImageJ software by investigators blind to experimental design, and recorded as minimum Feret diameter in μm.
Real‐time PCR
RNA was isolated from finely crushed snap‐frozen mouse quadriceps and heart samples using Trizol Reagent (Life Technologies), treated with DNAse (Promega; Madison, WI), and reverse transcribed using the SuperScript III kit (Life Technologies). Resulting cDNA was subjected to real‐time PCR using RQG SYBR Green supermix (Qiagen) in a Rotor Gene Q real‐time PCR machine (Qiagen). The following mouse‐specific primers were used: Fbxo32 (forward) 5′‐GCA GCC GCT CAG CAT TCC CA‐3′ and (reverse) 5′‐ACC GAC GGA CGG GAC GGA TT‐3′; Trim63 (forward) 5′‐AGG GCT CCC CAC CAC TGT GT‐3′ and (reverse) 5′‐TTG CCC CTC TCT AGG CCA CCG‐3′; Fbxo30 (forward) 5′‐ATC GAT GGC CCG TTA GTT ATT CA‐3′ and (reverse) 5′‐GCC CCT ATC TCA CCC TCA TCA AG‐3′; Acvr1b (forward) 5′‐GAA CCG CTA CAC AGT GAC CA‐3′ and (reverse) 5′‐ AAT TCC CGG CTT CCC TTG AG‐3′; Tgfbr1 (forward) 5′‐GCA TTG GCA AAG GTC GGT TT‐3′ and (reverse) 5′‐TGC CTC TCG GAA CCA TGA AC‐3′; Tgfb1 (forward) 5′‐GAC TCT CCA CCT GCA AGA CCA T‐3′ and (reverse) 5′‐GGG ACT GGC GAG CCT TAG TTT‐3′; Gapdh (forward) 5′‐AGC AGG CAT CTG AGG GCC CA‐3′ and (reverse) 5′‐ TGT TGG GGG CCG AGT TGG GA‐3′. Relative gene expression quantification was performed using the ΔΔCt method with either Gapdh or Acvr1b as the reference gene.
Statistical analysis
Statistical analysis was performed using unpaired, two‐tailed Student's t‐test or one‐way ANOVA followed by Tukey's HSD post hoc test (when ANOVA P < 0.05), where appropriate. Effect size is reported as Cohen's d (d) for t‐test analyses, and as eta‐squared (η2) for ANOVA analyses. Values are displayed as mean ± SEM. No data points were excluded from analysis in this study.
Author contributions
This study was designed by DWH, MM‐B, JYH, JJH, SE, and HLS. Experiments and data collection were performed by DWH, MM‐B, JYH, and JJH. Data analysis and interpretation were performed by DWH, MM‐B, JYH, and HLS. DWH, JYH, and HLS drafted and revised the manuscript.
Conflict of interest
JYH, SE, and JJH were employees of Cytokinetics Inc. at the time of this study. The other authors declare that they have no conflict of interest.
The paper explained.
Problem
The transforming growth factor β superfamily of signaling ligands can have substantial influence on striated muscle mass. Growth and differentiation (GDF) 11, a member of this family, has been purported as a therapeutic for striated muscle decrements; however, the effects of this molecule on muscle mass have not been described despite high homology to myostatin (Mstn), a potent stimulator of muscle atrophy. The objective of the current report was to delineate the effects of bioactive GDF11 on striated muscle mass.
Results
In cell culture experiments, we found that GDF11 and Mstn have similar signaling and atrophy‐inducing activities in skeletal myocytes. Using adeno‐associated virus to induce systemic overexpression of GDF11 in mice, substantial atrophy of skeletal and cardiac muscle was seen, resulting in a lethal wasting phenotype which did not occur in mice expressing similar levels of Mstn.
Impact
These data indicate that bioactive GDF11 at supraphysiological levels are not beneficial to striated muscle, causing wasting of both skeletal and cardiac muscle. Rather than a therapeutic agent, GDF11 is a deleterious biomarker involved in muscle wasting.
Supporting information
Expanded View Figures PDF
Review Process File
Acknowledgements
This work was funded by a Wellstone Muscular Dystrophy Cooperative Center grant (U54‐AR‐052646) from the NIH to HLS, Leducq Foundation funding (13CVD04) to HLS, and from funding from the Parent Project Muscular Dystrophy to HLS. The authors acknowledge and greatly appreciate the assistance of Jennifer Pham, Pedro Acosta, Alexandra Agathis, Adam George, Chris Philips, Morgan Venuti, and Cora Coker for their contributions in this study. We also thank Regeneron Pharmaceuticals for generously providing their myostatin C‐terminal antibody.
EMBO Mol Med (2017) 9: 531–544
References
- Bish LT, Morine KJ, Sleeper MM, Sweeney HL (2010) Myostatin is upregulated following stress in an Erk‐dependent manner and negatively regulates cardiomyocyte growth in culture and in a mouse model. PLoS ONE 5: e10230 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bodine SC, Latres E, Baumhueter S, Lai VK, Nunez L, Clarke BA, Poueymirou WT, Panaro FJ, Na E, Dharmarajan K et al (2001) Identification of ubiquitin ligases required for skeletal muscle atrophy. Science 294: 1704–1708 [DOI] [PubMed] [Google Scholar]
- Chen JL, Walton KL, Winbanks CE, Murphy KT, Thomson RE, Makanji Y, Qian H, Lynch GS, Harrison CA, Gregorevic P (2014) Elevated expression of activins promotes muscle wasting and cachexia. Faseb J 28: 1711–1723 [DOI] [PubMed] [Google Scholar]
- Cohn RD, Liang HY, Shetty R, Abraham T, Wagner KR (2007) Myostatin does not regulate cardiac hypertrophy or fibrosis. Neuromuscul Disord 17: 290–296 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Derynck R, Zhang YE (2003) Smad‐dependent and Smad‐independent pathways in TGF‐beta family signalling. Nature 425: 577–584 [DOI] [PubMed] [Google Scholar]
- Egerman MA, Cadena SM, Gilbert JA, Meyer A, Nelson HN, Swalley SE, Mallozzi C, Jacobi C, Jennings LL, Clay I et al (2015) GDF11 increases with age and inhibits skeletal muscle regeneration. Cell Metab 22: 164–174 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ge G, Hopkins DR, Ho WB, Greenspan DS (2005) GDF11 forms a bone morphogenetic protein 1‐activated latent complex that can modulate nerve growth factor‐induced differentiation of PC12 cells. Mol Cell Biol 25: 5846–5858 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harper SC, Brack A, MacDonnell S, Franti M, Olwin BB, Bailey BA, Rudnicki MA, Houser SR (2016) Is growth differentiation factor 11 a realistic therapeutic for aging‐dependent muscle defects? Circ Res 118: 1143–1150 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heineke J, Auger‐Messier M, Xu J, Sargent M, York A, Welle S, Molkentin JD (2010) Genetic deletion of myostatin from the heart prevents skeletal muscle atrophy in heart failure. Circulation 121: 419–425 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hinken AC, Powers JM, Luo G, Holt JA, Billin AN, Russell AJ (2016) Lack of evidence for GDF11 as a rejuvenator of aged skeletal muscle satellite cells. Aging Cell 15: 582–584 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Katsimpardi L, Litterman NK, Schein PA, Miller CM, Loffredo FS, Wojtkiewicz GR, Chen JW, Lee RT, Wagers AJ, Rubin LL (2014) Vascular and neurogenic rejuvenation of the aging mouse brain by young systemic factors. Science 344: 630–634 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kemaladewi DU, de Gorter DJ, Aartsma‐Rus A, van Ommen GJ, ten Dijke P, t'Hoen PA, Hoogaars WM (2012) Cell‐type specific regulation of myostatin signaling. Faseb J 26: 1462–1472 [DOI] [PubMed] [Google Scholar]
- Lach‐Trifilieff E, Minetti GC, Sheppard K, Ibebunjo C, Feige JN, Hartmann S, Brachat S, Rivet H, Koelbing C, Morvan F et al (2014) An antibody blocking activin type II receptors induces strong skeletal muscle hypertrophy and protects from atrophy. Mol Cell Biol 34: 606–618 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Loffredo FS, Steinhauser ML, Jay SM, Gannon J, Pancoast JR, Yalamanchi P, Sinha M, Dall'Osso C, Khong D, Shadrach JL et al (2013) Growth differentiation factor 11 is a circulating factor that reverses age‐related cardiac hypertrophy. Cell 153: 828–839 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McPherron AC, Lawler AM, Lee SJ (1997) Regulation of skeletal muscle mass in mice by a new TGF‐beta superfamily member. Nature 387: 83–90 [DOI] [PubMed] [Google Scholar]
- McPherron AC, Lawler AM, Lee SJ (1999) Regulation of anterior/posterior patterning of the axial skeleton by growth/differentiation factor 11. Nat Genet 22: 260–264 [DOI] [PubMed] [Google Scholar]
- McPherron AC, Huynh TV, Lee SJ (2009) Redundancy of myostatin and growth/differentiation factor 11 function. BMC Dev Biol 9: 24 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mendias CL, Gumucio JP, Davis ME, Bromley CW, Davis CS, Brooks SV (2012) Transforming growth factor‐beta induces skeletal muscle atrophy and fibrosis through the induction of atrogin‐1 and scleraxis. Muscle Nerve 45: 55–59 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miyazono K, Kamiya Y, Miyazawa K (2008) SUMO amplifies TGF‐beta signalling. Nat Cell Biol 10: 635–637 [DOI] [PubMed] [Google Scholar]
- Morine KJ, Bish LT, Pendrak K, Sleeper MM, Barton ER, Sweeney HL (2010a) Systemic myostatin inhibition via liver‐targeted gene transfer in normal and dystrophic mice. PLoS ONE 5: e9176 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morine KJ, Bish LT, Selsby JT, Gazzara JA, Pendrak K, Sleeper MM, Barton ER, Lee SJ, Sweeney HL (2010b) Activin IIB receptor blockade attenuates dystrophic pathology in a mouse model of Duchenne muscular dystrophy. Muscle Nerve 42: 722–730 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mueller TD, Nickel J (2012) Promiscuity and specificity in BMP receptor activation. FEBS Lett 586: 1846–1859 [DOI] [PubMed] [Google Scholar]
- Narola J, Pandey SN, Glick A, Chen YW (2013) Conditional expression of TGF‐beta1 in skeletal muscles causes endomysial fibrosis and myofibers atrophy. PLoS ONE 8: e79356 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Poggioli T, Vujic A, Yang P, Macias‐Trevino C, Uygur A, Loffredo FS, Pancoast JR, Cho M, Goldstein J, Tandias RM et al (2016) Circulating growth differentiation factor 11/8 levels decline with age. Circ Res 118: 29–37 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rodgers BD, Eldridge JA (2015) Reduced circulating GDF11 is unlikely responsible for age‐dependent changes in mouse heart, muscle, and brain. Endocrinology 156: 3885–3888 [DOI] [PubMed] [Google Scholar]
- Rosenkranz S (2004) TGF‐beta1 and angiotensin networking in cardiac remodeling. Cardiovasc Res 63: 423–432 [DOI] [PubMed] [Google Scholar]
- Sacheck JM, Hyatt JP, Raffaello A, Jagoe RT, Roy RR, Edgerton VR, Lecker SH, Goldberg AL (2007) Rapid disuse and denervation atrophy involve transcriptional changes similar to those of muscle wasting during systemic diseases. FASEB J 21: 140–155 [DOI] [PubMed] [Google Scholar]
- Sartori R, Schirwis E, Blaauw B, Bortolanza S, Zhao J, Enzo E, Stantzou A, Mouisel E, Toniolo L, Ferry A et al (2013) BMP signaling controls muscle mass. Nat Genet 45: 1309–1318 [DOI] [PubMed] [Google Scholar]
- Schafer MJ, Atkinson EJ, Vanderboom PM, Kotajarvi B, White TA, Moore MM, Bruce CJ, Greason KL, Suri RM, Khosla S et al (2016) Quantification of GDF11 and myostatin in human aging and cardiovascular disease. Cell Metab 23: 1207–1215 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sinha M, Jang YC, Oh J, Khong D, Wu EY, Manohar R, Miller C, Regalado SG, Loffredo FS, Pancoast JR et al (2014) Restoring systemic GDF11 levels reverses age‐related dysfunction in mouse skeletal muscle. Science 344: 649–652 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith SC, Zhang X, Zhang X, Gross P, Starosta T, Mohsin S, Franti M, Gupta P, Hayes D, Myzithras M et al (2015) GDF11 does not rescue aging‐related pathological hypertrophy. Circ Res 117: 926–932 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sumner CJ, Wee CD, Warsing LC, Choe DW, Ng AS, Lutz C, Wagner KR (2009) Inhibition of myostatin does not ameliorate disease features of severe spinal muscular atrophy mice. Hum Mol Genet 18: 3145–3152 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trendelenburg AU, Meyer A, Rohner D, Boyle J, Hatakeyama S, Glass DJ (2009) Myostatin reduces Akt/TORC1/p70S6K signaling, inhibiting myoblast differentiation and myotube size. Am J Physiol Cell Physiol 296: C1258–C1270 [DOI] [PubMed] [Google Scholar]
- Walker RG, Poggioli T, Katsimpardi L, Buchanan SM, Oh J, Wattrus S, Heidecker B, Fong YW, Rubin LL, Ganz P et al (2016) Biochemistry and biology of GDF11 and myostatin: similarities, differences, and questions for future investigation. Circ Res 118: 1125–1142 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Waning DL, Mohammad KS, Reiken S, Xie W, Andersson DC, John S, Chiechi A, Wright LE, Umanskaya A, Niewolna M et al (2015) Excess TGF‐beta mediates muscle weakness associated with bone metastases in mice. Nat Med 21: 1262–1271 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Winbanks CE, Chen JL, Qian H, Liu Y, Bernardo BC, Beyer C, Watt KI, Thomson RE, Connor T, Turner BJ et al (2013) The bone morphogenetic protein axis is a positive regulator of skeletal muscle mass. J Cell Biol 203: 345–357 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wolfman NM, McPherron AC, Pappano WN, Davies MV, Song K, Tomkinson KN, Wright JF, Zhao L, Sebald SM, Greenspan DS et al (2003) Activation of latent myostatin by the BMP‐1/tolloid family of metalloproteinases. Proc Natl Acad Sci USA 100: 15842–15846 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yokoe T, Ohmachi T, Inoue H, Mimori K, Tanaka F, Kusunoki M, Mori M (2007) Clinical significance of growth differentiation factor 11 in colorectal cancer. Int J Oncol 31: 1097–1101 [PubMed] [Google Scholar]
- Zhou X, Wang JL, Lu J, Song Y, Kwak KS, Jiao Q, Rosenfeld R, Chen Q, Boone T, Simonet WS et al (2010) Reversal of cancer cachexia and muscle wasting by ActRIIB antagonism leads to prolonged survival. Cell 142: 531–543 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Expanded View Figures PDF
Review Process File