

Abstract
Background
The loss of skeletal muscle mass (MM) or muscle function (MF) alone increases the risk for losing physical independence in older adults. We aimed to examine the independent and synergic associations of low MM and low MF, both criteria of sarcopenia, with the risk for losing projected physical independence in later life (+90 years old).
Methods
Cross‐sectional analyses were conducted in 3493 non‐institutionalized older adults (1166 males). Physical independence was assessed with a 12‐item composite physical function scale. Logistic regression was used to estimate the odds‐ratio (OR) for being at risk for losing physical independence.
Results
Approximately 30% of the participants were at risk for losing physical independence at 90 years of age. Independent analysis demonstrated that participants with low MM had 1.65 (95%CI: 1.27–2.31) increased odds for being at risk for losing physical independence and participants with low MF had 6.19 (95%CI 5.08–7.53) increased odds for being at risk. Jointly, having a low MM and a low MF increased the risk for losing physical independence to 12.28 (95%CI 7.95 to 18.96).
Conclusions
Although low MM represents a risk factor for losing physical independence, low MF seems to play a more dominant role in this relationship, with the presence of both sarcopenia criteria representing a substantial risk for losing physical independence in later life.
Keywords: sarcopenia, dynapenia, elderly, physical independence
Introduction
The aging process is accompanied by inherent physiological changes, which can lead to functional limitations that may reach the point where the person cannot fully take‐care of them self with an inherent impact on family and medical costs. Early detection of older adults at risk for losing physical independence and better comprehension of the associated factors are key determinants for healthy aging.1, 2
The European Working Group on Sarcopenia in Older People as reached a consensus, defining sarcopenia as a syndrome characterized by progressive and generalized loss of skeletal muscle mass (MM) and strength with a risk of adverse outcomes such as physical disability, poor quality of life and death.3 The working group recommends using the presence of both low muscle mass and low muscle function (MF) (assessed by strength or performance) for the diagnosis of sarcopenia. The reduction of skeletal muscle mass along with the loss of muscle strength3, 4, 5 have been linked to diminished health outcomes, including loss physical independence, impairment in cognitive autonomy and an increased risk for comorbidities and death in older adults.6, 7, 8, 9 In older adults the decline in muscle strength is two to five times faster than the loss of skeletal muscle mass,10 suggesting a loss in muscle quality11 with an impact on physical independence.10, 12, 13
Clark and Manini14 have previously suggested a conceptual approach that dissociates the age associated losses in skeletal muscle mass and muscle function. The authors additionally emphasize that the loss in muscle function represents a greater risk for poor health outcomes and physical dependence than the loss of muscle mass. Accordingly, monitoring muscle strength has greater feasibility and offers fewer limitations than assessing skeletal muscle mass in everyday practice.
The age related loss in muscle function has been associated with a greater risk for slow gait speed and mobility impairment when compared with obesity alone.16, 17 Likewise, low muscle function combined with abdominal obesity increases the risk for metabolic change more than each condition alone.18 Although both low muscle mass and low muscle function predispose older adults to poor health outcomes, there are differences in the associations of their components with aging.10 For instances, it has been determined that combined obesity with low muscle function, but not with low muscle mass, is predictive of the risk of falls in older ages.19
Despite the evidence indicating that low muscle function has a predominant role in health outcomes when compared with low muscle mass, the presence of both criterion is required for the diagnose of sarcopenia. Recently, it has been highlighted a heterogeneous predictive value for activities of daily living (ADL) disability across the different muscle parameters that are currently used to diagnose sarcopenia.15 However, whether or not there are differences when considering the independent or the synergic role of muscle mass and function in the projected ability for physical independence in later life (+90 years old) is still unclear. Therefore, the aim of this study was to examine the independent and synergic associations of muscle mass and muscle function with increased risk for losing physical independence in later life.
Methods
Design and subjects
A total of 3493 participants were considered for data analysis (1166 males and 2327 females). Data for the present study were derived from a cross‐sectional representative sample of the community‐residing Portuguese population, aged 65 and older, which included five sampling areas covering the entire mainland of Portugal.20 The study was carried out in full compliance with the Helsinki Declaration and approved by the local ethics committee. All participants read and signed the informed consent form before the testing procedures.
Outcomes measures
Anthropometry
Participants were weighed to the nearest 0.1 kg, height was measured to the nearest 0.1 cm, according to standardized procedures21 (Seca, Hamburg, Germany), and body mass index (BMI) was calculated (kg/m2).
Skeletal muscle mass
Skeletal muscle mass was estimated using the Lee et al. 22 equation and adjusted by height square to create the skeletal muscle index (SMI). Following previous studies,23, 24, 25 low muscle mass was categorized based on the lower 20th percentile, which in the present sample corresponded to a SMI lower than 9.1 kg/m2 for males and lower than 6.5 kg/m2 for females.
Muscle function
Muscle function was estimated using the 30‐s chair stand test.26 Low muscle function was then classified based on the 20th percentile for each sex adjusted for age and SMI. This represented a cutoff of nine repetitions for males and eight for females.
Physical independence
Having the physical ability needed to live independently was assessed through self‐report using the 12‐item Composite Physical Function (CPF) scale.26 The age‐adjusted scoring option for defining moderate functioning that reflects projected ability for physical independence at age 90 years was used in this study. In participants aged 90 and older, the scoring refers to current ability for physical independence.27 Accordingly, physical independence was dichotomized as: low functioning (high risk) and moderate to high functioning (low risk).
Covariates
Self‐reported education, medical history and medication were assessed by interviewer‐administered questionnaires. Educational attainment was categorized as: (a) no formal education, (b) 4 years of education, (c) 9 years of education, (d) 12 years of education and (e) higher education. Medical history for hypertension, elevated cholesterol or glycemia, current medication, the presence of any long‐standing condition (diabetes, asthma, cancer or cardiac disease) and current smoking status were also reported and classified in two categories (yes or no). BMI was included as a continuous variable.
Statistical analysis
Analyses were performed with SPSS (v.22.0, 2013 SPSS Inc., Chicago, Illinois, U.S.A.). Descriptive statistics (mean ± SD) were calculated for all outcome measurements. Independent‐sample Kruskal‐Wallis test were used to compare means between categories and groups of joint association between low muscle mass and low muscle function categories. Logistic regression analyses, with dichotomized physical independence as the dependent variable, were used to estimate odds‐ratio (OR) and 95% confident intervals (CI) according to exposure categories: (1) muscle mass or muscle function and (2) joint associations: muscle mass and muscle function categories (normal muscle mass and normal muscle function; normal muscle mass and low muscle function; low muscle mass and normal muscle function; low muscle mass and low muscle function). All analyses were adjusted for age, sex, education, medical history for chronic disease, hypertension, elevated cholesterol or glycemia, and current medication status, and BMI as continuous variable. For all tests significance was set at P < 0.05.
Results
Approximately 30% (22.5% males and 34% females) of the participants were classified at high risk for losing physical independence at 90+ years. The participants' characteristics are summarized in Table 1.
Table 1.
Participants' demographic, anthropometric and muscular strength characteristics
| All (n = 3493) | Males (n = 1166) | Females (n = 2327) | |
|---|---|---|---|
| Age (y) | 75.05 ± 7.3 | 75.31 ± 7.4 | 74.92 ± 7.3 |
| Height (m) | 1.57 ± 0.1 | 1.65 ± 0.1 | 1.53 ± 0.1 |
| Weight (kg) | 69.38 ± 12.2 | 74.89 ± 11.8 | 66.62 ± 11.5 |
| Skeletal muscular mass (kg) | 20.75 ± 5.6 | 27.07 ± 3.4 | 17.57 ± 3.3 |
| Skeletal muscular index | 8.27 ± 1.6 | 9.91 ± 1.0 | 7.45 ± 1.2 |
| Body mass index (kg/m2) | 28.03 ± 4.3 | 27.42 ± 3.8 | 28.33 ± 4.6 |
| 30‐s chair stand test (no rep.) | 13.19 ± 5.8 | 13.48 ± 5.6 | 13.04 ± 5.8 |
| Composite physical function (score) | 18.62 ± 6.4 | 19.75 ± 6.1 | 18.05 ± 6.4 |
The results for the independent association of muscle mass and muscle function with the risk for losing physical independence in older adults are presented in Table 2. Participants with low muscle mass had a 1.65 (95% CI 1.27 to 2.31) increased odds‐ratios for being at risk for losing physical independence comparing to normal muscle mass participants. Independent analysis also demonstrated that low muscle function was associated with an approximate six‐fold increase in the odds for being at risk for losing physical independence (OR: 6.19, 95%CI 5.08 to 7.53).
Table 2.
Odds‐ratio for being at risk for losing physical independence
| N | n (%) at risk | Odds‐ratio (95% CI) | |
|---|---|---|---|
| Muscle mass | |||
| normal (reference) | 2795 | 789 (28.2) | 1.00 |
| low | 698 | 265 (38.0) | 1.65 (1.27–2.31) |
| Muscle function | |||
| normal (reference) | 2795 | 633 (22.6) | 1.00 |
| low | 698 | 421 (60.3) | 6.19 (5.08–7.53) |
Model adjusted for sex, age, education, medical history for chronic disease, hypertension, elevated cholesterol or glycemia, current medication status and body mass index.
The participants' characteristics according to the joint categories of muscle mass and muscle function are summarized in Table 3. Participants with a low muscle mass are older than normal muscle mass participants (P < 0.05). The body weight of older adults with low muscle mass was lower than participants with normal muscle mass (P < 0.05). The CPF scores were lower for participants with low muscle function, regardless of their muscle mass category, compared with the other categories (P < 0.05).
Table 3.
Participants' demographic, body composition and muscular strength characteristics according to joint muscle mass and muscle function categories
| Normal MM and MF (n = 2256, 757 males) | Normal MM low MF (n = 539, 176 males) | Low MM normal MF (n = 539, 191 males) | Low MM and MF (n = 159, 42 males) | |
|---|---|---|---|---|
| Age (y) | 73.71 ± 6.6c , d | 74.30 ± 7.2c , d | 80.06 ± 7.8a , b | 79.62 ± 7.3a , b |
| Height (m) | 1.58 ± 0.1c , d | 1.57 ± 0.1d | 1.57 ± 0.1d | 1.54 ± 0.1a , b , c |
| Weight (kg) | 73.81 ± 10.4d , c | 73.01 ± 11.1c | 56.07 ± 7.7a , b | 53.46 ± 7.7a , b |
| SMM (kg) | 21.76 ± 10.2c , d | 21.64 ± 5.3c , d | 17.09 ± 5.2a , b , d | 15.69 ± 4.9a , b , c |
| SMI | 8.64 ± 1.4c , d | 8.68 ± 1.5c , d | 6.83 ± 1.4a , b | 6.48 ± 1.3a , b |
| BMI (kg/m2) | 29.27 ± 3.7c , d | 29.61 ± 3.8c , d | 22.84 ± 2.1a , b | 22.57 ± 2.5a , b |
| 30‐s CST (no rep.) | 15.29 ± 4.6b , c , d | 6.48 ± 3.8a , c , d | 13.60 ± 4.7a , b | 4.69 ± 3.6a , b |
| CPF (score) | 19.28 ± 6.0b , c , d | 14.61 ± 7.6a , c , d | 18.35 ± 6.1a , b , d | 12.26 ± 7.0a , b , c |
| Number at risk* | 479 (21.2%) | 310 (57.5%) | 154 (28.6%) | 111 (69.8%) |
Abbreviations: MM, muscle mass; MF, muscle function; SMI, skeletal muscle index; BMI, body mass index; 30‐s CST, 30‐seconds chair stand test; CPF, composite physical function scale; number the participants at risk for physical dependence.
Difference vs normal MM and MF;
Difference vs normal MM low MF;
Difference vs low MM normal MF;
Difference vs low MM and MF (P < 0.05).
The synergic associations of muscle mass and muscle function with the risk for losing physical independence are illustrated in Figure 1.
Figure 1.
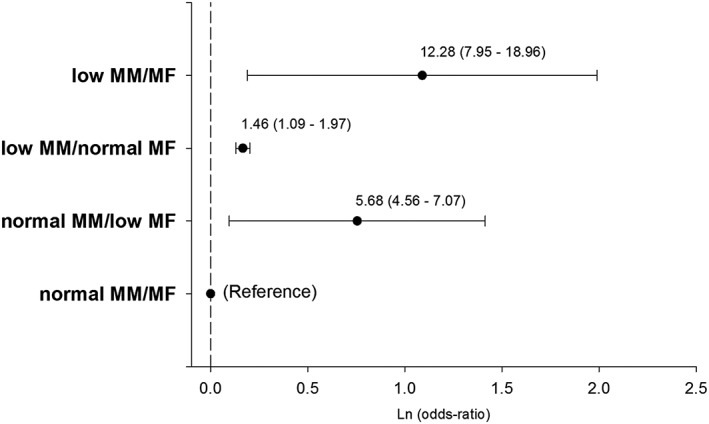
Joint association of muscle mass (MM)/muscle function (MF) categories [normal MM and MF; normal MM low MF; low MM normal MF; low MM and MF] with the risk for losing physical independence in older adults (n = 3493). *Results are presented as odds‐ratio (95% confident intervals) Model adjusted for sex, age, education, medical history for chronic disease, hypertension, elevated cholesterol or glycemia, current medication status and body mass index.
About 5% of the participants were within the low muscle mass and low muscle function category (69.8% at risk for losing physical independence), 15% in the low muscle mass and normal muscle function category (28.6% at risk for losing physical independence) and 15% in the normal muscle mass and low muscle function category (57.5% at risk for losing physical independence). Combined low muscle mass and low muscle function participants (OR: 12.28, 95%CI 7.95 to 18.96), normal muscle mass and low muscle function participants (OR: 5.68, 95%CI 4.56 to 7.07) and low muscle mass and normal muscle function participants (OR: 1.46, 95%CI 1.09 to 1.97) had increased odds for being at risk for losing physical independence comparing to the normal muscle mass and normal muscle function older adults.
Discussion
In the current investigation it was found that low muscle mass and low muscle function, both criteria to diagnose sarcopenia, independently predispose older adults for being at risk for losing projected physical independence at older ages (90+ years). Low muscle function seems to have the greatest impact on the risk for physical dependence compared with having low muscle mass alone. Additionally, there seems to be a synergic role between both parameters as older adults combining both low muscle mass and function presented the highest risk for losing physical independence.
Sarcopenia is a multifactorial syndrome; the aging process is responsible for a reduction in skeletal muscle mass of approximately 4.7% in males and 3.7% in females from the seventh decade of life. These age‐related changes seem to be more pronounced in the muscles of the lower limbs,10 and disuse, disease or anorexia accelerate these processes.28 Previous studies have highlighted low muscle mass as an independent risk factor for impairment in mobility29 and physical weakness.30 Corroborating these findings in the present study, it was verified that participants within the lowest muscle mass group were more likely to be at risk for physical dependence than their counterparts.
Recent data from longitudinal studies indicate that maintaining or gaining muscle mass does not prevent aging‐related declines in muscle function.31 Loss of muscle function after 75 years of age is two to five times faster than loss of skeletal muscle mass10 and has a greater impact in the loss of physical independence in older adults.10, 25, 31 In the present study, participants with lower muscle mass had lower scores in the CPF scale comparing to older adults with low muscle mass. Additionally, having the lowest muscle function was associated with increased odds for being at risk for losing physical independence.
Low muscle quality and low muscle strength of the lower limbs have been related to the loss of physical independence and mobility.12, 32, 33 These conditions have been associated with the aging process and aggregate factors, including reduced physical activity and associated diseases.10 Diagnosing low muscle strength has been made with the use of handgrip and isokinetic dynamometer force,11, 23, 25, 34 and despite the precision of these methods, their applicability in population studies is limited. The 30‐s CST provides a valid indicator of functional muscle strength of the lower limbs in older adults,35 with good reproducibility and low cost, and including the functional component of muscle strength.36 In this study, we used the 20th percentile to determine the cutoff points for low muscle function, verifying that performing fewer than nine repetitions in males and eight in females increased the risk of losing physical independence. The 30‐s CST is suggested as a useful tool to diagnose low muscle function in population studies, interventions and clinical practice.
The independent associations of low skeletal muscle mass, low muscle function and mortality risk were previously examined by Newman et al.,25 demonstrating that low skeletal muscle mass does not explain the association between muscular strength and mortality. Huang et al. 37 found that low muscle strength was associated with cognitive impairment in multiple dimensions and global cognitive function, but low muscle mass was associated only with impaired verbal fluency. Scott et al. 19 examined the relationship between obesity, low muscle mass and low muscle strength with the risk of falling, concluding that obesity combined with low muscle strength but not with low muscle mass predisposes older adults to the risk of falling. Alexander et al. 23 demonstrated that low muscle mass but not low muscle strength was associated with an increased risk for impaired physical independence. Cesari et al. 15 have recently verified that the different parameters that are present in the sarcopenia definition are heterogeneous in predicting the incidence of ADL disability. In the current investigation, we observed that, although participants with low muscle mass but normal muscle function were at risk for losing physical independence (OR = 1.5), the higher odds were observed in low muscle function older adults, regardless of their muscle mass status (normal muscle mass but low muscle function: OR = 5.7; SD: OR = 12.3).
From a practical point of view, the results presented in this investigation show that despite the inherent risk of losing of skeletal muscle mass with the aging process, the greater damage seems to be the loss of muscle function and muscle quality. Knowing that the loss of muscle function occurs faster and with a greater magnitude than the loss of skeletal muscle mass, it is of extreme importance to increase physical activity in older ages and promote the practice of exercise among older adults, with an emphasis in resistance training. Indeed, resistance training seems to be the most effective in maintaining and increasing muscle strength and quality in this population.38, 39 Even relatively short periods of intervention are able to promote significant changes in muscle strength and muscle quality.40
Strengths and limitations
The present study was performed with a large nationally representative database of older adults. Regardless, the investigation presents some limitations. In this study, skeletal muscle mass was estimated with the use of an equation. Imaging techniques (computed tomography, magnetic resonance and dual energy X‐ray absorptiometry) provide more accurate measures of skeletal muscle mass but are limited in population studies. The Lee et al. 22 equation provides a valid alternative in determining the skeletal muscle mass in older adults and can be used on a large scale with fewer associated costs, which facilitates its use in the clinical setting.
The current study was a cross‐sectional design; longitudinal studies should examine the association between low muscle mass and low muscle function with physical dependence to more definitively identify cause and effect.
Conclusions
Despite the fact that sarcopenia has been widely accepted has the age‐related loss of muscle mass and muscle function, in the current investigation it was demonstrated that, independently, older adults with low skeletal muscle mass or low muscle function, both criteria to diagnose sarcopenia, are more likely to be at risk for losing physical independence in later life (90+ years). Although a low muscle mass represents a single risk factor for physical independence, muscle function seems to have a leading role in this relationship, and together, both conditions play a synergetic role in increasing the risk for losing physical independence. Promoting physically active aging with a focus on resistance training programs, that not only aim to increase muscle mass but also muscle strength and function, are determinant to postpone physical dependence in later life.
Conflict of interest
Leandro dos Santos, Edilson S. Cyrino, Melissa Antunes, Diana A. Santos and Luís B. Sardinha, assert that they have no conflict of interest.
Acknowledgements
The authors wish to express their gratitude to all the participants for their cooperation in this study. L.S. and M.A., conducted this work during a visiting scholar period to the Faculty of Human Kinetics, University of Lisbon, Portugal, supported by the Capes Foundation within the Ministry of Education, Brazil (Process: 88887.065407/2014‐00 and process: 88887.090477/2014‐00, respectively). DAS is supported by the Portuguese Foundation for Science and Technology (Grant: SFRH/BPD/92462/2013).
The authors certify that they comply with the ethical guidelines for publishing in the Journal of Cachexia, Sarcopenia and Muscle: update 2015.41
Leandro dos Santos, Edilson S. Cyrino, Melissa Antunes, Diana A. Santos and Luís B. Sardinha, contributed equally to this work.
dos Santos, L. , Cyrino, E. S. , Antunes, M. , Santos, D. A. , and Sardinha, L. B. (2017) Sarcopenia and physical independence in older adults: the independent and synergic role of muscle mass and muscle function. Journal of Cachexia, Sarcopenia and Muscle, 8: 245–250. doi: 10.1002/jcsm.12160.
References
- 1. Wang L, van Belle G, Kukull WB, Larson EB. Predictors of functional change: a longitudinal study of nondemented people aged 65 and older. J Am Geriatr Soc 2002;50:1525–1534. [DOI] [PubMed] [Google Scholar]
- 2. Fried LP, Ferrucci L, Darer J, Williamson JD, Anderson G. Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care. J Gerontol A Biol Sci Med Sci 2004;59:255–263. [DOI] [PubMed] [Google Scholar]
- 3. Cruz‐Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European working group on sarcopenia in older people. Age Ageing 2010;39:412–423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Dam TT, Peters KW, Fragala M, Cawthon PM, Harris TB, McLean R, et al. An evidence‐based comparison of operational criteria for the presence of sarcopenia. J Gerontol A Biol Sci Med Sci 2014;69:584–590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Studenski SA, Peters KW, Alley DE, Cawthon PM, McLean RR, Harris TB, et al. The FNIH sarcopenia project: rationale, study description, conference recommendations, and final estimates. J Gerontol A Biol Sci Med Sci 2014;69:547–558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Tolea MI, Galvin JE. Sarcopenia and impairment in cognitive and physical performance. Clin Interv Aging 2015;10:663–671. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Fielding RA, Vellas B, Evans WJ, Bhasin S, Morley JE, Newman AB, et al. Sarcopenia: an undiagnosed condition in older adults. Current consensus definition: prevalence, etiology, and consequences. International working group on sarcopenia. J Am Med Dir Assoc 2011;12:249–256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Li C‐I, Li T‐C, Lin W‐Y, Liu C‐S, Hsu C‐C, Hsiung CA, et al. Combined association of chronic disease and low skeletal muscle mass with physical performance in older adults in the Sarcopenia and Translational Aging Research in Taiwan (START) study. BMC Geriatr 2015;15:11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Morley JE, Anker SD, von Haehling S. Prevalence, incidence, and clinical impact of sarcopenia: facts, numbers, and epidemiology‐update 2014. J Cachexia Sarcopenia Muscle 2014;5:253–259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Mitchell WK, Williams J, Atherton P, Larvin M, Lund J, Narici M. Sarcopenia, dynapenia, and the impact of advancing age on human skeletal muscle size and strength; a quantitative review. Front Physiol 2012;3:260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Goodpaster BH, Park SW, Harris TB, Kritchevsky SB, Nevitt M, Schwartz AV, et al. The loss of skeletal muscle strength, mass, and quality in older adults: the health, aging and body composition study. J Gerontol A Biol Sci Med Sci 2006;61:1059–1064. [DOI] [PubMed] [Google Scholar]
- 12. Venturelli M, Saggin P, Muti E, Naro F, Cancellara L, Toniolo L, et al. In vivo and in vitro evidence that intrinsic upper‐ and lower‐limb skeletal muscle function is unaffected by ageing and disuse in oldest‐old humans. Acta Physiol (Oxf) 2015;doi:10.1111/apha.12524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Grounds MD, Pinniger GJ. What is the mechanism for in vivo loss of skeletal muscle function in elderly females? Acta Physiol (Oxf) 2015;doi:10.1111/apha.12547. [DOI] [PubMed] [Google Scholar]
- 14. Clark BC, Manini TM. Sarcopenia =/= dynapenia. J Gerontol A Biol Sci Med Sci 2008;63:829–834. [DOI] [PubMed] [Google Scholar]
- 15. Cesari M, Rolland Y. Abellan Van Kan G, Bandinelli S, Vellas B, Ferrucci L. Sarcopenia‐related parameters and incident disability in older persons: results from the “invecchiare in Chianti” study. J Gerontol A Biol Sci Med Sci 2015;70:457–463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Yang M, Jiang J, Hao Q, Luo L, Dong B. Dynapenic obesity and lower extremity function in elderly adults. J Am Med Dir Assoc 2015;16:31–36. [DOI] [PubMed] [Google Scholar]
- 17. Bouchard DR, Janssen I. Dynapenic‐obesity and physical function in older adults. J Gerontol A Biol Sci Med Sci 2010;65:71–77. [DOI] [PubMed] [Google Scholar]
- 18. Senechal M, Dionne IJ, Brochu M. Dynapenic abdominal obesity and metabolic risk factors in adults 50 years of age and older. J Aging Health 2012;24:812–826. [DOI] [PubMed] [Google Scholar]
- 19. Scott D, Sanders KM, Aitken D, Hayes A, Ebeling PR, Jones G. Sarcopenic obesity and dynapenic obesity: 5‐year associations with falls risk in middle‐aged and older adults. Obesity (Silver Spring) 2014;22:1568–1574. [DOI] [PubMed] [Google Scholar]
- 20. Sardinha LB, Santos DA, Marques EA, Mota J. Criterion‐referenced fitness standards for predicting physical independence into later life. Exp Gerontol 2015;61:142–146. [DOI] [PubMed] [Google Scholar]
- 21. Lohman TG, Roche AF, Martorell R. Anthropometric standardization reference manual. Champaign, IL: Human Kinetics Books; 1988. [Google Scholar]
- 22. Lee RC, Wang Z, Heo M, Ross R, Janssen I, Heymsfield SB. Total‐body skeletal muscle mass: development and cross‐validation of anthropometric prediction models. Am J Clin Nutr 2000;72:796–803. [DOI] [PubMed] [Google Scholar]
- 23. Alexandre TS, Duarte YA, Santos JL, Wong R, Lebrao ML. Sarcopenia according to the European Working Group on Sarcopenia in Older People (EWGSOP) versus dynapenia as a risk factor for mortality in the elderly. J Nutr Health Aging 2014;18:751–756. [DOI] [PubMed] [Google Scholar]
- 24. Delmonico MJ, Harris TB, Lee JS, Visser M, Nevitt M, Kritchevsky SB, et al. Alternative definitions of sarcopenia, lower extremity performance, and functional impairment with aging in older men and women. J Am Geriatr Soc 2007;55:769–774. [DOI] [PubMed] [Google Scholar]
- 25. Newman AB, Kupelian V, Visser M, Simonsick EM, Goodpaster BH, Kritchevsky SB, et al. Strength, but not muscle mass, is associated with mortality in the health, aging and body composition study cohort. J Gerontol A Biol Sci Med Sci 2006;61:72–77. [DOI] [PubMed] [Google Scholar]
- 26. Rikli RE, Jones CJ. Development and validation of criterion‐referenced clinically relevant fitness standards for maintaining physical independence in later years. Gerontologist 2013;53:255–267. [DOI] [PubMed] [Google Scholar]
- 27. Rikli RE, Jones CJ. The reliability and validity of a 6‐minute walk test as a measure of physical endurance in older adults. J Aging Phys Act 1998;6:363–375. [Google Scholar]
- 28. Narici MV, Maffulli N. Sarcopenia: characteristics, mechanisms and functional significance. Br Med Bull 2010;95:139–159. [DOI] [PubMed] [Google Scholar]
- 29. Dufour AB, Hannan MT, Murabito JM, Kiel DP, McLean RR. Sarcopenia definitions considering body size and fat mass are associated with mobility limitations: the Framingham Study. J Gerontol A Biol Sci Med Sci 2013;68:168–174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Baumgartner RN, Koehler KM, Gallagher D, Romero L, Heymsfield SB, Ross RR, et al. Epidemiology of sarcopenia among the elderly in New Mexico. Am J Epidemiol 1998;147:755–763. [DOI] [PubMed] [Google Scholar]
- 31. Manini TM, Clark BC. Dynapenia and aging: an update. J Gerontol A Biol Sci Med Sci 2012;67:28–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Visser M, Deeg DJ, Lips P, Harris TB, Bouter LM. Skeletal muscle mass and muscle strength in relation to lower‐extremity performance in older men and women. J Am Geriatr Soc 2000;48:381–386. [DOI] [PubMed] [Google Scholar]
- 33. Reid KF, Naumova EN, Carabello RJ, Phillips EM, Fielding RA. Lower extremity muscle mass predicts functional performance in mobility‐limited elders. J Nutr Health Aging 2008;12:493–498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Lee WJ, Liu LK, Peng LN, Lin MH, Chen LK. Comparisons of sarcopenia defined by IWGS and EWGSOP criteria among older people: results from the I‐Lan longitudinal aging study. J Am Med Dir Assoc 2013;14:528.e1–528.e7. [DOI] [PubMed] [Google Scholar]
- 35. Jones CJ, Rikli RE, Beam WC. A 30‐s chair‐stand test as a measure of lower body strength in community‐residing older adults. Res Q Exerc Sport 1999;70:113–119. [DOI] [PubMed] [Google Scholar]
- 36. Skoffer B, Dalgas U, Mechlenburg I, Soballe K, Maribo T. Functional performance is associated with both knee extensor and flexor muscle strength in patients scheduled for total knee arthroplasty: a cross‐sectional study. J Rehabil Med 2015;47:454–459. [DOI] [PubMed] [Google Scholar]
- 37. Huang CY, Hwang AC, Liu LK, Lee WJ, Chen LY, Peng LN, et al. Association of dynapenia, sarcopenia and cognitive impairment among community‐dwelling older Taiwanese. Rejuvenation Res 2015;doi:10.1089/rej.2015.1710. [DOI] [PubMed] [Google Scholar]
- 38. Iolascon G, Di Pietro G, Gimigliano F, Mauro GL, Moretti A, Giamattei MT, et al. Physical exercise and sarcopenia in older people: position paper of the Italian Society of Orthopaedics and Medicine (OrtoMed). Clin Cases Miner Bone Metab 2014;11:215–221. [PMC free article] [PubMed] [Google Scholar]
- 39. Lenk K, Schuler G, Adams V. Skeletal muscle wasting in cachexia and sarcopenia: molecular pathophysiology and impact of exercise training. J Cachexia Sarcopenia Muscle 2010;1:9–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Fragala MS, Fukuda DH, Stout JR, Townsend JR, Emerson NS, Boone CH, et al. Muscle quality index improves with resistance exercise training in older adults. Exp Gerontol 2014;53:1–6. [DOI] [PubMed] [Google Scholar]
- 41. von Haehling S, Morley JE, Coats AJS, Anker SD. Ethical guidelines for publishing in the Journal of Cachexia, Sarcopenia and Muscle: update 2015. J Cachexia Sarcopenia Muscle 2015;6:315–316. [DOI] [PMC free article] [PubMed] [Google Scholar]