

Abstract
Angiofibrolipoma is a histological variant of lipoma, which commonly occurs in subcutaneous tissues. In the present report we illustrate the case of an angiofibrolipoma of the posterior upper mediastinum in a 75-year-old man presented with progressive chest pain. Xray chest showed a homogeneous opacity vertically oriented along the right lateral aspect of thoracic vertebrae with an obtuse angle to the mediastinum. The upper extremity of the mass extended above the superior clavicle, suggestive of a posterior mediastinal lesion. Thoracic magnetic resonance imaging revealed a posterior mediastinal mass, in keeping with a nonaggressive lesion, with particular endocanalar extension and heterogeneous signal and enhancement patterns that was highly suggestive of a mixed mesenchymal tumor. The tumor was incompletely removed by right postero-lateral thoracotomy with final diagnosis of angiofibrolipoma. To the author’s knowledge, such a case of angiofibrolipoma located in the posterior mediastinum has not been previously reported in the literature.
Key words: Angiofibrolipoma, Posterior mediastinum, MRI, Mesenchymal tumors
Competing interest statement
Conflict of interest: the authors declare no potential conflict of interest.
Introduction
Angiofibrolipoma, a form of mixed mesenchymal tumor, is a benign neoplasm composed of fibrocytes, capillaries and matured adipose tissues. It usually presents as a subcutaneous lesion, most commonly located in the back, the neck or the shoulders, but rarely found in the mediastinum. We report a case of an angiofibrolipoma of posterior upper mediastinum with an incomplete tumor removal.
Case Report
We report the case of a 75-year-old man with a history of 80 pack/year cigarette smoking, complaining of a progressive chest pain propagating to the back for the last 6 months.
Physical examination revealed a sharp pain along the costovertebral angles while chest auscultation and neurologic examination were entirely normal. Complete blood count, liver and renal function tests and C reactive protein level were normal.
Frontal postero-anterior radiography of the chest showed a homogeneous opacity, without air brochogram, located above the carina, vertically oriented along the right lateral aspect of thoracic vertebrae (TV). Its outer border presented an obtuse angle to the mediastinum and its upper extremity extended above the superior clavicle. It was suggestive of an upper posterior mediastinal opacity (Figure 1).
Figure 1.
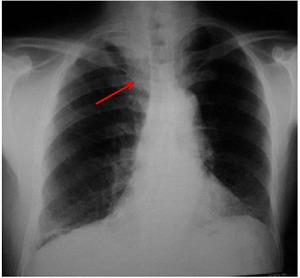
Posteroanterior X-ray chest (frontal incidence): i) homogeneous opacity without air bronchogram, vertically oriented along the right lateral aspect of thoracic vertebrae with an obtuse angle to the mediastinum suggestive of a mediastinal opacity; ii) the upper extremity of the mass extends above the superior clavicle, therefore, it is probably located within the posterior mediastinum (cervicothoracic sign); iii) no mediastal shift; iv) no spinal or costal abnormalities seen.
A thoracic enhanced computed tomography (CT) disclosed to a posterior mediastinal tumor with heterogeneous enhancement and endocanalar extension.
Subsequently, a thoracic magnetic resonance imaging (MRI) imaging was performed (1.5 Tesla, Philips, Amsterdam, the Netherlands) revealing a 30×20×35 mm sized posterior mediastinal tumor, oblong in shape, well defined, located in the right costovertebral gutter extending from T1 to T3 level (Figure 2). This mass presented a heterogeneous lowsignal intensity on T1- weighted images and a high-signal intensity on T2-weighted images. There were interspersed areas within the mass of high signal intensity on both T1 and T2-weighted images that vanished after fat suppression techniques confirming the presence of a fatty component (Figure 2).
Figure 2.
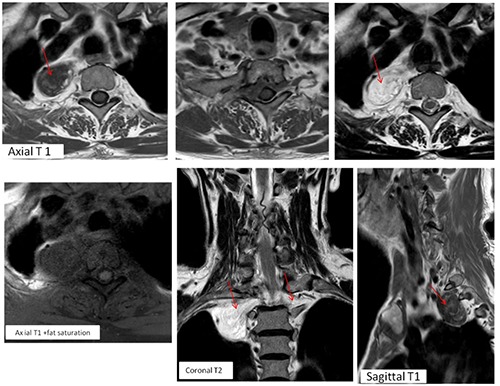
Non-enhanced magnetic resonance imaging T1 and T2-weighted images before and after fat saturation: i) a mass located in the right costovertebral gutter, well-marginated, with heterogeneous low-signal intensity on T1- weighted images and a high-signal intensity on T2-weighted images. ii) Presence of hyperintense areas within the mass on both T1 and T2 WI that became hypointense after fat suppression corresponding to a fatty component. iii) The tumor extends through the spinal canal, filling the anterior epidural space, from right to left T1-T2 intervertebral foramina. iv) The spinal cord is slightly compressed without signal abnormalities. v) Scalloping of the posterior margin of the body and posterior arches of T1 and T2 VT. vi) The tumor is responsible of widening of both foramina and scalloping of posterior vertebral body and arches of T1 and T2 without cortical destruction.
The fat-suppressed post contrast images showed an early, intense and heterogeneous enhancement suggesting a highly vascular tumor (Figure 3).
Figure 3.

Axial and sagittal fat-suppressed post contrast magnetic resonance imaging images: i) the mass shows an intense and heterogeneous enhancement; ii) tumoral extension through the spinal canal, filling the anterior epidural space, from right to left T1-2 intervertebral foramina that are enlarged; iii) there is no enhancement abnormalities of spinal cord next to the tumor.
This mass presented a particular extension through the spinal canal from right to left T1-T2 intervertebral foramina causing widening of both foramina and a scalloping of posterior vertebral body and arches of T1 and T2 without cortical destruction. It was filling the anterior epidural space, the spinal cord was slightly compressed but not invaded without any signal or enhancement abnormalities (Figures 2 and 3).
MRI findings were in keeping with a nonaggressive tumor and highly suggestive of a mixed mesenchymal tumor including fatty tissue: an angiomyolipoma was suspected.
A right postero-lateral thoracotomy through 4th intercostal space was performed for surgical excision and histopathological confirmative diagnosis. The extra foraminal portion of the lesion was completely resected with ligature and section of the sympathetic nerve. The endocanalar portion could not be removed, meanwhile, because of excess bleeding during spinal surgery approach. A preoperative embolization was discussed to enable easier resection at a later date.
Macroscopic examination revealed an oblong flaccid tumor of 2×3 cm with well circumscribed boundary and whitish color. Histology showed a mixed mesenchymal tumor intricately composed of dense fibrocollagenous tissue, mature adipocytes and thick-walled vascular vessels without the evidence of mitosis or cellular pleomorphism in all sections examined. In immunohistochemical staining, the tumor was positive for CD34 (for vascular component), S-100 protein (for adipocytes) and vimentine (for fibrocytes), smooth muscle actin and Desmine were negative (Figure 4).
Figure 4.

Pathological image of the tumor (Hematoxylin and Eosin, 10×): i) association of the three characteristic findings of angiofibrolipomas: mature adipocytes, vascular vessels and collagenous tissue; ii) no evidence of mitosis or cellular pleomorphism.
Histopathological findings were consistent with an angiofibrolipoma of posterior mediastinum.
Discussion
Posterior mediastinal masses include a wide histopathological and radiological spectrum where neurogenic tumors are most frequently encountered in more than 75% of cases.1,2 Mesenchymal tumors are uncommon accounting for only 6 to 8% of all mediastinal masses and are slightly more frequent in children.3 They represent a heterogeneous group of benign or malignant neoplasms originating from connective tissue elements: smooth and striated muscle, lymphatic tissue, fat, and vascular tissue.
Angiofibrolipoma is a benign mixed form of mesenchymal tumor and a rare histopathologic variant of lipoma. The other histological variants of lipomas include fibrolipomas, angiolipomas, angiomyolipomas, and infiltrating angiolipomas.4 This classification is based on the relationship between the fat, muscle, blood vessel, and connective tissues involved in the tumor structure.
Angiofibrolipoma is composed by fibrocytes, capillaries and matured adipose tissues. It usually occurs in the superficial soft tissues of the back, the neck or shoulders but it’s extremely rare in mediastinum with no previous case reported in the literature.
Due to its high contrast resolution, MRI is the most performant tool in tissue characterization, evaluation of extension into the spinal canal and invasion into surrounding tissues, which is important for planning the adequate therapy.
MRI of angiofibrolipoma in the soft tissues have been described in few case reports,5 but has not been previously reported in mediastinum.
In our case, the tumor was predominately hypointense on T1-weighted images and hyperintense on T2-weighted images with an intense and heterogeneous enhancement. The identification of a fatty component within the tumor was useful for the diagnosis.
According to the literature, fat containing tumors in posterior mediastinum that enlarge the neural foramina and enters the spinal canal narrows the differential diagnosis to ganglioneuroma, Schwannoma, or lipomatous mesenchymal tumor.1
In this case, the tumor demonstrated an unusual endocanalar extension with a long extradural segment spreading from right to left neural foramina. This finding argued against a neurogenic tumor. Indeed, these latter, may grow through the adjacent intervertebral foramen causing its widening and producing in some cases a dumbbell configuration but extension to the opposite foramen has not been reported.
Thus, the identification of a fatty component in a highly vascular tumor with such a particular transforaminal intraspinal involvement points to the diagnosis of a lipomatous mesenchymal tumor.
Conclusions
Although rare, mesenchymal tumors should be considered in the differential diagnosis of a posterior mediastinal mass. MRI is a performant tool for diagnosis and evaluation of transforaminal and intraspinal tumor propagation.
Acknowledgments
We are immensely grateful to our esteemed colleagues from surgical department and histopathology laboratory (Abderrahmen Mami hospital) who provided operative and histopathological findings for this article.
References
- 1.Duffy S, Jhaveri M, Scudierre J, et al. MR imaging of a posterior mediastinal ganglioneuroma: fat as a useful diagnostic sign. Am J Neuroradiol 2005;26:2658-62. [PMC free article] [PubMed] [Google Scholar]
- 2.Nakazono T, White CS, Yamasaki F, et al. MRI findings of mediastinal neurogenic tumors. Am J Roentgenol 2011;197:W643-52. [DOI] [PubMed] [Google Scholar]
- 3.Del Campo C, Mpougas PP. Compression of the superior vena cava by a mediastinal lipoma. Tex Heart Inst J 2000;27:297-8. [PMC free article] [PubMed] [Google Scholar]
- 4.Jacob A, Kneile J, Welling DB. Angiofibrolipoma of the ear canal. Laryngoscope 2005;115:1461-2. [DOI] [PubMed] [Google Scholar]
- 5.Uwale Eyesan S, Christopher Ayeni S, Adesope Adesina S, et al. Angiofibrolipoma of the calf. Rare Tumors 2013;5:e48. [DOI] [PMC free article] [PubMed] [Google Scholar]