

Abstract
Background
Neighborhood socioeconomic status (nSES) has been found to be associated with breast cancer risk. It remains unclear whether this association applies across racial/ethnic groups independent of individual-level factors, and is attributable to other neighborhood characteristics.
Methods
We examined the independent and joint associations of education and nSES with odds of breast cancer. Residential addresses were geocoded for 2,838 cases and 3,117 controls and linked to nSES and social and built environment characteristics. We estimated odds ratios (OR) and 95% confidence intervals (CI) using multilevel logistic regression controlling for individual-level breast cancer risk factors, and assessed the extent to which nSES associations were due to neighborhood characteristics.
Results
Women living in the highest versus lowest nSES quintile had a nearly two-fold greater odds of breast cancer, with elevated odds (adjusted ORs, 95% CI) for non-Hispanic whites (NHWs) (2.27, 1.45–3.56), African Americans (1.74, 1.07–2.83), U.S.-born Hispanics (1.82, 1.19–2.79), and foreign-born Hispanics (1.83, 1.06–3.17). Considering education and nSES jointly, ORs were increased for: low education/high nSES NHWs (1.83, 1.14–2.95), high education/high nSES NHWs (1.64, 1.06–2.54), and high education/high nSES foreign-born Hispanics (2.17, 1.52–3.09) relative to their race/ethnicity/nativity-specific low education/low nSES counterparts. Adjustment for urban and mixed-land use characteristics attenuated the nSES associations for most racial/ethnic/nativity groups except NHWs.
Conclusions
Our study provides empirical evidence for a role of neighborhood environments in breast cancer risk, specifically social and built environment attributes.
Impact
Considering the role of neighborhood characteristics among diverse populations may offer insights to understand racial/ethnic disparities in breast cancer risk.
Keywords: breast neoplasms, environment, residence characteristics, socioeconomic status
INTRODUCTION
Breast cancer is the most common cancer among women in all major racial/ethnic groups in the United States (U.S.) (1). Racial/ethnic disparities in breast cancer risk are well documented with substantially lower incidence rates among racial/ethnic minority groups compared to non-Hispanic white (NHW) women (1, 2). The underlying reasons for these racial/ethnic disparities in breast cancer risk remain unclear. Previous studies have focused on racial/ethnic differences in the distribution of individual-level reproductive and behavioral risk factors (3–5), yet the explanation for racial/ethnic risk differences is likely multidimensional, operating through both individual- and neighborhood-level factors (6).
A socioeconomic status (SES) gradient in breast cancer incidence is well-established, with evidence of positive associations with both individual-level SES measures (e.g., education, income, and/or occupation (7–11)), and contextual-level measures of neighborhood SES (nSES), (e.g., area-based characteristics of education, income, poverty, occupation, or multidimensional composite measures (reviewed in: (12))). However, only a few studies have been able to examine both individual- and contextual-level SES simultaneously, and their results are inconsistent (13–18). Population-based case-control studies (17, 18) support nSES as a risk factor for breast cancer, independent of individual-level education, reproductive and behavioral factors, while prospective cohort studies observed no nSES-breast cancer associations (13, 14, 16). These prior studies included NHW (13–17) or African American women (14), and only one study examined joint influences of individual-level SES and nSES on breast cancer risk (18).
The Neighborhoods and Breast Cancer Study (NABC) combined extensive questionnaire data on breast cancer risk factors from two large, multiethnic population-based studies of breast cancer conducted in the San Francisco Bay Area and small area-level social and built environment data from the California Neighborhoods Data System (CNDS) (19). To address the gaps in knowledge on the role of nSES in racial/ethnic disparities in breast cancer incidence, we examined the independent and joint associations of nSES and an individual-level indicator of SES – education - with breast cancer risk in NHW, African American, and U.S.- and foreign-born Hispanic women, while accounting for individual-level breast cancer risk factors. We further examined the extent to which social and built environment characteristics explained the nSES-breast cancer associations.
MATERIALS AND METHODS
Study population
The NABC study pooled data from the San Francisco Bay Area Breast Cancer Study (SFBCS), a case-control study of breast cancer conducted between 1995–2004 (20), and the Northern California Breast Cancer Family Registry (NC-BCFR), one of six international sites collaborating in the Breast Cancer Family Registry established in 1995 (21, 22). Cases diagnosed from 1995–2009 were enrolled in the NC-BCFR in several phases. This case-control analysis includes only cases diagnosed from 1995–1998. Both studies identified women with a first primary invasive breast cancer via regional population-based cancer registries that ascertain all incident cancers as part of the Surveillance, Epidemiology, and End Results (SEER) program and the California Cancer Registry (CCR). Details on the study design and methodology of the NABC study have been provided (23, 24). Briefly, harmonized questionnaire data on breast cancer risk factors from the SFBCS and the NC-BCFR were merged with neighborhood data from the CNDS (19) based on residential address at time of diagnosis for cases and interview for controls. Study participants provided written informed consent and all protocols were approved by the Institutional Review Board of the Cancer Prevention Institute of California.
The SFBCS identified cases aged 35–79 years, living in Alameda, Contra Costa, San Mateo, San Francisco, or Santa Clara counties at diagnosis. To enrich the sample for minorities, eligible cases included all Hispanics diagnosed from 1995–2002 all African Americans diagnosed from 1995–1999, and a 10% random sample of NHWs diagnosed from 1995–1999. Population-based controls from the same geographic area as the cases were identified through random-digit dialing and frequency-matched on self-reported race/ethnicity and 5-year age group to the expected distribution of cases. Self-reported race/ethnicity and study eligibility were assessed by a telephone screening interview with participation rates of 89% for cases contacted (alive, locatable, no physician refusal) and 92% for controls contacted. An in-person interview was completed by 2,258 (88%) eligible cases and 2,706 (85%) eligible controls.
The NC-BCFR identified cases aged 18–64 years diagnosed from 1995–2009 in several phases. They included cases living in Alameda, Contra Costa, Marin, San Mateo, San Francisco, Santa Clara, Santa Cruz, and Monterrey counties at diagnosis identified through the Greater Bay Area Cancer Registry (any race/ethnicity diagnosed from 1/1995 to 9/1998; Hispanics, African Americans, Chinese, Filipinas and Japanese diagnosed from 10/1998 to 4/2002; and Hispanics and African Americans diagnosed from 5/2002 to 8/2009). Additionally, the NC-BCFR included Hispanic and African American cases diagnosed from 1/2005 to 12/2006 and living in Sacramento and Solano counties at diagnosis; they were identified by the Sacramento and Sierra Cancer Registry. All cases with indicators of increased genetic susceptibility were eligible to enroll in the NC-BCFR (21). Cases not meeting these criteria were randomly sampled. Given the large number of diagnoses in NHW women, they were randomly sampled at 2.5%; racial/ethnic minorities were oversampled at 15% in Phase 1. Population-based controls from the same geographic area as the cases diagnosed from 1995–1998 were identified through Random Digit Dialing and frequency-matched on self-reported race/ethnicity and 5-year age group at a case:control ratio of 2:1. A telephone screening interview assessed study eligibility and self-identified race/ethnicity (participation: 85% of contacted cases and 82% of contacted controls). An in-person interview was completed by 3,631 (78%) cases selected for NC-BCFR and 626 (91%) eligible controls.
A total of 3,384 cases and 3,332 controls with complete interview and address data were eligible for this analysis after excluding NC-BCFR cases diagnosed from 1999–2009 without matched controls. We used the SFBCS interview data for 339 cases that participated in both studies. We excluded participants with non-geocodable addresses (198 cases, 38 controls), missing education (34 cases, 85 controls), and racial/ethnic groups for whom the numbers of controls were too few for analyses (Asian American (231 cases, 86 controls) and Other (11 cases, 6 controls) race/ethnicity), and cases with in situ breast cancer (n=11), prior breast cancer (n=49), or ultimately determined not to be a CCR-reportable case (n=12). Data on the remaining 2,838 cases and 3,117 controls were used in the present analysis.
Data Collection
The SFBCS and the NC-BCFR used similar structured questionnaires on breast cancer risk factors administered in-person at the participant’s home by professional trained bilingual and bicultural interviewers in English, Spanish or Chinese (20). Information was collected up to the reference year, defined as the calendar year before diagnosis (cases) or selection into the study (controls). Both studies collected information on demographics, migration history, menstrual and pregnancy history, breastfeeding, first-degree family history of breast cancer, personal history of benign breast disease, hormone use, height, weight, alcohol consumption, and physical activity. Data were harmonized according to common definitions. Body mass index (BMI; kg/m2) was calculated as self-reported weight in the reference year divided by height at interview (self-report in NC-BCFR; measured in SFBCS). Lifetime recreational activities were available from both studies and harmonized as described elsewhere (23).
Residential addresses at the time of diagnosis (cases) or the reference year (controls) were batch geocoded in ArcGIS (ArcGIS, Version 10; Environmental Systems Research Institute, Inc., 2011) and assigned a 2000 Census block group, an area with an average of 1,500 residents. A total of 304 (12%) block groups had only one of each case and control and 941 (36%) had one or more case and control. Addresses were standardized to conform to U.S. Postal Service specifications using ZP4 software (ZP4. Monterey, CA: Semaphore Corp., 2011). Additional manual review of addresses that did not batch geocode resulted in the overall successful geocoding of 97% of residences. We operationalized nSES based on a composite index created using principal component analysis and resulting in seven 2000 Census block group-level measures (Liu education index (25) that weights the proportion of residents aged ≥ 25 years with a given level of education by the number of years needed to attain that education level; proportion with a blue collar job; proportion aged ≥ 16 years in the workforce without a job; median household income, percent below 200% of the poverty line, median rent, median house value) (26), explaining 60% of the overall variability. We scaled nSES and population density (population/m2) based on the quintile distribution for all block groups in California. The highest- and lowest-nSES quintiles represent the best and worst nSES categories, respectively. Other block group-level measures, including percentage of foreign-born residents, percentage of crowded households (households with ≥ 1 occupant per room), and percentage of residents who commute ≥60 min/day by car or motorcycle (19), were scaled based on the quartile distribution among controls.
Neighborhood amenities within walking distance, quantified as 1,600 meter pedestrian network distance, from a participant’s geocoded residence were derived in ArcGIS per a defined activity window (one year prior to reference year, during the reference year and two years after the reference year) using business listings from Walls & Associates’ National Establishment Time-Series Database (27), farmers’ markets listings from the California Department of Food and Agriculture (28), and park listings from NavTeq’s NavStreets database (29). Neighborhood food and retail environment were characterized based on two metrics: Restaurant Environment Index (REI), defined as the ratio of the number of fast-food restaurants to other restaurants; and Retail Food Environment Index (RFEI), defined as the ratio of the number of convenience stores, liquor stores, and fast-food restaurants to supermarkets and farmers’ markets (30). Street connectivity at the Census tract level, a measure of walkability, was assessed using the gamma index, defined as the ratio of actual number of street segments to maximum possible number of intersections (31), with data from NavTeq’s NavStreets database (29). These neighborhood characteristics were scaled based on the tertile or quartile distributions among controls, to balance sample sizes across categories of each neighborhood measure.
Statistical analysis
Multivariable multilevel logistic regression models were used to estimate odds ratios (OR) and 95% confidence intervals (CI) for breast cancer risk associated with education and/or nSES, with a random intercept for each block group to account for clustering of individuals within neighborhoods. Stratified analyses are presented to examine differences across racial/ethnic groups and, among Hispanics, by nativity (U.S.-born vs. foreign-born). Models were adjusted for age, study, and risk factors associated with breast cancer risk (P < 0.05 in models adjusted for age, race/ethnicity, and study): first-degree family history of breast cancer, benign breast disease, age at menarche, parity, breastfeeding, age at first full-term birth, menopausal status, menopausal hormone therapy use, alcohol intake in reference year, and body mass index (BMI) in reference year. The lowest two nSES quintiles were collapsed for NHWs and U.S.-born Hispanics due to small numbers. We sequentially adjusted for additional neighborhood characteristics to determine the extent to which they explained the nSES-breast cancer associations. We created a composite variable to examine joint associations for education and nSES: low education (≤high school degree) versus high education (>high school degree) and low nSES (quintiles 1 to 3) versus high nSES (quintiles 4 to 5) (24). Tests for heterogeneity/interaction were performed by adding a multiplicative cross-product term of race/ethnicity and nativity with education, nSES, or composite education-nSES variable or education (low, high) with nSES (low, high) variables. Tests for trend were performed by entering the categorical variable as an ordinal parameter. Analyses were conducted using SAS (version 9.3, Cary, NC), with a 2-sided P value of < 0.05 considered statistically significant.
RESULTS
NHW, African American, U.S.-born Hispanic, and foreign-born Hispanic women comprised 40% (n=1,141), 20% (n=563), 20% (n=570), and 20% (n=564) of the breast cancer cases, respectively. Education and nSES were modestly correlated among cases and control (ρ=0.39 for both). Figure 1 shows the geographic locations of the cases and controls, overlaid onto the geographic variability of nSES. Among both cases and controls (Table 1), most NHWs had beyond high school education and lived in high-SES neighborhoods (quintiles 4 and 5). African Americans were more likely to live in low-SES neighborhoods regardless of education, while higher education corresponded with living in high-SES neighborhoods among NHW and Hispanic (U.S.- and foreign-born) women. A higher proportion of foreign-born compared to U.S.-born Hispanic women with lower education lived in low-SES neighborhoods. Across race/ethnicity and nativity, cases compared to controls were more educated and more likely to live in the highest-SES neighborhood (quintile 5), and therefore more likely to be in the highest concordant education-nSES category (Table 1).
Figure 1.
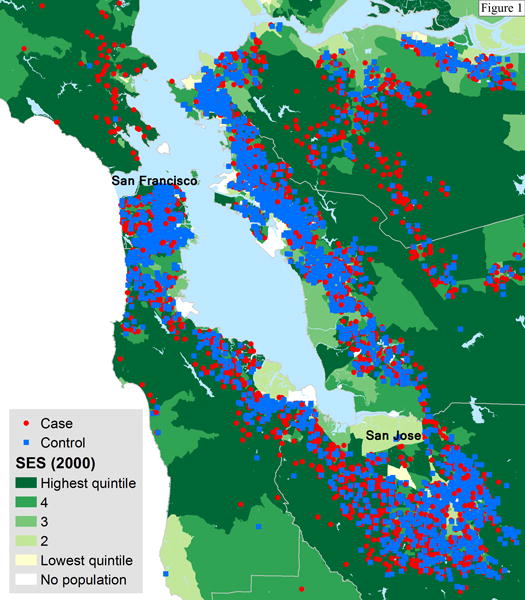
Locations of cases and controls in the Neighborhoods and Breast Cancer Study, 1995–2002 and geographic variability of composite neighborhood socioeconomic status (SES) for the San Francisco Bay Area based on seven U.S. Census 2000 block group-level measures: Liu education index, proportion with a blue collar job, proportion older than age 16 in the workforce without a job, median household income, percent below 200% of the poverty line, median rent, median house value. Neighborhood SES was scaled based on the quintile distribution for all block groups in California.
Table 1.
Distribution of socioeconomic status measures and breast cancer risk factors by race/ethnicity and nativity, Neighborhoods and Breast Cancer Study, San Francisco Bay Area, 1995–2002.
| Non-Hispanic white | African-American | U.S.-Born Hispanic | Foreign-Born Hispanic | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||
| Case n=1,141 | Control n=1,017 | Case n=563 | Control n=663 | Case n=570 | Control n=505 | Case n=564 | Control n=932 | Case n=2,838 | Control n=3,117 | |
|
| ||||||||||
| % | % | % | % | % | % | % | % | % | % | |
| Education | ||||||||||
| Some high school or less | 4.5 | 5.3 | 18.7 | 18.3 | 27.4 | 27.9 | 50.0 | 65.5 | 20.9 | 29.7 |
| High school degree or equivalent | 16.7 | 16.9 | 20.8 | 24.1 | 29.8 | 30.3 | 14.9 | 14.8 | 19.8 | 20.0 |
| Vocational/technical degree or some college | 35.4 | 35.2 | 41.2 | 39.7 | 28.8 | 27.7 | 19.5 | 11.3 | 32.1 | 27.8 |
| College degree or higher degree | 43.4 | 42.6 | 19.4 | 17.9 | 14.0 | 14.1 | 15.6 | 8.5 | 27.2 | 22.5 |
| nSESa | ||||||||||
| Quintile 1-low nSES | 1.1 | 1.1 | 13.5 | 19.8 | 3.3 | 3.6 | 5.1 | 7.2 | 4.8 | 7.3 |
| Quintile 2 | 3.1 | 7.0 | 29.1 | 31.8 | 11.8 | 17.0 | 18.3 | 25.2 | 13.0 | 19.3 |
| Quintile 3 | 9.0 | 11.8 | 21.0 | 18.6 | 19.5 | 25.5 | 23.8 | 27.0 | 16.4 | 20.0 |
| Quintile 4 | 24.0 | 26.5 | 22.2 | 18.4 | 29.6 | 27.1 | 25.4 | 26.3 | 25.1 | 24.8 |
| Quintile 5-high nSES | 62.8 | 53.6 | 14.2 | 11.5 | 35.8 | 26.7 | 27.5 | 14.3 | 40.7 | 28.5 |
| Education and nSESa,b | ||||||||||
| ≤ High school degree, low nSES | 5.1 | 7.4 | 29.7 | 35.0 | 25.1 | 31.3 | 38.5 | 51.9 | 20.6 | 30.4 |
| ≤ HS degree, high nSES | 16.1 | 14.8 | 9.8 | 7.4 | 32.1 | 26.9 | 26.4 | 28.3 | 20.1 | 19.2 |
| > HS degree, low nSES | 8.1 | 12.5 | 33.9 | 35.1 | 9.5 | 14.9 | 8.7 | 7.5 | 13.6 | 16.2 |
| > HS degree, high nSES | 70.7 | 65.3 | 26.6 | 22.5 | 33.3 | 26.9 | 26.4 | 12.2 | 45.7 | 34.1 |
| Study | ||||||||||
| Northern California Breast Cancer Family Registry | 48.5 | 37.4 | 5.2 | 10.9 | 4.9 | 7.1 | 5.5 | 3.6 | 22.6 | 16.7 |
| San Francisco Bay Area Breast Cancer Study | 51.5 | 62.6 | 94.8 | 89.1 | 95.1 | 92.9 | 94.5 | 96.4 | 77.4 | 83.3 |
| Age groups (y) | ||||||||||
| <45 | 23.0 | 21.0 | 20.6 | 17.2 | 21.8 | 20.4 | 27.0 | 26.3 | 23.0 | 21.7 |
| 45–54 | 29.5 | 30.2 | 30.2 | 30.3 | 30.2 | 30.3 | 31.4 | 31.3 | 30.2 | 30.6 |
| 55–64 | 29.0 | 26.1 | 23.8 | 27.0 | 25.8 | 22.2 | 24.5 | 26.0 | 26.4 | 25.6 |
| ≥65 | 18.5 | 22.7 | 25.4 | 25.5 | 22.3 | 27.1 | 17.2 | 16.4 | 20.4 | 22.1 |
| Family History of breast cancer | 36.3 | 14.7 | 14.2 | 12.2 | 14.4 | 14.1 | 11.0 | 5.4 | 22.5 | 11.3 |
| Benign Breast Disease | 23.9 | 17.9 | 21.0 | 16.3 | 17.9 | 17.0 | 14.7 | 9.9 | 20.3 | 15.0 |
| Age at Menarche (y)c | ||||||||||
| ≤11 | 19.5 | 20.1 | 22.4 | 22.2 | 29.5 | 29.9 | 24.8 | 19.3 | 23.1 | 21.9 |
| 12 | 27.5 | 27.5 | 29.1 | 25.2 | 27.2 | 24.4 | 22.9 | 18.0 | 26.8 | 23.7 |
| 13 | 30.1 | 29.0 | 22.0 | 26.5 | 22.3 | 24.4 | 23.0 | 22.7 | 25.5 | 25.9 |
| ≥14 | 22.2 | 23.0 | 25.8 | 25.5 | 20.5 | 21.0 | 28.5 | 39.1 | 23.8 | 28.0 |
| Parity | ||||||||||
| 0 | 24.9 | 23.0 | 17.2 | 13.1 | 13.3 | 10.1 | 12.1 | 4.8 | 18.5 | 13.4 |
| 1 | 14.8 | 15.2 | 19.0 | 18.6 | 14.0 | 9.3 | 11.5 | 9.3 | 14.8 | 13.2 |
| 2 | 32.3 | 32.6 | 22.2 | 24.1 | 26.0 | 22.0 | 25.2 | 19.1 | 27.6 | 25.1 |
| 3 | 16.7 | 16.2 | 18.1 | 19.6 | 21.4 | 26.5 | 21.1 | 23.1 | 18.8 | 20.7 |
| ≥4 | 11.3 | 12.9 | 23.4 | 24.6 | 25.3 | 32.1 | 30.1 | 43.7 | 20.3 | 27.7 |
| Breastfeeding (months)c | ||||||||||
| Nulliparous | 24.9 | 23.0 | 17.2 | 13.1 | 13.3 | 10.1 | 12.1 | 4.8 | 18.5 | 13.4 |
| 0 | 28.0 | 27.6 | 44.8 | 46.5 | 43.3 | 38.2 | 21.8 | 20.0 | 33.2 | 31.1 |
| <12 | 29.1 | 26.2 | 18.8 | 22.3 | 25.8 | 30.5 | 31.4 | 25.6 | 26.8 | 25.9 |
| 12–23 | 11.0 | 12.0 | 8.9 | 7.5 | 10.2 | 11.3 | 14.7 | 19.4 | 11.2 | 13.2 |
| ≥ 24 | 6.7 | 11.2 | 10.3 | 10.6 | 7.4 | 9.9 | 20.0 | 30.2 | 10.2 | 16.5 |
| Age at first full-term birth (y)c | ||||||||||
| Nulliparous | 24.9 | 23.0 | 17.2 | 13.1 | 13.3 | 10.1 | 12.1 | 4.8 | 18.5 | 13.4 |
| <20 | 10.0 | 9.0 | 33.9 | 36.8 | 23.5 | 28.9 | 17.9 | 25.5 | 19.0 | 23.1 |
| 20–24 | 28.1 | 29.0 | 29.1 | 32.4 | 35.4 | 34.5 | 35.6 | 35.7 | 31.3 | 32.6 |
| 25–29 | 21.6 | 21.1 | 11.0 | 11.3 | 16.8 | 17.0 | 20.7 | 20.9 | 18.4 | 18.3 |
| ≥30 | 15.2 | 17.8 | 8.7 | 6.3 | 10.7 | 9.3 | 13.7 | 12.0 | 12.7 | 12.3 |
| Years since last full-term birthc | ||||||||||
| Nulliparous | 24.9 | 23.0 | 17.2 | 13.1 | 13.3 | 10.1 | 12.1 | 4.8 | 18.5 | 13.4 |
| <2 | 2.3 | 0.8 | 1.1 | 1.1 | 0.9 | 1.0 | 1.6 | 2.5 | 1.6 | 1.4 |
| 2–4 | 3.7 | 4.6 | 2.1 | 1.2 | 2.3 | 2.6 | 4.3 | 4.2 | 3.2 | 3.4 |
| ≥5 | 68.8 | 71.5 | 79.4 | 84.6 | 83.3 | 85.9 | 81.9 | 87.3 | 76.4 | 81.4 |
| Ever hormonal contraception used | 67.7 | 73.5 | 59.3 | 64.4 | 66.5 | 69.1 | 56.0 | 56.8 | 63.5 | 65.8 |
| Postmenopausal status | 64.9 | 56.5 | 60.9 | 62.3 | 58.1 | 59.8 | 52.7 | 54.8 | 60.3 | 57.8 |
| Menopausal hormone therapy used | ||||||||||
| Never | 50.0 | 49.0 | 70.3 | 63.5 | 61.1 | 57.8 | 67.7 | 68.9 | 59.8 | 59.4 |
| Former | 19.0 | 29.0 | 15.1 | 26.7 | 12.8 | 32.9 | 14.4 | 24.5 | 16.1 | 27.8 |
| Current | 30.9 | 22.0 | 14.6 | 9.8 | 26.1 | 9.3 | 17.9 | 6.7 | 24.1 | 12.8 |
| Alcohol consumption (g/day)c,e | ||||||||||
| 0 | 35.9 | 41.3 | 61.6 | 63.7 | 53.9 | 58.6 | 67.2 | 71.5 | 50.8 | 57.9 |
| <5 | 22.3 | 21.2 | 17.4 | 16.7 | 24 | 21.8 | 18.1 | 19.3 | 20.8 | 19.8 |
| 5–9.9 | 12.3 | 12.0 | 5.5 | 5.1 | 5.4 | 7.3 | 5.1 | 4.4 | 8.1 | 7.5 |
| 10–14.9 | 10.3 | 9.1 | 3.2 | 5.6 | 7.2 | 4.6 | 5.1 | 3.0 | 7.3 | 5.8 |
| ≥15 | 18.6 | 16.2 | 12.1 | 8.7 | 9.1 | 7.5 | 4.4 | 1.8 | 12.6 | 8.9 |
| Lifetime recreational physical activity (hrs/wk) d | ||||||||||
| 0 | 6.2 | 5.8 | 16.7 | 17.3 | 16.7 | 18.8 | 30.0 | 33.4 | 15.1 | 18.6 |
| Quartile 1-low | 28.0 | 36.1 | 45.8 | 44.9 | 56.7 | 58.0 | 49.1 | 46.5 | 41.5 | 44.6 |
| Quartile 2 | 12.5 | 12.8 | 12.8 | 14.6 | 11.6 | 9.1 | 8.7 | 10.4 | 11.6 | 11.9 |
| Quartile 3 | 19.7 | 14.9 | 13.3 | 11 | 8.6 | 6.9 | 6.7 | 4.4 | 13.6 | 9.7 |
| Quartile 4-high | 33.6 | 30.4 | 11.4 | 12.1 | 6.5 | 7.1 | 5.5 | 5.4 | 18.1 | 15.2 |
| Body mass index (kg/m2)c,e | ||||||||||
| <25 | 56.2 | 51.0 | 28.6 | 25.0 | 33.7 | 26.5 | 28.9 | 20.2 | 40.8 | 32.3 |
| 25–29.9 | 23.9 | 26.8 | 31.6 | 32.3 | 32.3 | 28.9 | 36.3 | 41.5 | 29.6 | 32.7 |
| ≥30 | 19.1 | 21.7 | 38.5 | 41.6 | 33.5 | 43.0 | 32.1 | 33.8 | 28.4 | 33.0 |
Neighborhood socioeconomic status (nSES) based on composite index of seven U.S. Census 2000 block group-level measures: Liu education index, proportion with a blue collar job, proportion older than age 16 in the workforce without a job, median household income, percent below 200% of the poverty line, median rent, median house value. Quintiles based on statewide distributions.
Combined variable for education (high school degree or less vs. more than high school degree) and nSES (low (quintiles 1–3) vs. high (quintiles 4 and 5)).
Percentages may not add to 100 due to missing.
Pre-diagnosis (cases) or before referent date (controls).
In reference year.
For both cases and controls, there was substantial variability in the distribution of individual-level breast cancer risk factors (Table 1) and neighborhood factors (Table 2) by race/ethnicity and nativity. NHW women were more likely than other groups to be nulliparous, aged 30 years or more at first full-term birth, normal weight (BMI < 25), and alcohol consumers. African Americans and U.S.-born Hispanics were more likely compared to other groups to not have breastfed and to be obese (BMI ≥30). Foreign-born Hispanics were more likely than other groups to be older at menarche (≥14 years), have four or more children, breastfeed for more than 12 months, and have limited alcohol consumption. Across racial/ethnic and nativity groups, cases were less likely than controls to live in neighborhoods characterized by high (quartile 4) population density, high (quartile 4) household crowding, and high density (≥ 4) of parks.
Table 2.
Distribution of neighborhood characteristics by race/ethnicity and nativity, the Neighborhoods and Breast Cancer Study, 1995–2002.
| Neighborhood characteristics | Non-Hispanic white | African-American | U.S.-Born Hispanic | Foreign-Born Hispanic | ||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Case n=1,141 | Control n=1,017 | Case n=563 | Control n=663 | Case n=570 | Control n=505 | Casen=564 | Control n=932 | |
|
| ||||||||
| % | % | % | % | % | % | % | % | |
| Population density (per m2)a,b | ||||||||
| Quartile 1-low | 21.7 | 16.7 | 8.2 | 6.5 | 13.3 | 11.5 | 10.8 | 5.9 |
| Quartile 2 | 28.3 | 24.3 | 14.0 | 13.1 | 21.8 | 19.0 | 14.9 | 10.9 |
| Quartile 3 | 30.3 | 31.6 | 21.5 | 18.6 | 34.9 | 30.7 | 25.4 | 21.6 |
| Quartile 4-high | 19.6 | 27.4 | 56.3 | 61.8 | 30.0 | 38.8 | 48.9 | 61.6 |
| % crowded householdsa,c | ||||||||
| Quartile 1-low | 59.7 | 48.8 | 18.7 | 13.7 | 29.7 | 21.6 | 19.0 | 10.3 |
| Quartile 2 | 27.1 | 31.8 | 33.4 | 27.3 | 29.0 | 27.7 | 25.5 | 15.8 |
| Quartile 3 | 10.1 | 13.7 | 32.0 | 36.5 | 22.1 | 23.6 | 27.1 | 30.2 |
| Quartile 4-high | 3.2 | 5.8 | 16.0 | 22.5 | 19.3 | 27.1 | 28.4 | 43.8 |
| % commute by car/motorcyclea,c | ||||||||
| Quartile 1-low | 17.4 | 20.4 | 33.0 | 38.0 | 10.4 | 12.5 | 20.4 | 28.0 |
| Quartile 2 | 25.1 | 23.4 | 34.3 | 35.4 | 16.7 | 21.0 | 22.9 | 22.4 |
| Quartile 3 | 28.2 | 28.3 | 19.2 | 16.4 | 34.0 | 29.7 | 30.9 | 25.3 |
| Quartile 4-high | 29.4 | 27.9 | 13.5 | 10.1 | 39.0 | 36.8 | 25.9 | 24.3 |
| Restaurant environment indexd,e,f | ||||||||
| No fast food restaurants | 34.7 | 26.9 | 21.9 | 16.7 | 25.3 | 18.4 | 22.9 | 15.9 |
| Tertile 1-low | 20.1 | 24.3 | 22.7 | 20.4 | 18.1 | 19.2 | 24.5 | 26.6 |
| Tertile 2 | 17.3 | 19.3 | 26.5 | 30.5 | 24.9 | 29.5 | 27.0 | 28.9 |
| Tertile 3-high | 15.0 | 19.7 | 23.6 | 28.5 | 25.8 | 28.7 | 20.2 | 26.4 |
| No Restaurants | 13.0 | 9.8 | 5.3 | 3.9 | 6.0 | 4.2 | 5.5 | 2.3 |
| Retail food environment indexf,g | ||||||||
| No convenient stores, liquor stores and fast food restaurants | 9.6 | 7.4 | 4.1 | 3.3 | 4.4 | 5.2 | 3.7 | 2.4 |
| <1 | 37.9 | 41.9 | 61.8 | 72.7 | 42.6 | 45.2 | 57.8 | 63.4 |
| ≥1 | 38.4 | 40.4 | 29.8 | 21.0 | 45.4 | 44.8 | 32.5 | 31.7 |
| No retail food outlets | 14.2 | 10.3 | 4.3 | 3.0 | 7.5 | 5.0 | 6.0 | 2.6 |
| Number of recreational facilitiesc,f | ||||||||
| ≤1 | 35.7 | 28.4 | 27.9 | 27.6 | 29.3 | 29.3 | 27.0 | 21.1 |
| 2–3 | 23.8 | 25.0 | 26.6 | 22.8 | 25.8 | 26.1 | 22.9 | 24.4 |
| 4–7 | 22.5 | 24.7 | 24.2 | 29.3 | 28.1 | 26.7 | 25.2 | 28.5 |
| ≥8 | 18.0 | 21.9 | 21.3 | 20.4 | 16.8 | 17.8 | 25.0 | 26.0 |
| Number of parksf | ||||||||
| 0 | 20.3 | 17.1 | 8.9 | 9.1 | 18.4 | 15.1 | 11.2 | 9.8 |
| 1 | 26.4 | 25.8 | 21.1 | 17.7 | 26.0 | 26.5 | 22.0 | 22.8 |
| 2 | 21.4 | 20.9 | 19.7 | 17.8 | 24.7 | 25.7 | 23.4 | 23.0 |
| 3 | 14.3 | 14.1 | 19.7 | 21.4 | 17.4 | 16.2 | 19.3 | 18.5 |
| ≥4 | 17.6 | 22.2 | 30.6 | 34.1 | 13.5 | 16.4 | 24.1 | 26.1 |
| Street connectivity, gamma indexc,h | ||||||||
| Quartile 1-low | 43.1 | 35.1 | 17.6 | 14.9 | 34.0 | 28.9 | 24.1 | 19.0 |
| Quartile 2 | 28.8 | 26.2 | 19.9 | 16.1 | 29.5 | 30.5 | 31.4 | 25.0 |
| Quartile 3 | 15.9 | 19.0 | 28.8 | 35.6 | 20.7 | 23.4 | 20.4 | 26.7 |
| Quartile 4-high | 12.3 | 19.8 | 33.8 | 33.3 | 15.8 | 17.2 | 24.1 | 29.3 |
| % foreign-born residentsa,c | ||||||||
| Quartile 1-low | 47.4 | 38.9 | 33.2 | 32.7 | 24.7 | 20.8 | 16.7 | 9.1 |
| Quartile 2 | 30.5 | 32.9 | 29.7 | 24.1 | 29.8 | 25.9 | 22.5 | 17.4 |
| Quartile 3 | 14.8 | 18.9 | 24.3 | 25.9 | 26.1 | 29.3 | 26.4 | 29.0 |
| Quartile 4-high | 7.3 | 9.2 | 12.8 | 17.2 | 19.3 | 24.0 | 34.4 | 44.5 |
U.S. Census block group-level measure
Categorization based on the quartile distribution for block groups in California.
Categorization based on quartile distribution among controls in study population.
Categorization based on tertile distribution among controls with non-zero values in study population.
Ratio of the number of fast food restaurants to other restaurants.
Businesses/parks within walking distance of residence (1,600 m pedestrian network)
Ratio of the number of convenience stores, liquor stores, and fast food restaurants to supermarkets and farmers’ markets.
Ratio of actual number of street segments to maximum possible number of intersections per U.S. Census tract.
Education was associated with breast cancer risk only among Hispanics, with heterogeneity by race/ethnicity and nativity (Pheterogeneity=0.03; Table 3). A positive association with education was observed among foreign-born Hispanics without adjustment for nSES (Ptrend<0.01). The association was attenuated after adjustment for nSES (Ptrend=0.04) and only the OR estimate for vocational/technical degree or some college compared to some high school or less remained statistically significant (OR=1.62; 95% CI, 1.13–2.32). An opposite pattern of association was observed among U.S.-born Hispanics (Ptrend=0.07); statistically significant inverse associations were observed after adjustment for nSES (Ptrend=0.01).
Table 3.
Associations between education, neighborhood socioeconomic status and breast cancer risk by race/ethnicity and nativity, the Neighborhoods and Breast Cancer Study, 1995–2002.
| SES variable | Non-Hispanic white | African-American | U.S.-born Hispanics | Foreign-born Hispanics |
|---|---|---|---|---|
|
| ||||
| OR (95% CI)a | OR (95% CI)a | OR (95% CI)a | OR (95% CI)a | |
| Individual associationsb | ||||
| Education | ||||
| Some high school or less | 1.00 | 1.00 | 1.00 | 1.00 |
| High school degree or equivalent | 1.25 (0.75–2.09) | 0.89 (0.60–1.33) | 0.77 (0.53–1.12) | 1.03 (0.73–1.44) |
| Vocational/technical degree or some college | 1.16 (0.71–1.89) | 1.09 (0.75–1.58) | 0.70 (0.47–1.06) | 1.81 (1.28–2.57) |
| College degree or higher degree | 1.16 (0.70–1.92) | 1.08 (0.69–1.69) | 0.65 (0.39–1.08) | 1.54 (1.03–2.30) |
| Ptrend | 0.95 | 0.47 | 0.07 | <0.01 |
| nSESc | ||||
| Quintile 1-low nSES | 1.00 | 1.00 | ||
| Quintile 2 | 1.00 | 1.38 (0.94–2.02) | 1.00 | 1.00 (0.59–1.71) |
| Quintile 3 | 1.35 (0.80–2.26) | 1.77 (1.17–2.67) | 0.96 (0.63–1.47) | 1.20 (0.71–2.03) |
| Quintile 4 | 1.74 (1.09–2.76) | 1.77 (1.18–2.67) | 1.33 (0.89–2.01) | 1.21 (0.72–2.06) |
| Quintile 5-high nSES | 2.22 (1.43–3.46) | 1.76 (1.10–2.83) | 1.66 (1.10–2.52) | 2.09 (1.21–3.61) |
| Ptrend | <0.01 | 0.01 | <0.01 | <0.01 |
| Independent associationsb | ||||
| Education | ||||
| Some high school or less | 1.00 | 1.00 | 1.00 | 1.00 |
| High school degree or equivalent | 1.12 (0.67–1.88) | 0.86 (0.57–1.28) | 0.71 (0.48–1.04) | 0.94 (0.66–1.33) |
| Vocational/technical degree or some college | 1.00 (0.61–1.63) | 0.99 (0.68–1.45) | 0.63 (0.42–0.96) | 1.62 (1.13–2.32) |
| College degree or higher degree | 0.95 (0.57–1.58) | 0.95 (0.60–1.50) | 0.53 (0.31–0.89) | 1.34 (0.89–2.03) |
| Ptrend | 0.35 | 0.93 | 0.01 | 0.04 |
| nSESc | ||||
| Quintile 1-low nSES | 1.00 | 1.00 | ||
| Quintile 2 | 1.00 | 1.38 (0.94–2.02) | 1.00 | 0.97 (0.57–1.63) |
| Quintile 3 | 1.38 (0.82–2.31) | 1.76 (1.16–2.67) | 0.95 (0.62–1.46) | 1.14 (0.68–1.91) |
| Quintile 4 | 1.78 (1.12–2.84) | 1.77 (1.17–2.69) | 1.41 (0.93–2.13) | 1.11 (0.65–1.87) |
| Quintile 5-high nSES | 2.27 (1.45–3.56) | 1.74 (1.07–2.83) | 1.82 (1.19–2.79) | 1.83 (1.06–3.17) |
| Ptrend | <0.01 | 0.01 | <0.01 | <0.01 |
| Joint associationsb | ||||
| Education and nSESc | ||||
| ≤ High school degree, low nSES | 1.00 | 1.00 | 1.00 | 1.00 |
| ≤ High school degree, high nSES | 1.83 (1.14–2.95) | 1.57 (0.98–2.52) | 1.41 (0.98–2.04) | 1.15 (0.86–1.53) |
| > High school degree, low nSES | 0.99 (0.59–1.65) | 1.23 (0.90–1.68) | 0.65 (0.40–1.06) | 1.21 (0.78–1.89) |
| > High school degree, high nSES | 1.64 (1.06–2.54) | 1.39 (0.97–1.97) | 1.20 (0.81–1.78) | 2.17 (1.52–3.09) |
Note: Values in bold represent a P value < 0.05.
Odds ratios (OR) and 95% confidence intervals (CI) from multilevel logistic regression models with random intercept for each block group adjusted for age, study, family history of breast cancer, benign breast disease, age at menarche, parity, breast feeding, age at first full-term birth, menopausal status, menopausal hormonal therapy use, body mass index, and alcohol intake.
Education and neighborhood socioeconomic status (nSES) modeled in separate models for individual associations and modeled together in one model for independent associations. Joint associations based on combined education (high school degree or less vs. more than high school degree) and nSES (low (quintiles 1–3) or high (quintiles 4 and 5)) variable.
Composite index for nSES based on seven U.S. Census 2000 block group-level measures: Liu education index, proportion with a blue collar job, proportion older than age 16 in the workforce without a job, median household income, percent below 200% of the poverty line, median rent, median house value. Quintiles based on statewide distributions. The lowest two nSES quintiles were collapsed for non-Hispanic whites and US-born Hispanics due to small numbers.
Consistent associations between nSES and breast cancer risk were observed across race/ethnicity and nativity (Pheterogeneity=0.30), with women living in high-SES neighborhoods being at increased odds for breast cancer and with evidence of a positive dose-response gradient (Table 3). Across all racial/ethnic and nativity groups, living in the highest relative to lowest nSES quintiles (lowest two quintiles for NHWs and U.S.-born Hispanics) was associated with 66%-222% greater odds of breast cancer without adjustment for nSES and 74%-227% greater odds of breast cancer with adjustment for nSES. Considering the joint associations of education and nSES, different patterns of associations were observed across race/ethnicity and nativity (Pheterogeneity<0.01). Statistically significant positive associations were observed between high nSES and breast cancer (64–83% greater odds) regardless of individual education among NHWs (Pinteraction=0.72). Among foreign-born Hispanics, joint high education/high nSES was associated with 2-fold higher odds compared to their race/ethnic/nativity-specific low education/low nSES counterpart (Pinteraction=0.11).
Neighborhood SES-breast cancer associations were attenuated across race/ethnicity and nativity with adjustment for urban characteristics (Table 4, Model 2) and mixed-land use characteristics (Table 4, Model 3). Significant associations persisted with adjustment for urban characteristics only among NHWs and with adjustment for mixed-land use among NHWs and U.S.-born Hispanics. When accounting for education and nSES (Supplemental Table 1), we observed significant inverse associations between odds of breast cancer and population density among NHWs (Ptrend=0.01), household crowding among African Americans (Ptrend=0.02) and foreign-born Hispanics (Ptrend=0.02), REI among NHWs, African Americans, and foreign-born Hispanics (Ptrend≤0.01 for all), and street connectivity among NHWs (Ptrend=0.01).
Table 4.
Associations between education, neighborhood socioeconomic status and breast cancer risk independent of neighborhood contextual factors by race/ethnicity and nativity, the Neighborhoods and Breast Cancer Study, 1995–2002.
| Model 0 (Minimally- adjusted)a |
Model 1 (+ individual-level risk factors)b |
Model 2 (Model 1 + urban factors)c |
Model 3 (Model 1 + mixed-land use)d |
Model 4 (Model 1 + population density, % foreign-born)e |
|
|---|---|---|---|---|---|
|
| |||||
| OR (95% CI)f | OR (95% CI)f | OR (95% CI)f | OR (95% CI)f | OR (95% CI)f | |
| Non-Hispanic Whites | |||||
| Education | |||||
| Some high school or less | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| High school degree or equivalent | 1.04 (0.65–1.66) | 1.12 (0.67–1.88) | 1.10 (0.65–1.85) | 1.07 (0.64–1.82) | 1.10 (0.65–1.84) |
| Vocational/technical degree or some college | 0.91 (0.58–1.43) | 1.00 (0.61–1.63) | 0.96 (0.58–1.59) | 0.97 (0.58–1.60) | 0.97 (0.59–1.60) |
| College degree or higher degree | 0.87 (0.55–1.37) | 0.95 (0.57–1.58) | 0.91 (0.54–1.53) | 0.91 (0.54–1.54) | 0.94 (0.56–1.58) |
| Ptrend | 0.23 | 0.35 | 0.29 | 0.34 | 0.41 |
| nSESg | |||||
| Quintile 1,2-low nSES | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Quintile 3 | 1.48 (0.91–2.40) | 1.38 (0.82–2.31) | 1.27 (0.74–2.16) | 1.33 (0.78–2.25) | 1.30 (0.77–2.19) |
| Quintile 4 | 1.81 (1.17–2.79) | 1.78 (1.12–2.84) | 1.62 (0.97–2.70) | 1.58 (0.98–2.55) | 1.69 (1.05–2.70) |
| Quintile 5-high nSES | 2.37 (1.56–3.61) | 2.27 (1.45–3.56) | 1.72 (1.02–2.91) | 1.84 (1.16–2.93) | 1.96 (1.23–3.10) |
| Ptrend | <0.01 | <0.01 | 0.04 | 0.01 | <0.01 |
| Education and nSES | |||||
| ≤ High school degree, low nSES | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| ≤ High school degree, high nSES | 1.67 (1.07–2.59) | 1.83 (1.14–2.95) | 1.61 (0.98–2.66) | 1.59 (0.98–2.60) | 1.74 (1.08–2.81) |
| > High school degree, low nSES | 0.89 (0.55–1.42) | 0.99 (0.59–1.65) | 1.04 (0.62–1.73) | 1.01 (0.60–1.70) | 1.03 (0.62–1.71) |
| > High school degree, high nSES | 1.50 (1.01–2.23) | 1.64 (1.06–2.54) | 1.36 (0.85–2.18) | 1.39 (0.88–2.19) | 1.50 (0.97–2.34) |
| African Americans | |||||
| Education | |||||
| Some high school or less | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| High school degree or equivalent | 0.76 (0.52–1.12) | 0.86 (0.57–1.28) | 0.86 (0.58–1.28) | 0.87 (0.58–1.30) | 0.86 (0.58–1.29) |
| Vocational/technical degree or some college | 0.88 (0.62–1.26) | 0.99 (0.68–1.45) | 0.98 (0.67–1.43) | 1.00 (0.68–1.47) | 0.99 (0.68–1.45) |
| College degree or higher degree | 0.89 (0.58–1.35) | 0.95 (0.60–1.50) | 0.92 (0.58–1.44) | 0.99 (0.62–1.57) | 0.95 (0.60–1.49) |
| Ptrend | 0.83 | 0.93 | 0.93 | 0.81 | 0.95 |
| nSESg | |||||
| Quintile 1-low nSES | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Quintile 2 | 1.40 (0.96–2.05) | 1.38 (0.94–2.02) | 1.27 (0.86–1.87) | 1.09 (0.73–1.64) | 1.39 (0.95–2.04) |
| Quintile 3 | 1.73 (1.15–2.62) | 1.76 (1.16–2.67) | 1.54 (1.00–2.35) | 1.36 (0.87–2.12) | 1.82 (1.20–2.76) |
| Quintile 4 | 1.84 (1.22–2.78) | 1.77 (1.17–2.69) | 1.41 (0.90–2.22) | 1.11 (0.68–1.80) | 1.84 (1.21–2.81) |
| Quintile 5-high nSES | 1.86 (1.16–2.98) | 1.74 (1.07–2.83) | 1.26 (0.72–2.19) | 1.02 (0.57–1.81) | 1.78 (1.08–2.93) |
| Ptrend | <0.01 | 0.01 | 0.25 | 0.81 | <0.01 |
| Education and nSES | |||||
| ≤ High school degree, low nSES | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| ≤ High school degree, high nSES | 1.56 (0.99–2.47) | 1.57 (0.98–2.52) | 1.29 (0.79–2.09) | 1.15 (0.70–1.90) | 1.63 (1.02–2.62) |
| > High school degree, low nSES | 1.16 (0.86–1.56) | 1.23 (0.90–1.68) | 1.18 (0.86–1.62) | 1.22 (0.89–1.67) | 1.24 (0.90–1.70) |
| > High school degree, high nSES | 1.41 (1.02–1.96) | 1.39 (0.97–1.97) | 1.07 (0.72–1.60) | 0.98 (0.66–1.46) | 1.39 (0.96–2.00) |
| U.S.-born Hispanics | |||||
| Education | |||||
| Some high school or less | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| High school degree or equivalent | 0.84 (0.59–1.19) | 0.71 (0.48–1.04) | 0.69 (0.47–1.01) | 0.70 (0.47–1.03) | 0.70 (0.48–1.04) |
| Vocational/technical degree or some college | 0.85 (0.59–1.22) | 0.63 (0.42–0.96) | 0.61 (0.40–0.94) | 0.63 (0.41–0.95) | 0.62 (0.41–0.95) |
| College degree or higher degree | 0.72 (0.46–1.13) | 0.53 (0.31–0.89) | 0.51 (0.30–0.87) | 0.54 (0.32–0.92) | 0.53 (0.31–0.90) |
| Ptrend | 0.19 | 0.01 | 0.01 | 0.02 | 0.01 |
| nSESg | |||||
| Quintile 1,2-low nSES | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Quintile 3 | 1.03 (0.69–1.55) | 0.95 (0.62–1.46) | 0.90 (0.58–1.40) | 0.93 (0.60–1.45) | 0.92 (0.60–1.41) |
| Quintile 4 | 1.58 (1.06–2.34) | 1.41 (0.93–2.13) | 1.25 (0.78–2.01) | 1.41 (0.90–2.21) | 1.28 (0.83–1.95) |
| Quintile 5-high nSES | 1.99 (1.33–2.96) | 1.82 (1.19–2.79) | 1.43 (0.84–2.43) | 1.76 (1.09–2.83) | 1.54 (0.98–2.42) |
| Ptrend | <0.01 | <0.01 | 0.12 | <0.01 | 0.02 |
| Education and nSES | |||||
| ≤ High school degree, low nSES | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| ≤ High school degree, high nSES | 1.50 (1.07–2.10) | 1.41 (0.98–2.04) | 1.25 (0.82–1.89) | 1.43 (0.97–2.11) | 1.28 (0.88–1.86) |
| > High school degree, low nSES | 0.76 (0.49–1.19) | 0.65 (0.40–1.06) | 0.66 (0.40–1.07) | 0.68 (0.41–1.11) | 0.65 (0.40–1.06) |
| > High school degree, high nSES | 1.54 (1.09–2.17) | 1.20 (0.81–1.78) | 1.03 (0.65–1.64) | 1.19 (0.79–1.81) | 1.07 (0.71–1.60) |
| Foreign-born Hispanics | |||||
| Education | |||||
| Some high school or less | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| High school degree or equivalent | 1.15 (0.83–1.58) | 0.94 (0.66–1.33) | 0.92 (0.65–1.30) | 0.96 (0.68–1.37) | 0.94 (0.66–1.33) |
| Vocational/technical degree or some college | 1.93 (1.40–2.67) | 1.62 (1.13–2.31) | 1.58 (1.10–2.27) | 1.71 (1.18–2.46) | 1.61 (1.12–2.31) |
| College degree or higher degree | 1.97 (1.37–2.82) | 1.34 (0.89–2.03) | 1.27 (0.84–1.94) | 1.34 (0.88–2.04) | 1.27 (0.84–1.94) |
| Ptrend | <0.01 | 0.03 | 0.05 | 0.02 | 0.05 |
| nSESg | |||||
| Quintile 1-low nSES | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Quintile 2 | 1.00 (0.60–1.66) | 0.96 (0.57–1.63) | 0.91 (0.53–1.55) | 0.88 (0.50–1.53) | 0.96 (0.56–1.63) |
| Quintile 3 | 1.19 (0.72–1.97) | 1.14 (0.68–1.91) | 1.00 (0.59–1.70) | 1.04 (0.60–1.82) | 1.11 (0.66–1.88) |
| Quintile 4 | 1.21 (0.73–2.00) | 1.11 (0.65–1.87) | 0.82 (0.46–1.44) | 0.95 (0.54–1.69) | 1.03 (0.61–1.76) |
| Quintile 5-high nSES | 2.13 (1.26–3.62) | 1.83 (1.06–3.17) | 1.11 (0.59–2.11) | 1.46 (0.79–2.69) | 1.48 (0.84–2.62) |
| Ptrend | <0.01 | <0.01 | 0.88 | 0.08 | 0.11 |
| Education and nSES | |||||
| ≤ High school degree, low nSES | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| ≤ High school degree, high nSES | 1.31 (0.99–1.72) | 1.15 (0.86–1.53) | 0.81 (0.58–1.13) | 0.99 (0.73–1.35) | 1.00 (0.75–1.35) |
| > High school degree, low nSES | 1.59 (1.05–2.40) | 1.21 (0.78–1.89) | 1.14 (0.72–1.79) | 1.18 (0.75–1.86) | 1.18 (0.75–1.85) |
| > High school degree, high nSES | 3.03 (2.22–4.13) | 2.17 (1.52–3.09) | 1.45 (0.97–2.18) | 1.95 (1.34–2.84) | 1.81 (1.25–2.63) |
Note: Values in bold represent a P value < 0.05.
Minimally-adjusted Model 0 adjusted for age and study.
Adjusted for same covariates as Model 0 with additional adjustments for individual-level risk factors (family history of breast cancer, benign breast disease, age at menarche, parity, breast feeding, age at first full-term birth, menopausal status, menopausal hormonal therapy use, body mass index, and alcohol intake).
Adjusted for same covariates as Model 1 with additional adjustments for urban environment (population density scaled on quartile distribution for block groups in California and percentage of crowded households scaled on quartile distribution among controls; both U.S. Census block group-level measures).
Adjusted for same covariates as Model 1 with additional adjustments for mixed-land use factors (Street connectivity based on gamma index, ratio of actual number of street segments to maximum possible number of intersections per census track scaled on quartile distribution among controls; % of residents commute by car/motorcycle, U.S. Census block group-level measure scaled on quartile distribution for block groups in California; restaurant environment index, ratio of the number of fast food restaurants to other restaurants; retail food environment index, ratio of the number of convenience stores, liquor stores, and fast food restaurants to supermarkets and farmers’ markets; number of recreational facilities and number of parks scaled on quartile distribution among controls; businesses/parks based on walking distance of residence (1,600 m pedestrian network)).
Adjusted for same covariates as Model 1 with additional adjustment for population density (scaled on quartile distribution for block groups in California) and % of residents foreign-born (scaled on quartile distribution for controls); both U.S. Census block group level measures.
Odds ratios (OR) and 95% confidence intervals (CI) from multilevel logistic regression models with random intercept for each block group. Education and neighborhood socioeconomic status (nSES) modeled together in one model for independent associations. Joint associations based on combined education (≤ or > high school graduate) and nSES (low (quintiles 1–3) or high (quintiles 4 and 5)) variable.
Composite index for nSES based on seven U.S. Census 2000 block group-level measures: Liu education index, proportion with a blue collar job, proportion older than age 16 in the workforce without a job, median household income, percent below 200% of the poverty line, median rent, median house value. Quintiles based on statewide distributions. The lowest two nSES quintiles were collapsed for non-Hispanic whites and U.S.-born Hispanics due to small numbers.
DISCUSSION
This is the first study, to our knowledge, to investigate the independent and joint associations of individual- and neighborhood-level SES on breast cancer risk among multiple racial/ethnic groups and by nativity among Hispanics. Combining data from two population-based California studies, we observed a positive nSES gradient of increased odds of breast cancer independent of education and individual-level breast cancer risk factors. Women residing in the highest versus lowest nSES quintile had about a two-fold higher odds of breast cancer with consistent associations across race/ethnicity and nativity. Furthermore, when considering education and nSES jointly using a composite variable, higher nSES was consistently associated with increased odds of breast cancer regardless of education; however, for most groups except NHWs, this nSES association was attenuated after adjusting for neighborhood built environment characteristics.
The present study begins to examine the underlying mechanisms explaining the contextual role of high nSES on breast cancer risk. We found that adjustment for urban characteristics attenuated the nSES-breast cancer association among African American, U.S.-born Hispanic and foreign-born Hispanic women, consistent with prior studies (17, 18), suggesting that neighborhood characteristics related to urban areas partly drive the association with nSES. This is supported by studies showing higher breast cancer incidence in urban and suburban than rural regions (32). Adjustment for mixed-land use attenuated the nSES-breast cancer association among African Americans and foreign-born Hispanics. Access to and utilization of mammography has been hypothesized to explain the increased risk associated with high nSES; yet, the association persists in studies adjusting for mammography, although these studies are limited by lacking details on timing and frequency of mammography (14, 17, 18). We were unable to adjust for mammography in the present study because it was only asked in the SFBCS. Rather than reflecting a pure neighborhood effect, the consistent nSES-breast cancer association may reflect compositional effects of individual-level SES that is not fully captured by education. Further research is needed to identify the unique aspects of high nSES, urban environments, and/or residents within those environments that pre-dispose them to higher risk of breast cancer.
Our finding of higher odds of breast cancer among women residing in neighborhoods of higher SES independent of individual-level risk factors is consistent with other population-based case-control studies that assessed associations with nSES at diagnosis (17, 18); however, the magnitude of association in our study is higher. In a Wisconsin case-control study examining tract-level nSES (18) and a Massachusetts case-control study examining block-group level nSES (17), living in the highest compared to the lowest nSES quintile was associated with 20–30% higher odds of breast cancer among primarily NHW women, while in the present study we observed about two-folds higher odds of breast cancer among NHWs, with slightly lower odds among African Americans (OR=1.7) and Hispanics (OR=1.8 for U.S.-born; OR=1.9 for foreign-born). A higher magnitude of association (OR=1.69) was observed when considering a 10-year latency period in the Massachusetts study (17). The higher magnitude of association we observed in our study may reflect the younger age of the cases (66% aged <60 years) compared to the Wisconsin (mean age 62 years) and Massachusetts (30% aged <60 years) studies, as another study using cancer registry data has found greater nSES gradients in breast cancer incidence among younger populations (26).
In contrast, prospective studies show null associations between block group-level nSES and breast cancer risk after accounting for education and individual-level risk factors (13, 14, 16). In the Black Women’s Health Study, associations close to the null were observed between a block group nSES measure and breast cancer risk (14). However, nSES was associated with estrogen receptor-positive breast cancer, but associations were attenuated close to the null after adjustment for education, reproductive and behavioral risk factors (14). In contrast, we did not find an association with education in African American women, but a robust association with nSES; the differing results may be a function of potentially larger nSES variability in our sample (given that the San Francisco Bay Area is one of the highest SES regions in the U.S.), and differences in the timing of assessment of residential nSES. Limited sample size and diverse geographic area may account for the lack of association in the other prospective studies of mostly NHW women in Washington (13) and Maryland (16). We had limited power to examine differential nSES-breast cancer associations by race/ethnicity/nativity and breast cancer subtypes. Socio-cultural factors might influence tumor biology, leading to more aggressive phenotypes among African Americans and Hispanics compared to NHWs (33, 34).
Weak or null education-breast cancer associations after adjustment for individual-level breast cancer risk factors are consistent with prior studies among NHW and African American populations (9, 14, 17, 18, 35, 36). In our study, additional adjustment for nSES further attenuated the weak positive associations toward the null while other studies observed minimal attenuation with adjustment for nSES (17, 18). Previous studies among Hispanics have controlled for rather than examined education as a primary risk factor for breast cancer (4, 37). This is the first study, to our knowledge, to investigate the independent association of education with breast cancer risk among Hispanics. Although the association was modest and imprecise for college graduates, foreign-born Hispanics with a vocational/technical degree or some college had a 62% higher odds of breast cancer compared to their counterparts with less than a high school degree, independent of nSES. Conversely, among U.S.-born Hispanics, higher education was associated with reduced odds of breast cancer. In contrast, the nSES-breast cancer associations were in the same direction for foreign-born and U.S.-born Hispanics. Education may capture different exposures among U.S.-born relative to foreign-born Hispanics and other racial/ethnic groups. Although foreign-born Hispanics have lower breast cancer incidence than U.S.-born Hispanics (38), established breast cancer risk factors explain less of the breast cancer risk in foreign-born than in U.S.-born Hispanics (20), thus the higher odds may reflect unidentified early life or environmental exposures among foreign-born Hispanics with higher education. Education as a single measure of SES may not capture the relevant individual-level SES experience of foreign-born versus U.S.-born Hispanics (39, 40). Furthermore, SES is a complex and multidimensional construct and other metrics beyond education may explain racial/ethnic disparities in health (41, 42). Nevertheless, among a host of social factors, the structural social penalty of low education has been shown to be related with considerable adverse health outcomes (43).
Our study of pooled data from two population-based studies has several strengths. Foremost, it is the most racial/ethnically diverse study of nSES and breast cancer risk independent of individual-level breast cancer risk factors to date. Particularly, the sizable number of Hispanics cases allowed us to examine differential associations by nativity. We examined a suite of small-area level (block group) social and built environment attributes in relation to breast cancer risk as well as potentially explaining the nSES-breast cancer association. The data have high fidelity in comprehensively assessing a broad array of risk factors collected by bilingual and bicultural interviewers and race/ethnicity based on self-report.
Several limitations should be considered. Our study used secondary data to characterize neighborhood environments that do not capture individuals’ direct experience (e.g., access or utilization of amenities) and may not accurately characterize individuals’ self-defined neighborhood (44), potentially resulting in conservative estimates. Future studies should aim to include a combination of secondary (objective) and perceived measures of neighborhood environments (45). We did not have data on individual-level income or wealth, but education is a stable measure that is typically attained relatively early in life and associated with a more consistent SES gradient in breast cancer incidence than other measures (10). Cumulative exposures and lagged effects are important to consider for neighborhood studies and health (46), particularly given the now well-recognized significance of early-life exposures in breast cancer risk (47–51). We did not capture residential history and are unable to account for moves prior to diagnosis, potentially resulting in non-differential misclassification of neighborhood environments. Although our models account for clustering of individuals within neighborhoods, future studies should also consider spatial models. However, results from one large cohort study suggest that current residence may reasonably approximate longer term environmental exposures related to urbanicity (52).
In conclusion, we found consistent nSES-breast cancer associations across several U.S. racial/ethnic and nativity groups. Adjustment for specific neighborhood factors attenuated the associations, suggesting they partly explain the association with nSES. We also discovered diverging education-breast cancer associations between foreign-born and U.S.-born Hispanic women that warrant further investigation. In addition, foreign-born Hispanics appear to be more susceptible to the joint influence of both individual- and contextual-level SES on breast cancer risk. These results have important implications for targeting public health prevention strategies across racial/ethnic populations, provide potential leads in terms of focusing on high SES and urban communities, and better understanding breast cancer risk across the life course.
Supplementary Material
Acknowledgments
We thank Marilyn Winkleby, Sarah Shema and Clayton Schupp for their contributions. The collection of cancer incidence data used in this study was supported by the California Department of Public Health as part of the statewide cancer reporting program mandated by California Health and Safety Code Section 103885; the National Cancer Institute’s Surveillance, Epidemiology, and End Results Program under contract HHSN261201000140C awarded to the Cancer Prevention Institute of California, contract HHSN261201000035C awarded to the University of Southern California, and contract HHSN261201000034C awarded to the Public Health Institute; and the Centers for Disease Control and Prevention’s National Program of Cancer Registries, under agreement U58DP003862-01 awarded to the California Department of Public Health.
Financial Support: This work was supported by National Cancer Institute grant R01CA140058 (S.L. Gomez). The Breast Cancer Family Registry (BCFR) was supported by grant UM1 CA164920 from the National Cancer Institute. The San Francisco Bay Area Breast Cancer Study was supported by grants from the National Cancer Institute R01 CA63446 and R01 CA77305, Department of Defense (DOD) DAMD17-96-1-6071, and the California Breast Cancer Research Program (CBCRP) 4JB-1106 and 7PB-0068.
Footnotes
Conflicts of Interest: None
References
- 1.Kohler BA, Sherman RL, Howlader N, Jemal A, Ryerson AB, Henry KA, et al. Annual Report to the Nation on the Status of Cancer, 1975–2011, Featuring Incidence of Breast Cancer Subtypes by Race/Ethnicity, Poverty, and State. J Natl Cancer Inst. 2015;107:djv048. doi: 10.1093/jnci/djv048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Howlader N, Noone AM, Krapcho M, Miller D, Bishop K, Altekruse SF, Kosary CL, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA, editors. SEER Cancer Statistics Review. National Cancer Institute; Bethesda, MD: 1975–2013. http://seer.cancer.gov/csr/1975_2013/, based on November 2015 SEER data submission, posted to the SEER web site, April 2016. [Google Scholar]
- 3.Chlebowski RT, Chen Z, Anderson GL, Rohan T, Aragaki A, Lane D, et al. Ethnicity and breast cancer: factors influencing differences in incidence and outcome. J Natl Cancer Inst. 2005;97:439–48. doi: 10.1093/jnci/dji064. [DOI] [PubMed] [Google Scholar]
- 4.Pike MC, Kolonel LN, Henderson BE, Wilkens LR, Hankin JH, Feigelson HS, et al. Breast cancer in a multiethnic cohort in Hawaii and Los Angeles: risk factor-adjusted incidence in Japanese equals and in Hawaiians exceeds that in whites. Cancer Epidemiol Biomarkers Prev. 2002;11:795–800. [PubMed] [Google Scholar]
- 5.Gathani T, Ali R, Balkwill A, Green J, Reeves G, Beral V, et al. Ethnic differences in breast cancer incidence in England are due to differences in known risk factors for the disease: prospective study. Br J Cancer. 2014;110:224–9. doi: 10.1038/bjc.2013.632. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Krieger N. Theories for social epidemiology in the 21st century: an ecosocial perspective. Int J Epidemiol. 2001;30:668–77. doi: 10.1093/ije/30.4.668. [DOI] [PubMed] [Google Scholar]
- 7.Kelsey JL, Bernstein L. Epidemiology and prevention of breast cancer. Annu Rev Public Health. 1996;17:47–67. doi: 10.1146/annurev.pu.17.050196.000403. [DOI] [PubMed] [Google Scholar]
- 8.Kelsey JL, Horn-Ross PL. Breast cancer: magnitude of the problem and descriptive epidemiology. Epidemiol Rev. 1993;15:7–16. doi: 10.1093/oxfordjournals.epirev.a036118. [DOI] [PubMed] [Google Scholar]
- 9.Heck KE, Pamuk ER. Explaining the relation between education and postmenopausal breast cancer. Am J Epidemiol. 1997;145:366–72. doi: 10.1093/oxfordjournals.aje.a009114. [DOI] [PubMed] [Google Scholar]
- 10.Clegg LX, Reichman ME, Miller BA, Hankey BF, Singh GK, Lin YD, et al. Impact of socioeconomic status on cancer incidence and stage at diagnosis: selected findings from the surveillance, epidemiology, and end results: National Longitudinal Mortality Study. Cancer Causes Control. 2009;20:417–35. doi: 10.1007/s10552-008-9256-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lundqvist A, Andersson E, Ahlberg I, Nilbert M, Gerdtham U. Socioeconomic inequalities in breast cancer incidence and mortality in Europe-a systematic review and meta-analysis. Eur J Public Health. 2016 doi: 10.1093/eurpub/ckw070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Akinyemiju TF, Genkinger JM, Farhat M, Wilson A, Gary-Webb TL, Tehranifar P. Residential environment and breast cancer incidence and mortality: a systematic review and meta-analysis. BMC Cancer. 2015;15:191. doi: 10.1186/s12885-015-1098-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hastert TA, Beresford SA, Sheppard L, White E. Disparities in cancer incidence and mortality by area-level socioeconomic status: a multilevel analysis. J Epidemiol Community Health. 2015;69:168–76. doi: 10.1136/jech-2014-204417. [DOI] [PubMed] [Google Scholar]
- 14.Palmer JR, Boggs DA, Wise LA, Adams-Campbell LL, Rosenberg L. Individual and neighborhood socioeconomic status in relation to breast cancer incidence in African-American women. Am J Epidemiol. 2012;176:1141–6. doi: 10.1093/aje/kws211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Robert SA, Strombom I, Trentham-Dietz A, Hampton JM, McElroy JA, Newcomb PA, et al. Socioeconomic risk factors for breast cancer: distinguishing individual- and community-level effects. Epidemiology. 2004;15:442–50. doi: 10.1097/01.ede.0000129512.61698.03. [DOI] [PubMed] [Google Scholar]
- 16.Torio CM, Klassen AC, Curriero FC, Caballero B, Helzlsouer K. The modifying effect of social class on the relationship between body mass index and breast cancer incidence. Am J Public Health. 2010;100:146–51. doi: 10.2105/AJPH.2007.126979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Webster TF, Hoffman K, Weinberg J, Vieira V, Aschengrau A. Community- and individual-level socioeconomic status and breast cancer risk: multilevel modeling on Cape Cod, Massachusetts. Environ Health Perspect. 2008;116:1125–9. doi: 10.1289/ehp.10818. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Robert SA, Reither EN. A multilevel analysis of race, community disadvantage, and body mass index among adults in the US. Soc Sci Med. 2004;59:2421–34. doi: 10.1016/j.socscimed.2004.03.034. [DOI] [PubMed] [Google Scholar]
- 19.Gomez SL, Glaser SL, McClure LA, Shema SJ, Kealey M, Keegan TH, et al. The California Neighborhoods Data System: a new resource for examining the impact of neighborhood characteristics on cancer incidence and outcomes in populations. Cancer Causes Control. 2011;22:631–47. doi: 10.1007/s10552-011-9736-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.John EM, Phipps AI, Davis A, Koo J. Migration history, acculturation, and breast cancer risk in Hispanic women. Cancer Epidemiol Biomarkers Prev. 2005;14:2905–13. doi: 10.1158/1055-9965.EPI-05-0483. [DOI] [PubMed] [Google Scholar]
- 21.John EM, Hopper JL, Beck JC, Knight JA, Neuhausen SL, Senie RT, et al. The Breast Cancer Family Registry: an infrastructure for cooperative multinational, interdisciplinary and translational studies of the genetic epidemiology of breast cancer. Breast Cancer Res. 2004;6:R375–89. doi: 10.1186/bcr801. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.John EM, Miron A, Gong G, Phipps AI, Felberg A, Li FP, et al. Prevalence of pathogenic BRCA1 mutation carriers in 5 US racial/ethnic groups. JAMA. 2007;298:2869–76. doi: 10.1001/jama.298.24.2869. [DOI] [PubMed] [Google Scholar]
- 23.Keegan TH, Shariff-Marco S, Sangaramoorthy M, Koo J, Hertz A, Schupp CW, et al. Neighborhood influences on recreational physical activity and survival after breast cancer. Cancer Causes Control. 2014;25:1295–308. doi: 10.1007/s10552-014-0431-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Shariff-Marco S, Yang J, John EM, Sangaramoorthy M, Hertz A, Koo J, et al. Impact of neighborhood and individual socioeconomic status on survival after breast cancer varies by race/ethnicity: the Neighborhood and Breast Cancer Study. Cancer Epidemiol Biomarkers Prev. 2014;23:793–811. doi: 10.1158/1055-9965.EPI-13-0924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Liu L, Deapen D, Bernstein L. Socioeconomic status and cancers of the female breast and reproductive organs: a comparison across racial/ethnic populations in Los Angeles County, California (United States) Cancer Causes Control. 1998;9:369–80. doi: 10.1023/a:1008811432436. [DOI] [PubMed] [Google Scholar]
- 26.Yost K, Perkins C, Cohen R, Morris C, Wright W. Socioeconomic status and breast cancer incidence in California for different race/ethnic groups. Cancer Causes Control. 2001;12:703–11. doi: 10.1023/a:1011240019516. [DOI] [PubMed] [Google Scholar]
- 27.Walls & Associates. National Establishment Time-Series (NETS) Database, 2009. Oakland, CA: 2008. [Google Scholar]
- 28.California Department of Food and Agriculture, editor. California Department of Food and Agriculture. California Certified Farmers’ Market Database. 2010. [Google Scholar]
- 29.NavTeq, editor. NavTeq. NAVSTREETS Street Data Reference Manual v3.7. Jul 1, 2010. 2010. [Google Scholar]
- 30.California Center for Public Health Advocacy P, and the UCLA Center for Health Policy Research. The Link Between Local Food Environments and Obesity and Diabetes. Regents of the University of California, PolicyLink, and the California Center for Public Health Advocacy. Designed for Disease. 2008 [Google Scholar]
- 31.Berrigan D, Pickle LW, Dill J. Associations between street connectivity and active transportation. Int J Health Geogr. 2010;9:20. doi: 10.1186/1476-072X-9-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Reynolds P, Hurley SE, Quach AT, Rosen H, Von Behren J, Hertz A, et al. Regional variations in breast cancer incidence among California women, 1988–1997. Cancer Causes Control. 2005;16:139–50. doi: 10.1007/s10552-004-2616-5. [DOI] [PubMed] [Google Scholar]
- 33.Rauscher GH, Campbell RT, Wiley EL, Hoskins K, Stolley MR, Warnecke RB. Mediation of Racial and Ethnic Disparities in Estrogen/Progesterone Receptor-Negative Breast Cancer by Socioeconomic Position and Reproductive Factors. Am J Epidemiol. 2016;183:884–93. doi: 10.1093/aje/kwv226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Vona-Davis L, Rose DP. The influence of socioeconomic disparities on breast cancer tumor biology and prognosis: a review. J Womens Health (Larchmt) 2009;18:883–93. doi: 10.1089/jwh.2008.1127. [DOI] [PubMed] [Google Scholar]
- 35.Hvidtfeldt UA, Lange T, Andersen I, Diderichsen F, Keiding N, Prescott E, et al. Educational differences in postmenopausal breast cancer–quantifying indirect effects through health behaviors, body mass index and reproductive patterns. PLoS One. 2013;8:e78690. doi: 10.1371/journal.pone.0078690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Menvielle G, Kunst AE, van Gils CH, Peeters PH, Boshuizen H, Overvad K, et al. The contribution of risk factors to the higher incidence of invasive and in situ breast cancers in women with higher levels of education in the European prospective investigation into cancer and nutrition. Am J Epidemiol. 2011;173:26–37. doi: 10.1093/aje/kwq319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Hines LM, Risendal B, Slattery ML, Baumgartner KB, Giuliano AR, Sweeney C, et al. Comparative analysis of breast cancer risk factors among Hispanic and non-Hispanic white women. Cancer. 2010;116:3215–23. doi: 10.1002/cncr.25154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Keegan TH, John EM, Fish KM, Alfaro-Velcamp T, Clarke CA, Gomez SL. Breast cancer incidence patterns among California Hispanic women: differences by nativity and residence in an enclave. Cancer Epidemiol Biomarkers Prev. 2010;19:1208–18. doi: 10.1158/1055-9965.EPI-10-0021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Grieco EM, Acosta YD, de la Cruz GP, Gambino C, Gryn T, Larsen LJ, et al. The Foreign-Born Population in the United States: 2010. Washington, DC: 2012. May, [Google Scholar]
- 40.Kochhar R. The Occupational Status and Mobility of Hispanics. 2005 Dec;:15. 2005. [Google Scholar]
- 41.Braveman PA, Cubbin C, Egerter S, Chideya S, Marchi KS, Metzler M, et al. Socioeconomic status in health research: one size does not fit all. JAMA. 2005;294:2879–88. doi: 10.1001/jama.294.22.2879. [DOI] [PubMed] [Google Scholar]
- 42.Pollack CE, Cubbin C, Sania A, Hayward M, Vallone D, Flaherty B, et al. Do wealth disparities contribute to health disparities within racial/ethnic groups? J Epidemiol Community Health. 2013;67:439–45. doi: 10.1136/jech-2012-200999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Galea S, Tracy M, Hoggatt KJ, Dimaggio C, Karpati A. Estimated deaths attributable to social factors in the United States. Am J Public Health. 2011;101:1456–65. doi: 10.2105/AJPH.2010.300086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Pickett KE, Pearl M. Multilevel analyses of neighbourhood socioeconomic context and health outcomes: a critical review. J Epidemiol Community Health. 2001;55:111–22. doi: 10.1136/jech.55.2.111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Gomez SL, Shariff-Marco S, DeRouen M, Keegan TH, Yen IH, Mujahid M, et al. The impact of neighborhood social and built environment factors across the cancer continuum: Current research, methodological considerations, and future directions. Cancer. 2015;121:2314–30. doi: 10.1002/cncr.29345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Diez Roux AV, Mair C. Neighborhoods and health. Ann N Y Acad Sci. 2010;1186:125–45. doi: 10.1111/j.1749-6632.2009.05333.x. [DOI] [PubMed] [Google Scholar]
- 47.Williams DR, Mohammed SA, Shields AE. Understanding and effectively addressing breast cancer in African American women: Unpacking the social context. Cancer. 2016;122:2138–49. doi: 10.1002/cncr.29935. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Pudrovska T, Anikputa B. The role of early-life socioeconomic status in breast cancer incidence and mortality: unraveling life course mechanisms. J Aging Health. 2012;24:323–44. doi: 10.1177/0898264311422744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Sandvei MS, Lagiou P, Romundstad PR, Trichopoulos D, Vatten LJ. Size at birth and risk of breast cancer: update from a prospective population-based study. Eur J Epidemiol. 2015;30:485–92. doi: 10.1007/s10654-015-0045-2. [DOI] [PubMed] [Google Scholar]
- 50.Mahabir S. Association between diet during preadolescence and adolescence and risk for breast cancer during adulthood. J Adolesc Health. 2013;52:S30–5. doi: 10.1016/j.jadohealth.2012.08.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Colditz GA, Frazier AL. Models of breast cancer show that risk is set by events of early life: prevention efforts must shift focus. Cancer Epidemiol Biomarkers Prev. 1995;4:567–71. [PubMed] [Google Scholar]
- 52.Hurley SE, Reynolds P, Goldberg DE, Hertz A, Anton-Culver H, Bernstein L, et al. Residential mobility in the California Teachers Study: implications for geographic differences in disease rates. Soc Sci Med. 2005;60:1547–55. doi: 10.1016/j.socscimed.2004.07.018. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.