

Abstract
A review appropriateness of the current definition of blindness under National Programme for Control of Blindness (NPCB), Government of India. Online search of peer-reviewed scientific published literature and guidelines using PubMed, the World Health Organization (WHO) IRIS, and Google Scholar with keywords, namely blindness and visual impairment, along with offline examination of reports of national and international organizations, as well as their cross-references was done until December 2016, to identify relevant documents on the definition of blindness. The evidence for the historical and currently adopted definition of blindness under the NPCB, the WHO, and other countries was reviewed. Differences in the NPCB and WHO definitions were analyzed to assess the impact on the epidemiological status of blindness and visual impairment in India. The differences in the criteria for blindness under the NPCB and the WHO definitions cause an overestimation of the prevalence of blindness in India. These variations are also associated with an over-representation of refractive errors as a cause of blindness and an under-representation of other causes under the NPCB definition. The targets for achieving elimination of blindness also become much more difficult to achieve under the NPCB definition. Ignoring differences in definitions when comparing the global and Indian prevalence of blindness will cause erroneous interpretations. We recommend that the appropriate modifications should be made in the NPCB definition of blindness to make it consistent with the WHO definition.
Key words: Blindness, definition, National Programme for Control of Blindness, visual impairment, World Health Organization
The definitions of blindness have evolved over the years internationally and in India. The definition of blindness under the National Programme for Control of Blindness (NPCB), Government of India is different from the current definition adopted by the World Health Organization (WHO) in the International Classification of Diseases-10 (ICD-10). With the adoption of the Sustainable Development Goals and the growing recognition that health systems must strive to provide every individual the highest possible levels of healthy functioning around the world, there is a need to measure and classify visual impairments (VIs) and other aspects of health in a uniform fashion across all populations. Universality of classification has also been recognized as a fundamental underlying principal in the International Classification of Functioning, Disability and Health.[1] While the existing differences in definitions are likely to be known among the public health community, the same may not hold true when it comes to policy makers, and these important differences may get overlooked in discussions. Standardizing the measurement and classification of VI and blindness is essential for meaningful comparisons of the burden of blindness across countries.
In the current paper, we review the current definition of blindness in India as well as WHO and discus its implications and the impact on epidemiological prevalence of blindness and VI in our country. We performed online search of peer-reviewed scientific published literature, and guidelines using PubMed, WHO IRIS, and Google Scholar with keywords blindness and visual impairment. Review of published reports of NPCB and other national and international organizations, as well as their cross-references, was done until December 2016, to identify relevant documents on the definition of blindness.
Definition of Blindness
Traditionally, the definitions of blindness have fallen into two categories: functional definitions based on disability and definitions based on the measurement and quantification of VI (visual acuity [VA] and visual field).[2] In 1948, the WHO Expert Committee on Health Statistics endorsed two definitions of blindness. The measurement-based definition was a central VA of 20/200 or worse with the best correcting lens or a field defect, in which the field has contracted to such an extent that the widest diameter of visual field subtends an angular distance no more than 20°. The disability-based functional definition alluded to “economic blindness” which meant the inability to do any kind of work, industrial or otherwise, for which sight is essential. Both of these definitions were included in the first Manual of the International Statistical Classification of Diseases, Injuries, and Causes of Death.[3] The World Assembly of the World Council for the Welfare of the Blind adopted a functional definition of blindness in 1954.[4] Definitions of blindness used to vary from country to country, and in 1966, more than 65 definitions were being used across the world.[5] The definitions utilized common terminologies such as total blindness, economic blindness, and social blindness. Uncommonly, some countries followed terminologies of professional blindness, educational blindness, practical blindness, partially sighted, and legal blindness. Despite similar terminologies, the criterion used were highly varied. Economic blindness was impairment based in certain countries (Nigeria, Argentina, and Turkey) and disability based in others (Ghana, Somalia, and Panama) or could a combination of both (Mexico, Kuwait, Malaysia, and Singapore). A person could be classified as economic blind in one country but social blind in another.[4] In Canada, the definition is impairment based, i.e., best-corrected VA of ≤20/200 in the better eye or visual field of or less in any meridian.[2] Individuals who need welfare and legal protective measures have been classified as “legally blind” based on set impairment criterion (VA 20/200 or less in better eye with correction) in the United States under the Revenue Act of 1944. Social blindness refers to a degree of visual disability that hampers an individual from socially interacting with family and peer groups in a satisfactory manner and may be associated with serious impediment in education, personality, and development.[6] In the United Kingdom, a person can be certified as severely sight impaired if he/she is “so blind as to be unable to perform any work for which eyesight is essential.”[7]
Evolution of the World Health Organization Definition of Blindness
For the first time, an international standard definition of blindness was developed and included in the ICD-9 in 1975 [Table 1]. Under this classification, best-corrected VA in the better eye was used to classify VI in five categories: Categories 1 and 2 implying low vision and Categories 3–5 implying blindness. The criteria for blindness were best-corrected VA less than 20/400 in the better eye or visual field <10° around a central fixation. The purpose was to facilitate the collection of international statistical data on VI and blindness in a uniform manner that may be compared at a global level. Countries were advised to define blindness as per their own social and economic conditions but to report internationally as per the ICD-9 categories.[8,9] This classification system was retained in the ICD-10 although the final diagnoses' codes underwent a revamp as per the ICD-10 conventions. After the 2002 resolution adopted by the International Council of Ophthalmology on revision of ICD-10, the WHO formed a consultation group that recommended significant modifications to the classification.[10,11] These changes were ratified for inclusion as a revision in ICD-10, in October 2006.[12] It was recommended that VA should be measured with both eyes open with presenting correction if any. The cutoff level for defining blindness was retained, and patients with VA of less than 20/400 or a visual field of no more than 10° in a radius around the central point of fixation in the better eye were placed under blindness Category 3. Under this revision, the term “low vision” was replaced by two categories (1 and 2) of VI. Category 1 referred to the presenting VI <20/70–20/200 in the better eye (moderate VI) and Category 2 referred to the presenting VI <20/200–20/400 in the better eye (severe VI).[12] This is the current internationally accepted definition on blindness.
Table 1.
Categories of Visual impairment based on visual acuity criteria under World Health Organization International Classification of Disease (ICD) 9th revision and ICD-10 (2006 revision) and National Program for Control of Blindness (NPCB), India
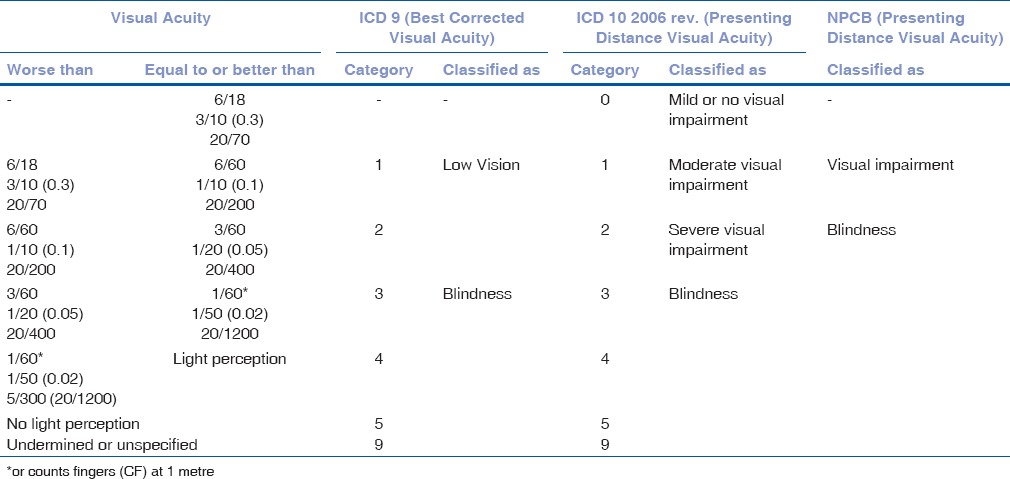
One of the major drivers for this change was a growing recognition that the use of “best-corrected” vision excluded a large proportion of people with VI and blindness due to uncorrected refractive errors and led to an underestimation of global burden of blindness and VI.[13,14,15,16,17] The earlier statistics on global blindness did not include refractive errors as a cause of blindness.[18] Interventions for elimination of avoidable blindness due to uncorrected refractive errors had been recognized in the Vision 2020: The right to sight initiative at its launch in 1999, but now, these interventions were accorded an even higher priority.[19,20]
Definition of Blindness under National Programme for Control of Blindness
“Total Blindness” was the term used in India in 1970 which referred to persons having no perception of light.[4] The multicentric survey of blindness in seven centers by the Indian Council of Medical Research in 1971–1974 reported the prevalence of “Total Blindness” (VA less than 20/400 in better eye with spectacle correction), “Economic Blindness” (VA less than 20/200 in the better eye with spectacle correction), and “One Eye Blindness” (VA less than 20/400 in one eye and better than 20/200 in the other eye with spectacle correction).[21] The document of the “National Plan for Prevention of Visual Impairment and Control of Blindness” launched in 1976 does not include any definition of blindness. A Central Coordination Committee gave the definition of blindness as (a) vision of 20/200 or less with best possible spectacle correction, (b) diminution of field of vision to 20° or less in the better eye, or (c) one eye has vision of 20/200 or less with best possible spectacle correction and the other eye has visual field of 20° or less.[22] The term “Manifest Blindness” has also been used in India for individuals having VA of less than 20/1200 in the better eye. The current definition of blindness adopted under the NPCB is presenting distance VA less than 20/200 in the better eye. A limitation of field of vision to under 20° from central point of fixation in the better eye is also considered blindness.[6]
Implications of the Current Definition of Blindness under National Programme for Control of Blindness
The NPCB definition is based on presenting VA instead of best-corrected VA. Presenting vision refers to the acuity obtained after the use of available refractive error correction, and if no refractive correction is being used, then VA is measured as such. After the 2006 revision, the ICD-10 definition is also based on the presenting vision, and the two definitions are consistent in this regard. The VA criteria under which an individual will be classified as blind in the two definitions are different, being 20/200 in the NPCB definition and 20/400 in the ICD-10 definition after the 2006 revision.
Given the stated differences in the NPCB and the WHO ICD-10 definition of blindness, comparing the prevalence of blindness while ignoring the underlying criterion may lead to misinterpretation of data. The prevalence of blindness with NPCB definition is represented much higher when compared to the prevalence in other countries that use the WHO definition of blindness. On the other hand, since the severe VI (presenting VA less than 20/200 to 20/400 in the better eye) is included as a component of blindness in NPCB definition, the prevalence of VI, per se, is lower in India with NPCB definition. The WHO has estimated nearly 8 million blind and another 54 million visually impaired in India.[23] For the same period, the estimates are 12 million blind and 50 million visually impaired in India using the NPCB definition.[24] The difference in terms of blindness in the two estimates is around 4 million people or 50% extra blind individuals, who correspond to the category of severe VI in the WHO definition, but are assessed as blind as per the NPCB definition. This difference in definition affects the prevalence of blindness in Indian population significantly and results in huge gaps in the magnitude of blindness and VI when compared to other countries. The blindness prevalence in India as per the WHO and NPCB definitions is 0.67% and 1.0%, respectively. This gap in prevalence is so significant that it may be comparable to the prevalence in undeveloped countries versus a developing country with emerging economy and a high-performing blindness control program. India has nearly 20% of the global blind population using the WHO definition, but it may be wrongly interpreted as 30% when a number of blind people are taken as per the NPCB definition, and the denominator is taken as per the global estimates by the WHO. The NPCB is one of the successful programs of the country meeting the various program output targets set under the various 5-year plans consistently, and more than 6 million cataract surgeries are performed per year in India.[25] In spite of such achievements, the magnitude of blindness in India appears to be high as the NPCB definition uses a lower threshold of VI to classify blindness. If NPCB continues with the same definition, the prevalence data will invariably be misinterpreted for both blindness as well as VI in the country.
The differences in definition of blindness not only affect the magnitude but also have an effect on the proportion of causes of blindness and VI. Uncorrected refractive errors are estimated to be the most common cause of VI globally. In the Indian definition, severe VI component is included in the definition of blindness, and therefore, the proportion of uncorrected refractive error is overrepresented as a cause of blindness in India. Due to this distinction, other causes of blindness such as glaucoma, corneal morbidity, and posterior segment diseases are underrepresented. The proportion of blindness due to uncorrected refractive error in the National Survey 2001 was estimated as 19.7%.[26] The proportion of blindness due to uncorrected refractive error was a quarter lower at 15% when blindness was assessed using the cutoff of 20/400. The proportion of glaucoma blindness was 5.9% and 8.0% for NPCB and WHO cutoffs, respectively.[27]
The NPCB definition of using presenting vision instead of best-corrected vision has resulted in availability of the data on importance of uncorrected refractive errors in causing blindness and VI. It was estimated that the best-corrected VA was associated with a gross underestimation of total burden of VI by about 38%.[28] Recognition of this issue based on studies from India was one of the important reasons that prompted the WHO to constitute its expert group and eventually the definition from best-corrected VA to presenting VA.
The Vision 2020 – right to sight initiatives recommends reducing the prevalence of blindness to 0.3% by the year 2020 to achieve the elimination of avoidable blindness.[29] The same goal has been kept under the NPCB without even realizing that the goals are as per the WHO definition of blindness.[30] We may be able to achieve the goals using WHO definition, but it may be extremely difficult if we keep the same goal as per NPCB definition of blindness since we will be addressing an extra 4 million individuals blind due to refractive errors as per the current NPCB definition. There remains no doubt that these individuals need to be targeted in our control efforts, but it should be from the point of view of reducing refractive error associated VI.
In the authors' personal discussions with various community eye health practitioners on this topic, continuing with the current definition of blindness by NPCB has been justified, as the higher magnitude of blindness (due to a skewed definition of blindness) is helpful in advocacy to motivate international agencies as well as government policymakers to provide more funds for the program. Here, it is important to reiterate that instead of giving wrong impressions to such agencies, the program should shift targets to visual impairment along with the blindness.
As recommended under the WHO-Global Action Plan 2014–2019 on Universal Eye Health, the aim should be to reduce avoidable VI as a global public health problem through international partners, improved coordination, and efficient monitoring with a focus on innovative approach in the prevention and treatment of eye diseases.[31] As per this action plan, the target is to reduce the prevalence of avoidable VI by 25% by 2019 from the baseline that was established by the WHO in 2010. To strengthen these initiatives, it is suggested that the name of the national program should be revised to “National Programme for Prevention of Visual Impairment and Control of Blindness.” The same was recommended nearly 50 years ago by Prof. L.P. Agarwal, who had a major role in initiating the NPCB in India.[32] This will help in program support to a target population of nearly 40 million (3.2%) visually impaired individuals as compared to 8 million when the program is focused only for the blind population. We need to evolve and keep pace with changing trends and current standard guidelines that are accepted globally.
In India, the Ministry of Social Justice and Empowerment (MoSJE) in India is responsible for developing programs to support persons with disabilities including VI. In a recent initiative, this ministry has constituted a committee to revise the definition of blindness and low vision for certification of blind and visually impaired. The committee has recommended for revision of the blindness cutoff to 20/400 instead of 20/200 which is currently being followed by NPCB, India. The only difference, here, is that the MoSJE classification will be applied to a person based on best-corrected VA and not presenting VA. It is essential that the same cutoff figure is used universally under all the programs associated with policy making and service provision for the blind and visually impaired.
Conclusion
Magnitude of blindness and the relative contribution of various causes have a direct effect on advocacy, allocation of resources, policymaking, and program planning. Universality in the definition of blindness across various regions of the world is a prerequisite for facilitating the collection of population-based data on the prevalence of vision impairment and blindness in a uniform and comparable manner and estimating the global burden of blindness. With the reasons outlined above, it is the opinion of the authors that there is a strong case for revision of the definition of blindness under NPCB to make it consistent with the definition recommended by the WHO. The proposed revision of definitions by the NPCB will majorly affect the policymaking related to blindness control activities without having any undue impact on disability benefits available to patients with VI.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.World Health Organization. Towards a Common Language for Functioning, Disability and Health: ICF. Geneva: WHO; 2002. [Google Scholar]
- 2.Leat SJ, Legge GE, Bullimore MA. What is low vision? A re-evaluation of definitions. Optom Vis Sci. 1999;76:198–211. doi: 10.1097/00006324-199904000-00023. [DOI] [PubMed] [Google Scholar]
- 3.World Health Organization. Expert Committee on Health Statistics. Third Report of a Meeting Held in Geneva from 21 to 26 November 1951. WHO. 1952. [Last cited on 2017 Jan 18]. Available from: http://www.who.int/iris/handle/10665/40190 .
- 4.Prevention of Blindness: Report by the Director-General. Geneva: WHO; 1972. World Health Assembly 25. [Google Scholar]
- 5.Sorsby A. Blindness in the world today. WHO Chron. 1967;21:369–73. [PubMed] [Google Scholar]
- 6.Murthy GV, Gupta SK, Bachani D. The Principles and Practice of Community Ophthalmology. New Delhi: National Program for Control of Blindness, Government of India; 2002. [Google Scholar]
- 7.Department of Health. Certificate of Vision Impairment: Explanatory Notes for Consultant Ophthalmologists and Hospital Eye Clinic Staff. United Kingdom. 2013. [Last cited on 2017 Jan 19]. Available from: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/213286/CVI-Explanatory-notes-in-DH-template.pdf .
- 8.World Health Organization. The Prevention of Blindness: Report of a WHO Study Group. Geneva: WHO; 1973. [PubMed] [Google Scholar]
- 9.World Health Organization. International Classification of Diseases. 9th Revision. Geneva: WHO; 1975. [Google Scholar]
- 10.Aspects and Ranges of Vision Loss with Emphasis on Population Surveys. Sydney: ICO; 2002. International Council of Ophthalmology. [Google Scholar]
- 11.Consultation on development of standards for characterization of vision loss and visual functioning: Geneva, 4-5 September 2003. Geneva: WHO; 2003. WHO Programme for the Prevention of Blindness and Deafness. [Google Scholar]
- 12.World Health Organization. List of Official ICD-10 Updates Ratified October 2006. Geneva: WHO; 2006. [Last cited on 2016 Apr 07]. Available from: http://www.who.int/classifications/icd/2006Updates.pdf . [Google Scholar]
- 13.Dandona L, Dandona R. What is the global burden of visual impairment? BMC Med. 2006;4:6. doi: 10.1186/1741-7015-4-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Dandona L, Dandona R. Estimation of global visual impairment due to uncorrected refractive error. Bull World Health Organ. 2008:86. doi: 10.2471/BLT.08.053652. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Naidoo KS, Leasher J, Bourne RR, Flaxman SR, Jonas JB, Keeffe J, et al. Global vision impairment and blindness due to uncorrected refractive error, 1990-2010. Optom Vis Sci. 2016;93:227–34. doi: 10.1097/OPX.0000000000000796. [DOI] [PubMed] [Google Scholar]
- 16.Dandona R, Dandona L. Refractive error blindness. Bull World Health Organ. 2001;79:237–43. [PMC free article] [PubMed] [Google Scholar]
- 17.Fotouhi A, Hashemi H, Mohammad K, Jalali KH. Tehran Eye Study. The prevalence and causes of visual impairment in Tehran: The Tehran Eye Study. Br J Ophthalmol. 2004;88:740–5. doi: 10.1136/bjo.2003.031153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Resnikoff S, Pascolini D, Etya'ale D, Kocur I, Pararajasegaram R, Pokharel GP, et al. Global data on visual impairment in the year 2002. Bull World Health Organ. 2004;82:844–51. [PMC free article] [PubMed] [Google Scholar]
- 19.Global Initiative for the Elimination of Avoidable Blindness. Geneva: WHO; 2000. World Health Organization Programme for the Prevention of Blindness and Deafness. [Google Scholar]
- 20.World Health Organization. Global Initiative for the Elimination of Avoidable Blindness: Action Plan 2006-2011. Geneva: WHO; 2007. [Google Scholar]
- 21.Ophthalmic research in ICMR. New Delhi: ICMR; [Last cited on 2016 Nov 01]. Indian Council for Medical Research. Available from: http://www.icmr.nic.in/oph-icmr.pdf . [Google Scholar]
- 22.Present status of National Programme for Control of Blindness 1992. New Delhi: Ministry of Health and Family Welfare, Government of India; 1992. Ophthalmology Section, Directorate General of Health Services. [Google Scholar]
- 23.Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. Br J Ophthalmol. 2012;96:614–8. doi: 10.1136/bjophthalmol-2011-300539. [DOI] [PubMed] [Google Scholar]
- 24.Neena J, Rachel J, Praveen V, Murthy GV. Rapid Assessment of Avoidable Blindness India Study Group. Rapid assessment of avoidable blindness in India. PLoS One. 2008;3:e2867. doi: 10.1371/journal.pone.0002867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.National Programme for Control of Blindness. Statistics. NPCB. [Last cited on 2017 Jan 19]. Available from: http://www.npcb.nic.in/index1.asp?linkid=93&langid=1 .
- 26.Murthy GV, Gupta SK, Bachani D, Jose R, John N. Current estimates of blindness in India. Br J Ophthalmol. 2005;89:257–60. doi: 10.1136/bjo.2004.056937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.National Survey on Blindness and Visual Outcomes after Cataract Surgery (2001-2002) AIIMS: New Delhi; 2002. [Last cited on 2016 Nov 01]. National Program for Control of Blindness, India. Available from: http://www.aiims.edu/images/depart/RPC/reports%20for%20web/1.%20NPCB%20National%20Blindness%20Survey%202001-02.pdf . [Google Scholar]
- 28.Dandona L, Dandona R. Revision of visual impairment definitions in the international statistical classification of diseases. BMC Med. 2006;4:7. doi: 10.1186/1741-7015-4-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.VISION 2020: The Right to Sight. [Last cited on 2017 Jan 19]. Available from: http://www.iapb.org/vision-2020/
- 30.National Programme for Control of Blindness, Government of India. [Last cited on 2015 Aug 02]. Available from: http://www.npcb.nic.in/
- 31.World Health Organization. Universal Eye Health: A Global Action Plan 2014-2019. Geneva: WHO; 2013. [Google Scholar]
- 32.Agarwal LP. National programme for prevention of visual impairment and control of blindness. Indian J Ophthalmol. 1978;25:1–5. [PubMed] [Google Scholar]