

Abstract
Background:
The injury of the triangular fibrocartilage complex (TFCC) is a common cause of ulnar-sided wrist pain. The aim of this study was to investigate if the high-resolution 3T magnetic resonance imaging (MRI) could demonstrate the detailed complex anatomy of TFCC in Chinese.
Methods:
Fourteen Chinese cadaveric wrists (from four men and three women; age range at death from 30 to 60 years; mean age at 46 years) and forty healthy Chinese wrists (from 20 healthy volunteers, male/female: 10/10; age range from 21 to 53 years with a mean age of 32 years) in Beijing Jishuitan Hospital from March 2014 to March 2016 were included in this study. All cadavers and volunteers had magnetic resonance (MR) examination of the wrist with coronal T1-weighted and proton density-weighted imaging with fat suppression in three planes, respectively. MR arthrography (MRAr) was performed on one of the cadaveric wrists. Subsequently, all 14 cadaveric wrists were sliced into 2 mm thick slab with band saw (six in coronal plane, four in sagittal plane, and four in axial plane). The MRI features of normal TFCC were analyzed in these specimens and forty healthy wrists.
Results:
Triangular fibrocartilage, the ulnar collateral ligament, and the meniscal homolog could be best observed on images in coronal plane. The palmar and dorsal radioulnar ligaments were best evaluated in transverse plane. The ulnotriquetral and ulnolunate ligaments were best visualized in sagittal plane. The latter two structures and the volar and dorsal capsules were better demonstrated on MRAr.
Conclusion:
High-resolution 3T MRI is capable to show the detailed complex anatomy of the TFCC and can provide valuable information for the clinical diagnosis in Chinese.
Keywords: Anatomy, Magnetic Resonance Imaging, Triangular Fibrocartilage Complex, Wrist
Introduction
Triangular fibrocartilage complex (TFCC) is composed of multiple distinct anatomic structures including the triangular fibrocartilage (TFC, the articular disk), meniscal homolog (MH), dorsal and volar distal radioulnar ligaments, the extensor carpi ulnaris tendon (ECU), ulnar collateral ligament (UCL), ulnotriquetral (UT) ligament, and the ulnolunate (UL) ligament.[1,2] The TFCC is the main stabilizer of the ulnar-sided wrist and the distal radioulnar joint (DRUJ). It is of significance in biomechanics and can dissolve and absorb the force between the ulna and ulnar side of the wrist. It helps to maintain the stability of the ulnocarpal joint and allows the stable motion of the wrist and the rotation of the forearm.[3,4,5,6,7,8,9,10]
Injury on structural components of the TFCC may cause ulnar-sided wrist pain and may lead to wrist instability. Due to the anatomic complexity of TFCC, it remains a challenge for radiologists to make an accurate imaging diagnosis.[11] Therefore, some injuries may be missed or misdiagnosed, especially in the early stage, resulting in delayed diagnosis and treatment, delayed functional recovery, and reduced quality of life. The early accurate diagnosis of the injuries is critical for choosing the appropriate treatment protocols.[12,13] Magnetic resonance imaging (MRI), a noninvasive method, can yield a high-resolution image of soft tissue and visualize the detailed anatomic structures of TFCC. Several studies have shown that MRI, especially high-resolution 3T MRI is the preferred imaging modality in the diagnosis of TFCC injuries.[14,15,16,17,18,19] Magnetic resonance (MR) examination can help select the right treatment for patients with TFCC injuries who complain ulnar-sided pain and can prevent further damages on patients’ wrists.[20]
This research was designed to outline the detailed anatomy and corresponding imaging appearance on the high-resolution 3T MRI of the normal TFCC using cadaveric specimens and healthy volunteers. We aimed to investigate if the high-resolution 3T MRI could demonstrate the detailed complex anatomy of TFCC in Chinese.
Methods
The study was adhered to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of Beijing Jishuitan Hospital. Written informed consent was obtained from all participants in this study.
Cadavers and subjects
Fourteen Chinese cadaveric wrists were provided by the Institute of Basic Sciences, Chinese Academy of Medical Sciences. There were four men and three women with age range between 30 and 60 years at death and mean age of 46 years old. All specimens contain distal part of radius and ulna, entire wrist and hand, which were kept at −42°C (Haier BioMedical, DW-40W100, Qingdao, China) for the following experiments. All specimens were thaw at room temperature for 24 h before MRI was taken. Radiographs on posteroanterior and lateral projections were taken before MRI to exclude any osseous abnormalities on all the specimens.
The normal MRI features of TFCC were analyzed on forty wrists (from twenty healthy Chinese volunteers, ten men and ten women; age range from 21 to 53 years with a mean age of 32 years) without a history of wrist injuries in Beijing Jishuitan Hospital from March 2014 to March 2016. The including standards of the healthy volunteers were as following: no history of traumatic injury on the wrist, no osteoarthritis of the radiocarpal joint, free of wrist pain, and with a normal range of motion in wrist.
Magnetic resonance imaging
MR examination was performed with a 3T MRI Unit (5680 DA Best, Philips Medical Systems, Netherlands) using a 16-channel hand-and-wrist receiver-only coil (Philips Hand/Wrist 16 3T Tim coil). The healthy volunteers were placed in prone position with the examined arms raised above the head, and the wrists were in neutral position in the center of the bore pinpointed by the laser mark. The cadaveric wrists were placed in the same way.
All cadaver specimens and wrists of volunteers underwent MRI with the following sequences: fat suppression proton density-weighted imaging (PD-FS) in axial, coronal, and sagittal planes (repetition time/echo time [TR/TE]: 2347–3657 ms/40–45 ms) and T1-weighted fast spin-echo in coronal plane (TR/TE: 521–780 ms/20–40 ms); section thickness: 2 mm; interslice space: 0.2 mm; number of excitations: 2–4; field of view: 100–120 mm; and voxel: 0.15–0.25 mm × 0.15–0.25 mm × 1.50 mm.
MR arthrography (MRAr) was performed on one of the cadaveric wrists by intra-articular injection of the contrast media (10 ml liquid mixture of 0.5 ml Gd-DTPA [Beijing Beilu Pharmaceutical Co., Ltd., Beijing, China] with 100 ml normal saline + 5 ml iohexol [Beijing Beilu Pharmaceutical Co., Ltd.]) with T1 fat-saturated (T1-FS) imaging in sagittal, coronal, and axial planes (TR/TE: 350 ms/34 ms).
Anatomic specimen preparation
After obtained MR images, all cadaveric specimens were immediately frozen in neutral position at −42°C and were kept at this temperature for at least 24 h. Those specimens were subsequently sliced into 2-mm-thick slices (that corresponded to the section thickness of the MR images) with a Stainless Steel Band Saw (American Meat Equipment Corp, Montebello, USA). Six specimens were sectioned along the coronal plane, four along the sagittal plane, and four along the axial plane. Each slice was digitally photographed (EOS 6D, Canon, Japan), and colored photographs were obtained for the anatomic correlation analysis with the corresponding MR images.
Magnetic resonance imaging: Anatomic comparison and analysis
All MR images were interpreted independently by two musculoskeletal radiologists who had 5–10 years of experience. TFCC of all these cadavers and volunteers was identified on the MR images according to their descriptions in literature. Based on the analysis of the MRI, the two radiologists reached a consensus regarding each structure of TFCC. The appearance of TFCC and signal intensity on MR images in 14 cadaveric specimens were compared with the appearance derived from the inspection of the corresponding colored photographs obtained from anatomic slices. The MR appearance of the normal TFCC in forty healthy wrists was analyzed and confirmed. Identification of each ligament of TFCC on MRI was by identifying the linear hyposignal intensity structure from its origin to its insertion on at least two diagnostic planes.
Results
Anatomy of the triangular fibrocartilage complex
Analysis of the gross specimens confirmed that TFCC was composed of TFC (the articular disk), MH, dorsal and volar distal radioulnar ligaments, ECU, UCL, UT, and UL ligaments [Figures 1-4].
Figure 1.

Schematic diagram of triangular fibrocartilage complex in the right wrist. (a) Coronal illustration; (b) axial illustration demonstrated the anatomy of TFCC; (c) sagittal illustration shows the volar and dorsal capsules (arrow) originated from the volar and dorsal aspect of the TFC and inserted into the volar and dorsal edges of the triquetrum (arrowhead). TFC: Triangular fibrocartilage; MH: Meniscus homolog; UCL: Ulnar collateral ligament; ECU: Extensor carpi ulnaris tendon; UL: Ulnolunate ligament; UT: Ulnotriquetral ligament; LT: Lunotriquetral ligament; ★: Prestyloid recess; △: Ligamentum subcruentum; R: Radius; U: Ulna; L: Lunate; T: Triquetrum; DRUL: Dorsal radioulnar ligament; VRUL: Volar radioulnar ligament.
Figure 4.

Triangular fibrocartilage complex in the right wrist of a 30-year-old cadaver specimen. (a) Sagittal anatomic comparison specimen; (b) sagittal T1-weighted image of the wrist showed the ulnotriquetral ligament and the triangular fibrocartilage; (c) sagittal T1 fat-saturated weighted image with MRAr in the specimen displayed in Figure 2 showed the ulnotriquetral ligament. Besides, there is an artifact in the dorsal side. Arrowhead: Ulnotriquetral ligament; Arrow: Triangular fibrocartilage; MRAr: Magnetic resonance arthrography.
The radial and ulnar sides of the triangular fibrocartilage
The TFC was the central structure of the TFCC. The radial side of the TFC was attached to the articular cartilage at the most distal aspect of the sigmoid notch of the radius. The ulnar side of the TFC inserted onto the ulnar fovea and the ulnar styloid process. The ulnar attachment of the TFC was composed of two distinct laminas, also refer to the triangular ligament [Figures 1 and 2]. The distal lamina was oriented horizontally and lay between the TFC and the styloid process of the ulna. It was also attached to the tip of the ulnar styloid process. The proximal lamina was oriented vertically and curved from the undersurface of the TFC to the ulnar fovea. The two laminas were separated by an intervening layer of fibrovascular tissue, also known as the ligamentum subcruentum [Figures 1 and 2], which was typically triangular in shape and extended into TFC proper from a broad base near the fovea of ulna.
Figure 2.

Triangular fibrocartilage complex (TFCC) in the right wrist of a 60-year-old cadaver specimen. (a) Coronal anatomic comparison specimen; (b) coronal PD-FS weighted image; (c) T1-weighted image of the wrist. Short arrow: The radial and ulnar insertions of TFC; △: Ligamentum subcruentum; Arrowhead: lunotriquetral ligament; ★: Meniscal homolog; Long white arrow: Prestyloid recess; White dotted arrow: Extensor carpi ulnaris; PD-FS: Proton density-weighted imaging with fat suppression.
Meniscal homolog
The MH extended from the ulnar styloid to the dorsal edge of the triquetrum, hamate, and the base of the fifth metacarpal. It was adjacent to the ECU dorsally and was connected to lunotriquetral ligament (which was not the component of TFCC) on the volar side, whereas it was close to the UCL on the lateral side and was connected to the triquetrum through UT ligament. There was a synovial space between the TFC and MH, where fibers from both TFC and MH were attached to the ulnar styloid process, also termed as the prestyloid recess [Figures 1 and 2].
The dorsal and volar distal radioulnar ligaments
The dorsal and volar distal radioulnar ligaments, the main components of dorsal and volar marginal portions of TFC, respectively, extended from dorsal and volar rims of the sigmoid notch to the base of the ulnar styloid process. These two ligaments inserted directly into the distal radius, whereas the central portion of TFC inserted into the hyaline cartilage of the distal radius [Figures 1 and 3]. The main function of these ligaments was to prevent dorsal and volar subluxation of the DRUJ.
Figure 3.

Triangular fibrocartilage complex in the left wrist of a 30-year-old cadaver specimen. (a) Transverse anatomic comparison specimen; (b) transverse PD-FS; (c) T1-weighted image. Arrowhead: The volar and dorsal radioulnar ligaments. Arrow: Triangular fibrocartilage; PD-FS: Proton density-weighted imaging with fat suppression.
The other components of the triangular fibrocartilage complex
The ECU ran along the dorsolateral side of the ulnocarpal joint and inserted at the base of the fifth metacarpal. UCL lay on the surface of the MH and linked to the ECU and the MH closely [Figure 1]. UT, UL, and ulnocapitate ligaments lay on the volar side of the wrist. UT and UL ligaments originated from the volar side of the volar distal radioulnar ligament, while ulnocapitate ligament had a direct bony origin from the fovea of the ulnar head and located more superficial to the junction between the UL and UT ligaments. These three ligaments inserted to the palmar sides of the triquetrum, lunate, and capitate bone, respectively [Figures 1, 2 and 4].
The volar and dorsal capsules
The volar and dorsal capsules were formed by the ulnocarpal ligaments (included UT and UL ligaments) and MH, respectively. They originated from the volar and dorsal aspect of the TFC and inserted into the volar and dorsal edges of the triquetrum [Figure 1].
Magnetic resonance imaging appearance of triangular fibrocartilage complex
On MR images, the normal TFC (the articular disk) showed low signal intensity in all the sequences including T1-weighted image and PD-FS. In coronal MR images, TFC, triangular ligament, MH, ECU, and UCL were all clearly appreciated [Figures 2 and 5]. In some cadavers and volunteers, lunotriquetral ligament, the dorsal distal radioulnar ligament, UT, and UL ligaments could be clearly identified. There were 14 Chinese cadaveric wrists and 30 healthy Chinese wrists could find the part of the ulnocapitate ligament on MR images. The UT, UL, and the ulnocapitate ligaments played an important role in preventing palmar subluxation of the ulnar carpus. All ligaments showed low signal intensity on PD-FS images. The normal TFC had an asymmetrical bowtie-shaped image with low signal intensity on coronal images. The signal intensity of the triangular ligaments was higher than that of the TFC and showed as hypointense or slightly hyperintense striated signal, and the ligamentum subcruentum presented as increased signal intensity on PD-FS images [Figures 2 and 5]. The MH showed as a triangular shape and ran along the lateral joint capsule [Figure 2].
Figure 5.
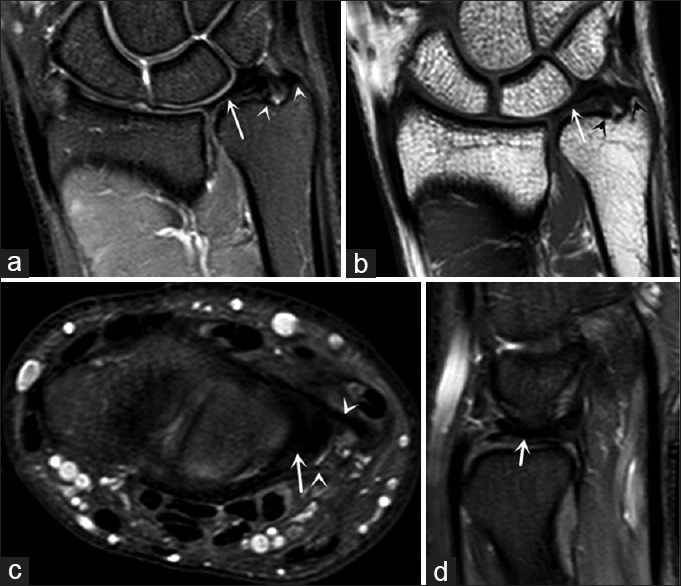
Normal triangular fibrocartilage complex in the right wrist of a 32-year-old healthy male volunteer. (a and b) Coronal PD-FS weighted image and coronal T1-weighted image of the wrist showed the TFCC had two attachments to the ulna, one inserting into the ulnar styloid tip (distal lamina) and the other one inserting into the fovea (proximal lamina) (arrowhead); (c) axial PD-FS weighted image showed the volar and dorsal radioulnar ligament (arrowhead); (d) sagittal image showed the band-like appearance of the TFC. Arrow: Triangular fibrocartilage; PD-FS: Proton density-weighted imaging with fat suppression; TFCC: Triangular fibrocartilage complex; TFC: Triangular fibrocartilage.
On the axial plane, volar and dorsal radioulnar ligaments were well recognized as a band of low signal intensity extending from the distal radius to the distal ulna along the volar and dorsal side of the TFC disk [Figures 3 and 5].
The TFC was biconcave shape in sagittal plane that was thick in the periphery and thin in the central portion [Figure 5]. On the sagittal plane, UT, UL ligaments, volar and dorsal capsules, and part of the ulnocapitate ligament could be well evaluated, which also showed band low signal intensity [Figure 4]. What is more, UT, UL ligaments, and the volar and dorsal capsules could be visualized more clearly on sagittal T1 FS images with MRAr [Figure 4].
Discussion
The TFCC is a fibrocartilage-ligament complex composed of multiple structures and plays an important role in stabilizing the DRUJ, transmitting the load between the carpus and ulna, and stabilizing the ulnar aspect of the wrist.[21] The complexity of the TFCC anatomy makes it difficult to diagnose the TFCC injuries accurately.[11] MRI, as a noninvasive examination, has a high resolution of soft tissue and can show the anatomic details of the TFCC. Therefore, MRI has become the single most important imaging modality for the hand surgeon and orthopedic surgeon in helping them to implement the appropriate treatment plans by revealing the nature, severity, location, and extent of the injuries and the associated injuries.[22,23,24,25,26,27]
MRAr will show some fine anatomy more clearly, improve the diagnosis of the lesion within the joint, and increase the sensitivity and accuracy of diagnosis.[28,29,30] In our study, we carried out the direct MRAr in one specimen, and in the sagittal plane, we could find the UT, UL ligaments, and the volar and dorsal capsules more clearly than conventional MRI.
As we have known, Palmer and Werner[8] first reported that the ulnocarpal ligaments were composed of the UT and UL ligaments. However, some literatures stated that the ulnocarpal ligaments also included the ulnocapitate ligament, and these ligaments were often titled as the ulnocarpal ligamentous complex.[10,31] In our study, we also can find the ulnocapitate ligament on both anatomic sections and MR images in some Chinese volunteers, which was inconsistent with what Theumann et al.[32] had found in their research where the ulnocapitate ligament was not seen on MR images. However, we failed to find the ulnocapitate ligament on MR images in ten wrists of volunteers involved in our study, and the discrepancy might be due to these structures were often confluent and indistinguishable from each other, as the literature stated.[10]
Although there are many descriptions about the complex anatomy of the TFCC, most of them put much emphasis on the coronal or axial view.[33] In our study, we found that the volar and dorsal capsules could be best visualized in sagittal images, especially with MRAr. Furthermore, by combining all three planes to make a comprehensive evaluation, we could find more details of the TFCC such as UT, UL, and the volar and dorsal capsules.
Due to the high sensitivity of MRI, it is easy to misdiagnose the normal variations in signal intensity as injury. Combining with literatures and our research,[34,35] we want to emphasis some common pitfalls about the structures. Ligamentum subcruentum, as a fibrovascular tissue, usually presents as increased signal intensity on PD-FS images and should not be misinterpreted as an injury to the ulnar attachment of the TFC. Prestyloid recess, a synovial space between the TFC and MH, is a normal synovial linked recess, may fill with joint fluid, presented as high signal intensity on PD-FS images, and should not be mistaken for an injury. On the coronal images, the proximal lamina appears as a striated pattern and internally relatively high signal intensity. It is a normal appearance due to bundles of collagen fibers with vascular connective tissue that produce the relative higher signal, may mimic or mask tears, and make it difficult to accurately diagnose the tears of the ulnar attachment.[36] Since the radial side of the TFC is attached to the articular cartilage at sigmoid notch of the distal radius directly, it is a normal finding that there is intermediate signal intensity between the hyposignal intensity TFC and the subchondral bone of the distal radius.
In conclusion, the TFCC is a complex structure, and the high-resolution 3T MRI is capable to demonstrate all the anatomic components. MRAr increases the sensitivity of detecting some of the smaller ligaments such as UT ligament. To evaluate the TFCC, one needs to look at the TFCC in all three planes. Familiar with the normal MR appearance of the normal structures is vital to distinguish normal anatomical structures from injuries.
Financial support and sponsorship
This study was supported by grants from the National Natural Science Foundation of China (No. 81371515), the Beijing Natural Science Foundation of China (No. 7142075), and the Capital Medical Development and Scientific Research Fund of China (No. 2016-2-1122).
Conflicts of interest
There are no conflicts of interest.
Footnotes
Edited by: Ning-Ning Wang
References
- 1.Oneson SR, Scales LM, Timins ME, Erickson SJ, Chamoy L. MR imaging interpretation of the palmer classification of triangular fibrocartilage complex lesions. Radiographics. 1996;16:97–106. doi: 10.1148/radiographics.16.1.97. doi: 10.1148/radiographics.16.1.97. [DOI] [PubMed] [Google Scholar]
- 2.Palmer AK. Triangular fibrocartilage disorders: Injury patterns and treatment. Arthroscopy. 1990;6:125–32. doi: 10.1016/0749-8063(90)90013-4. doi: 10.1016/0749-8063(90)90013-4. [DOI] [PubMed] [Google Scholar]
- 3.Nakamura T, Yabe Y, Horiuchi Y. Functional anatomy of the triangular fibrocartilage complex. J Hand Surg Br. 1996;21:581–6. doi: 10.1016/s0266-7681(96)80135-5. doi: 10.1016/S0266-7681(96)80135-5. [DOI] [PubMed] [Google Scholar]
- 4.Nakamura T, Yabe Y. Histological anatomy of the triangular fibrocartilage complex of the human wrist. Ann Anat. 2000;182:567–72. doi: 10.1016/S0940-9602(00)80106-5. doi: 10.1016/S0940-9602(00)80106-5. [DOI] [PubMed] [Google Scholar]
- 5.Cerezal L, de Dios Berná-Mestre J, Canga A, Llopis E, Rolon A, Martín-Oliva X, et al. MR and CT arthrography of the wrist. Semin Musculoskelet Radiol. 2012;16:27–41. doi: 10.1055/s-0032-1304299. doi: 10.1055/s-0032-1304299. [DOI] [PubMed] [Google Scholar]
- 6.Cerezal L, Abascal F, García-Valtuille R, Del Piñal F. Wrist MR arthrography: How, why, when. Radiol Clin North Am. 2005;43:709–31. doi: 10.1016/j.rcl.2005.02.004. viii. doi: 10.1016/j.rcl.2005.02.004. [DOI] [PubMed] [Google Scholar]
- 7.Ahn AK, Chang D, Plate AM. Triangular fibrocartilage complex tears: A review. Bull NYU Hosp Jt Dis. 2006;64:114–8. [PubMed] [Google Scholar]
- 8.Palmer AK, Werner FW. The triangular fibrocartilage complex of the wrist – Anatomy and function. J Hand Surg Am. 1981;6:153–62. doi: 10.1016/s0363-5023(81)80170-0. doi: 0.1016/S0363-5023(81)80170-0. [DOI] [PubMed] [Google Scholar]
- 9.Linscheid RL. Biomechanics of the distal radioulnar joint. Clin Orthop Relat Res. 1992;275:46–55. doi: 10.1097/00003086-199202000-00008. [PubMed] [Google Scholar]
- 10.von Borstel D, Wang M, Small K, Nozaki T, Yoshioka H. High-resolution 3T MR imaging of the triangular fibrocartilage complex. Magn Reson Med Sci. 2017;16:3–15. doi: 10.2463/mrms.rev.2016-0011. doi: 10.2463/mrms.rev.2016-0011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Yoshioka H, Burns JE. Magnetic resonance imaging of triangular fibrocartilage. J Magn Reson Imaging. 2012;35:764–78. doi: 10.1002/jmri.22840. doi: 10.1002/jmri.22840. [DOI] [PubMed] [Google Scholar]
- 12.Blazar PE, Chan PS, Kneeland JB, Leatherwood D, Bozentka DJ, Kowalchick R. The effect of observer experience on magnetic resonance imaging interpretation and localization of triangular fibrocartilage complex lesions. J Hand Surg Am. 2001;26:742–8. doi: 10.1053/jhsu.2001.24966. doi: 10.1053/jhsu.2001.24966. [DOI] [PubMed] [Google Scholar]
- 13.Yoshioka H, Ueno T, Tanaka T, Shindo M, Itai Y. High-resolution MR imaging of triangular fibrocartilage complex (TFCC): Comparison of microscopy coils and a conventional small surface coil. Skeletal Radiol. 2003;32:575–81. doi: 10.1007/s00256-003-0672-7. doi: 10.1007/s00256-003-0672-7. [DOI] [PubMed] [Google Scholar]
- 14.Fotiadou A, Patel A, Morgan T, Karantanas AH. Wrist injuries in young adults: The diagnostic impact of CT and MRI. Eur J Radiol. 2011;77:235–9. doi: 10.1016/j.ejrad.2010.05.011. doi: 10.1016/j.ejrad.2010.05.011. [DOI] [PubMed] [Google Scholar]
- 15.Clavero JA, Alomar X, Monill JM, Esplugas M, Golanó P, Mendoza M, et al. MR imaging of ligament and tendon injuries of the fingers. Radiographics. 2002;22:237–56. doi: 10.1148/radiographics.22.2.g02mr11237. doi: 10.1148/radiographics. 22.2.g02mr11237. [DOI] [PubMed] [Google Scholar]
- 16.Jeantroux J, Becce F, Guerini H, Montalvan B, Le Viet D, Drapé JL. Athletic injuries of the extensor carpi ulnaris subsheath: MRI findings and utility of gadolinium-enhanced fat-saturated T1-weighted sequences with wrist pronation and supination. Eur Radiol. 2011;21:160–6. doi: 10.1007/s00330-010-1887-3. doi: 10.1007/s00330-010-1887-3. [DOI] [PubMed] [Google Scholar]
- 17.Watanabe A, Souza F, Vezeridis PS, Blazar P, Yoshioka H. Ulnar-sided wrist pain. II. Clinical imaging and treatment. Skeletal Radiol. 2010;39:837–57. doi: 10.1007/s00256-009-0842-3. doi: 10.1007/s00256-009-0842-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Anderson ML, Skinner JA, Felmlee JP, Berger RA, Amrami KK. Diagnostic comparison of 1.5 Tesla and 3.0 Tesla preoperative MRI of the wrist in patients with ulnar-sided wrist pain. J Hand Surg Am. 2008;33:1153–9. doi: 10.1016/j.jhsa.2008.02.028. doi: 10.1016/j.jhsa.2008.02.028. [DOI] [PubMed] [Google Scholar]
- 19.Potter HG, Asnis-Ernberg L, Weiland AJ, Hotchkiss RN, Peterson MG, McCormack RR., Jr The utility of high-resolution magnetic resonance imaging in the evaluation of the triangular fibrocartilage complex of the wrist. J Bone Joint Surg Am. 1997;79:1675–84. doi: 10.2106/00004623-199711000-00009. doi: 10.2106/00004623-199711000-00009. [DOI] [PubMed] [Google Scholar]
- 20.Magee T. Comparison of 3-T MRI and arthroscopy of intrinsic wrist ligament and TFCC tears. AJR Am J Roentgenol. 2009;192:80–5. doi: 10.2214/AJR.08.1089. doi: 10.2214/AJR.08.1089. [DOI] [PubMed] [Google Scholar]
- 21.Vezeridis PS, Yoshioka H, Han R, Blazar P. Ulnar-sided wrist pain. Part I: Anatomy and physical examination. Skeletal Radiol. 2010;39:733–45. doi: 10.1007/s00256-009-0775-x. doi: 10.1007/s00256-009-0775-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Oneson SR, Timins ME, Scales LM, Erickson SJ, Chamoy L. MR imaging diagnosis of triangular fibrocartilage pathology with arthroscopic correlation. AJR Am J Roentgenol. 1997;168:1513–8. doi: 10.2214/ajr.168.6.9168716. doi: 10.2214/ajr.168.6.9168716. [DOI] [PubMed] [Google Scholar]
- 23.Tanaka T, Yoshioka H, Ueno T, Shindo M, Ochiai N. Comparison between high-resolution MRI with a microscopy coil and arthroscopy in triangular fibrocartilage complex injury. J Hand Surg Am. 2006;31:1308–14. doi: 10.1016/j.jhsa.2006.05.001. doi: 10.1016/j.jhsa.2006.05.001. [DOI] [PubMed] [Google Scholar]
- 24.Yoshioka H, Tanaka T, Ueno T, Carrino JA, Winalski CS, Aliabadi P, et al. Study of ulnar variance with high-resolution MRI: Correlation with triangular fibrocartilage complex and cartilage of ulnar side of wrist. J Magn Reson Imaging. 2007;26:714–9. doi: 10.1002/jmri.21084. doi: 10.1002/jmri. 21084. [DOI] [PubMed] [Google Scholar]
- 25.Amrami KK, Moran SL, Berger RA, Ehman EC, Felmlee JP. Imaging the distal radioulnar joint. Hand Clin. 2010;26:467–75. doi: 10.1016/j.hcl.2010.07.001. doi: 10.1016/j.hcl.2010.07.001. [DOI] [PubMed] [Google Scholar]
- 26.Xian JF, Chen M, Jin ZY. Magnetic resonance imaging in clinical medicine: Current status and potential future developments in China. Chin Med J. 2015;128:569–70. doi: 10.4103/0366-6999.151637. doi: 10.4103/0366-6999.151637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Xiao J, Cui GQ. Clinical and magnetic resonance imaging results of arthroscopic repair of intratendinous partial-thickness rotator cuff tears. Chin Med J. 2015;128:1496–501. doi: 10.4103/0366-6999.157669. doi: 10.4103/0366-6999.157669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Pahwa S, Srivastava DN, Sharma R, Gamanagatti S, Kotwal PP, Sharma V. Comparison of conventional MRI and MR arthrography in the evaluation wrist ligament tears: A preliminary experience. Indian J Radiol Imaging. 2014;24:259–67. doi: 10.4103/0971-3026.137038. doi: 10.4103/0971-3026.137038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Maizlin ZV, Brown JA, Clement JJ, Grebenyuk J, Fenton DM, Smith DE, et al. MR arthrography of the wrist: Controversies and concepts. Hand NY. 2009;4:66–73. doi: 10.1007/s11552-008-9149-4. doi: 10.1007/s11552-008-9149-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Fufa DT, Goldfarb CA. Sports injuries of the wrist. Curr Rev Musculoskelet Med. 2013;6:35–40. doi: 10.1007/s12178-012-9145-8. doi: 10.1007/s12178-012-9145-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Garcia-Elias M. Soft-tissue anatomy and relationships about the distal ulna. Hand Clin. 1998;14:165–76. [PubMed] [Google Scholar]
- 32.Theumann NH, Pfirrmann CW, Antonio GE, Chung CB, Gilula LA, Trudell DJ, et al. Extrinsic carpal ligaments: Normal MR arthrographic appearance in cadavers. Radiology. 2003;226:171–9. doi: 10.1148/radiol.2261011715. doi: 10.1148/radiol.2261011715. [DOI] [PubMed] [Google Scholar]
- 33.Daunt N. Magnetic resonance imaging of the wrist: Anatomy and pathology of interosseous ligaments and the triangular fibrocartilage complex. Curr Probl Diagn Radiol. 2002;31:158–76. doi: 10.1067/cdr.2002.125780. [PubMed] [Google Scholar]
- 34.Burns JE, Tanaka T, Ueno T, Nakamura T, Yoshioka H. Pitfalls that may mimic injuries of the triangular fibrocartilage and proximal intrinsic wrist ligaments at MR imaging. Radiographics. 2011;31:63–78. doi: 10.1148/rg.311105114. doi: 10.1148/rg.311105114. [DOI] [PubMed] [Google Scholar]
- 35.Skalski MR, White EA, Patel DB, Schein AJ, RiveraMelo H, Matcuk GR., Jr The traumatized TFCC: An illustrated review of the anatomy and injury patterns of the triangular fibrocartilage complex. Curr Probl Diagn Radiol. 2016;45:39–50. doi: 10.1067/j.cpradiol.2015.05.004. doi: 10.1067/j.cpradiol.2015.05.004. [DOI] [PubMed] [Google Scholar]
- 36.Cody ME, Nakamura DT, Small KM, Yoshioka H. MR imaging of the triangular fibrocartilage complex. Magn Reson Imaging Clin N Am. 2015;23:393–403. doi: 10.1016/j.mric.2015.04.001. doi: 10.1016/j.mric.2015.04.001. [DOI] [PubMed] [Google Scholar]