

Abstract
Research links Black-White health disparities to racial differences in socioeconomic status (SES), but understanding of the role of SES in racial health gaps has been restricted by reliance on static measures of health and socioeconomic well-being that mask the dynamic quality of these processes and ignore the racialized nature of the SES-health connection. Utilizing twenty-three years of longitudinal data from the Panel Study of Income Dynamics (1984-2007), this study uses multilevel growth curve models to examine how multiple dimensions of socioeconomic well-being—including long-term economic history and differential returns to SES—contribute to the life course patterning of Black-White health disparities across two critical markers of well-being: body mass index (N=9,057) and self-rated health (N=11,329). Findings indicate that long-term SES exerts a significant influence on both body mass index and self-rated health, net of point-in-time measures, and that Black-White health gaps are smallest in models that adjust for both long-term and current SES. I also find that Blacks and Whites receive differential health returns to increases in SES, which suggests that other factors—such as neighborhood segregation and exposure racial discrimination—may restrict Blacks from converting increases in SES into health improvements in the same way as Whites. Together, these processes contribute to the life course patterning of Black-White health gaps and raise concerns about previous misestimation of the role of SES in racial health disparities.
Keywords: racial health disparities, socioeconomic status, body mass index, self-rated health, life course, longitudinal analysis
Despite overall reductions in morbidity and mortality over the past century, Blacks in the United States are still more likely than Whites to experience death and disability from a range of diseases, including diabetes, cardiovascular disease, and cancer (Farmer and Ferraro 2005; Murphy, Xu, and Kochanek 2013; Williams et al. 2010). Scholars have characterized Blacks' high rates of morbidity as “first and worst,” whereby Blacks experience earlier onset of illness, greater severity of disease, and poorer survival rates than Whites (Williams et al. 2010). In the late nineteenth century, Du Bois (1899) claimed that the root causes of Black-White health disparities were social, due chiefly to the “vastly different conditions” in which Blacks and Whites lived and worked. Scholars today continue to recognize the social origins of racial health disparities. In particular, research identifies socioeconomic status (SES) as a fundamental determinant of health (Link and Phelan 1995), and efforts to understand the causes of racial health disparities have found that some of the observed Black-White gap in health can be explained by racial differences in SES (Clarke et al. 2010; Franks et al. 2006; Geronimus et al. 2001; Hayward et al. 2000; Williams et al. 2010). In general, studies find that accounting for the racial patterning of SES using point-in-time indicators such as annual income attenuates Black-White health disparities, but disparities persist even after “controlling” for SES.
While a wide body of research examines the contribution of SES to racial health disparities, critical gaps in the literature remain. In particular, while studies link cross-sectional levels of education, income, and wealth to mean level Black-White health gaps, few studies consider the role of long-term exposure to socioeconomic conditions (Pollack et al. 2007; Willson, Shuey, and Elder 2007), account for differential health returns to SES by race (Pearson 2008; Shuey and Willson 2008), or examine trajectories of health disparities across multiple outcomes using longitudinal data (Brown, O'Rand, and Adkins 2012). Together, these conceptual and methodological limitations raise critical questions about previous misestimation of the role of SES in producing Black-White health disparities across the life course. On the one hand, by excluding long-term measures of SES from model estimates, previous studies risk underestimating the role of SES in Black-White health gaps (Do 2009). On the other hand, by assuming that Blacks and Whites receive the same health benefits from increases in SES, previous estimates about the protective effects of SES may be overestimated (Pearson 2008). Further, limiting examinations of Black-White health gaps to cross-sectional studies of single health outcomes masks substantial variation in the role of various dimensions of SES in producing trajectories of racial health inequities across multiple domains of health.
This study aims to fill these gaps in the literature by examining the roles of multiple facets of socioeconomic well-being over time in the age patterning of Black-White health disparities. Utilizing more than twenty years of longitudinal data from the Panel Study of Income Dynamics (PSID), I use multilevel growth curve models to examine whether and how the incorporation of dynamic and multifaceted indicators of socioeconomic well-being—including cumulative exposure to economic conditions and differential health returns to socioeconomic resources—improves understanding of the role of SES in the life course patterning of Black-White disparities in body mass index and self-rated health. By conceptualizing and operationalizing SES as a multidimensional, dynamic, and racialized construct that shapes trajectories of multiple health outcomes, this study provides new knowledge of the determinants of Black-White health disparities and sheds light on potential leverage points for ameliorating racial health inequities.
Background
SES as a Fundamental Determinant of Health and Racial Health Disparities
Across the life course, low socioeconomic status is associated with increased morbidity and mortality risk (Krieger et al. 1997; Willson, Shuey, and Elder Jr 2007). There is no single mechanism underlying the link between SES and health, but instead there are a number of pathways through which SES shapes exposure to risks and access to health promoting resources and opportunities to ultimately affect health and well-being (Krieger, Williams, and Moss 1997; Link and Phelan 1995; Williams and Collins 1995). Compared to individuals of higher SES, lower SES individuals have less access to affordable healthy food options, less leisure time for physical activity, reduced access to medical care, and higher exposure to environmental toxins, violence, and psychosocial stress (Link and Phelan 1995; Williams and Collins 1995; Williams et al. 2010). Because SES reflects access to health-promoting resources, affects multiple disease outcomes through multiple mechanisms, and consequently maintains an association with disease even when intervening mechanisms change, SES can be considered a “fundamental cause” of health and disease risk (Link and Phelan 1995).
In addition to affecting health through multiple pathways, SES is also a multidimensional construct consisting of multiple components—such as education, income, and wealth—and research suggests that the individual components of SES may have unique associations with health. For example, while education may improve health by improving health efficacy and human capital, income can afford individuals access to the material resources needed to afford healthy lifestyles and proper preventive health care (Elo 2009; Lynch 2006). Further, studies document a strong association between wealth and health, net of other indicators of SES (Robert and House 1996; Pollack et al. 2007), with scholars hypothesizing that wealth may provide households with economic stability in times of diminished wages or economic distress (Boen and Yang 2016). For this reason, it is essential that studies of health include multiple measures of SES to fully capture the role of SES in affecting individual-level health and population-level health disparities (Braveman et al. 2005).
Given the racial stratification of socioeconomic resources in the U.S., a wide body of research links Black-White disparities in health to racial differences in SES. Though distinct, race and social class are interrelated dimensions of stratification that contribute to disparities in risk exposure, access to resources, and health (LaVeist 2005; Brown, O'Rand, and Adkins 2012). Phelan and Link (2015) argue that racism is a “fundamental cause” of disease, in large part due to its role in producing stark racial inequalities in SES. Compared to Whites, Blacks in the U.S. have lower levels of education (US Census 2012a), higher rates of unemployment (Bureau of Labor Statistics 2012), and higher poverty rates (US Census 2012b). Because SES is both a fundamental determinant of health (Link and Phelan 1995) and strongly patterned by race (Phelan and Link 2015), a number of studies find that racial health disparities are, at least partially, explained by racial differences in SES (Clarke et al. 2009; Do, Frank, and Finch 2012; Haas and Rohlfsen 2010; Haas, Krueger, and Rohlfsen 2012; Hayward et al 2000; Williams and Collins 1995; Williams et al. 2010).
Life Course Patterns of Racial Health Disparities
While a number of studies document racial health disparities in cross-sectional levels of health, less is known about racial differences in trajectories of health across the life course (Brown, O'Rand, and Akins 2012). A core principle of the life course perspective is an understanding that human development and aging are life-long processes (Pavalko and Willson 2011), and research documents significant variation in individual health over the life span. Further, research also finds that the magnitude, direction, and determinants of health gaps can also vary by outcome and across the life course. Research posits three main hypotheses related to the age patterning of racial health disparities. First, most studies of the life course patterning of Black-White health gaps find that disparities grow over time and diverge with age (Dupre 2007; Shuey and Willson 2008; Willson, Shuey, and Elder 2007), providing evidence of the “cumulative advantage hypothesis.” In racial disparities research, cumulative advantage suggests that racial health gaps grow though middle and late age, as Whites accumulate greater health and economic capital over time relative to Blacks. In addition to racial differences in the accumulation of life course capital, the process of cumulative advantage can be further amplified by racial differences in returns to resources (DiPrete and Eirich 2005; Shuey and Willson 2008). Second, other studies find that the racial health gap converges later in the life course—supporting the “age-as-leveler hypothesis” (House et al. 1994; House, Herd, and Lantz 2005; Kim and Miech 2009). This hypothesis holds that aging has negative health consequences for both advantage and disadvantaged population groups, and that biological frailty and senescence affect both groups in late life. As such, racial health disparities converge, and may even cross-over, in late life. Third, the “persistent inequality hypothesis” suggests that the magnitude of the Black-White health gap remains stable with age, with socioeconomic, demographic, and human capital factors having persistent effects on health across the life course (Ferraro and Farmer 1996; Haas and Rohlfsen 2010). While racial health disparities emerge early in the life course, this hypothesis suggests that the disparities are persistent across the life span.
Studies document that socioeconomic factors play a critical role in shaping age patterns of Black-White health inequities across the life course (Brown, O'Rand, and Akins 2012; Shuey and Willson 2008). In addition to affecting mean levels of health, research finds that the associations between various components of SES and health vary by life stage, which has implications for the life course patterning of racial health gaps (Dupre 2007; Willson, Shuey, and Elder 2007; Shuey and Willson 2008). For one, different components of SES may be more or less important for health at various life stages and, as a result, the associations between various components of SES and health may vary by age. For example, research finds that while income may best reflect the socioeconomic well-being of working-aged adults, wealth may have particularly strong associations with health indicators in later life, as individuals increasingly turn to their accumulated assets to support themselves and their families (Robert and House 1996; Boen and Yang 2016). In addition, similar to racial disparities in health, the magnitude of socioeconomic disparities in health may vary across the life course, as the advantages and disadvantages associated with the individual components of SES accumulate, diminish, or remain stable with age (Shuey and Willson 2008). As such, age variation in the associations between the various components of SES and health may play a critical role in the divergence, convergence, or persistence of health disparities across the life course.
Gaps in the Literature
Though socioeconomic factors are widely identified as key determinants of racial health disparities, critical gaps in the literature remain. First, previous research in this area has been limited by the inadequacy of standard, cross-sectional SES measures—such as annual income or annual wealth—to both capture the multidimensional and dynamic nature of socioeconomic well-being across the life course (Do 2009; Do, Frank, and Finch 2012; Pearson 2008). For one, annual income is unstable over time and does not necessarily reflect long term economic stability or instability. Income levels throughout the life course are incredibly volatile, and most individuals experience several sharp losses and gains in income throughout their lives (Duncan 1988; Rank and Hirschl 2001). Research suggests that slightly more than half of the U.S. population will experience poverty or affluence at some point in their lives, while only 20 percent of individuals will experience neither end of the income distribution (Rank and Hirschl 2001). Of those who experience poverty, most experience poverty spells of less than four years and approximately 50 percent exit poverty within a year (Stevens 1999). While cross-sectional measures of income and education are the most widely used indicators of SES in empirical research, studies of health inequities have increasingly incorporated measures of wealth (e.g., Bond Huie al. 2003; Hajat et al. 2010, 2011; Kim and Miech 2009; Robert and House 1996; Sweet et al. 2013). Incorporating measures of wealth into models of racial disparities is particularly critical, because while racial gaps in income are extreme, racial disparities in wealth are even larger (Taylor et al. 2011). Like income, however, wealth levels can also be volatile across the life cycle (Land and Russell 1996), and the wealth levels of Black households are particularly unstable and vulnerable to sharp losses (Pfeffer, Danzinger, and Schoeni 2013). As a result, cross-sectional measures of income and wealth are limited in their ability to capture the role of long-term socioeconomic well-being in the life course patterning of Black-White health disparities.
In the context of health, consideration of the duration of exposure to economic deprivation or advantage is particularly critical. Because it affects accumulation of economic and health capital over time, research suggests that long-term exposure to economic conditions has a greater effect on health than do temporary or episodic economic states (Ferraro and Kelley-Moore 2003; McDonough and Berglund 2003; McDonough et al. 2005; Williams and Collins 1995). For example, Willson, Shuey, and Elder (2007) found that, net of the beneficial effects of high annual income and wealth, those with persistently high income and wealth experienced additional health benefits; similarly, individuals who experienced long term exposure to economic deprivation faced additional health penalties. This temporal limitation is particularly problematic in the study of racial health disparities, as Blacks have lower poverty exit rates, higher poverty re-entry rates, and thus higher rates of long-term economic deprivation than Whites (Grieger and Wyse 2008; Iceland 2003; Stevens 1999). While a number of studies examine how the timing of exposure to economic conditions matters for health—particularly by studying the role of early-life SES on racial disparities in later life health (e.g., Glymour et al. 2008; Haas, Krueger, and Rohlfsen 2012)—few consider how the duration of exposure to socioeconomic conditions across the life course impact trajectories of Black-White health disparities.
Second, few studies account for the racialized nature of the social gradient in health by considering whether Blacks and Whites receive similar health returns to increases in SES (Pearson 2008). Research documents that Blacks and Whites receive different levels of economic return for their location in the educational and occupational hierarchies (Wilson 2007), and evidence of the “diminishing returns hypothesis” suggests that Blacks also receive fewer protective health benefits from increases in SES than Whites (Farmer and Ferraro 2005; Shuey and Willson 2008). Factors such as experiences with racial discrimination, stress associated with upward mobility, and contextual disadvantages associated with residential segregation may restrict highly educated Blacks from reaching their health potential, relative to their White SES peers (Hayward et al. 2000; Pearson 2008; Shuey and Willson 2008). Because increases in SES do not confer the same health benefits to Blacks as to Whites (Geronimus et al. 2001; Shuey and Willson 2008), failing to account for racial heterogeneity in the associations between SES and health may result in overestimating the protective effects of socioeconomic resources and underestimating the health risks of resource allocation for non-Whites, in particular (Pearson 2008).
Third, a wide body of research documents Black-White health disparities, but much of this research utilizes cross-sectional data to examine inequality in static health levels (Brown, O'Rand, and Adkins 2012; Kim and Miech 2009). Of the studies that do model age trajectories of health, many limit their analyses to older adult samples (Shuey and Willson 2008). These limitations raise both methodological and substantive concerns. Methodologically, studies that examine age variations in health using cross-sectional data risk conflating age and cohort variation (McDonough and Berglund 2003; Yang and Land 2013) and are subject to concerns about reverse causality in the association between SES and health (Smith 1999). Further, research on age trajectories of health that include only older individuals may be subject to concerns about selection bias, as individuals are, for a variety of largely unobserved reasons, “selected” for survival at older ages (Zajacova and Burgard 2013). Substantively, the over-reliance on findings from cross-sectional studies and older age samples restricts understanding of how intra-individual levels of health change over time, how Black-White health disparities vary across the life course, and how SES contributes to patterns of health improvement and decline as individuals age. Examinations of static health levels using cross-sectional, point-in-time health measures are unable to document and seek to understand intra-individual processes of aging (McDonough and Burglund 2003).
Finally, most studies of health disparities examine racial differences in a single health outcome, which masks potential variation in the social processes underlying racial disparities in different health outcomes (Brown, O'Rand, and Atkins 2012). Understanding whether and how the relationships between race, SES, and health vary across different outcomes is essential to developing and improving targeted intervention efforts aimed at reducing health inequities.
Research Objectives
The gaps in the literature outlined here are not without implications. In models of health disparities, the coefficient for race can be best understood as the unexplained racial health gap. By excluding multifaceted and dynamic measures of SES from models of racial health disparities, the coefficient estimates for race are potentially biased by the residual confounding of race and SES (Do 2009; Kaufman et al. 1997). Given that long-term patterns of income and wealth are both correlated with health and patterned by race, the unexplained race disparities signified by the point estimate for race could be overestimated. As a result, scholarly attention has increasingly turned to other possible explanations, such as racial differences in health behaviors, culture, or genetics (Krieger, Williams, and Moss 1997; Pearson 2008), to explain these “unexplained” racial health gaps. However, given that socioeconomic inequality may play a greater role in Black-White health inequities than has been estimated in previous studies, the quest for cultural, behavioral, and genetic explanations for unexplained racial health gaps may be unwarranted, as these “unexplained” racial health inequities may, in fact, be attributable to racial differences in SES. Further, because few studies consider whether Blacks and Whites receive differential returns to SES, previous estimates of the protective benefits of material resources may also be overestimated (Pearson 2008). In this way, efforts to reduce racial health gaps that focus exclusively on improving SES may prove insufficient if non-socioeconomic factors, such as experiences with racial discrimination, prevent Blacks from converting socioeconomic gains into health improvements in the same way as Whites.
This study extends the literature on race, SES, and health by being the first to simultaneously consider the role of dimensions of SES over time—including long-term SES and racial differences in health returns to SES—in the production of Black-White disparities in two essential health indicators across the life course. Linking dynamic and multifaceted measures of socioeconomic well-being with health trajectories using longitudinal data, this study has three specific objectives: 1) To examine the life-course patterning of Black-White disparities in body mass index and self-rated health; 2) To assess the roles of both cross-sectional and long-term SES in trajectories of Black-White health disparities; and 3) To examine whether Black-White differences in health returns to SES affect the magnitude of Black-White health gaps across the life course.
Data and Methods
Data
This study uses data from the Panel Study of Income Dynamics (PSID), which is a nationally representative, longitudinal study of individuals and their families in the United States. Started in 1968 as a way for the federal government to evaluate the War on Poverty, the original PSID sample was drawn from two independent samples: an oversample of 1,872 low income families from the Survey of Economic Opportunity (referred to as the “SEO sample”) conducted by the Census and a nationally representative sample of 2,930 families designed by the Survey Research Center at the University of Michigan (referred to as the “SRC sample”). Because of its focus on poverty, the original study included an over-sample of low-income and African American families. In combining the SEO and SRC samples, the PSID constituted a nationally probability sample of U.S. families. The PSID is now the longest running nationally representative longitudinal survey in the U.S., containing approximately 40 years of prospective life history data for the original families and their decedents (Institute for Social Research 2015). The analysis for this study includes data from eight survey waves that include information on health and wealth: 1984, 1989, 1994, 1999, 2001, 2003, 2005, and 2007. The body mass index analyses utilize data from 1999-2007 (the waves in which body mass index data was available), and the self-rated health analyses use all eight waves of data.
Analytic Sample
The analysis is limited to respondents aged 25 years and older who were listed as household “heads” or “wives” at the time of interview. Analytic samples include only Black and White respondents, as PSID did not begin consistently collecting data on representative samples of Latinos or Asians until 1997. In addition, the analytic samples are restricted to individuals who were interviewed at least three times to avoid problems with estimation (Singer and Willet 2003) and for whom there is complete data for the variables included in the analysis. Compared to those included in the analytic samples, respondents not included in the analyses were more likely to be Black, had lower levels of education, income, and wealth, and had longer durations of persistently low income and wealth (p<0001). Sensitivity analyses revealed that including individuals with fewer than three observations provided substantively similar results to analyses excluding respondents with fewer than three observations. In fact, the BMI results presented here are slightly conservative compared to model estimates that included respondents with fewer than three observations. The final analytic sample for the BMI analyses includes 9,057 respondents and 11,329 respondents for the self-rated health analyses.
Measures
Health
This study includes two essential markers of life course health: body mass index and self-rated health. Unlike measures of disability, disease, or mortality, which are most useful at older ages, these outcomes reflect continuous changes in well-being over time, which is particularly useful when estimating health trajectories (Deaton and Paxson 1998; Shaw and Krause 2002). Further, these outcomes encompass both subjective (in the case of self-rated health) and objective (in the case of body mass index) assessments of health.
I construct a continuous measure of body mass index (BMI) using self-reported data on respondent height and weight. Research indicates that BMI is highly predictive of disease and longevity, with higher BMI being linked to increased risk of cardiovascular disease, cancer, and premature mortality (Kopelman 2007). By including BMI as a continuous measure, this study will improve understanding of how various dimensions of SES predict weight loss and gain and, consequently, changes in BMI across the life course. Self-rated health is derived from a question asking respondents to rate their health as excellent, very good, good, fair, or poor. This variable is coded so that 1 represents excellent health and 5 represents poor health. Self-rated health has been validated across racial/ethnic groups (Chandola and Jenkinson 2000) and has been shown to be highly correlated with morbidity and mortality (Idler and Benyamini 1997; McDonough and Amick 2001).
SES
This study utilizes several measures of SES. Education is a time-constant, categorical measure of respondents' completed education (1=<high school; 2=high school or GED; 3=some college; 4=Bachelor's degree or higher). Annual household income, measured in tens of thousands of dollars, is adjusted for household size and inflation. Income is included as a lagged measure, so that health at time t is affected by income at time t-1. Total household wealth indicates a household's net worth measured in hundreds of thousands of dollars and, like the measure of income, is adjusted for household size and inflation and included as a lagged measure. Supplementary analyses revealed that the inclusion of polynomial and logged measures of income and wealth did not improve model fit and made the models more difficult to interpret, so only linear measures of income and wealth are included in the final models. Further, including income and wealth as continuous, rather than categorical, measures allowed me to retain as much information about these measures and their association with the outcomes as possible. To capture long-term patterns of income and wealth, I include time-varying measures of persistent income and persistent wealth, which are also adjusted for household size and inflation. Persistent high income and persistent high wealth are operationalized as the cumulative proportion of observations in which the respondent is in the top quintile of the income/wealth distribution. Similarly, persistent low income and persistent low wealth are defined as the cumulative proportion of observations in which a respondent is in the bottom quintile of the income/wealth distribution.
In order to examine whether Blacks and Whites receive differential health returns to SES, I include SES-by-race interaction terms for each of the SES measures. To examine how racial differences in the health returns to SES contribute to the life course patterning of health inequities, three-way interaction terms between all SES measures, race, and age are also included.
Other Measures
Race is included as a dummy variable (1=Black). For the majority of the sample, race is self-reported. In some cases, race is reported by the household head. Age is measured in years at the time of each survey and is centered on the youngest age of the sample (25 years) in order to aid in interpretation of parameter estimates. This study also includes a measure of quadratic age, as the effect of age of health trajectories may be curvilinear. Because research suggests that there are cohort differences in health trajectories, an indicator of cohort membership is included. Consistent with Willson, Shuey, and Elder et al. (2007) and Yang and Lee (2009), the cohort measure was constructed by dividing the sample into 10-year cohorts according to year of birth. Other measures include gender (1=female) and geographic region (1=South). To account for the varying number of observations between respondents, I include a continuous measure of total respondent observations. Finally, consistent with Chen, Yang, and Liu (2010), I include measures indicating death and non-response during the survey period to adjust for the impact of attrition on model estimates.
Analytic Strategy
I estimate changes in the outcomes using growth curve models, which are multilevel models used to estimate changes in individual outcomes over time using longitudinal data (Raudenbush and Bryk 2002). In these models, observations at different points in time at level 1 are “nested” within individuals at level 2. Growth curve models can be used to estimate models for data that are unbalanced in time (Raudenbush and Bryk 2002), as is the case with the PSID data. These models allow me to examine the effect of socioeconomic factors on both intra-individual trajectories of health and on Black-White health gaps across the life course. For BMI, I run linear models with random intercept and slope components. In the BMI models, only the intercept and slope (i.e., “age” coefficient) include random components. For self-rated health, I utilize mixed effects ordered logistic regression models with random intercepts only. Supplementary analyses revealed that, substantively, the BMI results were consistent across linear regression and ordered logit model specifications, where BMI categories included underweight (BMI<18.5 kg/m2), normal weight (BMI 18.5-24.9 kg/m2), overweight (BMI 25.0-29.9 kg/m2), and obese/extremely obese (BMI≥30.0 kg/m2). Further, self-rated health results were consistent across linear regression and ordered logit model specifications. Results for the linear BMI models are reported as coefficients with standard errors, and results of the ordered categorical self-rated health models are presented as odds ratios with 95% confidence intervals. All models were run in Stata 14. Standard errors account for the clustering of observations within individuals and individuals within households.
For model specification, Model 1 is an unadjusted model of Black-White disparities in the outcomes. Model 2 includes demographic controls but does not adjust for SES. Model 3 adjusts for SES using point-in-time measures of SES, including education, income, and wealth. Model 4 adjusts for SES using the long-term measures of SES. Model 5 incorporates both point-in-time and long-term measures of SES in order to better estimate how cumulative measures of SES affect the life course patterning of Black-White health disparities, net of point-in-time measures. Further, Model 5 indicates the extent to which simultaneous inclusion of multi-dimensional measures of SES account for Black-White health gaps.
Models with the subscript “a” include interaction terms for the SES measures and race, which allows me to examine whether Blacks and Whites receive differential health returns to SES. Model 3a builds on Model 3 by including interaction terms for Black*education, Black*income, and Black*wealth for both the intercept and the growth rate. Model 4a builds on Model 4 and includes interaction terms for Black*persistent low/high income and Black*persistent low/high wealth for both the intercept and the growth rate. Model 5a is the fully adjusted model that includes all SES measures plus race-by-SES interactions for both the growth rate and intercept.
In order to examine the life course patterning of Black-White disparities in BMI and self-rated health and assess the extent to which socioeconomic factors shape the life course patterning of the health gaps, I consider the magnitudes and directions of the parameter estimates for race, race*age, and race*age2 across the models. Evidence of the cumulative advantage hypothesis would include both a Black-White disparity in the intercept and a growth in the racial disparity with age; evidence of the age-as-leveler hypothesis would include an initial Black-disadvantage in the intercept but a declining racial disparity with age; and evidence of the persistent inequality hypothesis would include a significant racial disparity in the intercept, but no statistically significant racial disparity in growth rate with age.
Results
Descriptive Statistics
Table 1 displays the sample descriptive statistics for all waves combined by race. On average, Whites in the sample have better health and more socioeconomic resources than Blacks. Whites have lower BMIs, better self-rated health, and higher levels of educational attainment, annual income, and annual wealth than Black respondents (p<0.001). Further, Black respondents spend more time in the bottom of the income and wealth distributions than White respondents, while White respondents are more likely than Blacks to experience persistently high income and wealth (p<0.001).
Table 1. Sample Descriptive Statistics.
| Full Sample (N=11,329)a | Whites (N=7,844) | Blacks (N=3,485) | |||||
|---|---|---|---|---|---|---|---|
| Variable | Mean/Proportion | SD | Mean/Proportion | SD | Mean/Proportion | SD | p-valueb |
| Body mass index (kg/m2) | 27.44 | 5.81 | 26.66 | 5.38 | 29.28 | 6.35 | <0.001 |
| Self-rated health (1=excellent, 5=poor) | 2.39 | 1.04 | 2.27 | 1.01 | 2.69 | 1.05 | <0.001 |
| Completed education | |||||||
| <High school | 0.21 | - | 0.16 | - | 0.33 | - | <0.001 |
| High school or GED | 0.40 | - | 0.39 | - | 0.42 | - | |
| Some college | 0.20 | - | 0.21 | - | 0.17 | - | |
| Bachelor's degree or higher | 0.19 | - | 0.24 | - | 0.07 | - | |
| Total household income | 45,012 | 60,620 | 52,375 | 69,175 | 26,907 | 21,988 | <0.001 |
| Total household wealth | 174,685 | 694,870 | 228,772 | 810,089 | 41,697 | 177,838 | <0.001 |
| Proportion waves low incomec | 0.20 | 0.31 | 0.12 | 0.23 | 0.39 | 0.38 | <0.001 |
| Proportion waves high incomec | 0.20 | 0.30 | 0.26 | 0.32 | 0.06 | 0.17 | <0.001 |
| Proportion waves low wealthc | 0.20 | 0.31 | 0.12 | 0.25 | 0.38 | 0.37 | <0.001 |
| Proportion waves high wealthc | 0.20 | 0.33 | 0.27 | 0.36 | 0.03 | 0.12 | <0.001 |
| Gender (1=female) | 0.54 | - | 0.52 | - | 0.61 | - | <0.001 |
| Age (in years) | 46.29 | 14.35 | 47.22 | 14.86 | 43.99 | 12.71 | <0.001 |
| Death (1=died) | 0.06 | - | 0.06 | - | 0.06 | - | 0.251 |
| Nonresponse (1=nonresponder) | 0.05 | - | 0.05 | - | 0.07 | - | <0.001 |
| Total number respondent observations | 6.20 | 1.81 | 6.34 | 1.78 | 5.88 | 1.83 | <0.001 |
| Residence in South (1=South) | 0.42 | - | 0.31 | - | 0.70 | - | <0.001 |
Sample size based on self-rated health analytic sample, with exception of BMI measure (N=9,057)
p-value provided for the difference between Blacks and Whites; two-tailed test
for descriptive statistics, proportion of waves in which respondent was high/low income/wealth was calculated at respondent's final observation
Multilevel Growth Curve Models
BMI
Life Course Patterning of the Black-White BMI Gap
The results of the BMI models are presented in Table 2. The coefficient for race, which indicates the unexplained mean level racial disparity in BMI, is largest in Models 1 and 2, where there are no controls for SES. While including the point-in-time measures of SES in Model 3 results in just a 12 percent reduction in the race gap in BMI over Model 1, including the cumulative SES measures in Model 4 reduces the unexplained race gap by 26 percent over Model 1. Including both the cross-sectional and cumulative measures of SES in Model 5 reduces the coefficient for race over Models 3 and 4, where the cross-sectional and cumulative SES measures are included separately. The racial disparity in mean BMI is smallest in Model 5a, when the point-in-time, cumulative SES measures, and race-by-SES interaction terms are included. Regarding the growth rate of the racial disparity with age, the coefficient for Black*age across all models reveals that the magnitude of Black-White BMI gaps are stable across the life course. Together, these results suggest that SES is a key driver of Black-White disparities in BMI, though the Black-White BMI gap persists even after adjusting for BMI. Further, the life course patterning of Black-White BMI disparities is consistent with the persistent inequality hypothesis, where the magnitude of Black-White differences in BMI remains stable with age. Figure 1, which is based on the fully adjusted Model 5a, visually depicts the life course patterning of Black-White BMI disparities, where the Black-White health gap is relatively stable with age. As indicated by the Akaike information criterion (AIC) statistic, Model 5a, which adjusts for all SES measures and accounts for racial differences in health returns to SES, provides the best model fit.
Table 2. Multilevel Growth Curve Models of Body Mass Index, PSID 1999-2007 (N =9,057).
| Baseline models | Point-in-time SES models | Cumulative SES models | Fully adjusted models | |||||
|---|---|---|---|---|---|---|---|---|
|
|
|
|
|
|||||
| Model 1 | Model 2 | Model 3 | Model 3a | Model 4 | Model 4a | Model 5 | Model 5a | |
| Coeff. (SE) | Coeff. (SE) | Coeff. (SE) | Coeff. (SE) | Coeff. (SE) | Coeff. (SE) | Coeff. (SE) | Coeff. (SE) | |
| Fixed effect parameters | ||||||||
| For intercept | ||||||||
| Race (Black=1) | 2.19*** | 2.21*** | 1.92*** | 1.76*** | 1.63*** | 1.43*** | 1.49*** | 1.13* |
| (0.27) | (0.27) | (0.28) | (0.43) | (0.28) | (0.35) | (0.28) | (0.49) | |
| Education (<HS is reference) | ||||||||
| High school | -0.75** | -0.83** | -0.55* | -0.65* | ||||
| (0.24) | (0.31) | (0.24) | (0.31) | |||||
| Some college | -1.26*** | -1.52*** | -0.90** | -1.26*** | ||||
| (0.28) | (0.34) | (0.28) | (0.34) | |||||
| BA degree or higher | -2.68*** | -2.93*** | -2.02*** | -2.36*** | ||||
| (0.31) | (0.36) | (0.33) | (0.37) | |||||
| Income | -0.0001 | -1.70e-05 | 0.0005 | 0.0003 | ||||
| (0.001) | (0.001) | (0.0007) | (0.001) | |||||
| Wealth | -0.0003** | -0.0004** | -0.0002 | -0.0003** | ||||
| (9.71e-05) | (0.0001) | (9.85e-05) | (0.0001) | |||||
| Black* education (<HS is reference) | ||||||||
| Black* high school | -0.004 | 0.03 | ||||||
| (0.50) | (0.50) | |||||||
| Black* some college | 0.82 | 1.09 | ||||||
| (0.62) | (0.62) | |||||||
| Black* BA degree or higher | 1.39 | 1.73* | ||||||
| (0.86) | (0.88) | |||||||
| Black* income | -0.004 | 0.01 | ||||||
| (0.004) | (0.005) | |||||||
| Black* wealth | 0.0005 | 0.0004 | ||||||
| (0.0003) | (0.0003) | |||||||
| Persistent low income | 0.97*** | 0.63* | 0.84*** | 0.45 | ||||
| (0.22) | (0.30) | (0.23) | (0.31) | |||||
| Persistent high income | -0.59* | -0.55* | -0.36 | -0.26 | ||||
| (0.26) | (0.28) | (0.27) | (0.29) | |||||
| Persistent low wealth | 1.16*** | 1.09*** | 1.07*** | 0.96*** | ||||
| (0.21) | (0.26) | (0.21) | (0.26) | |||||
| Persistent high wealth | -1.30*** | -1.50*** | -1.04** | -1.15*** | ||||
| (0.31) | (0.32) | (0.31) | (0.33) | |||||
| Black* persistent low income | 0.01 | 0.01 | ||||||
| (0.02) | (0.02) | |||||||
| Black* persistent high income | 0.07 | 0.07* | ||||||
| (0.04) | (0.04) | |||||||
| Black* persistent low wealth | -0.04* | -0.04* | ||||||
| (0.02) | (0.02) | |||||||
| Black* persistent high wealth | -0.05 | -0.03 | ||||||
| (0.04) | (0.04) | |||||||
| Gender (female=1) | -0.98*** | -1.03*** | -1.02*** | -1.08*** | -1.08*** | -1.09*** | -1.09*** | |
| (0.12) | (0.12) | (0.12) | (0.11) | (0.15) | (0.11) | (0.11) | ||
| Cohort | 0.15** | 0.18*** | 0.17*** | 0.10* | 0.10* | 0.13** | 0.12** | |
| (0.04) | (0.04) | (0.04) | (0.04) | (0.04) | (0.04) | (0.04) | ||
| Region (South=1) | 0.25* | 0.21* | 0.21 | 0.23 | 0.22 | 0.21 | 0.21 | |
| (0.12) | (0.12) | (0.12) | (0.12) | (0.12) | (0.12) | (0.12) | ||
| Death | -0.62 | -0.86** | -0.85* | -0.59 | -0.59 | -0.75* | -0.75* | |
| (0.35) | (0.35) | (0.35) | (0.35) | (0.35) | (0.35) | (0.35) | ||
| Nonresponse | -0.49* | -0.49** | -0.48* | -0.54* | -0.54* | -0.53* | -0.53** | |
| (0.23) | (0.23) | (0.23) | (0.23) | (0.23) | (0.23) | (0.23) | ||
| Total number of observations | -0.29** | -0.21** | -0.21* | -0.25** | -0.26** | -0.21* | -0.21* | |
| (0.09) | (0.09) | (0.09) | (0.08) | (0.08) | (0.08) | (0.08) | ||
| For linear growth rate | ||||||||
| Age | 0.19*** | 0.20*** | 0.21*** | 0.22*** | 0.23*** | 0.23*** | 0.24*** | 0.24*** |
| (0.01) | (0.01) | (0.01) | (0.01) | (0.01) | (0.01) | (0.01) | (0.01) | |
| Black* age | 0.04 | 0.03 | 0.03 | 0.01 | 0.03 | 0.03 | 0.02 | 0.01 |
| (0.02) | (0.02) | (0.02) | (0.02) | (0.02) | (0.02) | (0.02) | (0.03) | |
| Education* age (<HS is reference) | ||||||||
| High school* age | -0.002 | -0.01 | -0.002 | -0.01 | ||||
| (0.008) | (0.01) | (0.01) | (0.01) | |||||
| Some college* age | 0.01 | 0.005 | 0.01 | 0.01 | ||||
| (0.01) | (0.01) | (0.01) | (0.01) | |||||
| BA degree or higher* age | 0.01 | 0.01 | 0.01 | 0.01 | ||||
| (0.01) | (0.01) | (0.01) | (0.01) | |||||
| Income* age | 8.55e-06 | 2.71e-06 | -2.64e-06 | 3.75e-07 | ||||
| (2.37e-05) | (2.40e-05) | (2.44e-05) | (2.47e-05) | |||||
| Wealth* age | 6.81e-06** | 9.66e-06** | 4.71e-06 | 7.32e-06* | ||||
| (2.63e-06) | (2.89e-06) | (2.66e-06) | (-2.93e-06) | |||||
| Black* education* age (<HS is reference) | ||||||||
| Black* high school* age | 0.03 | 0.03 | ||||||
| (0.02) | (0.02) | |||||||
| Black* some college* age | -0.003 | -0.01 | ||||||
| (0.02) | (0.02) | |||||||
| Black* BA degree or higher* age | -0.03 | -0.04 | ||||||
| (0.03) | (0.03) | |||||||
| Black* income* age | 0.0003 | 7.06e-06 | ||||||
| (0.0002) | (0.0002) | |||||||
| Black* wealth* age | -8.44e-06 | -8.51e-06 | ||||||
| (1.26e-05) | (1.29e-05) | |||||||
| Persistent low income* age | -0.02** | -0.02 | -0.02** | -0.02 | ||||
| (0.01) | (0.01) | (0.01) | (0.01) | |||||
| Persistent high income* age | -0.002 | -0.01 | -0.003 | -0.01 | ||||
| (0.01) | (0.01) | (0.01) | (0.01) | |||||
| Persistent low wealth* age | -0.01 | 0.01 | -0.01 | 0.01 | ||||
| (0.01) | (0.01) | (0.01) | (0.01) | |||||
| Persistent high wealth* age | 0.01 | 0.01 | 0.01 | 0.01 | ||||
| (0.01) | (0.01) | (0.01) | (0.01) | |||||
| Black* persistent low income* age | 0.52 | 0.85 | ||||||
| (0.46) | (0.48) | |||||||
| Black* persistent high income* age | -1.03 | -1.57 | ||||||
| (0.87) | (0.91) | |||||||
| Black* persistent low wealth* age | 0.22 | 0.33 | ||||||
| (0.43) | (0.43) | |||||||
| Black* persistent high wealth* age | 1.94 | 1.19 | ||||||
| (1.09) | (1.11) | |||||||
| For quadratic growth rate | ||||||||
| Age2 | -0.003*** | -0.003*** | -0.003*** | -0.003*** | -0.003*** | -0.003*** | -0.003*** | -0.003*** |
| (0.0002) | (0.0002) | (0.0002) | (0.0002) | (0.0002) | (0.0002) | (0.0002) | (0.0002) | |
| Black* age2 | -0.001 | -0.001 | -0.0005 | -0.0002 | -0.0004 | -0.0005 | -0.0004 | -0.0003 |
| (0.0004) | (0.0004) | (0.0004) | (0.0004) | (0.0004) | (0.0004) | (0.0004) | (0.0004) | |
|
| ||||||||
| Model fit statistics | ||||||||
| AIC | 208424 | 208234 | 165432 | 165428 | 208111 | 208097 | 165292 | 165263 |
|
| ||||||||
| Number of observations | 31,507 | 31,507 | 31,507 | 31,507 | 31,507 | 31,507 | 31,507 | 31,507 |
| Number of respondents | 9,057 | 9,057 | 9,057 | 9,057 | 9,057 | 9,057 | 9,057 | 9,057 |
Notes: Results presented as coefficients; standard errors in parentheses. In interest of space, only fixed effects parameters are displayed.
p<0.001,
p<0.01,
p<0.05
Figure 1. Age Trajectory of Body Mass Index by Race (N=9,057).
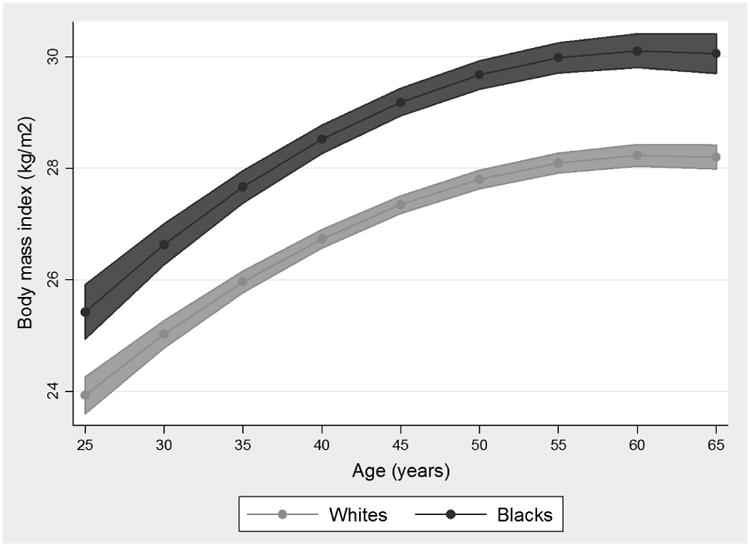
Note: Figure based on results from Model 5a (the fully adjusted model) of Table 1.
SES and Black-White BMI Inequity
Models 3, 4, and 5 assess the effects of multiple indicators of SES on BMI and indicate the extent to different dimensions of SES contribute Black-White health gaps. The results in Model 3, which adjusts for the cross-sectional measures of SES, indicate that increases in education are associated with lower BMI, net of income and wealth. I also find that increases in wealth are associated with lower BMI (-0.0003, p=0.003), and that the impact of wealth on BMI decreases slightly with age, as indicated by the coefficient for wealth*age. I find no association between income and BMI, net of education and wealth. The reduction in the coefficients for race in Model 3 compared to Model 2, which has no controls for SES, indicates that Black-White disparities in cross-sectional levels of SES help to account for the Black-White gap in BMI.
Model 4 of Table 2 includes measures of cumulative SES and documents the extent to which long-term patterns of income and wealth shape BMI trajectories and contribute to the Black-White disparity in BMI. The positive coefficients for the persistent low income (0.97, p<0.001) and persistent low wealth (1.16, p<0.001) reveal that long-term exposure to economic deprivation has detrimental effects on health. Conversely, Model 4 reveals that persistent high income (-0.59, p=0.02) and persistent high wealth (-1.30, p<0.001) protect against increases in BMI. While the effects of long-term wealth remain stable across the life course, the effects of persistent low income on BMI decrease with age. The reduction in the mean Black-White disparity in Model 4 over Models 1 and 2 indicates that racial differences in long-term SES are determinants of the Black-White disparity in mean BMI, though the measures of long-term SES do not produce racial differences in the growth rate of the BMI disparity with age.
In Model 5, I simultaneously include both point-in-time and cumulative SES measures. Results indicate that education continues to be protective against increases in BMI, even when the measures of income, education, and cumulative SES are included in the model. The protective effects of education remain stable with age. Further, persistent low income (0.84, p<0.001) and persistent low wealth (1.07, p<0.001) are associated with increases in BMI, whereas persistent high wealth (-1.04, p=0.001) offers protective benefits. Consistent with Model 4, Model 5 also reveals that the health effects of long-term low income decrease with age. These results suggest that the point-in-time and cumulative measures of SES each account for portions of the observed mean level racial BMI gap and may independently contribute to Black-White disparities in BMI. After accounting for multiple dimensions of SES in Model 5, the coefficient for race, which signifies the unexplained Black-White BMI disparity, is greatly reduced in magnitude over Models 1, 2, 3, and 4.
Differential Returns to SES
Models 3a, 4a, and 5a assess whether Blacks and Whites receive differential health returns to SES. Results from Model 3a suggests that Blacks and Whites receive similar health protection from increases in the point-in-time SES measures. Model 4a examines whether Blacks and Whites receive differential health returns to the cumulative measures of SES and reveals that Blacks are less harmed by persistent low wealth than Whites (-0.04, p=0.04). Model 5a, which includes race-by-SES interaction terms for all the SES measures, indicates that Blacks receive fewer health returns to attending college, receive less protective benefits from persistent high income, and are less harmed by persistent low wealth than Whites. Together, results from these models offer evidence that increases in SES do not protect Blacks from increases in BMI in the same way as Whites.
Self-Rated Health
Life Course Patterning of the Black-White Self-Rated Health Gap
The results of the self-rated health analyses are presented in Table 3. Consistent with the BMI results, the odds ratio for race, which indicates the unexplained racial disparity in mean self-rated health, is largest in Model 1. Controlling for demographic characteristics and attrition in Model 2 results in a modest attenuation of the mean race disparity in self-rated health over the unadjusted model. However, including the point-in-time measures of SES in Model 3 results a 36 percent reduction in the race gap in self-rated health over Model 1. When the cumulative SES measures are included in Model 4, the unexplained race gap in self-rated health is reduced by nearly 50 percent over Model 1. Including both the point-in-time and cumulative SES measures in Model 5 further reduces the magnitude of the Black-White disparity in mean levels of self-rated health. In Model 5a, which includes all the SES measures and race-by-SES interaction terms for all SES measures, the coefficient for race is no longer significant, suggesting that fully accounting for SES and racial differences in health returns to SES fully explains the Black-White disparity in mean levels of self-rated health. Across all models in Table 3, the odds ratio (OR) for Black*age is greater than 1, and the OR for Black*age2 is less than 1, indicating that the racial gap in self-rated diverges with age but diminishes slightly at older ages, providing evidence of the cumulative advantage hypothesis. Figure 2, which is based on the fully adjusted Model 5a, illustrates Black-White differences in the probability of reporting “poor” or “excellent” health across the life course and demonstrates how racial disparities in these levels of self-rated health diverge with age. Adjusting for point-in-time SES measures in Model 3 does nothing to reduce the racial disparity in the growth rate of health with age over Models 1 or 2. The race coefficient for growth rate is smallest in Models 3a, 4, 5, and 5a, where I account for race differences in health returns to the point-in-time measures, include the measures of cumulative SES, and fully adjust for all SES measures and race differences in returns to SES, respectively. This suggests that racial differences in long-term exposure to economic conditions and returns to increases in SES are at least partially responsible for the divergence of the Black-White health gap with age. The AIC statistics reported in Table 3 suggest that Model 5a provides the best model fit.
Table 3. Multilevel Growth Curve Models of Self-Rated Health, PSID 1984-2007 (N =11,329).
| Baseline models | Point-in-time SES models | Cumulative SES models | Fully adjusted models | |||||
|---|---|---|---|---|---|---|---|---|
|
|
|
|
|
|||||
| Model 1 | Model 2 | Model 3 | Model 3a | Model 4 | Model 4a | Model 5 | Model 5a | |
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Fixed effect parameters | ||||||||
| For intercept | ||||||||
| Race (Black=1) | 2.72*** | 2.25*** | 1.73*** | 1.49* | 1.37** | 1.45* | 1.27* | 1.22 |
| (2.19 - 3.39) | (1.81 - 2.81) | (1.39 - 2.16) | (1.05 - 2.13) | (1.09 - 1.73) | (1.07 - 1.96) | (1.01 - 1.59) | (0.79 - 1.87) | |
| Education (<HS is reference) | ||||||||
| High school | 0.70*** | 0.69*** | 0.80* | 0.79 | ||||
| (0.58 - 0.85) | (0.54 - 0.88) | (0.67 - 0.97) | (0.62 - 1.00) | |||||
| Some college | 0.33*** | 0.31*** | 0.42*** | 0.38*** | ||||
| (0.27 - 0.42) | (0.23 - 0.40) | (0.34 - 0.53) | (0.29 - 0.50) | |||||
| BA degree or higher | 0.15*** | 0.13*** | 0.22*** | 0.20*** | ||||
| (0.12 - 0.19) | (0.10 - 0.17) | (0.17 - 0.29) | (0.15 - 0.27) | |||||
| Income | 0.98*** | 0.98*** | 0.99 | 1.00 | ||||
| (0.96 - 0.99) | (0.97 - 0.99) | (0.98 - 1.00) | (0.98 - 1.01) | |||||
| Wealth | 0.97*** | 0.97*** | 0.98** | 0.97** | ||||
| (0.96 - 0.98) | (0.95 - 0.98) | (0.96 - 0.99) | (0.96 - 0.99) | |||||
| Black* education (<HS is reference) | ||||||||
| Black* high school | 0.99 | 0.97 | ||||||
| (0.67 - 1.47) | (0.66 - 1.44) | |||||||
| Black* some college | 1.15 | 1.16 | ||||||
| (0.71 - 1.87) | (0.71 - 1.90) | |||||||
| Black* BA degree or higher | 2.03* | 1.67 | ||||||
| (1.07 - 3.84) | (0.87 - 3.23) | |||||||
| Black* income | 0.95 | 0.96 | ||||||
| (0.90 - 1.00) | (0.90 - 1.03) | |||||||
| Black* wealth | 1.04 | 1.04 | ||||||
| (1.00 - 1.09) | (0.99 - 1.08) | |||||||
| Persistent low income | 2.71*** | 4.05*** | 2.18*** | 3.22*** | ||||
| (2.18 - 3.38) | (2.99 - 5.47) | (1.74 - 2.73) | (2.38 - 4.37) | |||||
| Persistent high income | 0.49*** | 0.45*** | 0.71* | 0.66*** | ||||
| (0.38 - 0.63) | (0.34 - 0.59) | (0.54 - 0.93) | (0.50 - 0.88) | |||||
| Persistent low wealth | 1.69*** | 1.50** | 1.56*** | 1.35* | ||||
| (1.37 - 2.09) | (1.15 - 1.96) | (1.26 - 1.92) | (1.04 - 1.77) | |||||
| Persistent high wealth | 0.59** | 0.61** | 0.72* | 0.75 | ||||
| (0.43 - 0.79) | (0.44 - 0.83) | (0.53 - 0.97) | (0.54 - 1.04) | |||||
| Black* persistent low income | 0.47** | 0.45** | ||||||
| (0.30 - 0.73) | (0.28 - 0.73) | |||||||
| Black* persistent high income | 3.16** | 3.35* | ||||||
| (1.36 - 7.33) | (1.34 - 8.37) | |||||||
| Black* persistent low wealth | 1.37 | 1.44 | ||||||
| (0.88 - 2.11) | (0.93 - 2.22) | |||||||
| Black* persistent high wealth | 0.99 | 0.82 | ||||||
| (0.30 - 3.24) | (0.25 - 2.77) | |||||||
| Gender (female=1) | 1.45*** | 1.39*** | 1.38*** | 1.27*** | 1.29*** | 1.27*** | 1.28*** | |
| (1.32 - 1.59) | (1.27 - 1.52) | (1.26 - 1.51) | (1.16 - 1.39) | (1.17 - 1.41) | (1.16 - 1.39) | (1.17 - 1.40) | ||
| Cohort | 1.01 | 1.06** | 1.06*** | 0.97 | 0.97 | 1.01 | 1.01 | |
| (0.97 - 1.06) | (1.02 - 1.11) | (1.02 - 1.11) | (0.93 - 1.01) | (0.93 - 1.01) | (0.96 - 1.05) | (0.97 - 1.05) | ||
| Region (South=1) | 1.36*** | 1.29*** | 1.29*** | 1.32*** | 1.31*** | 1.30*** | 1.28*** | |
| (1.23 - 1.51) | (1.17 - 1.42) | (1.17 - 1.42) | (1.20 - 1.46) | (1.19 - 1.44) | (1.18 - 1.43) | (1.17 - 1.41) | ||
| Death | 2.46*** | 1.94*** | 1.93*** | 2.54*** | 2.55*** | 2.22*** | 2.21*** | |
| (2.00 - 3.02) | (1.59 - 2.38) | (1.58 - 2.36) | (2.09 - 3.10) | (2.09 - 3.11) | (1.82 - 2.70) | (1.81 - 2.69) | ||
| Nonresponse | 0.82 | 0.85 | 0.85 | 0.77** | 0.78* | 0.79* | 0.80* | |
| (0.67 - 1.00) | (0.70 - 1.03) | (0.70 - 1.03) | (0.64 - 0.93) | (0.65 - 0.95) | (0.66 - 0.95) | (0.66 - 0.96) | ||
| Total number of observations | 0.88*** | 0.95** | 0.95*** | 0.90*** | 0.90*** | 0.94*** | 0.94** | |
| (0.85 - 0.92) | (0.92 - 0.99) | (0.92 - 0.99) | (0.86 - 0.93) | (0.87 - 0.93) | (0.90 - 0.97) | (0.91 - 0.98) | ||
| For linear growth rate | ||||||||
| Age | 1.04*** | 1.05*** | 1.07*** | 1.07*** | 1.08*** | 1.08*** | 1.08*** | 1.08*** |
| (1.03 - 1.05) | (1.04 - 1.06) | (1.06 - 1.08) | (1.06 - 1.09) | (1.07 - 1.09) | (1.07 - 1.09) | (1.07 - 1.10) | (1.07 - 1.10) | |
| Black* age | 1.04*** | 1.04*** | 1.04*** | 1.03* | 1.03** | 1.04*** | 1.03** | 1.03* |
| (1.02 - 1.06) | (1.02 - 1.06) | (1.02 - 1.05) | (1.01 - 1.05) | (1.01 - 1.05) | (1.02 - 1.06) | (1.011 - 1.047) | (1.00 - 1.05) | |
| Education* age (<HS is reference) | ||||||||
| High school* age | 0.99** | 0.99*** | 0.99 | 0.99* | ||||
| (0.98 - 0.99) | (0.98 - 0.99) | (0.99 - 1.00) | (0.98 - 1.00) | |||||
| Some college* age | 1.00 | 0.99 | 1.00 | 1.00 | ||||
| (0.99 - 1.01) | (0.98 - 1.00) | (0.99 - 1.01) | (0.99 - 1.01) | |||||
| BA degree or higher* age | 1.00 | 1.00 | 1.01 | 1.00 | ||||
| (0.99 - 1.01) | (0.99 - 1.01) | (1.00 - 1.02) | (1.00 - 1.01) | |||||
| Income* age | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| (1.00 - 1.00) | (1.00 - 1.00) | (1.00 - 1.00) | (1.00 - 1.00) | |||||
| Wealth* age | 1.001** | 1.001*** | 1.001** | 1.001** | ||||
| (1.00 - 1.001) | (1.00 - 1.001) | (1.00 - 1.001) | (1.00 - 1.001) | |||||
| Black* education* age (<HS is reference) | ||||||||
| Black* high school* age | 1.01 | 1.01 | ||||||
| (0.99 - 1.02) | (0.99 - 1.02) | |||||||
| Black* some college* age | 1.02* | 1.02 | ||||||
| (1.00 - 1.04) | (1.00 - 1.04) | |||||||
| Black* BA degree or higher* age | 1.00 | 1.01 | ||||||
| (0.98 - 1.03) | (0.98 - 1.03) | |||||||
| Black* income* age | 1.00 | 1.00 | ||||||
| (1.00 - 1.00) | (1.00 - 1.00) | |||||||
| Black* wealth* age | 1.00 | 1.00 | ||||||
| (1.00 - 1.000) | (1.00 - 1.00) | |||||||
| Persistent low income* age | 0.99 | 0.98** | 0.99 | 0.99** | ||||
| (0.98 - 1.00) | (0.97 - 0.99) | (0.99 - 1.00) | (0.98 - 1.00) | |||||
| Persistent high income* age | 1.00 | 1.00 | 0.99 | 1.00 | ||||
| (0.99 - 1.01) | (0.99 - 1.01) | (0.98 - 1.00) | (0.99 - 1.01) | |||||
| Persistent low wealth* age | 1.02** | 1.03*** | 1.02** | 1.04*** | ||||
| (1.01 - 1.03) | (1.02 - 1.05) | (1.01 - 1.03) | (1.02 - 1.05) | |||||
| Persistent high wealth* age | 0.99 | 0.99 | 0.99* | 0.99* | ||||
| (0.98 - 1.00) | (0.98 - 1.00) | (0.98 - 1.00) | (0.98 - 1.00) | |||||
| Black* persistent low income* age | 1.02 | 1.02* | ||||||
| (1.00 - 1.03) | (1.00 - 1.04) | |||||||
| Black* persistent high income* age | 0.96* | 0.95* | ||||||
| (0.93 - 0.99) | (0.92 - 0.99) | |||||||
| Black* persistent low wealth* age | 0.96** | 0.96*** | ||||||
| (0.95 - 0.98) | (0.94 - 0.98) | |||||||
| Black* persistent high wealth* age | 1.00 | 1.01 | ||||||
| (0.96 - 1.04) | (0.97 - 1.05) | |||||||
| For quadratic growth rate | ||||||||
| Age2 | 1.001*** | 1.001*** | 1.001** | 1.001* | 1.00 | 1.00 | 1.00 | 1.00 |
| (1.00 - 1.001) | (1.00 - 1.001) | (1.00 - 1.001) | (1.00 - 1.001) | (1.00 - 1.00) | (1.00 - 1.00) | (1.00 - 1.00) | (1.00 - 1.00) | |
| Black* age2 | 0.999*** | 0.999*** | 0.999*** | 0.999*** | 0.999*** | 0.999*** | 0.999*** | 0.999*** |
| (0.999 - 1.00) | (0.999 - 1.00) | (0.999 - 1.00) | (0.999 - 1.00) | (0.999 - 1.00) | (0.999 - 1.00) | (0.999 - 1.00) | (0.999 - 1.00) | |
|
| ||||||||
| Model fit statistics | ||||||||
| AIC | 117987 | 117702 | 116944 | 116920 | 116737 | 116708 | 116414 | 116379 |
|
| ||||||||
| Number of observations | 51,230 | 51,230 | 51,230 | 51,230 | 51,230 | 51,230 | 51,230 | 51,230 |
| Number of respondents | 11,329 | 11,329 | 11,329 | 11,329 | 11,329 | 11,329 | 11,329 | 11,329 |
Notes: Results presented as odds ratios; 95% confidence intervals in parentheses. In interest of space, only fixed effects parameters are displayed.
p<0.001,
p<0.01,
p<0.05
Figure 2. Age Trajectories of “Poor” and “Excellent” Self-Rated Health by Race (N=11,329).
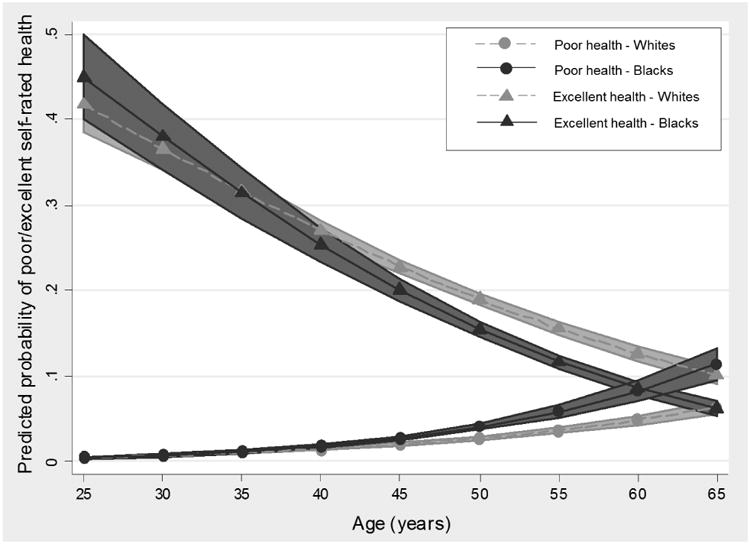
Note: Figure based on results from Model 5a (the fully adjusted model) of Table 2.
SES and Black-White Self-Rated Health Inequity
Model 3 includes the cross-sectional SES measures and indicates that increases in education, income, and wealth are associated with better self-rated health. Compared to those without a high school degree, individuals with a high school degree with receive slightly more health returns to education with age (high school*age=0.99, 95% CI: 0.98-1.00). Further, health returns to increases in wealth diminish slightly with age. The reduction in the OR for race in Model 3 compared to Model 2 indicates that Black-White disparities in cross-sectional SES levels help to account for the Black-White gap in mean levels of self-rated health; however, inclusion of these measures does not reduce the race gap in the growth rate of self-rated health with age.
Model 4 of Table 3 includes measures of cumulative SES. Results reveal that long-term exposure to low income (OR=2.71, 95% CI: 2.18 – 3.38) and low wealth (OR=1.69; 95% CI: 1.37 – 2.09) have detrimental effects on self-rated health. On the other hand, long-term exposure to high income and high wealth are protective against poor self-rated health. Whereas the effects of long-term low income remain stable with age, the effect of long-term low wealth on self-rated health is magnified with age. Accounting for racial differences in long term SES in Model 4 reduces the Black-White disparity in both mean levels of self-rated health and the growth rate of the racial disparity with age over Models 1 and 2, the baseline models, and Model 3, which includes the point-in-time SES measures, suggesting that the cumulative SES measures are key determinants of the age patterning of racial disparities in self-rated health.
Model 5 includes both the point-in-time and cumulative SES measures and reveals that increases in education and wealth are protective against poor self-rated health. While the protective effects of education on health are stable across the life course, the protective effects of wealth wane slightly with age. Further, net of the income and wealth in any particular year, long-term exposure high income and wealth are protective against poor self-rated health, while long-term exposure to low income and wealth harm health. The effects of long-term low and high wealth on self-rated health are magnified with age. Compared to Models 3 and 4, which include the point-in-time and cumulative SES measures separately, the racial disparity in mean levels of self-rated health in Model 5 is greatly reduced in magnitude, suggesting that both the point-in-time and cumulative SES measures contribute to racial disparities in self-rated health.
Differential Returns to SES
Regarding the differential returns hypothesis, Model 3a suggests that, while education, income, and wealth are all protective against poor self-rated health, Blacks do not receive the same health returns to a college degree as Whites (Black*BA degree or higher=2.03, 95% CI: 1.07-3.84). Further, as they age, Blacks receive fewer health returns to having some college education than Whites. Consistent with Model 4, Model 4a reveals that persistent high income and wealth are protective against poor self-rated health, while persistent low income and wealth are detrimental for health. However, Blacks are less harmed by persistent low income than Whites, but receive fewer protective benefits from persistently high income than Whites (a gap that narrows with age). Further, as they age, Blacks are less harmed by persistent low wealth than Whites. Model 5a includes all of the SES measures and accounts for racial differences in health returns to both the point-in-time and cumulative SES measures. Consistent with Model 4a, Model 5a reveals that Blacks are less harmed by long-term exposure to low income (Black*persistent low income=0.45; 95% CI: 0.28-0.73) but receive less protection from long-term high income (Black*persistent high income=3.35, 95% CI: 1.34-8.37) than Whites, though these racial gaps narrow with age. Further, as they age, Blacks are less harmed by persistent low wealth than Whites.
Discussion
Given the persistence and magnitude of Black-White health disparities across time and space, understanding the social factors producing racial disparities in morbidity and mortality has been a focus of scientific inquiry for decades. A wide body of research documents that Black-White differences in socioeconomic well-being are key determinants of health inequities (Clarke et al. 2010; Franks et al. 2006; Geronimus et al. 2001; Hayward et al. 2000; Williams et al. 2010), yet understanding of the role of SES in the life course patterning of racial health inequities has been restricted by static measures of health and SES that mask both the dynamic nature of these processes and ignore the racialized nature of the SES-health connection. By modeling trajectories of Black-White health disparities using longitudinal data on multiple health outcomes and multi-dimensional measures of SES over time, this research advances understanding of the dynamics and determinants of racial health stratification across the life course.
This study offers four key contributions to the literature. First, this study improves understanding of the patterning and determinants of Black-White health inequities across the life course. To date, few studies have examined how racial disparities across multiple outcomes shift and change across the life course using longitudinal data (Brown, O'Rand, and Adkins 2012), leaving questions about the age patterning of health inequities unanswered. I document significant age variation in the magnitude sources of the Black-White health gap that varies by outcome and age—heterogeneity that is otherwise masked when examining singular health outcomes at one particular point in time. Across all of the BMI models presented in Table 2, the magnitude of the Black-White BMI disparity remains stable with age, offering evidence of the persistent inequality hypothesis. By contrast, results from all of the self-rated health models presented in Table 3 offer evidence of cumulative advantage, where the Black-White gap in self-rated health grows and diverges with age. While adjustment for point-in-time SES in Model 3, long-term SES in Model 4, and both dimensions of SES in Model 5 attenuated the Black-White health gap in mean levels of BMI and self-rated health, the racial disparity in self-rated health grew—at a rather uninterrupted rate—across the life course, even after full adjustment for SES. These results suggest that, whereas BMI trajectories may be established earlier in the life course, individuals' assessments of their own health may be particularly vulnerable to exposure to social conditions as they age. Despite the differences in the age trajectories of health inequity across the outcomes, results from this study suggest that intervening on population-level health disparities is most critical early in the life course, before these disparities emerge and, in the case of self-rated health, diverge with age.
Further, results from this study also indicate that the effects of various dimensions of SES on levels of health inequities also vary with age, contributing to the age patterning of health disparities. Across both outcomes, measures of education, wealth, and cumulative SES predicted mean levels of BMI and self-rated health. However, the protective effects of wealth on BMI and self-rated health declined slightly with age, while the harmful effects of persistent low income and—in the case of self-rated health—persistent low wealth diminished with age. These findings on the decreased power of socioeconomic factors to predict health in old age could be the result of various factors. For one, it may suggest that biological frailty in old age affects advantaged and disadvantaged populations similarly, such that socioeconomic resources are less protective from health declines in old age. The diminished effects of the SES measures in later life could also result from the availability of social insurance programs for older adults, including Social Security and Medicare, which may “level the playing field” in terms of reducing socioeconomic health disparities in late life (Brown, O'Rand, and Adkins 2012).
Second, results from this study suggest that point-in-time and long-term SES independently impact health and may capture different dimensions of socioeconomic well-being. For both outcomes, I find that adjusting for the point-in-time SES measures in Model 3 resulted in a significant reduction in the race gap in both BMI and self-rated health over the unadjusted models. Further, including the measures of long-term SES in Model 4 also produced a significant attention of the racial gap in both outcomes. However, the race gaps in BMI and self-rated health were smallest in Models 5 and 5a, when measures of both point-in-time and long-term SES were included. When both the point-in-time and long-term SES measures were included in Model 5, each set of SES indicators largely maintained their associations with BMI and self-rated health, net of one another. This finding suggests that the point-in-time and cumulative SES measures may reflect different dimensions of socioeconomic well-being and affect health through different mechanisms. Whereas cross-sectional income and wealth levels may afford individuals improved opportunities and health behaviors and reduced psychosocial stress in the short-term, the long-term measures capture duration of exposure to economic conditions. Compared to point-in-time measures of SES, measures of persistently low SES reflect the “weathering” effects (Geronimus 1992) of long-term economic deprivation, whereas measures of persistent high SES reflect the cumulative advantages and accumulation of health capital associated with long-term prosperity (Willson, Shuey, and Elder 2007). Findings regarding the unique contributions of the various SES measures to racial health disparities suggest that empirical studies must consider how the temporalization of SES and health, including how the timing and duration of exposures, impacts trajectories of well-being and inequality (Brown, O'Rand, and Adkins 2012; McDonough and Berglund 2003). Further, by documenting how health at any particular point is affected both by current SES and by past socioeconomic exposures, this study demonstrates the critical importance and centrality of the life course perspective to empirical studies of social stratification and health (Pavalko and Wilson 2011). In order to fully capture the role of SES in health disparities, studies must consider both current and past socioeconomic conditions. These findings also speak to the importance of interrupting patterns of long-term poverty and deprivation early in the life course, when the health effects of long-term socioeconomic disadvantage that emerge over time may be interrupted or reduced.
Third, this study finds that the health returns to various dimensions of SES are not equivalent across racial groups. In particular, analyses revealed that, compared to Whites, Blacks received less health returns to higher education, a gap that grew across the life course. Blacks also received less health protection from persistently income wealth than Whites. Figure 3 visually depicts how college educated Blacks, in particular, receive less protection against increases in BMI than Whites. As seen in Figure 3, while White BMI trajectories demonstrate a clear educational gradient, the BMI trajectories of Blacks who did not complete high school, who had a high school degree, and who had some college education are virtually indistinguishable from one another. Further, Blacks with a Bachelor's degree or higher have similar BMI trajectories to Whites who did not finish high school. These findings suggest that a combination of other factors, such as exposure to neighborhood economic disadvantage (Do et al. 2008; Williams and Collins 2001), experiences with racial discrimination (Bratter and Gorman 2011; Williams, Neighbors, and Jackson 2003), and stress associated with educational attainment and mobility (Pearson 2008), may prevent higher SES Blacks from achieving their fullest health potential relative to Whites and contribute the socioeconomic patterning of the Black health disadvantage. While the mechanisms producing differential returns to SES are not explored in present study, these findings document that failure to consider whether Blacks and Whites differentially benefit from increases in SES may result in misestimating the health effects of economic prosperity and upward mobility. Further, findings from this study suggest that policy and intervention efforts that aim to reduce Black-White health disparities by concentrating solely on improving individual socioeconomic opportunities will fall short in closing health gaps unless the psychosocial, contextual, and other factors driving racial health gaps are also addressed.
Figure 3. Age Trajectory of BMI by Race and Education (N=9,057).
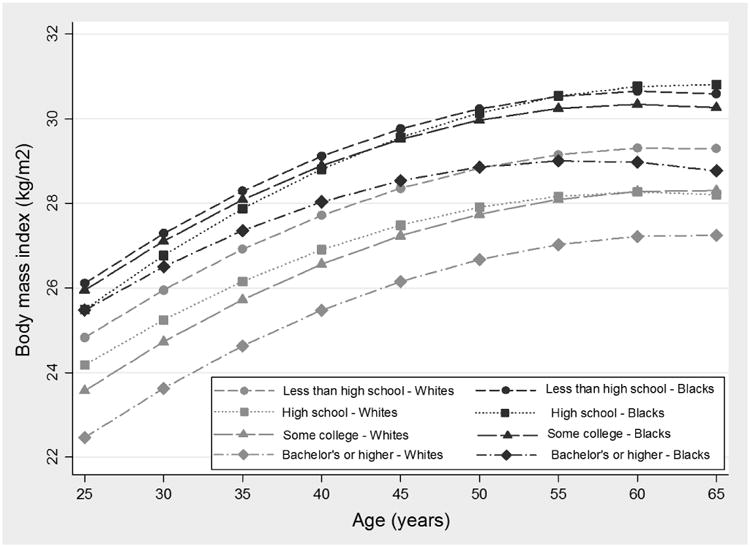
Note: Figure based on results from Model 5a (the fully adjusted model) of Table 1.
Finally, the findings presented here indicate that studies of racial health disparities that utilize single, cross-sectional measures of SES are subject to concerns about the residual confounding of race and SES. While adjusting for SES using point-in-time measures such as income, education, and wealth explained a portion of racial health gaps, these measures did not fully capture the role of SES in Black-White disparities in BMI and self-rated health. For both outcomes, mean racial health gaps were smallest in the fully adjusted models that included both the point-in-time and long-term SES were simultaneously included. This suggests that, by relying solely on cross-sectional measures of SES and failing to capture racial differences in long-term socioeconomic well-being, studies of racial health disparities risk overestimating the unexplained race residual and underestimating the role of SES in health inequity. This is not without implications. When studies “control” for SES using inadequate measures of socioeconomic well-being, they are left with significant “unexplained” racial differences in health. In turn, there has been a resurgence of studies directed towards uncovering other potential explanations for racial health gaps, including racial differences in genetics (see Roberts [2013] for a review). This return to a biological construction of race is troubling, given the evidence presented here and in other studies (e.g., Do, Frank, and Finch 2012; Kaufman et al. 1997; Pollack et al. 2007) that suggests that the role of social factors in racial health gaps has been largely underestimated. At the very least, findings from the present study indicate that socioeconomic factors are a primary driver of racial health inequities and that scholars should continue to develop and utilize nuanced and dynamic measures of life course SES in order to improve scientific understanding of racial health gaps.
This study is not without limitations. First, because of data limitations, respondents in this study are not observed until early adulthood, resulting in left censoring. As a result, findings presented here likely underestimate Black-White disparities in both SES and health, as Blacks are more likely to experience economic disadvantage and mortality in early life (Shuey and Willson 2008). Second, while this study focused on Black-White health disparities, future analyses should extend examinations to other racial and ethnic groups, as the social processes underlying the life course patterns of health inequity may vary (Brown, O'Rand, and Adkins 2012). Third, this study relies on self-reported health data. Future studies should consider the role of SES in racial disparities in more objective markers of health, including biomarkers of physiological well-being. Finally, though body mass index has been linked to increased risk of cardiovascular disease, cancer, and mortality (Kopleman 2007), research suggests that measures of abdominal adiposity, such as waist-to-hip ratio or waist circumference, may be independent, potentially stronger predictors of weight-related disease (Ashwell, Gunn, and Gibson 2012; Pischon et al. 2008). Future research should examine the linkages between race, SES, and indicators of abdominal obesity.
In sum, the present study raises several issues about the measurement and operationalization of health and SES in studies of racial health disparities. Findings from this study suggest that the role of SES in Black-White health gaps has been largely underestimated, in part because of empirical reliance on static measures of SES. The present study documents the critical importance of dynamic, cumulative measures of SES in driving age trajectories of racial health inequities across multiple outcomes. This study also documents that by failing to account for racial differences in returns to socioeconomic resources, previous studies may have overestimated the protective effects of SES for non-Whites, in particular. Beyond the empirical or methodological concerns outlined here, however, this study's findings regarding the unique and joint contributions of socioeconomic and non-socioeconomic factors to health disparities is of critical policy importance (LaVeist 2005; Pearson 2008). On the one hand, evidence suggests that racial health disparities could be greatly reduced by leveling the socioeconomic playing field. On the other hand, this study suggests that efforts to address socioeconomic inequality alone will not eliminate Black-White health gaps. Findings from this study document that socioeconomic differences between Blacks and Whites are critical—and largely underestimated—drivers of racial health inequities. I find that socioeconomic factors account for a more substantial portion of Black-White health gaps than has been previously estimated and urge future studies of racial health inequities to consider how multiple dimensions of short- and long-term socioeconomic well-being shape trajectories of health inequality. Findings from this study also suggest, however, that socioeconomic factors are not the only drivers of Black-White health gaps. Blacks do not receive the same health returns to increases in SES as Whites, and racial health gaps still exist—though in much smaller magnitude—after robust adjustment for SES. In this way, this study also provides support the notion that, when it comes to health, socioeconomic resources cannot “buy” Blacks all of the privileges, opportunities, and protections associated with whiteness (Pearson 2008). Consistent with Phelan and Link (2015), this study suggests that racism is a “fundamental cause” of racial disparities in health and disease, largely because of its role in producing stark racial disparities in SES. Still, in order to successfully advance racial health equity, policy and intervention efforts must consider how racism in the U.S. harms health both directly and indirectly through both economic and non-economic processes.
References
- Ashwell M, Gunn P, Gibson S. Waist to height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: systematic review and meta analysis. Obesity Reviews. 2012;13(3):275–86. doi: 10.1111/j.1467-789X.2011.00952.x. [DOI] [PubMed] [Google Scholar]
- Boen C, Yang YC. The physiological impacts of wealth shocks in late life: Evidence from the Great Recession. Social Science & Medicine. 2016;150:221–230. doi: 10.1016/j.socscimed.2015.12.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bond Huie SA, Krueger PM, Rogers RG, Hummer RA. Wealth, Race, and Mortality. Social Science Quarterly. 2003;84(3):667–84. [Google Scholar]
- Bratter JL, Gorman BK. Is discrimination an equal opportunity risk? Racial experiences, socioeconomic status, and health status among black and white adults. Journal of Health and Social Behavior. 2011;52(3):365–382. doi: 10.1177/0022146511405336. [DOI] [PubMed] [Google Scholar]
- Braveman P, Cubbin C, Egerter S, Chideya S, Marchi K, Metzler M, Posner S. Socioeconomic Status in Health Research: One Size Does Not Fit All. JAMA. 2005;294:2879–2888. doi: 10.1001/jama.294.22.2879. [DOI] [PubMed] [Google Scholar]
- Brown TH, O'Rand AM, Adkins DE. Race-Ethnicity and Health Trajectories: Tests of Three Hypotheses across Multiple Groups and Outcomes. Journal of Health and Social Behavior. 2012;53(3):359–77. doi: 10.1177/0022146512455333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bureau of Labor Statistics. Employment Status of the Civilian Population by Race, Sex, and Age. [Accessed October 30, 2012];2012 http://www.bls.gov/news.release/empsit.t02.htm.
- Chandola T, Jenkinson C. Validating Self-Rated Health in Different Ethnic Groups. Ethnicity and Health. 2000;5(2):151–9. doi: 10.1080/713667451. [DOI] [PubMed] [Google Scholar]
- Chen F, Yang Y, Liu G. Social Change and Socioeconomic Disparities in Health over the Life Course in China: A Cohort Analysis. American Sociological Review. 2010;75(1):126–50. doi: 10.1177/0003122409359165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clarke P, O'Malley P, Johnston L, Schulenberg J. Social disparities in BMI trajectories across adulthood by gender, race/ethnicity and lifetime socio-economic position: 1986–2004. Int J Epidemiol. 2009;38(2):499–509. doi: 10.1093/ije/dyn214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deaton AS, Paxson CH. Aging and Inequality in Income and Health. American Economic Review. 1998;88:248–53. [Google Scholar]
- DiPrete TA, Eirich GM. Cumulative Advantage as a Mechanism for Inequality: A Review of Theoretical and Empirical Developments. Annual Review of Sociology. 2006;32:271–97. [Google Scholar]
- Do DP. The dynamics of income and neighborhood context for population health: Do long-term measures of socioeconomic status explain more of the black/white health disparity than single-point-in-time measures? Social Science and Medicine. 2009;68:1368–75. doi: 10.1016/j.socscimed.2009.01.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Do DP, Finch BK, Basurto-Davila R, Bird C, Escarce J, Lurie N. Does place explain racial health disparities? Quantifying the contribution of residential context to the Black/white health gap in the United States. Social Science and Medicine. 2008;67(8):1258–68. doi: 10.1016/j.socscimed.2008.06.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Do DP, Frank R, Finch BK. Does SES explain more of the black/white health gap than we thought? Revisiting our approach toward understanding racial disparities in health. Social Science and Medicine. 2012;74:1385–93. doi: 10.1016/j.socscimed.2011.12.048. [DOI] [PubMed] [Google Scholar]
- DuBois WEB. The Philadelphia Negro: A Social Study. Philadelphia, PA: University of Pennsylvania; 1899. [Google Scholar]
- Duncan G. The volatility of family income over the life course. In: Bates P, Featherman D, Lerner R, editors. Life Span Development and Behavior. Vol. 9. Hillsdale, NJ: Lawrence Erlbaum Assoc; 1988. pp. 317–58. [Google Scholar]
- Dupre ME. Educational Differences in Age-Related Patterns of Disease: Reconsidering Cumulative Advantage and Age-as-Leveler. Journal of Health and Social Behavior. 2007;48(1):1–15. doi: 10.1177/002214650704800101. [DOI] [PubMed] [Google Scholar]
- Elo IT. Social class differentials in health and mortality: Patterns and explanations in comparative perspective. Annual Review of Sociology. 2009;35:553–572. [Google Scholar]
- Farmer M, Ferraro K. Are Racial Disparities in Health Conditional on Socioeconomic Status? Social Science and Medicine. 2005;60:191–204. doi: 10.1016/j.socscimed.2004.04.026. [DOI] [PubMed] [Google Scholar]
- Ferraro K, Farmer M. Double Jeopardy, Aging as Leveler, or Persistent Inequality? A Longitudinal Analysis of White and Black Americans. Journals of Gerentology: Social Sciences. 1996;51B(6):S319–28. doi: 10.1093/geronb/51b.6.s319. [DOI] [PubMed] [Google Scholar]
- Ferraro K, Kelley-Moore J. Cumulative Disadvantage and Health: Long-Term Consequences of Obesity? American Sociological Review. 2003;68:707–29. [PMC free article] [PubMed] [Google Scholar]
- Franks P, Muenning P, Lubetkin E, Jia H. The burden of disease associated with being African-American in the United States and the contribution of socio-economic status. Social Science and Medicine. 2006;62:2469–78. doi: 10.1016/j.socscimed.2005.10.035. [DOI] [PubMed] [Google Scholar]
- Geronimus AT. The weathering hypothesis and the health of African-American women and infants: evidence and speculations. Ethnicity and Disease. 1992;2(3):207–21. [PubMed] [Google Scholar]
- Geronimus AT, Bound J, Waidmann TA, Colen CG, Steffick D. Inequality in Life Expectancy, Functional Status, and Active Life Expectancy across Selected Black and White Populations in the United States. Demography. 2001;38(2):227–51. doi: 10.1353/dem.2001.0015. [DOI] [PubMed] [Google Scholar]
- Grieger L, Wyse J. The Growing Racial Divide in US Children's Long-Term Poverty at the End of the Twentieth Century. Ann Arbor, MI: Population Studies Center; 2008. [Google Scholar]
- Glymour M, Avendaño S Haas, Berkman L. Lifecourse social conditions and racial disparities in incidence of first stroke. Annals of Epidemiology. 2008;18(12):904–12. doi: 10.1016/j.annepidem.2008.09.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haas S, Krueger P, Rohlfsen L. Race/ethnic and nativity disparities in later life physical performance: the role of health and socioeconomic status over the life course. Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2012;67(2):238–48. doi: 10.1093/geronb/gbr155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haas S, Rohlfsen L. Life course determinants of racial and ethnic disparities in functional health trajectories. Social science & medicine. 2010;70(2):240–50. doi: 10.1016/j.socscimed.2009.10.003. [DOI] [PubMed] [Google Scholar]
- Hajat A, Kaufman JS, Rose KM, Siddiqi A, Thomas JC. Do the wealthy have a health advantage? Cardiovascular disease risk factors and wealth. Social Science and Medicine. 2010;71(11):1935–1942. doi: 10.1016/j.socscimed.2010.09.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hajat A, Kaufman JS, Rose KM, Siddiqi A, Thomas JC. Long-term effects of wealth on mortality and self-rated health status. American Journal of Epidemiology. 2011;173(2):192–200. doi: 10.1093/aje/kwq348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayward M, Miles T, Crimmins E, Yang Y. The Significance of Socioeconomic Status in Explaining the Racial Gap in Chronic Health Conditions. American Sociological Review. 2000;65(6):910–930. [Google Scholar]
- House J, Herd P, Lantz P. Continuity and Change in Social Stratification of Aging and Health over the Life Course: Evidence from a Nationally Representative Longitudinal Study from 1988-2001/2002. Journals of Gerontology: Social Sciences. 2005;60(S2):15–26. doi: 10.1093/geronb/60.special_issue_2.s15. [DOI] [PubMed] [Google Scholar]
- House JS, Lepkowski JM, Kinney AM, Mero RP, Kessler RC, Herzog AR. The Social Stratification of Aging and Health. Journal of Health and Social Behavior. 1994;35(3):213–234. [PubMed] [Google Scholar]
- Iceland J. Current Population Reports, 70-91. Washington, D.C: US Census Bureau; 2003. Dynamics of Economic Well-Being, Poverty 1996-1999. [Google Scholar]
- Idler E, Benyamini Y. Self-Rated Health and Mortality: A Review of Twenty-Seven Community Studies. Journal of Health and Social Behavior. 1997;35:21–37. [PubMed] [Google Scholar]
- Institute for Social Research. PSID Main Interview User Manual: Release 2015. Ann Arbor: University of Michigan; 2015. [Google Scholar]
- Kaufman JS, Cooper RS, Mc Gee DL. Socioeconomic Status and Health in Blacks And Whites: The Problem of Residual Confounding and the Resiliency of Race. Epidemiology. 1997;8(6):621–628. [PubMed] [Google Scholar]
- Kim J, Miech R. The Black-White Difference in Age Trajectories of Functional Health over the Life Course. Social Science and Medicine. 2009;68(4):717–725. doi: 10.1016/j.socscimed.2008.12.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kopelman P. Health risks associated with overweight and obesity. Obesity Reviews. 2007;8(S1):13–17. doi: 10.1111/j.1467-789X.2007.00311.x. [DOI] [PubMed] [Google Scholar]
- Krieger N, Williams DR, Moss NE. Measuring Social Class in Public Health Research: Concepts, Methodologies, and Guidelines. Annual Review of Public Health. 1997;18:341–78. doi: 10.1146/annurev.publhealth.18.1.341. [DOI] [PubMed] [Google Scholar]
- Land KC, Russell ST. Wealth accumulation across the adult life course: stability and change in sociodemographic covariate structures of net worth data in the Survey of Income and Program Participation, 1984–1991. Social Science Research. 1996;254:423–62. doi: 10.1006/ssre.1996.0019. [DOI] [PubMed] [Google Scholar]
- LaVeist T. Disentangling race and socioeconomic status: a key to understanding health inequalities. J Urban Health. 2005;82.2(3):iii26–iii34. doi: 10.1093/jurban/jti061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Link B, Phelan J. Social Conditions as a Fundamental Cause of Disease. Journal of Health and Social Behavior. 1995;35:80–94. [PubMed] [Google Scholar]
- McDonough P, Amick BC. The social context of health selection: a longitudinal study of health and employment. Social Science and Medicine. 2001;53(1):135–145. doi: 10.1016/s0277-9536(00)00318-x. [DOI] [PubMed] [Google Scholar]
- McDonough P, Berglund P. Histories of poverty and self-rated health trajectories. Journal of Health and Social Behavior. 2003:198–214. [PubMed] [Google Scholar]
- Murphy SL, Xu J, Kochanek KD, K D. Deaths: Final Data for 2010. National Vital Statistics Reports. 2013;60(4) [PubMed] [Google Scholar]
- National Cancer Institute. National Institutes of Health. [Accessed 7 April 2012];Cancer Health Disparities. 2006 http://www.cancer.gov/cancertopics/factsheet/disparities/cancer-health-disparities#statistics.
- Pavalko E, Willson A. Life Course Approaches to Health, Illness, and Healing. In: Pescolido BA, editor. Handbook of the Sociology of Health, Illness, and Healing. Springer; 2011. [Google Scholar]
- Pearson JA. Can't buy me Whiteness. Du Bois Review: Social Science Research on Race. 2008;5(01):27–47. [Google Scholar]
- Pfeffer FT, Danziger S, Schoeni RF. Wealth Disparities before and after the Great Recession. The ANNALS of the American Academy of Political and Social Science. 2013;650(1):98–123. doi: 10.1177/0002716213497452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Phelan J, Link B. Is Racism a Fundamental Cause of Inequalities in Health? Annual Review of Sociology. 2015;41(1):311–330. [Google Scholar]
- Pischon T, et al. General and abdominal adiposity and risk of death in Europe. New England Journal of Medicine. 2008;359(20):2105–20. doi: 10.1056/NEJMoa0801891. [DOI] [PubMed] [Google Scholar]
- Pollack C, Chideya S, Cubbin C, Williams B, Dekker M, Braveman P. Should Health Studies Measure Wealth? A Systematic Review. American Journal of Preventive Medicine. 2007;33(3):250–264. doi: 10.1016/j.amepre.2007.04.033. [DOI] [PubMed] [Google Scholar]
- Rank MR, Hirschl TA. The Likelihood of Poverty across the American Adult Life Span. Social Work. 1999;44:201–16. [Google Scholar]
- Rank MR, Hirschl TA. Rags or riches: estimating the probabilities of poverty and affluence across the adult American life span. Social Science Quarterly. 2001;82:651–69. [Google Scholar]
- Raudenbush S, Bryk A. Hierarchical Linear Models: Applications and Data Analysis Methods. Sage; 2002. [Google Scholar]
- Robert S, House JS. SES Differentials in Health by Age and Alternative Indicators of SES. Journal of Aging and Health. 1996;8(3):359–88. doi: 10.1177/089826439600800304. [DOI] [PubMed] [Google Scholar]
- Roberts D. Fatal invention: How science, politics, and big business re-create race in the twenty-first century. The New Press; 2013. [Google Scholar]
- Shaw BA, Krause N. The Impact of Salient Role Stress on Trajectories of Health in Late Life among Survivors of a Seven-Year Panel Study: Analyses of Individual Growth Curves. International Journal of Aging and Human Development. 2002;52:97–116. doi: 10.2190/RBH7-6P1R-LKQH-E9YR. [DOI] [PubMed] [Google Scholar]
- Shuey K, Willson A. Cumulative Disadvantage and Black-White Disparities in Life-Course Health Trajectories. Research on Aging. 2008;30(2):200–225. [Google Scholar]
- Singer J, Willet J. Applied Longitudinal Analysis: Modeling Change and Event Occurrence. NY: Oxford University Press; 2003. [Google Scholar]
- Smith JP. Healthy bodies and thick wallets: the dual relation between health and economic status. The journal of economic perspectives: a journal of the American Economic Association. 1999;3(2):144. [PMC free article] [PubMed] [Google Scholar]
- Stevens AH. Climbing out of Poverty, Falling Back in: Measuring the Persistence of Poverty over Multiple Spells. Journal of Human Resources. 1999;34(3):557–88. [Google Scholar]
- Sweet E, Nandi A, Adam EK, McDade TW. The high price of debt: Household financial debt and its impact on mental and physical health. Social Science and Medicine. 2013;91:94–100. doi: 10.1016/j.socscimed.2013.05.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taylor P, Kochhar R, Fry R, Velasco G, Motel S. Twenty-to-One: Wealth Gap Rises to Record Highs between Whites, Blacks, and Hispanics. Washington, DC: Pew Research Center; 2011. [Google Scholar]
- U.S. Census Bureau. Educational Attainment by Race and Hispanic Origin: 1970-2010. [Accessed October 30, 2012];2012a http://www.census.gov/compendia/statab/2012/tables/12s0229.pdf.
- U.S. Census Bureau. People Below Poverty Level and Below 125 Percent of Poverty Level by Race and Hispanic Origin: 1980 to 2009. [Accessed October 30, 2012];2012b http://www.census.gov/compendia/statab/2012/tables/12s0711.pdf.
- Williams D, Collins C. US Socioeconomic and Racial Differences in Health: Patterns and Explanations. Annual Review of Sociology. 1995;21:349–386. [Google Scholar]
- Williams DR, Collins C. Racial residential segregation: a fundamental cause of racial disparities in health. Public Health Reports. 2001;116(5):404. doi: 10.1093/phr/116.5.404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams DR, Neighbors HW, Jackson JS. Racial/ethnic discrimination and health: findings from community studies. American Journal of Public Health. 2003;93(2):200–8. doi: 10.2105/ajph.93.2.200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams D, Mohammed SA, Leavell J, Collins C. Race, Socioeconomic Status, and Health: Complexities, Ongoing Challenges, and Research Opportunities. Annals of the New York Academy of Sciences. 2010;1186(1):69–101. doi: 10.1111/j.1749-6632.2009.05339.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Willson A, Shuey K, Elder G. Cumulative Advantage Processes as Mechanisms of Inequality in Life Course Health. American Journal of Sociology. 2007;112(6):1886–1924. [Google Scholar]
- Wilson G. Racialized Life-Chance Opportunities across the Class Structure: The Case of African Americans. Annals of the American Academy of Political and Social Science. 2007;609:215–232. [Google Scholar]
- Yang Y, Land KC. Age-period-cohort analysis: new models, methods, and empirical applications. CRC Press; 2013. [Google Scholar]
- Yang Y, Lee LC. Sex and race disparities in health: Cohort variations in life course patterns. Social Forces. 2009;87(4):2093–2124. [Google Scholar]
- Zajacova A, Burgard SA. Healthier, wealthier, and wiser: A demonstration of compositional changes in aging cohorts due to selective mortality. Population Research and Policy Review. 2013;32(3):311–24. doi: 10.1007/s11113-013-9273-x. [DOI] [PMC free article] [PubMed] [Google Scholar]