

Abstract
Various techniques for piriformis muscle release have been published previously. However, it is imperative we continue to improve on existing techniques as well as develop new ones that may further optimize outcomes. Therefore, we aimed to describe an endoscopic technique for the release of the piriformis muscle in those with symptoms of sciatic nerve compression. Using the posterolateral portal, we are able to perform a complete release of the piriformis from the greater trochanter and the piriformis fossa with care to protect the external rotators and the sciatic nerve. It is our belief that this technique can be easily replicated by practitioners who read this technical note.
The piriformis functions in the abduction and external rotation of the hip during its flexion. Because it is dorsal to the sciatic nerve, the contraction of the piriformis may lead to severe pain that radiates down one or both of the lower extremities.1 This is commonly referred to as piriformis syndrome. In addition, these patients may complain of an inability to sit for longer than 30 minutes and paresthesias of the lower extremities.1 There are a number of causes of this condition such as muscular hypertrophy, history of trauma to the hip or pelvis, or anatomical abnormalities.2, 3, 4, 5 There are a number of conservative measures such as injections, medications, and physical therapy that may be used to manage these patients.6, 7, 8
Despite these conservative measures, some patients may eventually require a surgical release of the muscle to decompress the nerve and provide marked pain relief.8 Various techniques for piriformis muscle release have been published previously.2, 9, 10 Although very few complications and satisfactory outcomes have been observed in previous studies, there is some concern that current techniques do not allow for an optimal visualization of the sciatic nerve.10, 11 Hence, it is imperative we continue to improve on existing techniques as well as develop new ones that may further optimize outcomes. Therefore, we aimed to describe an endoscopic technique for the release of the piriformis muscle in those with symptoms of sciatic nerve compression (Video 1).
Surgical Technique
Step 1: Preparation and Portal Creations
The patient is placed in the lateral position using a bean bag. The greater trochanter is palpated, and the standard posterolateral (PL) and accessory lateral portals are then created (Fig 1). The PL portal is used for the arthroscopic camera at 30° and the accessory lateral portal is used for electrocautery and vapor (Crossfire Arthroscopic Resection System; Stryker Orthopedics, Mahwah, NJ).
Fig 1.
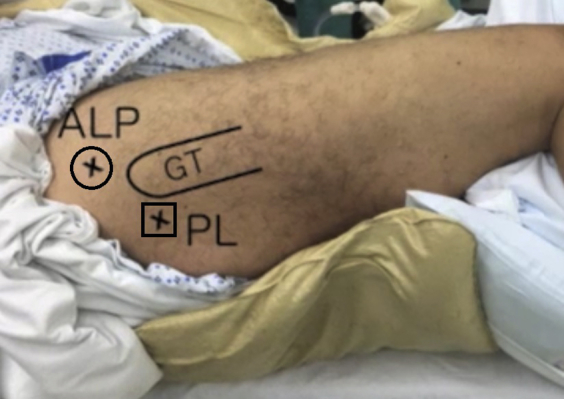
The patient is placed in the lateral position using a bean bag. The greater trochanter is then identified and the posterolateral and accessory lateral portals are marked using a surgical marker and created. (ALP, accessory lateral portal; GT, greater trochanter; PL, posterolateral.)
Step 2: Bursectomy
The trochanteric bursa is identified using the camera within the PL portal, and a bursectomy is performed via the accessory portal using the standard arthroscopic technique to expose the external rotators and the piriformis (Fig 2). The dissection is then carried out medially to expose the sciatic nerve with adhesive bands dissected off proximally and distally.
Fig 2.

A bursectomy is being performed using electrocautery to expose the short external rotators and the piriformis. The dissection is carried out medially to expose the sciatic nerve with adhesive bands dissected off proximally and distally.
Step 3: Identify and Isolate the Piriformis
From the view of the camera within the PL portal, we then are able to identify the piriformis tendon as it courses proximal to the muscular portion of the short external rotators (Fig 3).
Fig 3.
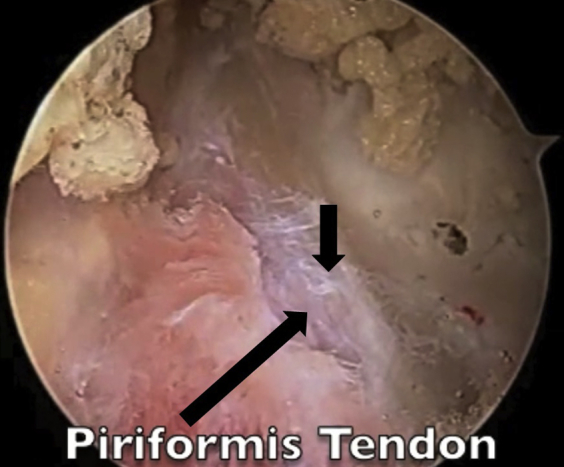
The piriformis tendon has been identified proximal to the muscular portion of the short external rotators after a complete bursectomy.
Step 4: Follow Course of the Sciatic Nerve and Perform Neurolysis
Using cautery, the piriformis tendon is isolated. The sciatic nerve is then identified as it courses near the piriformis using the camera within the PL portal. The bursectomy is then continued using electrocautery and vapor via the accessory portal to allow for complete visualization of the nerve proximally and distally (Fig 4). The proximal and distal portions of the sciatic nerve are released for the complete visualization of the course of the nerve (Figs 5 and 6).
Fig 4.

The sciatic nerve has been sufficiently exposed by releasing the nerve both proximally and distally.
Fig 5.

A proximal neurolysis is performed to identify the complete course of the sciatic nerve.
Fig 6.

A distal neurolysis is performed to identify the complete course of the sciatic nerve.
Step 5: Complete Release of the Piriformis Muscle
Once the proximal and distal portions of the sciatic nerve have been completely isolated, the piriformis muscle is released off the piriformis fossa and the greater trochanter using electrocautery via the accessory portal (Fig 7). Care is taken to perform a complete release so as to allow the tendon to heal at a lengthened position, and thus decrease the chances of the recurrence of sciatic nerve entrapment due to piriformis syndrome (Fig 8). Complete visualization of the release is performed using a 30° camera within the PL portal. Refer to Table 1 for pearls and pitfalls regarding each step.
Fig 7.

The piriformis is completely released off the piriformis fossa and the greater trochanter using electrocautery. Care is taken to perform a complete release so as to allow the tendon to heal at a lengthened position to decrease the chances of recurrence of sciatic nerve entrapment.
Fig 8.

A completed piriformis muscle release.
Table 1.
Pearls and Pitfalls for Each Step of the Technique
| Step | Description | Pearls and Pitfalls |
|---|---|---|
| 1 | Create a standard posterolateral portal and the accessory lateral portal for visualization and electrocautery, respectively | – |
| 2 | Perform a bursectomy | Continue until the piriformis and the short external rotators are identified |
| 3 | Identify and isolate the piriformis tendon | Avoid damage to the short external rotators because they are distal to the piriformis |
| 4 | Identify the sciatic nerve and perform a complete neurolysis of the proximal and distal portions of the nerve | Ensure completed bursectomy before proceeding with neurolysis to allow complete visualization |
| 5 | Release the piriformis muscle off the piriformis fossa and the greater trochanter | If the release is not complete, there is a higher risk of recurrence of piriformis syndrome |
Discussion
Piriformis syndrome is a rare condition with numerous potential causes leading to compression of the sciatic nerve that may eventually require decompression through the release of the muscle. Although other techniques have shown satisfactory results with a low incidence of complications, we find it imperative to be able to follow the course of the sciatic nerve to ensure a safe and complete release of the muscle (see Table 2 for advantages and disadvantages of the techniques). Therefore, we have presented our surgical technique that allows for decompression of the sciatic nerve by the release of the piriformis while identifying the course of the sciatic nerve.
Table 2.
Advantages and Disadvantages of Our Technique Versus the Standard Technique
| Technique | Advantages | Disadvantages |
|---|---|---|
| Our technique | • Smaller incision • Less dissection required to gain good visualization of the sciatic nerve • Decreased blood loss • Decreased postoperative pain |
• Harder to ensure full bursectomy • Theoretical increased risk of damage to short external rotators |
| Conventional open | • Full visualization of the sciatic nerve • Full visualization of the bursa during bursectomy |
• Larger incision • Increased blood loss • Increased postoperative pain • More dissection required for complete visualization of the sciatic nerve |
Although not commonly studied, there are 2 small studies that have evaluated the efficacy of piriformis release. Most recently, Park et al.11 evaluated the clinical outcomes of arthroscopic sciatic nerve decompression (n = 60 hips). After a mean 24-month follow-up (range, 24-38 months), they reported that 88% (n = 53) of patients were satisfied with their outcomes and there were no postoperative complications. Similarly, Martin et al.10 evaluated a series of patients who were released endoscopically (n = 35). After a mean follow-up of 12 months (range, 6-24 months), the mean modified Harris Hip Scores improved substantially (54 to 78 points). In addition, they reported markedly less pain according to the visual analog scale (7 to 2 points). Hence, these 2 studies show that piriformis release can offer great benefit to patients whose condition is refractory to conservative measures.
In conclusion, our arthroscopic surgical technique represents a viable option for those who require the surgical release of their piriformis muscle. It is our belief that this technique can be easily replicated by practitioners who read this technical note. However, future studies should focus on the outcomes of arthroscopic surgical techniques such as ours that attempt to maximize efficacy while minimizing the risk of complications.
Footnotes
The authors report the following potential conflict of interest or source of funding: T.P.P. receives support from Shaklee. V.K.M. receives support from MD Advantage; he is also a board member of New Jersey Orthopaedic Society. A.J.S. receives support from MD Advantage and Mitek.
Supplementary Data
The patient is placed in the right lateral decubitus position using a bean bag. Both anterior accessory and posterolateral portals (PLP) are marked and created. Using electrocautery via the accessory portal and with the camera within the PLP, a bursectomy is performed to appropriately expose the piriformis as well as the short external rotators. Once the bursectomy is complete, the sciatic nerve is then appropriately identified and a proximal and distal neurolysis are performed (with the camera remaining within the PLP and instruments within the accessory portal). Once the course of the sciatic nerve has been completely identified, a full release of the piriformis is performed using electrocautery.
References
- 1.Hopayian K., Song F., Riera R., Sambandan S. The clinical features of the piriformis syndrome: A systematic review. Eur Spine J. 2010;19:2095–2109. doi: 10.1007/s00586-010-1504-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Benson E.R., Schutzer S.F. Posttraumatic piriformis syndrome: Diagnosis and results of operative treatment. J Bone Joint Surg Am. 1999;81:941–949. [PubMed] [Google Scholar]
- 3.Benzon H.T., Katz J.A., Benzon H.A., Iqbal M.S. Piriformis syndrome: Anatomic considerations, a new injection technique, and a review of the literature. Anesthesiology. 2003;98:1442–1448. doi: 10.1097/00000542-200306000-00022. [DOI] [PubMed] [Google Scholar]
- 4.Kraus E., Tenforde A.S., Beaulieu C.F., Ratliff J., Fredericson M. Piriformis syndrome with variant sciatic nerve anatomy: A case report. PMR. 2016;8:176–179. doi: 10.1016/j.pmrj.2015.09.005. [DOI] [PubMed] [Google Scholar]
- 5.Natsis K., Totlis T., Konstantinidis G.A., Paraskevas G., Piagkou M., Koebke J. Anatomical variations between the sciatic nerve and the piriformis muscle: A contribution to surgical anatomy in piriformis syndrome. Surg Radiol Anat. 2014;36:273–280. doi: 10.1007/s00276-013-1180-7. [DOI] [PubMed] [Google Scholar]
- 6.Jabbari B., Machado D. Treatment of refractory pain with botulinum toxins—An evidence-based review. Pain Med. 2011;12:1594–1606. doi: 10.1111/j.1526-4637.2011.01245.x. [DOI] [PubMed] [Google Scholar]
- 7.Santamato A., Micello M.F., Valeno G. Ultrasound-guided injection of botulinum toxin type A for piriformis muscle syndrome: A case report and review of the literature. Toxins (Basel) 2015;7:3045–3056. doi: 10.3390/toxins7083045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Masala S., Crusco S., Meschini A., Taglieri A., Calabria E., Simonetti G. Piriformis syndrome: Long-term follow-up in patients treated with percutaneous injection of anesthetic and corticosteroid under CT guidance. Cardiovasc Intervent Radiol. 2012;35:375–382. doi: 10.1007/s00270-011-0185-z. [DOI] [PubMed] [Google Scholar]
- 9.Dezawa A., Kusano S., Miki H. Arthroscopic release of the piriformis muscle under local anesthesia for piriformis syndrome. Arthroscopy. 2003;19:554–557. doi: 10.1053/jars.2003.50158. [DOI] [PubMed] [Google Scholar]
- 10.Martin H.D., Shears S.A., Johnson J.C., Smathers A.M., Palmer I.J. The endoscopic treatment of sciatic nerve entrapment/deep gluteal syndrome. Arthroscopy. 2011;27:172–181. doi: 10.1016/j.arthro.2010.07.008. [DOI] [PubMed] [Google Scholar]
- 11.Park M.S., Yoon S.J., Jung S.Y., Kim S.H. Clinical results of endoscopic sciatic nerve decompression for deep gluteal syndrome: Mean 2-year follow-up. BMC Musculoskelet Disord. 2016;17:218. doi: 10.1186/s12891-016-1062-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The patient is placed in the right lateral decubitus position using a bean bag. Both anterior accessory and posterolateral portals (PLP) are marked and created. Using electrocautery via the accessory portal and with the camera within the PLP, a bursectomy is performed to appropriately expose the piriformis as well as the short external rotators. Once the bursectomy is complete, the sciatic nerve is then appropriately identified and a proximal and distal neurolysis are performed (with the camera remaining within the PLP and instruments within the accessory portal). Once the course of the sciatic nerve has been completely identified, a full release of the piriformis is performed using electrocautery.