

Abstract
Background
Breast cancer is the leading cause of cancer deaths among women in the Caribbean and accounts for >1 million disability adjusted life years. Little is known about the social inequalities of this disease in the Caribbean. In support of the Rio Political Declaration on addressing health inequities, this article presents a systematic review of evidence on the distribution, by social determinants, of breast cancer risk factors, frequency, and adverse outcomes in Caribbean women.
Methods
MEDLINE, EMBASE, SciELO, CINAHL, CUMED, LILACS, and IBECS were searched for observational studies reporting associations between social determinants and breast cancer risk factors, frequency, or outcomes. Based on the PROGRESS-plus checklist, we considered 8 social determinant groups for 14 breast cancer endpoints, which totalled to 189 possible ways (‘relationship groups’) to explore the role of social determinants on breast cancer. Studies with >50 participants conducted in Caribbean territories between 2004 and 2014 were eligible for inclusion. The review was conducted according to STROBE and PRISMA guidelines and results were planned as a narrative synthesis, with meta-analysis if possible.
Results
Thirty-four articles were included from 5,190 screened citations. From these included studies, 75 inequality relationships were reported examining 30 distinct relationship groups, leaving 84% of relationship groups unexplored. Most inequality relationships were reported for risk factors, particularly alcohol and overweight/obesity which generally showed a positive relationship with indicators of lower socioeconomic position. Evidence for breast cancer frequency and outcomes was scarce. Unmarried women tended to have a higher likelihood of being diagnosed with breast cancer when compared to married women. While no association was observed between breast cancer frequency and ethnicity, mortality from breast cancer was shown to be slightly higher among Asian-Indian compared to African-descent populations in Trinidad (OR 1.2, 95% CI 1.1–1.4) and Guyana (OR 1.3, 95% CI 1.0–1.6).
Conclusion
Study quantity, quality, and variability in outcomes and reporting limited the synthesis of evidence on the role of social determinants on breast cancer in the Caribbean. This report represents important current evidence on the region, and can guide future research priorities for better describing and understanding of Caribbean breast cancer inequalities.
Electronic supplementary material
The online version of this article (doi:10.1186/s12939-017-0540-z) contains supplementary material, which is available to authorized users.
Background
Among females in the Caribbean, breast cancer was the leading cause of cancer deaths, and accounted for 1.4 million disability adjusted life years (DALYs) in 2013 [1–3]. Age-standardized breast cancer mortality rates in the Caribbean have shown a 37% increase to 20.6 per 100,000 since 1990; this is in contrast to the decrease seen among many industrialised countries [1, 2].
Despite this high regional burden, little is known about the social distribution of breast cancer incidence and outcomes within the Caribbean. Internationally, social inequalities in breast cancer burden and outcomes are evident, such as by race and education [4–8]. Examining whether there are differences among populations groups, and determining their basis, can guide policy towards improving outcomes.
In 2007, the Port of Spain Declaration was affirmed by Caribbean Community (CARICOM) Heads of Government, aimed at the prevention and control of non-communicable diseases (NCDs), and there is an ongoing progress evaluation of political responses to this commitment [9, 10]. The World Health Organization (WHO) Commission on the Social Determinants of Health (CSDH) has highlighted the role of health research in understanding health inequalities and inequities, and through the 2011 Rio Political Declaration, countries have committed to monitoring, understanding and addressing health inequities [11, 12]. These agreements have set the scene for efforts to understand the social drivers of chronic disease, including cancers.
To date, there has been no published systematic review of research evidence on the social determinants of breast cancer among Caribbean populations. This systematic review is guided by the analytical framework to examine social determinants of disease by the WHO CSDH [13]. This review uses a simplified version of the framework to answer the primary research question: what is the distribution, by known social determinants of health, of the risk factors, frequency, and adverse outcomes of breast cancer among female populations living in the Caribbean?
Methods
Full details of the review methodology are available in the study protocol (see Additional File 1). The protocol was guided by a previous systematic review of social determinants of diabetes [14] and an initial scoping review of the social determinants of breast cancer.
Eligibility criteria
Observational studies were sought that reported relationships between a social determinant and known risk factors for breast cancer (alcohol intake, overweight/obesity, infrequent breastfeeding, physical inactivity, dietary sugar, ionizing radiation, late age at first pregnancy, and low parity), disease frequency (incidence or prevalence), or disease outcomes (cancer stage at diagnosis, cancer grade at diagnosis, recurrence, survival, mortality). Articles written in the dominant Caribbean languages (English, Spanish, French, and Dutch) were sought from 32 Caribbean territories. Included studies drew upon samples from either the general population or from healthcare facility catchments. No age restrictions were used in determining study eligibility. Sample sizes ≤50 were excluded as unlikely to be representative of underlying populations. Risk factors were identified using three compendiums of evidence-based information: The Global Burden of Disease Consortium, UpToDate, and Cancer Epidemiology and Control [15–17]. Articles presenting risk factor data from a sample of combined genders or males only were excluded so as to more accurately represent the risk factor profile in females. The selection of social determinants was guided by the extension of the PRISMA statement for the transparent reporting of systematic reviews and meta-analyses with a focus on health equity, which recommends the “PROGRESS-Plus” checklist: place of residence, race or ethnicity (alternatively culture or language), occupation, gender, religion, education, socio-economic position (SEP), and social capital [18]. Age was not examined as a social determinant for overweight/obesity and breast cancer frequency and outcomes due to its biological associations with these variables. Reports published between January 2004 and December 2014 were considered for inclusion. This 10-year period was selected as relevant to the current situation and able to inform policy response as it is taking place within the context of a major review of regional and national policy responses in the Caribbean to NCDs [10].
Search strategy, study selection, data extraction
The databases searched were: MEDLINE (via Pubmed); EMBASE (via Ovid); SciELO; CINAHL (via EBSCO); CUMED, LILACS, and IBECS (via WHO Virtual Health Library) [19–23]. The final search was conducted in February 2015. The search strategies are detailed in a supplementary file (See Additional File 2). Search results were maintained in Endnote reference management software [24].
Study selection and data abstraction were undertaken in duplicate by two independent reviewers (CB, SH); any inconsistencies were resolved by a third reviewer (NS-G). Study selection was conducted in two stages. First, titles and abstracts were screened to identify potentially relevant articles; second, full-text screening of potentially relevant articles identified articles for inclusion in the review. If inadequate information was available for decision-making in the first stage, the article automatically progressed to full-text review. In addition to those not meeting the inclusion criteria, 10 articles were either inaccessible or awaiting publication [25–34]. With guidance by the STROBE statement on strengthening the reporting of observational studies in epidemiology and the PRISMA-Equity statement [35, 36], an electronic data abstraction form was created in the REDCap database (see Additional file 1) [37].
Risk of bias assessment
Risk of bias was assessed using a tool adapted from STROBE and Cochrane ACROBAT-NRSi guidelines (see Additional file 1) [35, 38]. Bias was assessed at the relationship level across 5 domains: confounding (was control for known and potential confounders adequate?); participant selection (is the sample representative of the target population?); missing data (is the data reasonably complete?); outcome measurement (is a social determinant/risk factor/disease endpoint appropriately measured?); selective reporting (is a relationship selectively reported?). Articles were classified as having serious, moderate, low, or unclear risk of bias. Two reviewers (CB, NS-G) made an independent judgement on the overall risk of bias of each included article, considering each domain as equally important and also the direction and magnitude of the bias from each domain. Discrepancies were discussed by the two reviewers to achieve consensus.
Synthesis of results
The review was planned as a narrative synthesis with supplementary meta-analysis if possible. Key study details were presented, followed by a description of associations between a social determinant and either a risk factor, a measure of disease frequency, or a measure of disease outcomes. The number and type of inequality relationships were summarised in an ‘evidence gap map’ – a visual tool to highlight the current evidence on the known social determinants of breast cancer in the Caribbean and a guide for focusing future research [39]. Meta-analysis of quantitative evidence was planned for inequality relationships reported by ≥2 studies with low to moderate heterogeneity and classified as having a low or moderate risk of bias [38]. Meta-analysis was not performed because of lack of sufficient evidence (number and quality) for each domain of social indicators.
Results
Summary of included studies
Thirty-four articles from 32 original studies were included from 5,190 screened citations (Fig. 1). Of these 34 articles, 23 reported on breast cancer risk factors, 9 reported on breast cancer frequency, and 3 reported on breast cancer outcomes (1 article examined both breast cancer frequency and outcomes); 10 social determinants were examined (Table 1).
Fig. 1.
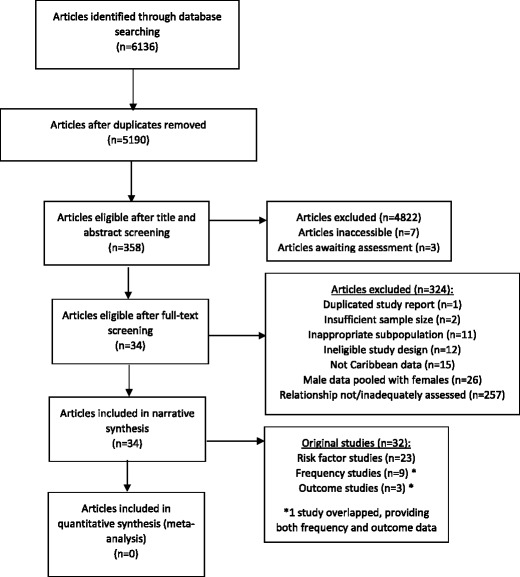
Flowchart of search strategy and article selection
Table 1.
Characteristics of 34 articles describing the social distribution of breast cancer in Caribbean women [40–70, 72, 73]
| Study-level characteristics | Inequality relationships reported | Main Findings | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Article (n = 34) | Study design | Sample size | Age range | Study-base | Country | Proxies used | Risk Factor | Frequency | Outcome | |
| Agyemang, 2009 [46] | Cross-sectional | 855 | 12 to 17 | School | Suriname | EthnicityO | / | / | Mean BMIs across ethnicity: Hindu (19.5 ± 4.0), Creole (20.8 ± 3.8), Javanese (19.3 ± 3.0), Maroon (21.3 ± 4.1), mixed (20.3 ± 3.5). p = 0.02. Maroon girls had a higher BMI than Hindustani girls (p = 0.03) and Javanese (p < 0.01) girls. | |
| EthnicityPI | Proportions of girls who exercise ≥5–7 days per week across ethnicities: Hindu (7.4%), Creole (6.0%), Javanese (4.4%), Maroon (4.0%), mixed (8.2%). p = 0.74 | |||||||||
| Alvarez, 2009 [63] | Registry-based | / | (all) | Population | Cuba | / | ResidenceI | / | Moderately higher risk for breast cancer (CAR smoothed RR of 1.21–1.26) observed in La Cuidad de Habana and two nighboring districts of Matanzas relative to the national Cuban average, but there were no significant rural/urban distictions among these and other municipalities examined. | |
| Block, 2012 [40] (a) | Cross-sectional | 2,017 | 18 to 104 | Population | Grenada | AgeAlc | / | / | Proportion of women who consume 1–2 drinks/day or 1–7 drinks/week across age groups: <35 (3.2%), 35–44 (4.9%), 45–54 (6.5%), 55–64 (7.6%), >64 (2.2%). p = 0.93 | |
| AgePI | Proportion women who walk/bike continuously for >10 min/day across age groups: <35 (79.5%), 35–44 (81.1%), 45–54 (80.1%), 55–64 (7.6%), >64 (2.2%). p = <0.001. Proportion of women who spend leisure time sedentary for >10 min/day across age groups: <35 (78.1%), 35–44 (79.9%), 45–54 (82.9%), 55–64 (83.8%), >64 (83.5%). p = 0.53. | |||||||||
| Blum, 2004 [41] (a) | Cross-sectional | 15,695 | 10 to 18 | School | Antigua, Bahamas, Barbados, British Virgin Islands, Dominica, Guyana, Jamaica, St. Lucia | Religious attendance | ReligionAlc | / | / | For girls attending religious service within the past 3 months, the odds for alcohol use weekly or daily is is 0.50 (p < 0.001). |
| Brathwaite, 2011 [47] (a) | Cross-sectional | 6,947 | 21 to 60 | Population | Bahamas | Education – (in addition to individual) maternal education, paternal education; Income – household expenditure | EducationO,O,O | / | / | Proportions and CI of obesity across levels of maternal education: primary school or less (44.6%, 37.9–51.5), high school (29.3%, 23.7–35.7), technical or vocational (43.0%, 14.1–77.6), college/university (20.1%, 10.8–34.5). p = 0.002. Proportions and CI of obesity across levels of paternal education: primary school or less (41.4%, 34.4–48.7), high school (31.7%, 26.3–37.6), technical or vocational (18.7%, 4.9–50.5), college/university (21.7%, 12.3–35.5). p = 0.021. Proportions and CI of obesity across levels of individual education: primary school or less (36.7%, 25.9–49.0), high school (43.9%, 38.6–49.4), technical or vocational (26.6%, 13.3–46.2), college/university (24.6%, 18.6–31.9). p = 0.0001. Logistic regression shows participant education to predicts obesity (OR 0.706, 95% CI 0.586–0.850, p = <0.00001) |
| ResidenceO | Proportions and CI of obesity by residence type: nonurban (43.8%, 38.0–49.8), urban (37.0%, 32.4, 41.9).p = 0.080. | |||||||||
| IncomeO | Proportions and CI of obesity are as follows across income levels: 1/poorest (40.1%, 31.2–49.7), 2 (49.5%, 39.6–59.5), 3 (42.4%, 34.3–51.0), 4 (32.3%, 25.8–39.5), 5/wealthiest (29.9%, 23.5–37.1). p = 0.006. | |||||||||
| Social household structureO | Proportions and CI of obesity across household heading: non-female headed household (37.0%, 32.1–42.3), female headed household (38.6%, 32.7–44.9). p = 0.678. | |||||||||
| Bryan, 2012 [48] | Cross-sectional | 801 | 18+ | Region/community | Jamaica | Health insurance status | IncomeO | / | / | BMI mean ranks across health insurance status: has health insurance (452.18), does not have health insurance (383.32), does not know (277.80). “Body mass index was higher for those with health insurance”. (p value not given) |
| Chatman, 2004 [60] | Cross-sectional | 599 | 14 to 45 | Health facility | Jamaica | AgeBf | / | / | Proportions of breastfeeding (exclusive, nonexclusive): <20 (14.3%, 12.5%), 20–29 (52.6%, 55.8%), >29 (33.1%, 31.7%). p = 0.8. Regression results not shown – but age stated to not be a significant predictor of breastfeeding exclusivity. | |
| EducationBf | Proportions of breastfeeding (exclusive, nonexclusive): no education (0.75%, 0.2%), primary education (27.8%, 22.2%), beyond primary education (71.4%, 77.4%), missing information (0%, 0.2%). p = 0.4. Regression results not shown – but education stated to not be a significant predictor of breastfeeding exclusivity. | |||||||||
| IncomeBf | Proportions of breastfeeding (exclusive, nonexclusive) by main source of income: mother (11.3%, 10.3%), father (53.4%, 36.1%), other (35.3%, 53.6%). p = 0.0005. Regression results not shown – but source of income stated not to be a significant predictor of breastfeeding exclusivity. | |||||||||
| Marital statusBf | Proportions of breastfeeding (exclusive, nonexclusive): single (39.1%, 40.0%), married (21.1%, 16.9%), common law (39.9%, 43.1%). p = 0.8. Regression results not shown – but marital status stated to not be a significant predictor of breastfeeding exclusivity. | |||||||||
| OccupationBf | Proportions of breastfeeding (exclusive, nonexclusive) across maternal job status: employed (21.1%, 31.0%), unemployed (79.0%, 68.8%), missing (0%, 0.2%). p = 0.07. Proportions of breastfeeding (exclusive, nonexclusive) across paternal job status: employed (88.7%, 92.3%), unemployed (9.8%, 6.4%), not sure (1.5%, 1.3%). p = 0.4. Regression found that when the father was the main financial source for the family as compared families with the mother was the main source of income, the likelihood of exclusive breastfeeding was doubled (adjusted OR 2.03; 95% CI 1.4–3.0). | |||||||||
| Dubois, 2011 [49] (a) | Cross-sectional | 1,674 | 10 to 11 | School | Jamaica | SEP – household crowding, geographical index | SEPO | / | / | Proportion of overweight/obesity across SES levels: low (8.3%), medium (14.9%), high (14.2%). p = ≥0.05. Regression for overweight/obesity across SES levels: medium (OR 1.87, 95% CI 1.0–3.4), high (OR 1.74, 95% CI 0.9-3.3) (ref: low). |
| Social household structureO | Proportion of overweight/obesity across family structure: two-parent family (13.8%), blended family (13.5%), single-parent (10.8%). p = ≥0.05). Regression for overweight/obesity across family structure: blended family (OR 1.0, 95% CI 0.6–1.6), single-parent (OR 0.79, 95% CI 0.4–1.3) (ref: two-parent family). | |||||||||
| Ferguson, 2011 [50] (a) | Cross-sectional | 839 | 18 to 20 | Population | Jamaica | Education – parental education; Occupation – head of household occupation | EducationO | / | / | Prevalence of elevated waist circumference according to parental education: tertiary (12.50%), secondary (14.08%), primary/all age (28.43%), don’t know (18.18%). p = 0.002 for association; p = 0.002 for trend. Regression for central obesity accross to parental education: secondary (OR 1.72, 95% CI 0.74–4.01, p = 0.205), primary/all age (OR 6.14, 95% CI 2.05-18.40, p = 0.001), don’t know (OR 4.61, 95% CI 1.47–14.39, p = 0.009) (reference: tertiary). |
| OccupationO | Prevalence of elevated waist circumference according to head of household occupation status: highly skilled (12.43%), skilled (13.55%), semi/unskilled (21.84%), other (22.81%). p = 0.013 for association; p = 0.009 for trend. Regression for central obesity accross parental occupation: skilled (OR 2.55, 95% CI 0.99–6.57, p = 0.054), semi/unskilled (OR 3.37, 95% CI 1.22–9.29, p = 0.019), other (OR 4.67, 95% CI 1.17–18.55, p = 0.029) (ref: highly skilled). | |||||||||
| Grievink, 2004 [51] | Cross-sectional | 2,025 | 18+ | Population | Bonaire, St. Eustatius, Saba | EducationO | / | / | Proportion and regression for obesity across education level: low (36.8%, reference), intermediate (36.7%, OR 0.9, 95% CI 0.6–1.3), high (27.2%, OR 0.6, 95% CI 0.4-0.9). Proportion and regression for high waist circumference across education level: low (69.4%, reference), intermediate (50.8%, OR 0.7, 95% CI 0.5–0.9), high (44.0%, OR 0.5, 95% CI 0.3–0.7). Proportion and regression for high waist to hip ratio across eduation level: low (78.4%, reference), intermediate (65.3%, OR 1.0, 95% CI 0.7–1.6), high (55.1%, OR 0.6, 95% CI 0.4–0.9). | |
| IncomeO | Proportion and regression for obesity across income level: <825 USD (34.9%, reference), 825–1650 USD (33.9%, OR 1.0, 95% CI 0.7–1.4), >1650 (33.3%, OR 0.9, 95% CI 0.6–1.4). Proportion and regression for high waist circumference across income level: <825 USD (58.3%, reference), 825–1650 USD (54.3%, OR 1.0, 95% CI 0.7–1.5), >1650 (51.2%, OR 1.0, 95% CI 0.7–1.4). Proportion and regression high waist to hip ratio across income level: <825 USD (70.7%, reference), 825–1650 USD (65.0%, OR 1.0, 95% CI 0.7–1.4), >1650 (56.8%, OR 0.7, 95% CI 0.5–1.1). | |||||||||
| OccupationO | Proportion and regression for obesity across occupation level: low (36.8%, reference), intermediate (36.7%, OR 0.9, 95% CI 0.6–1.3), high (27.9%, OR 0.7, 95% CI 0.5–0.9). Proportion and regression for high waist circumference across occupation level: low (57.1%, reference), intermediate (54.8%, OR 1.0, 95% CI 0.7–1.4), high (50.8%, OR 0.8, 95% CI 0.6–1.1). Proportion and regression for high waist to hip ratio across occupation level: low (67.6%, reference), intermediate (66.4%, OR 1.0, 95% CI 0.7–1.5), high (63.8%, OR 0.8, 95% CI 0.6–1.2). | |||||||||
| Hernández, 2013 [64] | Registry-based | / | (all) | Region/community | Cuba | / | ResidenceI | / | There existed spacial clustering (RR 1.63, p = 0.015) and spacial-time clustering (RR 1.91, p = 0.016) of breast cancer incidence in: Encrucijada, Camajuani, Caibarien, Santa Clara, but not in the other municipalities. But there were no significant rural/urban distictions among these and other municipalities examined. | |
| Ichinohe, 2005 [52] | Cross-sectional | 1,935 | / | Population | Jamaica | EducationO | / | / | Regression for education as a predictor of BMI: β -0.560, CI −0.795–0.325, p = 0.000. There is a lower prevelance of obesity in those with more education. | |
| Marital statusO | Regression for marital status as a predictor of BMI: β -0.168, CI −0.329–0.007, p = 0.041. There is a lower prevalence of obesity in married persons. | |||||||||
| Joseph, 2014 [65] | Cross-sectional | 2,582 | / | Health facility | Trinidad & Tobago | / | EthnicityC | / | Regression for incident breast cancer cases: white (crude OR 1.22, 95% CI 0.36–4.06; adjusted OR 1.42, 95% CI 0.4–5.0), East Indian (crude OR 0.99, 95% CI 0.54–1.82; adjusted OR 0.98, 95% CI 0.47–2.04), mixed (crude OR 0.83, 95% CI 0.5–1.37; adjusted OR 0.79, 95% CI 0.43–1.44), Asian and other (crude OR 0.71, 95% CI 0.09–5.35; adjusted OR 0.76, 95% CI 0.44–1.20), missing (crude OR 0.83, 95% CI 0.54–1.28; adjusted OR 0.73, 95% CI 0.44–1.20) (ref: African ancestry). | |
| Marital statusC | Proportions (#) of incident breast cases: single/separated/widowed/divorced (62), married/common law (66), missing (3). Regression for incident breast cancer cases: married/common law (crude OR 0.82, 95% CI 0.58–1.17), missing (crude OR 0.92, 95% CI 0.28–3.02) (ref: single/separated/widowed/divorced). | |||||||||
| Kim, 2007 [42] (a) | Cross-sectional | 3,408 | 60+ | Region/community | Barbados, Cuba | AgeAlc | / | / | Barbados: Proportions of older adults who consumed alcohol ≥4 days/week across age group: 60–65 (3.2%), 66–70 (2.0%), 71–75 (2.2%), 76–80 (2.5%), >80 (3.2%). Cuba: Proportions of older adults who consumed alcohol ≥4 days/week across age group: 60–65 (1.8%), 66–70 (0.6%), 71–75 (0.4%), 76–80 (1.6%), >80 (0.9%). | |
| EducationAlc | Barbados: Proportions of older adults who consumed alcohol ≥4 days/week, across years of education: none (unreliable data), 1–6 (1.1%), 7–12 (8.1%), >12 (11.2%). Cuba: Proportions of older adults who consumed alcohol ≥4 days/week, across years of education: none (0.0%), 1–6 (1.1%), 7–12 (1.3%), >12 (1.5%). | |||||||||
| Marital statusAlc | Barbados: Proportions of older adults who consumed alcohol ≥4 days/week: union (4.8%), other (2.1%). Cuba: Proportions of older adults who consumed alcohol ≥4 days/week: union (1.2%), other (1.1%). | |||||||||
| ResidenceAlc | Proportions of older adults who consumed alcohol ≥4 days/week: Barbados (2.7%), Cuba (1.1%) | |||||||||
| Laborde, 2013 [53] (a) | Cross-sectional | 6025 | (all) | Population | Puerto Rico | EducationO | / | / | Regression for overweight: college (OR 1.060, 95% CI 0.904–1.243, p = 0.472) (ref: no college). Regression for class 1 obese: college (OR 0.819, 95% CI 0.672–0.999, p = 0.048) (ref: no college). Regression for class 2/3 obese: college (OR 0.586, 95% CI 0.469–0.734, p = 0.000) (ref: no college). | |
| IncomeO | Regression for overweight across income bracket: $15000–24999 (OR 1.143, 95% CI 0.962–1.358, p = 0.130), $25000–49000 (OR 1.148, 95% CI 0.926–1.422, p = 0.209), >$49000 (OR 0.887, 95% CI 0.651–1.209, p = 0.447) (ref:<$15000). Regression for class 1 obesity: $15000–24999 (OR 1.131, 95% CI 0.914–1.400, p = 0.259), $25000–49000 (OR 1.064, 95% CI 0.810–1.398, p = 0.657), >$49000 (OR 0.777, 95% CI 0.510–1.183, p = 0.239) (ref:<$15000). Regression for class 2/3 obesity: $15000–24999 (OR 0.662, 95% CI 0.519–0.846, p = 0.001), $25000–49000 (OR 0.540, 95% CI 0.385–0.757, p = 0.000), >$49000 (OR 0.255, 95% CI 0.130–0.499, p = 0.000) (ref:<$15000). | |||||||||
| Marital statusO | Regression for overweight: married (OR 1.029, 95% CI 0.894–1.185, p = 0.690) (ref: not married). Regression for class 1 obesity: married (OR 1.210, 95% CI 1.016–1.442, p = 0.032) (ref: not married). Regression for class 2/3 obesity: married (OR 0.969, 95% CI 0.794–1.181, p = 0.752) (ref: not married). | |||||||||
| Latimer, 2004 [43] | Cross-sectional | 972 | 11 to 19 | School | Puerto Rico | AgeAlc | / | / | Proportions of lifetime, 12-month, and 3-month alcohol use: middle school age groups (58.3%, 42.1%, 31.6%), high school age groups (77.0%, 57.3%, 31.6%). | |
| Mendez, 2004 [54] (a) | Cross-sectional | 2,096 | 25 to 74 | Population | Jamaica | IncomeO | / | / | Proportions and regression for overweight across monthly income: <$1000 (30.4%, reference), $1000–3000 (32.7%, OR 0.96, 95% CI 0.65–1.42), $3001–6000 (31.7%, OR 1.61, 95% CI 1.04–2.48), >$6000 (36.9%, OR 1.70, 95% CI 0.97–2.98). Proportion and regression for obesity across monthly income: <1000 (32.5%, reference), 1000–3000 (26.1%, OR 0.75, 95% CI 0.50-1.13), 3001–6000 (41.8%, OR 1.83, 95% CI 1.19–2.80), >6000 (34.4%, OR 1.66, 0.95–2.92). Multivariate ORs comparing prevalence in women above vs below the poverty line were significant for overweight and obesity. | |
| Morales, 2013 [66] | Case–control | 1,126 | 21+ | Population | Puerto Rico | / | EducationC | / | Regression for breast cancer: grades 1–8 (crude OR 5.77, 95% CI 2.9-11.7; adjusted OR 3.38, 95% CI 1.5-5.7; p = 0.003), grades 9–12 (crude OR 1.72, 95% CI 1.3–2.2; adjusted OR 1.33, 95% CI 0.9–1.9; p = 0.086) (ref: associate or higher degree). | |
| Marital statusC | Regression for breast cancer: divorced (crude OR 3.59, 95% CI 2.1–5.8; adjusted OR 2.57, 95% CI 1.4–4.4; p = 0.002), single (crude OR 2.11, 95% CI 1.2–3.6; adjusted OR 1.36, 95% CI 0.7–2.6; p = 0.421), widow (crude OR 2.74, 95% CI 1.5–5.0; adjusted OR 2.08, 95% CI 1.1–4.0; p = 0.039) (ref: married). | |||||||||
| Nam, 2012 [55] (a) | Cross-sectional | 5,786 | 65+ | Region/community | Barbados, Cuba | EducationO | / | / | Barbados: Mean years of education: low waist circumference (5.1 ± 0.2), high waist circumference (5.2 ± 0.2). p > 0.01. Cuba: Mean years of education: low waist circumference (6.2 ± 0.2), high waist circumference (6.5 ± 0.2), p > 0.01. | |
| Marital statusO | Barbados: Proportion of married females: low waist circumference (24.6%), high waist circumference (22.6%). p > 0.01. Cuba: Proportion of married females: low waist circumference (11.1%), high waist circumference (19.5%). p < 0.001. | |||||||||
| ResidenceO | Proportion of women with high waist circumference: Barbados (63%), Cuba (48.5%). | |||||||||
| Nemesure, 2009 [67] (a) | Case control | 722 | 21+ | Population | Barbados | / | EducationC | / | Mean years of education: breast cancer cases (12.1 ± 3.8,), controls (11.7 ± 3.3). p = 0.13 | |
| Marital statusC | Proportion of marital status types (breast cancer cases, controls): single and never married (30.2%, 35.7%), married or living together (42.3%, 41.0%), separated or divorced (14.9%, 11.9%), widowed (12.6%, 11.4%). p = 0.46. | |||||||||
| OccupationC | Proportion of occupations (breast cancer cases, controls): housewife/homemaker (11.3%, 7.1%), professor/administrative/managerial (19.4%, 13.2%), other (69.4%, 79.7%). p = 0.01. Regression for breast cancer: professional occupation (OR 1.36, 95% CI 0.83–2.24), housewife/homemaker (OR 1.58, 95% CI 0.86–2.89), (ref: other). | |||||||||
| Ohene, 2005 [44] (a) | Cross-sectional | 15,695 | 10 to 18 | School | Antigua, Bahamas, Barbados, British Virgin Islands, Dominica, Grenada, Guyana, Jamaica, St. Lucia | AgeAlc | / | / | Proportions of alcohol use within past 12 months, across age group: 10–12 (3.1%) 13–15 (7.3%), 16–18 (11.1%) | |
| Pérez-Ríos, 2008 [61] (a) | Cross-sectional | 1,695 | 15 to 49 | Population | Puerto Rico | AgeBf | / | / | Proportion of women initiating breastfeeding across age group: 15–24 (61.3%), 25–34 (67.7%), 35–49 (61.4%). p = 0.024. Regression for breastfeeding initiation: 25–34 (crude OR 0.76, 95% CI 0.60–0.95; adjusted OR 1.04, 95% CI 0.81–1.35), 35–49 (crude OR 1.00, 95% CI 0.74–1.34; adjusted OR 1.39, 95% CI 1.00–1.95) (ref: 15–24). | |
| EducationBf | Proportion of women initiating breastfeeding across education level: 0–8 school years (49.5%), 9–11 school years (55.3%), high-school diploma (62.9%), associate degree/some university without diploma (70.0%), baccalaureate/postgraduate (81.2%). p = 0.0001. Regression for breastfeeding initiation: 9–11 school years (crude OR 0.79, 95% CI 0.55–0.08; adjusted OR 0.88, 95% CI 0.60–1.29), high-school diploma (crude OR 0.58, 95% CI 0.42–0.08; adjusted OR 0.67, 95% CI 0.47–0.94), associate degree/some university without diploma (crude OR 0.42, 95% CI 0.30–0.59; adjusted OR 0.49, 95% CI 0.34–0.72), baccalaureate/postgraduate (crude OR 0.23, 95% CI 0.15–0.34; adjusted OR 0.29, 95% CI 0.17–0.45). | |||||||||
| Marital statusBf | Proportion of women initiating breastfeeding: married (70.2%), living together (54.5%), without a partner (57.6%). p = 0.0001. Regression for breastfeeding initiation: living together (crude OR 1.96, 95% CI 1.53–2.52; adjusted OR 1.55, 95% CI 1.18–2.05), without a partner (crude OR 1.73, 95% CI 1.33–2.26; adjusted OR 1.45, 95% CI 1.09–1.92) (ref: married). | |||||||||
| OccupationBf | Proportion of women initiating breastfeeding: employed (71.9%), unemployed (61.0%,). p = 0.0001. Regression for breastfeeding initiation: employed (crude OR 1.63, 95% CI 1.31–2.03; adjusted OR 1.15, 95% CI 0.89–1.48) (ref: unemployed). | |||||||||
| Rivera-Lugo, 2007 [62] | Cross-sectional | 200 | 22+ | Health facility | Puerto Rico | AgeBf | / | / | Results not stated because simple logistic regression showed a p= > 0.10 for exclusive postpartum breastfeeding. | |
| EducationBf | Regression for exclusive postpartum breastfeeding: high school or less (OR 0.354, 95% CI 0.046–2.736, p = 0.320), vocational/associate degree (OR 0.649, 95% CI 0.168–2.511, p = 0.531), some college level (OR 0.807, 95% CI 0.190–3.435, p = 0.772), bachelor degree (OR 1.145, 95% CI 0.384–3.416, p = 0.808) (ref: masters/doctorate). | |||||||||
| IncomeBf | Regression for exclusive breastfeeding: $0–2000 (OR 0.301, CI 0.082–1.112, p = 0.072), $2001–3000 (OR 0.460, CI 0.140–1.514, p = 0.201), $3001–$4000 (OR 0.317, CI 0.101–0.994, p = 0.049) (ref: >$4000) (reference). | |||||||||
| Marital statusBf | Results not stated because simple logistic regression showed a p= > 0.10 for exclusive postpartum breastfeeding. | |||||||||
| Santana, 2011 [72] | Registry-based | 1,819 | (all) | Region/community | Cuba | / | / | Residence | Number of deaths and crude mortality rates (per 100,000) respectively of prostate cancer across municipality: Contramaestre (6, 11.7), Mella (5, 28.9), San Luis (7, 15.9), II Frente (2, 10.3), Songo-La Maya (10, 21.6), Santiago (72, 28.5), Palma (8, 13.0), III Frente (3, 21.3), Guamá (2, 11.9). Weak preponderance of prosatate cancer in more urban areas (no significance testing done). | |
| Shirley, 2010 [68] | Registry-based | 772 | 21 to 96 | Population | Jamaica | / | ResidenceC | / | Proportion of incident breast cancer cases by parish: Kingston & St. Andrew (34.7%), Manchester (22.9%), St. Catherine (13.9%), St. Ann (7.3%), St. Mary (5.1%), St. Thomas (4.4%), St. James (3.9%), Portland (3.2%), St. Elizabeth (2.5%), Clarendon (1.9%). No urban/rural trend found (no significance testing done) | |
| Sinnapah, 2009 [56] | Cross-sectional | 780 | 10 to 18 | School | Guadeloupe | EthnicityO,PI | / | / | ETHNICITY - Means of daily duration of leisure-time physical activity (“LTPA”) (hours/day): Asian-Indians (1.25 ± 1.19), other (1.51 ± 1.29). Means of absolute time spent in activities (light, moderate, vigorous): Asian-Indian (2.9 ± 3.8, 3.2 ± 4.2, 2.5 ± 3.9), other (2.3 ± 4.4, 4.2 ± −5.0, 3.9 ± 5.1). Means of average intensity of LTPA (MET): Asian-Indian (4.5 ± 1.7), other (5.0 ± 1.9). Means of maximal intensity of LTPA (MET): Asian-Indian (7.1 ± 2.3), other (7.7 ± 2.7). OVERWEIGHT/OBESITY - Mean BMI: Asian-Indian (18.8 ± 3.0), other (20.2 ± 3.7). p < 0.05. | |
| Sinnapah, 2009 [57] | Cross-sectional | 122 | 17 to 66 | Health facility | Guadeloupe | EthnicityO,PI | / | / | ETHNICITY -Mean physical activity levels: Asian-Indian (1.62 ± 0.22), other (1.74 ± 0.34). p = <0.05. OVERWEIGHT/OBESITY - Means of BMI: Asian-Indians (24.4 ± 4.0), others (24.4 ± 4.3). p > 0.05. | |
| Sinnapah, 2009 [58] | Cross-sectional | 720 | 11 to 17 | School | Guadeloupe | EthnicityO | / | / | Results are stratified by age groups - <14 and >14. Mean BMI (<14 and >14): Asian Indian (19.0 + 3.5, 21.1 + 5.3), other (20.3 + 4.0, 21.4 + 4.0). p > 0.05. Mean waist circumference: Asian Indian (65.5+/−8.8, 68.1+/−8.7), other (68.5+/−8.7, 70.2+/−8.9). p = <0.05. Mean waist to hip ratio: Asian Indian (0.75 + 0.04, 0.74 + 0.06), other (0.76 + 0.05, 0.73 + 0.04). p < 0.05. Mean % body fat: Asian Indian (25.2 + 5.7, 26.6 + 5.2), other (24.3 + 5.5, 25.1 + 5.9). p < 0.05. Proportions of obesity (all ages): Asian Indian (2.2%), other (7.2%). No p-value given. | |
| Taioli, 2012 [73] | Registry-based | 3,710 | all | Population | Trinidad & Tobago, Guyana | / | / | Ethnicity | Trinidad: Regression for breast cancer mortality across ethnicity: white (HR 1.3, 95% CI 0.8–1.9), Indian (HR 1.2, 95% CI 1.1–1.4), other/unknown (HR 1.3, 95% CI 1.1–1.5) (ref: black). Guyana: Regression for breast cancer mortality across ethnicity: white (HR 1.1, 95% CI 0.4–2.6), Indian (HR 1.3, 95% CI 1.0–1.6), other/unknown (HR 1.0, 95% CI 0.7–1.5). | |
| Torres, 2007 [69] | Cross-sectional | / | 25 to 50 | Population | Cuba | / | ResidenceI | / | Means (range) of incidence rates per 100,000 are as follows - Pinar del Rio, Havana, Cienfuegos,Villa Clara, Ciego de Avila (≤20.7); Sancti Spiritus, Matanzas, Isla de Juventud (20.8-24.9); Camaguey, Holguin, Granma (25.0-36.8); Santiago de Cuba, Guantanamo, Las Tunas (≥36.9). No urban/rural differences. | |
| Torres-Cintrón, 2010 | Registry-based | / | (all) | Population | Puerto Rico | / | ResidenceI | Residence | INCIDENCE - Standardized incidence (per 100,000), rate ratios and CI across regions of Puerto Rico: Northwest (70.8, 0.99, 0.91–1.08), North (64.3, 0.90, 0.84–0.97), Central (72.4, 1.01, 0.95–1.07), East (64.7, 0.90, 0.80–1.02), Northeast (77.1, 1.08, 1.03–1.13), Southeast (58.5, 0.82, 0.76–0.88), South (64.0, 0.89, 0.84–0.96), Southwest (70.4, 0.98, 0.90–1.07). Figures for the North, Northeast, Southeast, and South are significantly different from overall Puerto Rico (p < 0.05), but there were no significant rural/urban distinctions between these and other municipalities examined. MORTALITY - Standardized mortality (per 100,000), rate ratios and CI across regions of Puerto Rico: Northwest (13.3, 0.81, 0.66–0.99), North (13.8, 0.85, 0.72–0.99), Central (172., 1.05, 0.93–1.19), East (20.4, 1.25, 0.99–1.56), Northeast (19.1, 1.17, 1.06–1.29), Southeast (15.2, 0.93, 0.81–1.06), South (14.7, 0.90, 0.78–1.03)), Southwest (15.8, 0.97, 0.81–1.15) (ref: Puerto Rico). Figures for the North, Northwest, and Northeast are significantly different from overall Puerto Rico (p < 0.05), but there were no significant rural/urban distinctions between these and other municipalities examined. | |
| Tull, 2005 [59] | Cross-sectional | 893 | 20+ | Regional/community | US Virgin Islands (St. Croix only) | EthnicityO | / | / | Proportions and CI of overweight: Hispanic white (30.7%, 8.7–52.7), Hispanic black (35.6%, 23.0–48.2), nonhispanic black immigrant (33.9%, 26.3–41.5), nonhispanic black USVI-born (26.75, 16.0–37.4). p > 0.05. Proportions and CI obesity: Hispanic white (43.5%, 26.5–61.4), Hispanic black (35.6%, 23.0–48.2), nonhispanic black immigrant (44.3%, 37.9–50.7), nonhispanic black USVI-born (38.8%, 29.9–47.7). | |
| van Leeuwaarde, 2011 [70] | Registry-based | / | (all) | Population | Suriname | / | EthnicityI | / | Proportions and incidence rates (per 100,000 per year) of breast cancer: Creole (37.2%, 35.7), Maroons (1.9%, 2.2), Hindu (29.4%, 18.2), Javanese (17.9%, 20.8), Chinese (1.9%, not given), mixed (7.4%, 10.1), Dutch (1.4%, not given), other (2.9%, not given). Note these proportions also reflect the ethnography of the general Suriname population. | |
| Varona, 2011 [45] (a) | Cross-sectional | 22,851 | 15+ | Population | Cuba | Income – perception of economic situation | AgeAlc | / | / | Proportions and CI of females consuming alcohol in past 30 days across age group: 15–19 (11.4%, 8.9–13.9), 20–39 (14.6%, 13.2–15.9), 40–59 (9.3%, 8.0–10.5), >59 (2.7%, 1.8–3.6). |
| EducationAlc | Proportions and CI of females consuming alcohol in past 30 days: primary school (4.8%, 3.8–5.7), middle school (10.7%, 9.4–12.1), high school (13.9%, 12.4–15.4), university (13.2%, 10.8–15.7). | |||||||||
| EthnicityAlc | Proportions and CI of females consuming alcohol in past 30 days: white (8.2%, 7.3–9.0), mestizo (14.7%, 12.9–16.5), black (14.9%, 12.3–17.6). | |||||||||
| IncomeAlc | Proportions and CI of females consuming alcohol in past 30 days: excellent (8.4%, 2.3–14.6), good (11.8%, 10.0–13.6), fair (10.2%, 9.2–11.1), poor (9.2%, 7.4–10.9), very poor (10.9%, 7.6–14.1). | |||||||||
| Marital statusAlc | Proportions and CI of females consuming alcohol in past 30 days: unmarried (14.1%, 12.3–16.0), married or cohabiting (10.0%, 9.0–10.9), divorced or separated (12.0%, 9.9–14.0), widowed (2.5%, 1.4–3.7). | |||||||||
| OccupationAlc | Proportions and CI of females consuming alcohol in past 30 days: manager (18.8%, 13.8–23.7), administrator (14.7%, 10.5–18.8), upper-level technician (13.1%, 10.1–16.1), middle-level technician (12.6%, 10.0–16.1), labourer (14.0%, 10.5–17.2), service worker (16.0%, 13.2–18.8). | |||||||||
• (a) - Articles are components of larger studies: (Block, [40]) - Grenada Heart Project [100]; ((Blum, [41]), (Ohene, [44])) - Caribbean Youth Health Survey [101]; (Brathwaite, [47]) - 2001 Bahamas Living Conditions Survey [102]; ((Nam, [55]), (Kim, [42])) – [Health, Wellbeing and Aging] [103]; (Dubois, [49]) - Jamaica Youth Risk and Resiliency Behaviour Survey of 2007 [104]; (Ferguson, [50]) - Jamaica Birth Cohort [105]; (Laborde, [53]) - Behavioral Risk Factor Surveillance System [106]; (Mendez, [54]) - International Collaborative Study on Hypertension in Blacks [107]; (Nemesure, [67]) - The Barbados National Cancer Study [67]; (Pérez-Ríos, [61]) - Puerto Rico Reproductive Health Survey [108]; (Varona, [45]) – 2011 National Survey on Risk Factors and Chronic Diseases [109]
• Social determinants listed under “Risk Factors” are designated as “Alc” for alcohol; “Bf” for limited breastfeeding; “O” for overweight/obesity; and “PI” for physical inactivity
• Social determinants listed under “Frequency” are designated as “I” for incidence and “C” for numbers of cases
• All social determinants listed under “Outcome” are examined by mortality
Included articles reported on studies conducted in English-speaking (Antigua, Bahamas, Barbados, British Virgin Islands, Dominica, Grenada, Guyana, Jamaica, St. Lucia, Trinidad and Tobago, United States Virgin Islands); French-speaking (Guadeloupe); Dutch-speaking (Bonaire, St. Eustatius, Saba, Suriname); and Spanish-speaking (Cuba, Puerto Rico) territories. Most studies originated in Cuba (n = 7) and Jamaica (n = 7). Across the 8 categories of social determinants, there were a total of 15 different social determinants and 14 review endpoints, leaving 189 possible inequality relationship groups that could have been reported (Fig. 2). Only 30 (16%) of these relationship groups were reported by the 34 articles, leaving 159 relationship groups (84%) without an evidence base. There were 75 inequality relationships reported: 59 on breast cancer risk factors, 13 on breast cancer frequency, and 3 on breast cancer outcomes.
Fig. 2.
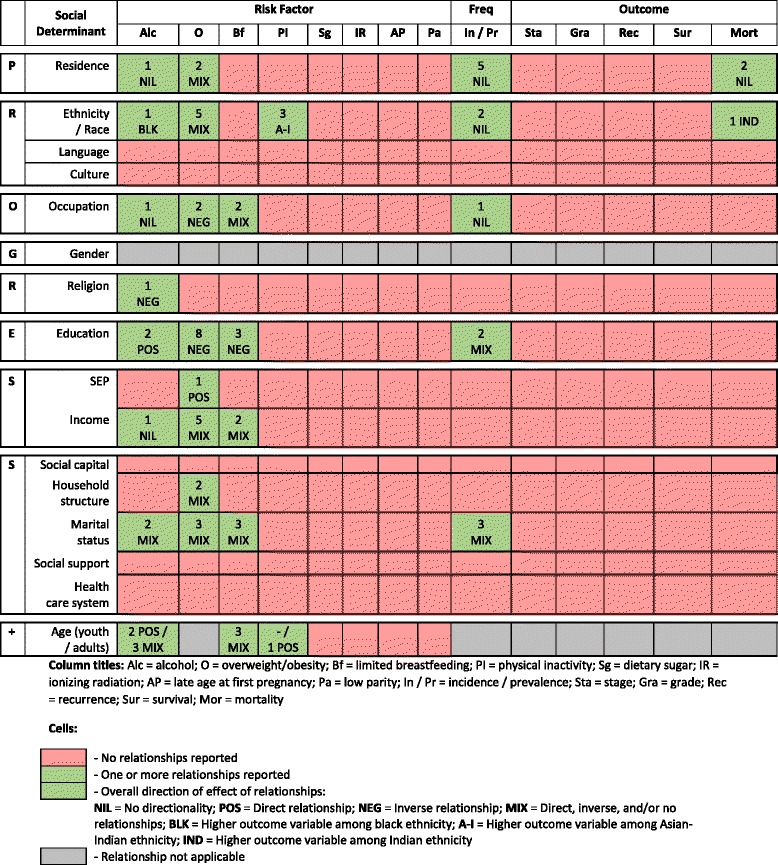
Summary of 75 inequality relationships from 34 articles between a social determinant and review endpoint [40–70, 72, 73]. Legend: Age and limited breastfeeding cells do not separate youth and adult samples as the studies have combined these age groups in their samples
Risk of bias of included studies
Of the 34 articles, 16 were classified as moderate-risk, 14 were classified as serious-risk, 1 was classified as unclear-risk, 2 were classified as moderate/serious-risk, and 1 was classified as serious/unclear-risk (Table 2). At the relationship-level, of the 75 relationships, 35 were classified as moderate-risk, 34 were classified as serious-risk, and 6 were classified as unclear-risk. Figure 3 details the proportion of relationship classifications within each of the 5 risk of bias domains. Overall, lack of adjustment for confounding was the main contributor to an increased risk of bias, followed by non-disclosure or inadequate handling of missing data.
Table 2.
| Article (n = 34) | Relationship (n = 75) | Bias domain | ||||||
|---|---|---|---|---|---|---|---|---|
| Endpoint | Social determinant | Confounding | Participant selection | Missing data | Measurement of outcomes | Selective reporting | OVERALL | |
| Agyemang, 2009 [46] | Overweight/obesity | Ethnicity | Serious | Low | Low | Moderate | Low | Serious |
| Physical inactivity | Ethnicity | Serious | Low | Low | Low | Low | Moderate | |
| Alvarez, 2009 [63] | Incidence | Residence | Serious | Low | Unclear | Low | Low | Moderate |
| Block, 2012 [40] | Alcohol | Age | Serious | Moderate | Serious | Moderate | Serious | Serious |
| Physical inactivity | Age | Serious | Moderate | Serious | Moderate | Serious | Serious | |
| Blum, 2004 [41] | Alcohol | Religion | Low | Unclear | Unclear | Moderate | Low | Unclear |
| Brathwaite, 2011 [47] | Overweight/obesity | Educationind | Serious | Moderate | Low | Low | Low | Moderate |
| Overweight/obesity | Educationmat | Serious | Moderate | Low | Low | Low | Moderate | |
| Overweight/obesity | Educationpat | Serious | Moderate | Low | Low | Low | Moderate | |
| Overweight/obesity | Income | Serious | Moderate | Low | Low | Low | Moderate | |
| Overweight/obesity | Residence | Serious | Moderate | Low | Low | Low | Moderate | |
| Overweight/obesity | Social household structure | Serious | Moderate | Low | Low | Low | Moderate | |
| Bryan, 2012 [48] | Overweight/obesity | Incomeins | Serious | Low | Unclear | Serious | Low | Serious |
| Chatman, 2004 [60] | Breastfeeding | Age | Low | Serious | Serious | Moderate | Low | Serious |
| Breastfeeding | Education | Low | Serious | Serious | Moderate | Low | Serious | |
| Breastfeeding | Income | Low | Serious | Serious | Moderate | Low | Serious | |
| Breastfeeding | Marital status | Low | Serious | Serious | Moderate | Low | Serious | |
| Breastfeeding | Occupation | Low | Serious | Serious | Moderate | Low | Serious | |
| Dubois, 2011 [49] | Overweight/obesity | SEP | Low | Unclear | Low | Serious | Low | Serious |
| Overweight/obesity | Social household structure | Moderate | Unclear | Low | Low | Low | Moderate | |
| Ferguson, 2010 [50] | Overweight/obesity | Education | Moderate | Moderate | Low | Low | Low | Moderate |
| Overweight/obesity | Occupation | Moderate | Moderate | Low | Low | Low | Moderate | |
| Grievink, 2004 [51] | Overweight/obesity | Education | Moderate | Low | Low | Low | Moderate | Moderate |
| Overweight/obesity | Income | Moderate | Low | Low | Low | Moderate | Moderate | |
| Overweight/obesity | Occupation | Moderate | Low | Low | Low | Moderate | Moderate | |
| Hernández, 2013 [64] | Incidence | Residence | Serious | Low | Unclear | Low | Low | Moderate |
| Ichinohe, 2005 [52] | Overweight/obesity | Education | Moderate | Serious | Low | Low | Low | Serious |
| Overweight/obesity | Marital status | Moderate | Serious | Low | Low | Low | Serious | |
| Joseph, 2014 [65] | Incident cases | Ethnicity | Moderate | Serious | Unclear | Low | Low | Serious |
| Incident cases | Marital status | Serious | Serious | Unclear | Low | Low | Serious | |
| Kim, 2007 [42] | Alcohol | Age | Moderate | Low | Unclear | Moderate | Low | Moderate |
| Alcohol | Education | Moderate | Low | Unclear | Moderate | Low | Moderate | |
| Alcohol | Marital status | Moderate | Low | Unclear | Moderate | Low | Moderate | |
| Alcohol | Residence | Moderate | Low | Unclear | Low | Low | Moderate | |
| Laborde, 2013 [53] | Overweight/obesity | Education | Serious | Moderate | Unclear | Serious | Low | Serious |
| Overweight/obesity | Income | Serious | Moderate | Unclear | Serious | Low | Serious | |
| Overweight/obesity | Marital status | Serious | Moderate | Unclear | Serious | Low | Serious | |
| Latimer, 2004 [43] | Alcohol | Age | Moderate | Serious | Low | Moderate | Serious | Serious |
| Mendez, 2004 [54] | Overweight/obesity | Income | Moderate | Moderate | Unclear | Low | Low | Moderate |
| Morales, 2013 [66] | Incident cases | Education | Moderate | Low | Low | Low | Low | Moderate |
| Incident cases | Marital status | Moderate | Low | Low | Low | Low | Moderate | |
| Nam, 2012 [55] | Overweight/obesity | Education | Serious | Low | Serious | Low | Serious | Serious |
| Overweight/obesity | Marital status | Serious | Low | Serious | Low | Serious | Serious | |
| Overweight/obesity | Residence | Serious | Low | Serious | Low | Serious | Serious | |
| Nemesure, 2009 [67] | Incident cases | Education | Moderate | Serious | Low | Low | Low | Serious |
| Incident cases | Marital status | Moderate | Serious | Low | Low | Low | Serious | |
| Incident cases | Occupation | Moderate | Serious | Low | Low | Low | Serious | |
| Ohene, 2005 [44] | Alcohol | Age | Serious | Unclear | Unclear | Moderate | Low | Serious |
| Pérez-Ríos, 2008 [61] | Breastfeeding | Age | Moderate | Unclear | Low | Moderate | Low | Moderate |
| Breastfeeding | Education | Moderate | Unclear | Low | Moderate | Low | Moderate | |
| Breastfeeding | Marital status | Moderate | Unclear | Low | Moderate | Low | Moderate | |
| Breastfeeding | Occupation | Moderate | Unclear | Low | Moderate | Low | Moderate | |
| Rivera-Lugo, 2007 [62] | Breastfeeding | Age | Moderate | Serious | Unclear | Moderate | Low | Serious |
| Breastfeeding | Education | Moderate | Serious | Unclear | Moderate | Low | Serious | |
| Breastfeeding | Income | Moderate | Serious | Unclear | Moderate | Low | Serious | |
| Breastfeeding | Marital status | Moderate | Serious | Unclear | Moderate | Low | Serious | |
| Santana, 2011 [72] | Mortality | Residence | Serious | Low | Unclear | Low | Low | Moderate |
| Shirley, 2010 [68] | Incident cases | Residence | Serious | Low | Unclear | Low | Low | Moderate |
| Sinnapah, 2009 [56] | Overweight/obesity | Ethnicity | Serious | Low | Moderate | Unclear | Serious | Serious |
| Physical inactivity | Ethnicity | Serious | Low | Moderate | Unclear | Serious | Serious | |
| Sinnapah, 2009 [57] | Overweight/obesity | Ethnicity | Serious | Serious | Low | Moderate | Low | Serious |
| Physical inactivity | Ethnicity | Serious | Serious | Low | Moderate | Serious | Serious | |
| Sinnapah, 2009 [58] | Overweight/obesity | Ethnicity | Moderate | Low | Low | Low | Moderate | Moderate |
| Taioli, 2012 [73] | Mortality | Ethnicity | Moderate | Low | Unclear | Low | Low | Moderate |
| Torres, 2007 [69] | Incidence | Residence | Serious | Low | Unclear | Low | Low | Moderate |
| Torres-Cintrón, 2010 | Incidence | Residence | Moderate | Low | Unclear | Low | Low | Moderate |
| Mortality | Residence | Moderate | Low | Unclear | Low | Low | Moderate | |
| Tull, 2005 [59] | Overweight/obesity | Ethnicity | Serious | Unclear | Unclear | Low | Low | Serious |
| van Leeuwaarde, 2011 [72] | Incidence | Ethnicity | Serious | Low | Unclear | Low | Low | Moderate |
| Varona, 2011 [45] | Alcohol | Age | Moderate | Low | Unclear | Moderate | Low | Moderate |
| Alcohol | Education | Serious | Low | Unclear | Moderate | Low | Unclear | |
| Alcohol | Ethnicity | Serious | Low | Unclear | Moderate | Low | Unclear | |
| Alcohol | Income | Serious | Low | Unclear | Moderate | Low | Unclear | |
| Alcohol | Marital status | Serious | Low | Unclear | Moderate | Low | Unclear | |
| Alcohol | Occupation | Serious | Low | Unclear | Moderate | Low | Unclear | |
ind – individual; ins – type of health insurance; mat – maternal; pat – paternal
Fig. 3.
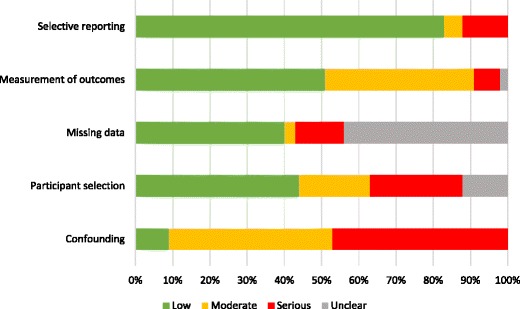
The proportion of risk of bias classifications of the 75 relationships among each of the 5 risk of bias domains [40–70, 72, 73]
Results of inequality relationships
Risk factors
Alcohol
There were 14 inequality relationships for alcohol, reported across 8 social determinants in 6 articles: age (n = 5), education (n = 2), ethnicity (n = 1), income (n = 1), marital status (n = 2), occupation (n = 1), religion (n = 1), residence (n = 1) [40–45].
All adolescent studies found that older adolescents consumed more alcohol than younger adolescents [43, 44], with less conclusive findings among adults [40, 42, 45]. Persons with higher education tended to drink more than those with less education in Barbados and Cuba [42, 45]. For example, 1.1% of elderly in Barbados with 1–6 years education versus 11.8% of persons with >12 years education consumed alcohol ≥4 days/week [42]; likewise, 4.8% (95% CI 3.8–5.7) of Cuban adults with primary level education versus 13.2% (95% CI 10.8–15.7) with university level education consumed alcohol in the past 30 days [45]. However, Cuban elderly report low frequency of consumption across all education levels (0%–1.5% consume alcohol ≥4 days/week) [42, 45]. This is in line with the one article examining residence, which reported higher frequency in overall consumption in Barbados (2.7%) as compared to Cuba (1.1%) [42]. With respect to ethnicity, more black and mestizo Cubans reported alcohol consumption (14.9%, 95% CI 12.3–17.6 and 14.7%, 95% CI 12.9, 16.5 respectively) within the past 30 days than white Cubans (8.2%, 95% CI 7.3–9.0) [45]. A large regional study found that adolescents with increased religious service attendance consumed alcohol less frequently than those who had less attendance (OR 0.50, p < 0.001) [41]. Studies examining marital status showed mixed findings; those examining income and occupation showed no association [42, 45].
Overweight/Obesity
There were 28 inequality relationships for overweight/obesity, reported across 8 social determinants in 14 articles: education (n = 8), ethnicity (n = 5), income (n = 5), marital status (n = 3), occupation (n = 2), residence (n = 2), social household structure (n = 2), and SEP (n = 1) [46–59].
Studies examining education and occupation tended towards a negative relationship [47, 50–53, 55]. All but one study (examining elderly) reported overweight/obesity to be associated with lower levels of individual education [47, 50–53], as well as maternal and paternal education [50]. Adults with lower-level occupations and children with parents working in lower-level occupations tended to be more overweight/obese than those with higher-level occupations [50, 51]. Yet reports on income showed mixed results [47, 48, 51, 53, 54], and the single study examining SEP showed higher levels of overweight/obesity among Jamaican girls of a higher family SEP (OR 1.87, 95% CI 1.0-3.4) [49]. Studies reporting on ethnicity, marital status, social household structure and residence showed mixed results.
Limited breastfeeding
There were 13 inequality relationships for breastfeeding, reported across 5 social determinants in 3 articles: age (n = 3), education (n = 3), income (n = 2), marital status (n = 3), and occupation (n = 2) [60–62].
The likelihood of breastfeeding initiation was higher among older mothers in Puerto Rico (OR 1.39, 95% CI 1.00–1.95 for 35–49 year olds), with no age differences found in Jamaica [60, 61]. Also, Puerto Rican mothers who practiced breastfeeding initiation and exclusive breastfeeding tended to be more educated than those who did not [61, 62]. Mixed results were found for marital status, income, and occupation; to note is that Jamaican mothers who were employed were less likely to exclusively breastfeed (of those employed, 21.1% exclusively breastfeed versus 31.0% nonexclusively breastfeed), while Puerto Rican mothers who were employed were more likely to initiate breastfeeding (crude OR 1.63, 95% CI 1.31–2.03; adjusted OR 1.15, 95% CI 0.89–1.48) [60, 61].
Physical inactivity
There were 4 inequality relationships for physical inactivity, reported across 2 social determinants in 4 articles: age (n = 1), ethnicity (n = 3) [40, 46, 56, 57].
In Grenada, the amount of persons participating in physical activity through walking/biking drastically decreased by 72.5% (p = <0.001) after 54 years of age; at the same time, the amount of persons participating in >10 min of leisure time per day was also found to gradually increase with age (78.1% for persons <35 years old to 83.5% for persons >64 years old, p = 0.53) [40]. The two studies examining ethnicity found that Guadeloupian Asian-Indian adults reported lower levels physical activity than their non-Asian-Indian counterparts when considering time and level of vigour of activity (physical activity level score mean 1.62 (SD 0.22) versus mean 1.74 (SD 0.34), p = <0.05) [56, 57].
Frequency & outcomes
Fewer studies examined the social determinants of the frequency and outcomes of breast cancer, than those for risk factors. There were 13 inequality relationships for breast cancer frequency, reported across 5 social determinants in 9 articles: education (n = 2), ethnicity (n = 2), marital status (n = 3), occupation (n = 1), and residence (n = 5) [63–71]. Most articles reported the number of new breast cancer cases, with 4 out of the 9 articles converting these counts to a breast cancer incidence rate. Relationships examining occupation, residence, and ethnicity showed no association. A Puerto Rico study found a higher likelihood of breast cancer among women with only primary and secondary education as compared to women with higher education (OR 3.38, 95% CI 1.5–5.7 for primary; OR 1.33, 95% CI 0.9–1.9 for secondary) [66]. Lastly, unmarried women in Puerto Rico tended to have a higher likelihood of being diagnosed with breast cancer as compared to married women (divorced OR 2.57, 95% CI 1.4–4.4; single OR 1.36, 95% CI 0.7–2.6; widow OR 2.08, 95% CI 1.1–4.0) [66], but no differences were seen in Trinidad or Barbados.
There were 3 inequality relationships for breast cancer mortality, reported across 2 social determinants in 3 articles: ethnicity (n = 1) and residence (n = 2) [72, 73]. No evidence found reporting on the other 4 breast cancer outcomes. While no associations were observed between breast cancer frequency and ethnicity, mortality from breast cancer was shown to be higher among Indian-decent compared to African-descent populations in Trinidad (OR 1.2, 95% CI 1.1–1.4) and Guyana (OR 1.3, 95% CI 1.0–1.6) [73].
Discussion
Summary of evidence
This systematic review examined the extent of evidence on the influence of social determinants of health on breast cancer risk factors, frequency, and adverse outcomes in the Caribbean. Thirty-four articles from 32 separate studies were included. With 189 possible ways of exploring the role of social determinants on breast cancer, 75 inequality relationships were reported within 30 distinct relationship groups, leaving 159 (84%) relationship groups without an evidence base. The results of this review highlight a critical evidence gap on the effects of social determinants on breast cancer among Caribbean women, with limitations in the quantity and quality of published evidence. Nearly half of the articles were classified as having serious risk of bias, mostly because of failure to adjust for important potential confounders. Furthermore, included articles reported a range of inconclusive findings for each relationship group, at least partly due to study heterogeneity and small numbers of studies available for each relationship group.
Measures of breast cancer frequency and adverse outcomes showed weak relationships with social determinants. Though, the racial disparity in breast cancer mortality between women of Indian origin and women of African origin in two different settings is worthy further investigation. The connection between breast cancer and social inequity is a not a new phenomenon. While low social status is known to place women at a higher risk of developing and dying from breast cancer [74, 75], a higher social status tends to predispose women to certain reproductive risk factors including later age at first pregnancy, lower parity and less breastfeeding [76, 77]. However, a higher SEP also affords women a higher screening rate, an earlier stage of diagnosis, and improved treatment effect and adherence, indicating a complex interchange of risk and protection [74, 75, 78]. Our depicted lack of regional evidence seems a logical result of the absence of a structured network of cancer surveillance in the Caribbean [79, 80]. Cancer registries exist in only twelve Caribbean territories, of which only four are considered high-quality [80, 81]. Challenges are wide-reaching, with limitations in resources, political will, policy and regulation, healthcare service, data quality and security, and local, regional, and international communication and collaboration [80, 81]. The PAHO Plan of Action for Cancer Prevention and Control 2008–2015 [82] has detailed areas for improvement in monitoring and surveillance and consequently, the regional Caribbean Cancer Registry Hub was conceptualized and is progressing towards implementation [81]. While this Hub is expected to greatly improve regional cancer surveillance efforts, measures of inequalities should be highlighted in its plans, with hopes to increase attention to social determinants of cancers and advance health promotion in this area.
Most results lie within the relationships between social determinants and breast cancer risk factors. Overall, Caribbean women with indicators of a lower SEP could be at a higher risk of breast cancer as they reported a higher alcohol intake (except for education), higher levels of overweight/obesity, and limited breastfeeding. The trends reported between age and education with breastfeeding is in line with evidence in other settings, with low maternal education being the strongest predictor of poor breastfeeding practices [83–86]. The inverse relationship between overweight/obesity and education and occupation is similar to what is found in other middle and higher income regions; while being overweight or obese was previously thought to be a condition of the elite, more recent transitions have occurred whereby obesity is shifting towards the persons with a lower socioeconomic standing, particularly as the country’s gross national product increases [87–89]. Typically though, alcohol consumption is found to be higher among persons of a higher SEP [90, 91]. Yet the relationship between alcohol and SEP is complex. Varying environmental factors such as alcohol availability and affordability, economic development, culture, and national alcohol policy flout the gradient typically observed whereby risk factor harm increases with decreasing SEP [90, 91]. The Caribbean is particularly vulnerable to this risk factor as its cultural norms embrace alcohol consumption as a commonplace social activity, which is further compounded by a lack of national alcohol policies [92–94]. While no relationships were reported on social capital, the inverse relationship between alcohol and religion is noteworthy. Religiosity is consistently shown to be protective from substance use by creating a positive personal identity, fostering community acceptance, and providing a coping outlet for stress [95–97]. The Caribbean touts a predominant religious identity which could confer some form of protection from alcohol’s influence on breast cancer and the wider range of NCDs afflicting the region.
Continued and standardized approaches to understanding risk factor profiles is a key element in efforts to reduce cancer risk factors, as evidenced in the WHO’s recommended STEPwise approach to Surveillance (STEPS) [98]. With relevant information on social determinants included in this instrument, it is up to Caribbean territories to fulfil their commitment to the Port-of-Spain Declaration in continuing to implement this in their ongoing efforts to reduce NCDs such as breast cancer [99].
Limitations
The review was limited by a small number of articles within each relationship group, the validity of which was further limited by their significant risk of bias. Further, few studies investigating the effects of social determinants on health have also explored the interrelationships among the social determinants themselves. The Caribbean has been considered as one region in this review, masking the possible and important country-level variations in the relative importance of social determinants. Country-level information on screening and access to treatment such as mammogram screening rates and wait times for diagnosis or treatment are important potential confounders that were not assessed. Publication bias is an important concern as no explicit searching was conducted for grey literature due to limited resources.
Conclusions
This review highlights a crucial gap in the quantity and quality of the evidence examining the social determinants of breast cancer risk factors, frequency, and outcomes. Risk factors were the main endpoints for which relationships with social determinants were reported, with implications for age, ethnicity, education, SEP, and religion. Information on frequency and outcomes were limited, but held implications on marital status and ethnicity respectively. Although the need for more research in this area is acknowledged, this effort should also include an attempt at standardizing reporting guidelines for observational studies of health inequality. Finally, the development of a validated risk of bias assessment tool is imperative for systematic reviewing of observational studies.
Additional files
“Study Protocol”, which details the study protocol for the systematic review. (PDF 1800 kb)
“Search Strategy”, which details the search strategies of the database. (PDF 469 kb)
Acknowledgements
Members of the U.S. Caribbean Alliance for Health Disparities Research Group outside of the writing group are acknowledged for their support in this research: Nadia Bennett, Aurelian Bidulescu, Trevor Ferguson, Damian Francis, Christopher Hassell, Anselm JM Hennis, Lynda Williams, and Novie Younger-Coleman.
Members of the USCAHDR Group (in alphabetical order)
Alvarado M: Chronic Disease Research Centre, Bridgetown, Barbados, West Indies.
Bennett N: The University of the West Indies, Kingston, Jamaica, West Indies.
Bidulescu A: Indiana University, Bloomington, IN, USA.
Brown C: Chronic Disease Research Centre, Bridgetown, Barbados, West Indies.
Ferguson T: The University of the West Indies, Kingston, Jamaica, West Indies.
Francis D: The University of the West Indies, Kingston, Jamaica, West Indies.
Hambleton IR: Chronic Disease Research Centre, Bridgetown, Barbados, West Indies.
Harris EN: The University of the West Indies, Kingston, Jamaica, West Indies.
Hassell C: Chronic Disease Research Centre, Bridgetown, Barbados, West Indies.
Hennis AJM: Chronic Disease Research Centre, Bridgetown, Barbados, West Indies.
Hercules S: Chronic Disease Research Centre, Bridgetown, Barbados, West Indies.
Howitt C: Chronic Disease Research Centre, Bridgetown, Barbados, West Indies.
MacLeish M: Sullivan Alliance, Alexandria, VA, USA.
Murphy M: The University of the West Indies, Cave Hill, Barbados, West Indies.
Samuels TA:Chronic Disease Research Centre, Bridgetown, Barbados, West Indies.
Sobers-Grannum N: The University of the West Indies, Cave Hill, Barbados, West Indies.
Sullivan L: Sullivan Alliance, Alexandria, VA, USA.
Unwin N: Chronic Disease Research Centre, Bridgetown, Barbados, West Indies.
Wilks R: The University of the West Indies, Kingston, Jamaica, West Indies.
Williams L: Chronic Disease Research Centre, Bridgetown, Barbados, West Indies.
Younger-Coleman N: The University of the West Indies, Kingston, Jamaica, West Indies.
Funding
This study was fully supported by grant number U24MD006959 from the National Institute on Minority Health and Health Disparities. The funding body was not involved in the design of the study, collection, analysis, and interpretation of data, nor the writing the manuscript. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Minority Health and Health Disparities or the National Institutes of Health.
Availability of data and materials
The data that support the findings of this study are available from the databases used in the study but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of the original study author.
Authors’ contributions
CRB – design of the work, acquisition, analysis, and interpretation of data, drafting the work, final approval of the version to be published. IRH – conception and design of the work, analysis and interpretation of data, drafting the work, revising it critically for important intellectual content, final approval of the version to be published. SMH – design of the work, acquisition and interpretation of data, final approval of the version to be published. MA – design of the work, acquisition and interpretation of data, final approval of the version to be published. MMM – design of the work, analysis and interpretation of data, final approval of the version to be published. NU – conception and design of the work, interpretation of data, revising it critically for important intellectual content, final approval of the version to be published. ENH – conception and design of the work, revising it critically for important intellectual content, final approval of the version to be published. RW – conception and design of the work, revising it critically for important intellectual content, final approval of the version to be published. MM – conception and design of the work, revising it critically for important intellectual content, final approval of the version to be published. LS – conception and design of the work, revising it critically for important intellectual content, final approval of the version to be published. NS-G – conception and design of the work, acquisition, analysis and interpretation of data, drafting the work, revising it critically for important intellectual content, final approval of the version to be published.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Not applicable.
Abbreviations
- CINAHL
Cumulative Index of Nursing and Allied Health Literature
- CSDH
Commission on the Social Determinants of Health
- CUMED
Cuba Medicina
- EMBASE
Excerpta Medica Database
- IBECS
Índice Bibliográfico Español en Ciencias de la Salud
- LILACS
Latin American and Caribbean Health Sciences
- MEDLINE
Medical Literature Analysis and Retrieval System Online, or MEDLARS Online
- NCD
Non-communicable disease
- SciELO
Scientific Electronic Library Online
- SEP
Socioeconomic position
- STROBE
Strengthening the reporting of observational studies in epidemiology
- USCAHDR
United States Caribbean Alliance for Health Disparities Research Group
- WHO
World Health Organization
Footnotes
Electronic supplementary material
The online version of this article (doi:10.1186/s12939-017-0540-z) contains supplementary material, which is available to authorized users.
This article has been updated to correct the supplementary materials and to correct a typo within Figure 2.
Contributor Information
Catherine R. Brown, Email: catherine.brown@cavehill.uwi.edu
Ian R. Hambleton, Email: ian.hambleton@resources4research.com
Shawn M. Hercules, Email: shawnhercules@gmail.com
Miriam Alvarado, Email: miriamalva10@gmail.com.
Nigel Unwin, Email: nigel.unwin@cavehill.uwi.edu.
Madhuvanti M. Murphy, Email: madhuvanti.murphy@cavehill.uwi.edu
E. Nigel Harris, Email: enigel.harris@uwimona.edu.jm.
Rainford Wilks, Email: rainford.wilks@uwimona.edu.jm.
Marlene MacLeish, Email: mmacleish@msm.edu.
Louis Sullivan, Email: Sullivan@pemsm.com.
Natasha Sobers-Grannum, Email: natasha.sobers@cavehill.uwi.edu.
The U.S. Caribbean Alliance for Health Disparities Research Group (USCAHDR):
M. Alvarado, N. Bennet, A. Bidulescu, CR. Brown, T. Ferguson, D. Francis, I. R. Hambleton, E. N. Harris, C. Hassell, A. J. M. Hennis, SM. Hercules, C. Howitt, M. MacLeish, MM. Murphy, T. A. Samuels, N. Sobers-Grannum, L. Sullivan, N. Unwin, R. Wilks, L. Williams, and N. Younger-Coleman
References
- 1.Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095–128. doi: 10.1016/S0140-6736(12)61728-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Institute for Health Metrics and Evaluation. GBD Compare. 2013. http://vizhub.healthdata.org/gbd-compare/arrow. Accessed 13 Mar 2016.
- 3.World Health Organization. Global Health Observatory data repository. 2015. http://apps.who.int/gho/data/view.main.DALYNUMWBDCPLACV?lang=en. Accessed 8 Jan 2015.
- 4.Hiatt RA, Pasick RJ, Stewart S, Bloom J, Davis P, Gardiner P, et al. Cancer screening for underserved women: the Breast and Cervical Cancer Intervention Study. Cancer Epidemiol Biomark Prev Publ Am Assoc Cancer Res Cosponsored Am Soc Prev Oncol. 2008;17(8):1945–9. doi: 10.1158/1055-9965.EPI-08-0172. [DOI] [PubMed] [Google Scholar]
- 5.Hiatt RA, Breen N. The social determinants of cancer: a challenge for transdisciplinary science. Am J Prev Med. 2008;35(Suppl 2):S141–150. doi: 10.1016/j.amepre.2008.05.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gerend MA, Pai M. Social determinants of Black-White disparities in breast cancer mortality: a review. Cancer Epidemiol Biomark Prev Publ Am Assoc Cancer Res Cosponsored Am Soc Prev Oncol. 2008;17(11):2913–23. doi: 10.1158/1055-9965.EPI-07-0633. [DOI] [PubMed] [Google Scholar]
- 7.Hussain SK, Altieri A, Sundquist J, Hemminki K. Influence of education level on breast cancer risk and survival in Sweden between 1990 and 2004. Int J Cancer J Int Cancer. 2008;122(1):165–9. doi: 10.1002/ijc.23007. [DOI] [PubMed] [Google Scholar]
- 8.Wheeler SB, Reeder-Hayes KE, Carey LA. Disparities in breast cancer treatment and outcomes: biological, social, and health system determinants and opportunities for research. Oncologist. 2013;18(9):986–93. doi: 10.1634/theoncologist.2013-0243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Caribbean Community Secretariat. Declaration of Port-of-Spain: Uniting to stop the epidemic of chronic NCDs. 2011. http://caricom.org/media-center/communications/statements-from-caricom-meetings/declaration-of-port-of-spain-uniting-to-stop-the-epidemic-of-chronic-ncds. Accessed 7 Jan 2016.
- 10.International Development Research Council. Evaluating CARICOM’s Political Commitments for Non-Communicable Disease Prevention and Control. 2015. https://www.idrc.ca/en/project/evaluating-caricoms-political-commitments-non-communicable-disease-prevention-and-control. Accessed 10 Nov 2015.
- 11.Commission on Social Determinants of Health. Closing the gap in a generation: health inequity through action on the social determinants of health. 2008. http://www.who.int/social_determinants/final_report/csdh_finalreport_2008.pdf. Accessed 20 July 2015.
- 12.World Health Organization. Rio political declaration on social determinants of health. 2011. http://www.who.int/sdhconference/declaration/Rio_political_declaration.pdf?ua=1. Accessed 20 July 2015.
- 13.Blas E, Kurup AS, editors. Equity, social determinants, and public health programmes. World Health Organization. 2010. http://whqlibdoc.who.int/publications/2010/9789241563970_eng.pdf. Accessed 27 Oct 2014.
- 14.Sobers-Grannum N, Murphy MM, Nielsen A, Guell C, Samuels TA, Bishop L, et al. Female gender is a social determinant of diabetes in the Caribbean: a systematic review and meta-analysis. PLoS ONE. 2015;10(5):e0126799. doi: 10.1371/journal.pone.0126799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2224–60. doi: 10.1016/S0140-6736(12)61766-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Chen W. Factors that modify breast cancer risk in women. 2014. http://www.uptodate.com/contents/factors-that-modify-breast-cancer-risk-in-women?source=search_result&search=risk+factors+for+breast+cancer&selectedTitle=1~150#H1202338. Accessed 29 Mar 2016.
- 17.Schottenfeld D, Jr JFF, editors. Cancer Epidemiology and Prevention. 3. New York: Oxford University Press; 2006. [Google Scholar]
- 18.O’Neill J, Tabish H, Welch V, Petticrew M, Pottie K, Clarke M, et al. Applying an equity lens to interventions: using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J Clin Epidemiol. 2014;67(1):56–64. doi: 10.1016/j.jclinepi.2013.08.005. [DOI] [PubMed] [Google Scholar]
- 19.U.S. National Library of Medicine. Fact Sheet MEDLINE, PubMed, and PMC (PubMed Central): How are they different? 2015. http://www.nlm.nih.gov/pubs/factsheets/dif_med_pub.html. Accessed 13 Aug 2015.
- 20.Elsevier R&D Solutions. Embase Fact Sheet. 2015. https://www.elsevier.com/__data/assets/pdf_file/0016/59011/R_D_Solutions_Embase_Fact_Sheet-Web.pdf. Accessed 13 Aug 2015.
- 21.SciELO, FAPESP, BIRME. SciELO. SciELO. n.d. Available from: http://www.scielo.br/. Accessed 13 Aug 2015.
- 22.EBSCO. CINAHL Database. 2015. https://health.ebsco.com/products/the-cinahl-database. Accessed 13 Aug 2015.
- 23.Centro Nacional de Información de Ciencias Médicas, Infomed. Bibliographic Databases. BVS Cuba: Biblioteca Virtual en Salud. n.d. http://www.bvsite.sld.cu/php/level.php?lang=en&component=30&item=3. Accessed 13 Aug 2015.
- 24.EndNote. Philadephia: Thomson Reuters; 2014. www.endnote.com. Accessed 10 Nov 2015.
- 25.Harrison A, James C, Jackson M, Vaughn MS. Imapct of body image and self-esteem on Jamaican adolescent behaviour. Galenos: In Turkey; 2013. [Google Scholar]
- 26.Rojas NBA, Herrera AFD, González MD. Cuban prospective study of tobacco. Alcohol Mortal Glob Heart Suppl. 2014;9(1):e225–6. doi: 10.1016/j.gheart.2014.03.2042. [DOI] [Google Scholar]
- 27.Craw L, Saunders N, Koelink E, Roth J, Aronson L, Silverman M. Paediatrics and Child Health. Vancouver: Churchill Livingstone; 2010. Anthropometric measurement of school-aged children in Guyana, South America. [Google Scholar]
- 28.Rivera J, Alvarez N, Quintana E, Cruz-Correa J, Orengo JC. Características sociales y clínicas del embarazo en adolescentes. Bol Asoc Med P R. 2007;99(1):8–12. [PubMed] [Google Scholar]
- 29.Macías C, Pita G, Basabe Tuero B, Herrera Javier D, Lanyau Y. Hábitos, actitudes y preferencias alimentarias en adolescentes de enseñanza media de La Habana. Rev Esp Nutr Comunitaria. 2009;15(1):13–22. [Google Scholar]
- 30.Acosta SJ, Suárez AR, Pita G, Peña PR. Bajo peso al nacer y sobrepeso en niños menores de cinco años en Cuba. Rev Esp Nutr Comunitaria Span J Community Nutr. 2008;14(4):225–30. [Google Scholar]
- 31.Lanyau Y, Triana MH, Herrera D, Sánchez MED, Reyes D, Toledo EM, et al. Estado nutricional de la vitamina B1 en adultos mayores no institucionalizados. Rev Esp Nutr Comunitaria Span J Community Nutr. 2005;11(1):34–40. [Google Scholar]
- 32.García-Fragoso L, Medina M, Ortiz N. Factors associated to continuing breastfeeding after returning to work in a group of mothers in Puerto Rico. Bol Asoc Médica P R. 2012;104(1):12–5. [PubMed] [Google Scholar]
- 33.Gonzalez J, Fernandes M, Garcia F. Exclusive breastfeeding reduces asthma in a group of children from the Caguas municipality of Puerto Rico. Boletin Asoc Medica P R. 2010;102(1):10–2. [PubMed] [Google Scholar]
- 34.Reid SD, Ramcharan C, Ghany K. Substance abuse among first admissions to the psychiatric unit of a general hospital in Trinidad. West Indian Med J. 2004;53(2):95–9. [PubMed] [Google Scholar]
- 35.von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–9. doi: 10.1016/j.jclinepi.2007.11.008. [DOI] [PubMed] [Google Scholar]
- 36.Welch V, Petticrew M, Tugwell P, Moher D, O’Neill J, Waters E, et al. PRISMA-Equity 2012 extension: reporting guidelines for systematic reviews with a focus on health equity. PLoS Med. 2012;9(10):e1001333. doi: 10.1371/journal.pmed.1001333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde J. Research electronic data capture (REDCap) - A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–81. doi: 10.1016/j.jbi.2008.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.A Cochrane risk of bias assessment tool: for non-randomized studies of interventions (ACROBAT-NRSI), version 1.0.0. The Cochrane Collaboration. 2014. http://www.riskofbias.info. Accessed 11 Nov 2015.
- 39.Snilstveit B, Vojtkova M, Bhavsar A, Gaarder M. Evidence gap maps: A tool for promoting evidence-informed policy and prioritizing future research. 2013. Report No.: WPS6725. https://openknowledge.worldbank.org/bitstream/handle/10986/16941/WPS6725.pdf. Accessed 31 May 2016. [DOI] [PubMed]
- 40.Block RC, Dozier AM, Hazel-Fernandez L, Guido JJ, Pearson TA. An epidemiologic transition of cardiovascular disease risk in Carriacou and Petite Martinique, Grenada: the Grenada Heart Project, 2005–2007. Prev Chronic Dis. 2012;9:E90. doi: 10.5888/pcd9.110167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Blum RW, Ireland M. Reducing risk, increasing protective factors: findings from the Caribbean Youth Health Survey. J Adolesc Health Off Publ Soc Adolesc Med. 2004;35(6):493–500. doi: 10.1016/S1054-139X(04)00097-7. [DOI] [PubMed] [Google Scholar]
- 42.Kim S, De La Rosa M, Rice CP, Delva J. Prevalence of smoking and drinking among older adults in seven urban cities in Latin America and the Caribbean. Subst Use Misuse. 2007;42(9):1455–75. doi: 10.1080/10826080701212501. [DOI] [PubMed] [Google Scholar]
- 43.Latimer WW, Floyd LJ, Vasquez M, O’Brien M, Arzola A, Rivera N. Substance use among school-based youths in Puerto Rico: differences between gender and grade levels. Addict Behav. 2004;29(8):1659–64. doi: 10.1016/j.addbeh.2004.02.038. [DOI] [PubMed] [Google Scholar]
- 44.Ohene S-A, Ireland M, Blum RW. The clustering of risk behaviors among Caribbean youth. Matern Child Health J. 2005;9(1):91–100. doi: 10.1007/s10995-005-2452-6. [DOI] [PubMed] [Google Scholar]
- 45.Varona P, Chang M, García RG, Bonet M. Tobacco and alcohol use in Cuban women. MEDICC Rev. 2011;13(4):38–44. doi: 10.1590/S1555-79602011000400009. [DOI] [PubMed] [Google Scholar]
- 46.Agyemang C, Oudeman E, Zijlmans W, Wendte J, Stronks K. Blood pressure and body mass index in an ethnically diverse sample of adolescents in Paramaribo, Suriname. BMC Cardiovasc Disord. 2009;9:19. doi: 10.1186/1471-2261-9-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Brathwaite N, Brathwaite A, Taylor M. The socio-economic determinants of obesity in adults in the Bahamas. West Indian Med J. 2011;60(4):434–41. [PubMed] [Google Scholar]
- 48.Bryan GC, Johnson JA, Dawes L, Samuel C. An assessment of the risk factors for type 2 diabetes among women in rural Jamaica. West Indian Med J. 2012;61(8):809–13. [PubMed] [Google Scholar]
- 49.Dubois L, Francis D, Burnier D, Tatone-Tokuda F, Girard M, Gordon-Strachan G, et al. Household food insecurity and childhood overweight in Jamaica and Québec: a gender-based analysis. BMC Public Health. 2011;11:199. doi: 10.1186/1471-2458-11-199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Ferguson TS, Tulloch-Reid MK, Younger NOM, Knight-Madden JM, Samms-Vaughan M, Ashley D, et al. Prevalence of the metabolic syndrome and its components in relation to socioeconomic status among Jamaican young adults: a cross-sectional study. BMC Public Health. 2010;10:307. doi: 10.1186/1471-2458-10-307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Grievink L, Alberts JF, O’Niel J, Gerstenbluth I. Waist circumference as a measurement of obesity in the Netherlands Antilles; associations with hypertension and diabetes mellitus. Eur J Clin Nutr. 2004;58(8):1159–65. doi: 10.1038/sj.ejcn.1601944. [DOI] [PubMed] [Google Scholar]
- 52.Ichinohe M, Mita R, Saito K, Shinkawa H, Nakaji S, Coombs M, et al. The prevalence of obesity and its relationship with lifestyle factors in Jamaica. Tohoku J Exp Med. 2005;207(1):21–32. doi: 10.1620/tjem.207.21. [DOI] [PubMed] [Google Scholar]
- 53.Laborde JE, Sáez-Santiago E. Association between obesity and symptoms of depression of adults in Puerto Rico. P R Health Sci J. 2013;32(3):132–7. [PubMed] [Google Scholar]
- 54.Mendez MA, Cooper RS, Luke A, Wilks R, Bennett F, Forrester T. Higher income is more strongly associated with obesity than with obesity-related metabolic disorders in Jamaican adults. Int J Obes Relat Metab Disord J Int Assoc Study Obes. 2004;28(4):543–50. doi: 10.1038/sj.ijo.0802584. [DOI] [PubMed] [Google Scholar]
- 55.Nam S, Kuo Y-F, Markides KS, Al SS. Waist circumference (WC), body mass index (BMI), and disability among older adults in Latin American and the Caribbean (LAC) Arch Gerontol Geriatr. 2012;55(2):e40–47. doi: 10.1016/j.archger.2012.04.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Sinnapah S, Antoine-Jonville S, Hue O. Is the leisure-time physical activity of Asian Indian Guadeloupean adolescents different from that of their island counterparts? Ethn Health. 2009;14(3):303–14. doi: 10.1080/13557850802509214. [DOI] [PubMed] [Google Scholar]
- 57.Sinnapah S, Antoine-Jonville S, Donnet JP, Hue O. Asian Indians of Guadeloupe are less physically active than their island counterparts. Scand J Med Sci Sports. 2009;19(2):222–7. doi: 10.1111/j.1600-0838.2007.00743.x. [DOI] [PubMed] [Google Scholar]
- 58.Sinnapah S, Antoine-Jonville S, Hue O. Asian Indian adolescents from Guadeloupe are fatter than their island counterparts. Br J Nutr. 2009;102(12):1820–7. doi: 10.1017/S000711450999122X. [DOI] [PubMed] [Google Scholar]
- 59.Tull ES, Thurland A, LaPorte RE. Metabolic syndrome among Caribbean-born persons living in the U.S. Virgin Islands. Rev Panam Salud Pública Pan Am J Public Health. 2005;18(6):418–26. doi: 10.1590/S1020-49892005001000005. [DOI] [PubMed] [Google Scholar]
- 60.Chatman LM, Salihu HM, Roofe MEA, Wheatle P, Henry D, Jolly PE. Influence of knowledge and attitudes on exclusive breastfeeding practice among rural Jamaican mothers. Birth Berkeley Calif. 2004;31(4):265–71. doi: 10.1111/j.0730-7659.2004.00318.x. [DOI] [PubMed] [Google Scholar]
- 61.Pérez-Ríos N, Ramos-Valencia G, Ortiz AP. Cesarean delivery as a barrier for breastfeeding initiation: the Puerto Rican experience. J Hum Lact Off J Int Lact Consult Assoc. 2008;24(3):293–302. doi: 10.1177/0890334408316078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Rivera-Lugo M, Parrilla-Rodríguez AM, Dávila-Torres RR, Albizu-García C, Rios-Motta R. Full breastfeeding during the postpartum hospitalization and mothers’ report regarding baby friendly practices. Breastfeed Med Off J Acad Breastfeed Med. 2007;2(1):19–26. doi: 10.1089/bfm.2006.0025. [DOI] [PubMed] [Google Scholar]
- 63.Alvarez PL-L, Guerra-Yi ME, Faes C, Alvarez YG, Molenberghs G. Spatial analysis of breast and cervical cancer incidence in small geographical areas in Cuba, 1999–2003. Eur J Cancer Prev Off J Eur Cancer Prev Organ ECP. 2009;18(5):395–403. doi: 10.1097/CEJ.0b013e32832f9b93. [DOI] [PubMed] [Google Scholar]
- 64.Hernández NEB, Rodriguez MA, Fleites OA. Análisis espacial de la morbimortalidad del cáncer de mama y cérvix: Villa Clara. Cuba. 2004–2009. Rev Esp Salud Pública. 2013;87(1):49–57. doi: 10.4321/S1135-57272013000100006. [DOI] [PubMed] [Google Scholar]
- 65.Joseph M, Thorpe L, Annandsingh C, Laquis G, Lee Young J, Kwasniewski J, et al. Breast cancer diagnosis from screening in trinidad and tobago: opportunities for cancer prevention. J Immigr Minor Health Cent Minor Public Health. 2014;16(3):409–15. doi: 10.1007/s10903-012-9767-3. [DOI] [PubMed] [Google Scholar]
- 66.Morales L, Alvarez-Garriga C, Matta J, Ortiz C, Vergne Y, Vargas W, et al. Factors associated with breast cancer in Puerto Rican women. J Epidemiol Glob Health. 2013;3(4):205–15. doi: 10.1016/j.jegh.2013.08.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Nemesure B, Wu S-Y, Hambleton IR, Leske MC, Hennis AJ, Barbados National Cancer Study Group Risk factors for breast cancer in a black population--the Barbados National Cancer Study. Int J Cancer J Int Cancer. 2009;124(1):174–9. doi: 10.1002/ijc.23827. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Shirley SE, Sinclair PA, Stennett MA, Codrington G, Bhatt R, Escoffery CT. The pathology of breast cancer in Jamaica: the National Public Health Laboratory study. West Indian Med J. 2010;59(2):177–81. [PubMed] [Google Scholar]
- 69.Torres P, Guerra M, Galán Y, García M, Lezcano M, Fernández L. Incidencia y mortalidad por cáncer en la mujer cubana: Trienio 2000–2002. Rev Cuba Med. 2007 Sep;46(2):0–0.
- 70.van Leeuwaarde RS, Vrede MA, Henar F, Does R, Issa P, Burke E, et al. A nationwide analysis of incidence and outcome of breast cancer in the country of Surinam, during 1994–2003. Breast Cancer Res Treat. 2011;128(3):873–81. doi: 10.1007/s10549-011-1404-7. [DOI] [PubMed] [Google Scholar]
- 71.Torres-Cintrón M, Ortiz AP, Pérez-Irizarry J, Soto-Salgado M, Figueroa-Vallés NR, De La Torre-Feliciano T, et al. Incidence and mortality of the leading cancer types in Puerto Rico: 1987–2004. P R Health Sci J. 2010;29(3):317–29. [PubMed] [Google Scholar]
- 72.Santana RS, Santana ÁLS, García ICC, Cisnero MB. Mortalidad por tumores malignos en Santiago de Cuba durante 2010. MEDISAN. 2011;15(11):1510–6. [Google Scholar]
- 73.Taioli E, Attong-Rogers A, Layne P, Roach V, Ragin C. Breast cancer survival in women of African descent living in the US and in the Caribbean: effect of place of birth. Breast Cancer Res Treat. 2010;122(2):515–20. doi: 10.1007/s10549-009-0702-9. [DOI] [PubMed] [Google Scholar]
- 74.Merletti F, Galassi C, Spadea T. The socioeconomic determinants of cancer. Environ Health. 2011;10(Suppl 1):S7. doi: 10.1186/1476-069X-10-S1-S7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Kogevinas M, Pearce N, Susser M, Boffetta, editors. Social Inequalities and Cancer [Internet]. France: lnternational Agency for Research on Cancer. 1997. https://www.iarc.fr/en/publications/pdfs-online/epi/sp138/SP138.pdf. Accessed 29 Mar 2016.
- 76.Bigby J, Holmes MD. Disparities across the breast cancer continuum. Cancer Causes Control. 2005;16(1):35–44. doi: 10.1007/s10552-004-1263-1. [DOI] [PubMed] [Google Scholar]
- 77.Menvielle G, Kunst AE, Van Gils CH, Peeters PHM, Boshuizen H, Overvad K, et al. The contribution of risk factors to the higher incidence of invasive and in situ breast cancers in women with higher levels of education in the European prospective investigation into cancer and nutrition. Am J Epidemiol. 2011;173(1):26–37. doi: 10.1093/aje/kwq319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Reeder-Hayes KE, Wheeler SB, Mayer DK. Health disparities across the breast cancer continuum. Semin Oncol Nurs. 2015;31(2):170–7. doi: 10.1016/j.soncn.2015.02.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Pan American Health Organization, World Health Organization. Cancer in the Americas - basic indicators 2013. 2013. http://www.paho.org/hq/index.php?option=com_docman&task=doc_download&gid=25330&Itemid=. Accessed 5 July 2016.
- 80.Banydeen R, Rose AMC, Martin D, Aiken W, Alexis C, Andall-Brereton G, et al. Advancing cancer control through research and cancer registry collaborations in the Caribbean. Cancer Control J Moffitt Cancer Cent. 2015;22(4):520–30. doi: 10.1177/107327481502200420. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Martin D. Implementation of the Caribbean Cancer Registry Hub. National Cancer Institute. n.d. http://www.naaccr.org/AC2015/Presentations/53.pdf. Accessed 7 July 2016.
- 82.Pan American Health Organization, CARMEN. Proposed PAHO plan of action for cancer prevention and control 2008–2015. 2008. http://www.cuidadospaliativos.org/archives/PAHO_Cancer_Plan.pdf. Accessed 11 Sept 2014.
- 83.Jones JR, Kogan MD, Singh GK, Dee DL, Grummer-Strawn LM. Factors associated with exclusive breastfeeding in the united states. Pediatrics. 2011;128(6):1117–25. doi: 10.1542/peds.2011-0841. [DOI] [PubMed] [Google Scholar]
- 84.Mohammed ES, Ghazawy ER, Hassan EE. Knowledge, attitude, and practices of breastfeeding and weaning among mothers of children up to 2 years Old in a rural area in El-minia governorate, Egypt. J Fam Med Prim Care. 2014;3(2):136–40. doi: 10.4103/2249-4863.137639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Dubois L, Girard M. Social determinants of initiation, duration and exclusivity of breastfeeding at the population level: the results of the Longitudinal Study of Child Development in Quebec (ELDEQ 1998–2002) Can J Public Health Rev Can Santé Publique. 2003;94(4):300–5. doi: 10.1007/BF03403610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Boccolini CS, Carvalho ML de, Oliveira MIC de, Boccolini CS, Carvalho ML de, Oliveira MIC de. Factors associated with exclusive breastfeeding in the first six months of life in Brazil: a systematic review. Rev Saúde Pública. 2015; doi:10.1590/S0034-8910.2015049005971. [DOI] [PMC free article] [PubMed]
- 87.Monteiro C, Erly M, Conde W, Popkin B. Socioeconomic status and obesity in adult populations of developing countries: a review. Bull World Health Organ. 2004;82(12):891–970. [PMC free article] [PubMed] [Google Scholar]
- 88.Loring B, Robertson A. Obesity and inequities: Guidance for addressing inequities in overweight and obesity. 2014. http://www.euro.who.int/__data/assets/pdf_file/0003/247638/obesity-090514.pdf. Accessed 29 May 2016.
- 89.Dinsa G, Goryakin Y, Fumagalli E, Suhrcke M. Obesity and socioeconomic status in developing countries: a systematic review. Obes Rev. 2012;13(11):1067–79. doi: 10.1111/j.1467-789X.2012.01017.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Loring B. Alcohol and inequities: guidance for addrsesign inequities in alcohol-related harm. 2014. http://www.euro.who.int/__data/assets/pdf_file/0003/247629/Alcohol-and-Inequities.pdf. Accessed 29 May 2016.
- 91.World Health Organization. Global status report on alcohol and health, 2014. 2014. http://apps.who.int/iris/bitstream/10665/112736/1/9789240692763_eng.pdf. Accessed 29 May 2016.
- 92.Reid SD. Time for a regional alcohol policy – a literature review of the burden of normative alcohol use in the Caribbean. J Public Health Policy. 2015;36(4):469–83. doi: 10.1057/jphp.2015.27. [DOI] [PubMed] [Google Scholar]
- 93.Ligeon C, Gregorowicz P, Jolly CM. Factors influencing alcohol consumption in the Caribbean and Latin American countries. In Puerto Rico: Caribbean Agro-Economic Society. 2007. Available from: http://ageconsearch.umn.edu/handle/36956. Accessed 7 July 2016.
- 94.Rehm J. The need for alcohol policy in the Caribbean. n.d. http://www.healthycaribbean.org/newsletters/oct-2014/The-need-for-alcohol-policy-in-the-Caribbean.pdf. Accessed 29 Mar 2016.
- 95.Sebena R, El Ansari W, Stock C, Orosova O, Mikolajczyk RT. Are perceived stress, depressive symptoms and religiosity associated with alcohol consumption? A survey of freshmen university students across five European countries. Subst Abuse Treat Prev Policy. 2012;7:21. doi: 10.1186/1747-597X-7-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Drabble L, Trocki KF, Klinger JL. Religiosity as a protective factor for hazardous drinking and drug use among sexual minority and heterosexual women: findings from the national alcohol survey. Drug Alcohol Depend. 2016;161:127–34. doi: 10.1016/j.drugalcdep.2016.01.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Miller L, Davies M, Greenwald S. Religiosity and substance use and abuse among adolescents in the national comorbidity survey. J Am Acad Child Adolesc Psychiatry. 2000;39(9):1190–7. doi: 10.1097/00004583-200009000-00020. [DOI] [PubMed] [Google Scholar]
- 98.World Health Organization. STEPwise approach to noncommunicable disease risk factor surveillance (STEPS) 2016. http://www.who.int/chp/steps/riskfactor/en/. Accessed 12 July 2016. [DOI] [PMC free article] [PubMed]
- 99.Healthy Caribbean Coalition. A civil society strategic plan of action for prevention & control of NCDs for countries of the Caribbean community 2012–2016. 2012. http://healthycaribbean.org/Strategic-Plan-2012-16/HCC_Strategic_Plan_2012-16.pdf. Accessed 2 June 1016.
- 100.Fuster V. Grenada Heart Project - Community Health Action to Encourage Healthy Behaviors (GHP CHANGE). 2016. https://clinicaltrials.gov/ct2/show/NCT02428920. Accessed 2 Oct 2016.
- 101.Blum RW, Halcón L, Beuhring T, Pate E, Campell-Forrester S, Venema A. Adolescent Health in the Caribbean: Risk and Protective Factors. Am J Public Health. 2003;93(3):456–60. doi: 10.2105/AJPH.93.3.456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Department of Statistics. Bahamas Living Conditions Survey 2001. Nassau, The Bahamas: Department of Statistics. 2004. http://www.centralbankbahamas.com/download/BLCS%202001%20poverty.pdf. Accessed 22 Feb 2016.
- 103.Bunker CH, Patrick AL, Konety BR, Dhir R, Brufsky AM, Vivas CA, et al. High prevalence of screening-detected prostate cancer among Afro-Caribbeans: the Tobago Prostate Cancer Survey. Cancer Epidemiol Biomark Prev Publ Am Assoc Cancer Res Cosponsored Am Soc Prev Oncol. 2002;11(8):726–9. [PubMed] [Google Scholar]
- 104.Fox K, Gordon-Strachan G. Jamaican Youth Risk and Resiliency Behaviour Survey 2005. 2007. Report No.: TR-07-58. Available from: http://www.cpc.unc.edu/measure/resources/publications/tr-07-58. Accessed 22 Feb 2016.
- 105.McCaw-Binns A, Ashley D, Samms-Vaughan M, Wilks R, Ferguson T, Younger N, et al. Cohort Profile: The Jamaican 1986 Birth Cohort Study. Int J Epidemiol. 2011;40(6):1469–76. [DOI] [PubMed]
- 106.Division of Population Health, Center for Chronic Disease Prevention and Health Promotion. Behavioral Risk Factor Surveillance System. 2016. http://www.cdc.gov/brfss/index.html. Accessed 2 Oct 2016.
- 107.Cooper R, Rotimi C, Ataman S, McGee D, Osotimehin B, Kadiri S, et al. The prevalence of hypertension in seven populations of west African origin. Am J Public Health. 1997;87(2):160–8. doi: 10.2105/AJPH.87.2.160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Davila AL, Ramos Gi, Mattei H. Puerto Rico Encuesta de Salud Reproductiva 1995–1996. Division of Reproductive Health-Centers for Disease Control and Prevention. 1998. http://stacks.cdc.gov/view/cdc/8235. Accessed 2 Oct 2016.
- 109.National Hygiene, Epidemiology and Microbiology Institute. Encuesta Nacional de Factores de Riesgo y Actividades Preventivas de las Enfermedades no Trasmisibles. Havana: Ministry of Public Health. 2002. Report No.: 2.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
“Study Protocol”, which details the study protocol for the systematic review. (PDF 1800 kb)
“Search Strategy”, which details the search strategies of the database. (PDF 469 kb)
Data Availability Statement
The data that support the findings of this study are available from the databases used in the study but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of the original study author.