

Abstract
Purpose
To summarize the recent literature describing the application of modern technologies in the study of patients with geographic atrophy (GA) secondary to age-related macular degeneration (AMD).
Methods
Review of the literature describing the terms and definitions used to describe GA, imaging modalities used to capture and measure GA, and the tests of visual function and functional deficits that occur in patients with GA.
Results
In this paper we describe the evolution of the definitions used to describe GA. We compare imaging modalities used in the characterization of GA, report on the sensitivity and specificity of the techniques where data exist, and describe the correlations between these various modes of capturing the presence of GA. We review the functional tests that have been used in patients with GA, and critically examine their ability to detect and quantify visual deficits.
Conclusion
Ophthalmologists and retina specialists now have a wide range of assessments available for the functional and anatomic characterization of GA in patients with AMD. To date, studies have been limited by their unimodal approach and we recommend that future studies of GA use multimodal imaging. We also suggest strategies for the optimal functional testing of patients with GA.
Keywords: Age-related macular degeneration, geographic atrophy
Introduction
In patients with age-related macular degeneration (AMD), geographic atrophy (GA) manifests as sharply demarcated areas of loss of the retinal pigment epithelium (RPE), choriocapillaris, and overlying photoreceptors that develop primarily in the macular retina and expand over time.1, 2 With no proven treatments, GA represents an important unmet need as it leads to visual impairment and affects more than 5 million people worldwide.3 It has been estimated that by the year 2020, a projected 196 million individuals will suffer from AMD, and that this number will increase to 288 million by the year 2040.4 A 2014 meta-analysis reported that approximately half of patients with late-stage AMD have GA.4 The prevalence data on GA in this study were limited, and the authors noted that this estimate was based on data from only 8 of the 39 population based studies included in the analysis. A more recent meta-analysis based on data in the United States reported that the incidence of GA and neovascular AMD were 1.9 and 1.8 per 1000 American whites aged ≥50 years.5 Prevalence rates for the two forms of advanced AMD were comparable across all age groups.
The natural history of AMD has been studied extensively. In the early stages, characteristic findings are the presence of drusen, which can manifest with or without RPE irregularities (hypopigmentation or hyperpigmentation).6 These features do not result in overt vision loss although functional deficits can be detected using appropriately designed psychophysical tests. The risk of progression of early AMD to intermediate and late stages may depend on ocular factors such as RPE depigmentation, drusen size, 7, 8 and presence of reticular pseudodrusen (RPD). 9 Higher prevalence of RPD has been reported in patients with GA compared with early, intermediate, or no AMD,10–13 with the presence of RPD conferring a hazard ratio for progression to GA as high as 4.9.9 As AMD progresses there can be profound effects on visual function (e.g. when GA involves the central retina), including the presence of scotoma in the visual field, impaired facial recognition, and compromised reading ability.1
Some data suggest that in patients who have developed GA, more than a third will lose three or more lines of visual acuity on the standard eye chart within 2 years, due to the progressive loss of retinal tissue.14 Vision loss is more likely when the GA involves the central macula; more than half of patients with GA encroaching upon the fovea will suffer this severity of vision loss in the same time frame when compared to extrafoveal GA.14 Even when GA is not center-involving, patients can suffer significant deficits in visual function, such as compromised reading ability and impaired vision in dim lighting.15 The occurrence of GA with concomitant choroidal neovascularization (CNV) is not uncommon, and is associated with an even greater risk of severe vision loss than GA alone.7, 16, 17 Sunness et al showed that 86% of eyes with GA that developed CNV lost three or more lines of visual acuity over 2 years, compared to only 27% in eyes with GA that did not develop CNV.18
The pathophysiology of GA is influenced by a number of factors including age, smoking, and body mass index. Genetic susceptibility is now increasingly recognized as an important contributor to AMD and more than 19 genetic polymorphisms have been demonstrated to influence AMD risk. Of note, five of these genetic variants are encoded by genes that modulate the complement system, and four of those are within the alternative complement pathway.19–21 Inflammatory processes are hypothesized to play a key role in AMD, including those mediated by complement,22–26 and may contribute to the eventual loss of the choriocapillaris, photoreceptors, and retinal pigment epithelium (RPE) cells.27–29
In the absence of RPE, photoreceptors become nonviable and therefore areas of GA that are identified using imaging techniques correspond to scotomas in the visual field.30 In a proportion of eyes, GA can grow in a unique foveal-sparing pattern that tends to involve the fovea only late in the course of the disease.1, 15, 16, 31, 32 This type of GA may not result in any worsening of best-corrected visual acuity (BCVA) as the center of the fovea is preserved. BCVA is widely accepted by the clinical community and regulatory authorities worldwide as a key measure of visual function and represents the gold standard by which the efficacy of treatment is judged. However, BCVA is a measure of central acuity of the fovea and does not assess all nuances of comprehensive visual function. The drawback of relying solely on BCVA as a measure of ocular health was shown elegantly by Sunness et al who demonstrated that when GA was present in eyes with BCVA 20/50 or better, other features of visual function were considerably impaired. These included contrast sensitivity, low-luminance BCVA, and reading speed.15 Impairment of visual function can also be detected and monitored using microperimetry, even in patients with preserved BCVA.33, 34 BCVA by itself does not adequately capture the visual deficits experienced by patients with foveal-sparing GA. Therefore clinical studies involving patients with GA that aim to quantify changes in visual function and correlate them with disease worsening will need to incorporate additional endpoints that account for the underlying pathophysiologic processes of the disease.
A number of existing and new technologies enable the quantitative morphological assessment of GA, including color fundus photography (CFP), fundus autofluorescence (FAF), and optical coherence tomography (OCT). In addition, the armamentarium of functional assessments beyond BCVA now include multifocal electroretinography (mfERG); microperimetry, low luminance visual acuity (LLVA), reading speed, contrast sensitivity, and patient-centered outcome measures. In this review, we will summarize the recent literature describing the application of these techniques to the study of patients with GA secondary to AMD.
Methods
PubMed literature searches were conducted to identify articles describing the study of GA secondary to AMD using anatomic or functional measures. Broad initial searches encompassed all techniques for evaluation of retinal anatomy; anatomic techniques identified for coverage in the review (CFP, FAF, angiography, and OCT) were those that are most widely implemented in the study of GA. Literature searches for data describing functional measures were based on broad initial searches for studies assessing visual function in AMD, with subsequent searches deriving from terms and references generated within these results based on prevalence of use (e.g. mfERG, microperimetry, LLVA, reading speed, and patient-reported outcome measures). Search terms encompassed the broader AMD population to capture titles not explicitly mentioning GA but possibly containing this subgroup (e.g. ((age[ti] AND macular[ti] AND degeneration[ti]) AND (fundus[ti] AND (color[ti] OR autofluoresc*[ti]))). In addition to PubMed searches, a search of clinicaltrials.gov was conducted to tabulate active GA trials as of March 1, 2016 with clinical endpoints involving GA lesion assessment.
Morphological Measures of Geographic Atrophy
The criteria for diagnosis of GA differs across grading systems and imaging modality. The best established grading system, which was developed in the 1980s, was based on color image grading. However, the definitions have not remained constant and there has been continual change in the parameters used to define the presence of GA on color fundus images. The first clear definition of GA was proposed by the Wisconsin Age-Related Maculopathy Grading System in which GA was defined as an area of pallor in the fundus with visibility of the underlying choroidal blood vessels and sharply defined borders, occupying a diameter ≥175 μm.6, 35, 36 Subsequently the definitions were used to identify the presence of GA by the International Age-Related Maculopathy Grading System, and the Age-Related Eye Disease Study (AREDS). However, other studies have used larger definitions of GA. The Complications of Age-Related Macular Degeneration Prevention Trial (CAPT) specified a diameter >250 μm for definition of GA,37 and in the AREDS2 study the minimum diameter of the area was increased to 433 μm.38 Currently there is no international consensus on the minimum diameter for the diagnosis of GA.
In addition, changes have been proposed in the grading of AMD severity level with regards to the presence of GA. In the AREDS grading system, the presence of GA qualifies patients as having either intermediate or advanced AMD, depending on whether or not there is central involvement.6 In the classification system recently developed by the Beckman Initiative for Macular Research, the presence of any GA regardless of location qualifies as evidence of advanced AMD.39
Color Fundus Photography
Morphological endpoints are important outcomes in clinical trials of all stages of AMD, as they are based on directly measurable physical characteristics. As such they generate reproducible, reliable, objective clinical information. Morphological endpoints are unaffected by patient compliance, comprehension, or cognitive status, which can influence psychophysical or functional endpoints.
Seminal research in the characterization of GA by CFP was accomplished in the natural history studies by Sunness et al, and by the AREDS research group.6, 40, 41 Using color images captured on 35 mm film, these studies helped to shape the methodology for quantification of GA area. AREDS recruited more than 4700 participants with and without AMD for the study of the natural history and the role of mineral and antioxidant supplements in disease progression.42 The CFP grading system implemented in AREDS was an extension of the Wisconsin Age-Related Maculopathy Grading System.35 A standardized grid was used for size estimation of the retinal features of early and late AMD; eyes were then assigned to one of four severity levels according to the size and type of abnormalities observed on CFP.6 In the initial AREDS classification scheme, patients with GA were classified as either severity level 3 (intermediate) or 4 (advanced) based on foveal involvement; more recently, Ferris et al have proposed the updated and simplified Beckman AMD classification scheme in which eyes with GA regardless of location are categorized as late AMD (Figure 1).39 At the time of AREDS, grading was performed by trained, certified technicians under the supervision of ophthalmologists, and this method continues to be used in present studies. More recently with the advent of digital photography, several image analysis technologies are being used to explore the possibility of automated delineation of the area of GA.43–47
Fig 1.

AREDS macular grid and Beckman AMD severity grading system using CFP. Brighter areas on CFP correspond to GA and loss of pigmented epithelium. Standardized circles C0 (63 μm) and C1 (125 μm) are used for determination of drusen size.
In patients with AMD, areas of GA are identified with CFP in part by their distinctly different color (depigmented) compared to adjacent areas of healthy retina (Figure 1), as well as by the presence of sharply demarcated borders and increased visibility of choroidal vessels.40 Key characteristics of imaging techniques for quantitation of GA include the ability of the technique to reproducibly measure GA area and ability to predict progression of GA area. In this regard, CFP has certain limitations that have led to the complementary use of other imaging modalities for the quantitation of GA area. One important limitation of CFP is the limit of resolution with this technology. CFP uses light in the visible spectrum to capture the fundus image and identify the boundaries of the various structures by their color. However, it is challenging to demarcate areas of distinct morphology but indistinct color. For example, with CFP it is difficult to distinguish GA that has a pale yellowish hue from either depigmented RPE or areas of drusen that also appear yellowish.48 Good stereophotography may facilitate quantification by allowing the borders of GA lesions to be seen more sharply; however, it is not always possible to obtain high-quality stereophotographs in the context of large studies. Therefore the reproducibility of GA measurements with CFP can be less compared to other methodologies such as FAF.49 As a result, other imaging technologies have come into use as adjunctive measures of GA morphology. Another limitation of CFP is difficulty in visualizing reticular pseudodrusen, which are known to be associated with an increased risk of GA.
Fundus Autofluorescence
FAF is the current standard imaging technology for the morphological assessment of GA, and is often used in conjunction with CFP. In this technique, the fluorescence signal originates from lipofuscin, a naturally occurring compound within RPE cells.50 Lipofuscin is a heterogeneous, cross-linked material composed of oxidized protein, lipid, metal ions, and sugar residues that form intracellular aggregates in RPE cells.51, 52 Lipofuscin absorbs light of a specific wavelength and emits the absorbed light at a different wavelength,53 and this property is exploited to image the RPE (Figure 2). In the healthy eye, the pattern of autofluorescence is distributed uniformly, diminishing toward the fovea due to absorption by macular pigment. In eyes with GA, distinctly dark areas are observed where the atrophy of lipofuscin-containing RPE cells leaves an absence of fluorescent signal. Due to the contrasting boundaries between areas of absent and surviving RPE in FAF images, this modality offers better delineation in the identification of atrophic regions.49, 54, 55 For imaging of central GA, the use of green-light FAF may offer a more accurate means of measuring GA area than blue-light FAF.56
Fig 2.

Assessment of GA using FAF. In a healthy retina, lipofuscin autofluorescence is distributed uniformly in a pattern that diminishes toward the fovea. In contrast, distinct dark areas are evident in the eye with GA, where death of lipofuscin-containing RPE cells leaves a region of hypofluorescence. Different FAF patterns in the junctional zone have been correlated with varying risk of GA progression.55 IQR, interquartile ratio.
In addition, FAF provides an important diagnostic not currently available with other imaging modalities.55 In the junctional zone (i.e., the boundary between dead and surviving RPE regions), bright areas of hyperfluorescence are often observed. These hyperfluorescent areas are believed to represent regions of cells that are stressed and more likely to become atrophic.57, 58 In support of this observation is the finding that abnormal autofluorescence at the boundary of the dead and surviving RPE predicts the risk of GA progression,58, 59 and furthermore specific patterns of hyperfluorescence also predict the risk of GA worsening (Figure 2).55, 60, 61
The predictive power of FAF imaging makes it a useful assessment for the study of GA in clinical trials, not only for the evaluation of treatment efficacy, but potentially for defining inclusion criteria. For example, use of FAF for identification of eyes at greater risk for rapid growth of GA area could allow for selection of a patient population that enables a shorter trial duration, requires fewer patients, and still allows for appropriate statistical power.58
Given its more recent emergence and adoption in clinical practice, characterization of GA by FAF has been quantitatively evaluated in comparison with fundus photography. In a single-site study of 10 patients with GA, we (S.R. Sadda, Doheny Image Reading Center) compared the agreement between GA area measured by masked readers at a reading center using FA and CFP, and found excellent agreement between the two imaging modalities (Spearman correlation, r = 0.986).62 In this study, we showed that GA areas obtained by FAF were larger by 0.178 ± 0.45 mm2 (P = 0.0001).
Khanifar et al evaluated data from 72 eyes with GA for which FAF images had been acquired and graded along with CFP photos.49 To compare these imaging modalities, three independent graders calculated the total area of GA using both techniques. The results showed that the two instruments had very good agreement. Differences between GA area as measured by FAF and CFP were close to zero, with FAF-CFP correlation coefficients of 0.85, 0.87, and 0.93 across the three graders. In this study a small (nonsignificant) trend was observed; in eyes with very little GA, FAF tended to measure larger areas than CFP. The authors note that the enhanced contrast of FAF may allow greater sensitivity versus CFP for detection of small areas of atrophy, while this enhanced sensitivity may be accompanied by somewhat reduced accuracy in patients with very small regions of atrophy (potentially overestimating the actual GA area to some extent).49, 63 However, the average measurement differences between imaging modalities was small.
In the Geographic Atrophy Progression (GAP) study, FAF and CFP measurements were available for 321 patients.61 From baseline through 18 months, CFP measured significantly larger GA lesion areas than FAF, but the correlation between the two modalities was very high (r=0.89–0.94). In addition, the lesion size change from baseline was similar as measured by FAF and CFP at month 6 (0.78–0.88 mm2, P=0.164), month 12 (1.57–1.85 mm2, P=0.023), and month 18 (3.17–3.14 mm2, P=0.944). In practice and in clinical studies, FAF continues to be used as an integral measurement for the observation of GA area in patients with AMD (Table).
Table.
Ongoing Phase 2 and 3 Clinical Trials Evaluating GA lesions Registered on ClinicalTrials.gov as of March 1, 2016
| Study Name, NCT Identifier | Study Type | Enrollment | Primary Outcome Measure* |
|---|---|---|---|
| A Study Investigating the Efficacy and Safety of Lampalizumab Intravitreal Injections in Patients With Geographic Atrophy Secondary to Age-Related Macular Degeneration (CHROMA), NCT02247479 | Phase 3 Interventional | 936 | Change in GA area, as assessed by FAF |
| A Study Investigating the Safety and Efficacy of Lampalizumab Intravitreal Injections in Patients With Geographic Atrophy Secondary to Age-Related Macular Degeneration (SPECTRI), NCT02247531 | Phase 3 Interventional | 936 | Change in GA area, as assessed by FAF |
| A Phase 2b/3 Multicenter, Randomized, Double-Masked, Dose-Ranging Study Comparing the Efficacy and Safety of Emixustat Hydrochloride (ACU-4429) With Placebo for the Treatment of Geographic Atrophy Associated With Dry Age-Related Macular Degeneration (SEATTLE), NCT01802866 | Phase 2b/3 Interventional | 480 | Change in GA area |
| A Randomized, Double Blind, Placebo Controlled Study Evaluating ORACEA® in Subjects With Geographic Atrophy Secondary to Non-Exudative Age-Related Macular Degeneration (TOGA), NCT01782989 | Phase 2/3 Interventional | 286 | Rate of enlargement in area of geographic atrophy in the study eye during the treatment period |
| A Safety and Efficacy Study of Brimonidine Intravitreal Implant in Geographic Atrophy Secondary to Age-related Macular Degeneration (BEACON), NCT02087085 | Phase 2 Interventional | 300 | Change from baseline in atrophic lesion area in the study eye |
| A Study to Evaluate the Safety and Clinical Response of Subretinal Administration of CNTO 2476 in Participants With Geographic Atrophy (PRELUDE), NCT02659098 | Phase 2 Interventional | 255 | Change in GA lesion growth as measured by FAF (secondary endpoint) |
| Study of APL-2 Therapy in Patients Geographic Atrophy (FILLY), NCT02503332 | Phase 2 Interventional | 240 | Change in square root GA lesion size from baseline, as measured by FAF |
| Clinical Study to Investigate Safety and Efficacy of GSK933776 in Adult Patients With Geographic Atrophy Secondary to Age-related Macular Degeneration, NCT01342926 | Phase 2 Interventional | 184 | Rate of change in area of GA from baseline |
| CLG561 Proof-of-Concept Study as a Monotherapy and in Combination With LFG316 in Subjects With Geographic Atrophy (GA), NCT02515942 | Phase 2 Interventional | 114 | (1) Safety events and (2) change in GA lesion size from baseline, as measured by FAF |
| A Study of Lampalizumab Intravitreal Injections Administered Every Two Weeks or Every Four Weeks to Patients With Geographic Atrophy, NCT02288559 | Phase 2 Interventional | 90 | Mean change in GA area, as measured by FAF |
| The Effect of Metformin on the Progression of Geographic Atrophy in Patients With Age-related Macular Degeneration, NCT02684578 | Phase 2 Interventional | 100 | Change in GA area as measured by FAF |
| Evaluation of Oral Minocycline in the Treatment of Geographic Atrophy Associated With Age-Related Macular Degeneration, NCT02564978 | Phase 2 Interventional | 62 | Rate of change in GA area as measured by FAF |
| A Multicenter, Prospective Epidemiologic Study of the Progression of Geographic Atrophy Secondary to Age-Related Macular Degeneration (PROXIMA-A), NCT02479386 | Observational | 360 | Primary outcomes evaluate visual function; secondary outcomes include measurement of GA area by FAF |
| Prospective Natural History Study of Fundus Autofluorescence Imaging in Age-related Macular Degeneration (FAM-Study) Using Confocal Scanning Laser Ophthalmoscopy, NCT00393692 | Observational | 300 | Change of GA size from baseline, as assessed by FAF |
| An Epidemiologic Study of Disease Progression in Patients With Geographic Atrophy Secondary to Age-Related Macular Degeneration (Proxima B), NCT02399072 | Observational | 200 | Change in GA area, as assessed by FAF |
| Directional Spread in Geographic Atrophy (DSGA), NCT02051998 | Observational | 130 | Change of GA size from baseline |
Unless otherwise specified as a secondary endpoint
A downside of FAF imaging is that the bright imaging light may be uncomfortable for patients, particularly when using shorter-wavelength blue light. Concerns have been raised that blue light (even within the ANSI standards) may be harmful for patients with susceptible diseases of the retina.64–66 Also, due to absorption by macular pigment, it is usually not possible to determine the extent of foveal involvement by the atrophic lesion using blue light autofluorescence alone.
Optical Coherence Tomography
Imaging techniques such as CFP and FAF provide 2-dimensional (2-D) images taken from an axial perspective, with limited depth information. OCT on the other hand is a tomographic technique that yields 2-D and 3-D high-resolution information. Most commonly, 2-D high-resolution OCT B-scans are used to provide important cross-sectional information for assessment of retinal layers (Figure 3A), evaluation of GA lesion area (Figure 3B), and measurement of GA lesion growth (Figure 3C). OCT data can also be summed in the axial direction to yield en face projection images for comparison with CFP or FAF. In en face OCT, 3-D images are constructed from a series of 2-D longitudinal cross-sections of retinal layers (B-scans).
Fig 3.

Characterization of GA using SD-OCT. A. 2-D OCT of a healthy eye showing individual retinal layers. B. 2-D OCT of an eye with GA showing degradation of RPE and neural layers and enhancement of signal from the choroid. C. 2-D OCT for quantitation of GA progression. Highlighted green area corresponds to retina lost to atrophy from baseline to follow-up, allowing measurement of change in retinal thickness and GA lesion boundaries. RNFL, retina nerve fiber layer; GCL, ganglion cell layer; IPL, inner plexiform layer; INL, inner nuclear layer; OPL, outer plexiform layer; ONL, outer nuclear layer (1 = external limiting membrane; 2 = inner photoreceptor layer; 3 = photoreceptor outer segment-RPE interdigitation; 4 = RPE-Bruch’s membrane complex; 5 = choriocapillaris and choroid).
Time-domain OCT became commercially available in 1996 with the Zeiss Stratus (Carl Zeiss Meditec, Dublin, CA). This instrument provided ophthalmologists the opportunity to view cross-sectional details of the human retina in vivo for the first time.67 Although this was a significant advancement in the diagnosis and study of retinal disease, the resolution and technical capabilities of time-domain tomography limited its application.68 By 2003 successive advancements in OCT technology led to the commercial availability of spectral domain OCT (SD-OCT), which has sufficient speed and resolution for better assessment of individual retinal layers and has enhanced our understanding of the cellular events that lead to GA.67
In healthy eyes, the individual layers of the retina appear on 2-D OCT as well-defined bands (Figure 3A). The characteristic defects of GA manifest as a sharply demarcated region of degradation in the RPE and photoreceptor layers, and increased reflectivity from the underlying choroid and choriocapillaris (Figure 3B).69 Thinning and apposition of the overlying nuclear layer is also evident above the areas of RPE atrophy.70 In many eyes with GA, wedge-shaped hyporeflective structures between Bruch’s membrane and the outer plexiform layer may become evident on OCT.71, 72 These structures could be useful for defining the OCT boundaries of photoreceptor layers, which may be important in clinical trials of therapies that aim to preserve the viability of this retinal layer in patients with GA.72
The high-resolution imaging of retinal microstructure afforded by SD-OCT is also helpful in the assessment of the progression and pathophysiology of GA.70, 73 In one study, data were compared in 20 subjects with GA for whom both SD-OCT macular volume and FAF images had been acquired (on separate instruments).73 This study demonstrated good agreement between GA area calculated by automated analysis of SD-OCT data and that calculated by FAF. In another study, a prospective evaluation of 46 eyes with GA showed that combined FAF and SD-OCT techniques using the Spectralis instrument (Heidelberg Engineering, Heidelberg, Germany) facilitated the accurate serial imaging of the same retinal location across multiple office visits over a period of months. This technique revealed previously undetectable dynamic changes in the retina of patients with GA.70 More recently, a false-color fusion method has been developed to allow simultaneous visualization and quantification of both drusen and GA in SD-OCT images.74
The rate of GA area progression in eyes with AMD has been evaluated using SD-OCT to image the photoreceptor and RPE layers of the retina.75 Thirty patients with GA were followed for 1 year, with assessment of GA area at baseline and worsening over time measured by three graders using an axial projection of the sub-RPE layer. Separately, the SD-OCT signal corresponding to the en face photoreceptor layer was also visualized. When these two layers were superimposed to examine the relationship between photoreceptors and GA, areas showing degradation of the photoreceptor ellipsoid zone (or inner segment-outer segment junction line) predicted where the GA area would later expand. The authors noted the important implications of this technique for future clinical trials that use reduction of GA progression as a primary endpoint. For example, it was suggested that if photoreceptor degradation inevitably leads to growth of GA into these areas, then regardless of effective intervention, this additional area of photoreceptor loss should be taken into account and adjusted for when calculating the primary outcome measure.
At present, these emerging SD-OCT methods for assessment of GA area and retinal morphology are not optimized nor standardized for extensive use in clinical trials, though they hold promise for the future. As experience with new SD-OCT protocols and algorithms increases and automated software programs are refined, the ability to study and monitor GA lesions by SD-OCT will become more widespread. OCT imaging may also contribute to a better understanding of underlying pathologic mechanisms in AMD and GA, may suggest new biomarkers related to disease progression, and might potentially indicate new therapeutic targets in AMD.
Contrast-Based Imaging (Angiography)
Fluorescein angiography (FA) and indocyanine green angiography (ICGA) are techniques commonly used to assess neovascularization in patients with neovascular AMD.76–78 FA involves intravenous administration of the dye fluorescein, followed by fluorophore excitation with blue light. As the dye reaches the eye, selective imaging of the retinal vasculature reveals abnormal blood vessel characteristics (e.g., retinal nonperfusion) and subretinal vascular defects (e.g., CNV lesions) as leakage of the dye diffuses through the retina. While the primary role of FA in the assessment of GA is to exclude the presence of CNV, angiography can also provide high contrast for delineation of the GA lesion as areas of atrophy typically show well-demarcated areas of staining, whereas areas of depigmentation or RPE disturbance may only show poorly demarcated hyperfluorescence that can fade over time.
Direct imaging of the choroidal vasculature with FA is hampered by rapid leakage from the overlying choriocapillaris and absorption of dye fluorescence by RPE. In contrast, the ICGA emission wavelength is longer and less prone to absorption by RPE. Its pharmacodynamics are characterized by nearly complete binding to plasma protein, which slows efflux from the choriocapillaris, resulting in better imaging of subretinal vasculature.79
In patients with GA, ICGA reveals lesion boundaries in addition to distinct pathophysiologic findings that are not evident using other imaging modalities.80 These may include direct visualization of the choroidal vasculature81 and aneurysms of choroidal vessels.82 ICGA may aid in differential diagnoses, for example through differentiation of GA versus occult CNV lesions83 or Stargardt disease.84 Age at clinical presentation may be a helpful distinction between GA due to AMD and Stargardt disease, whereas imaging with FA and ICGA reveals striking differences between the two modalities. Stargardt atrophy most often presents as hypofluorescence on both FA and ICGA (dark atrophy), whereas GA lesions due to AMD typically present as hypofluorescence only on FA.84
Functional Tests
Multifocal Electroretinography
Direct measurement of photoreceptor signaling within the retina in response to a light stimulus can be measured using focal electroretinography (fERG) and mfERG.85, 86 This technology uses electrodes in contact with the cornea during testing. In multifocal techniques, upon application of light stimuli in regular patterns that scan the retina, photoreceptor signaling is detected by the corneal electrode. By varying the intensity of the light stimulus, the functionality and sensitivity of specific areas of the retina can be mapped (Figure 4).
Fig 4.
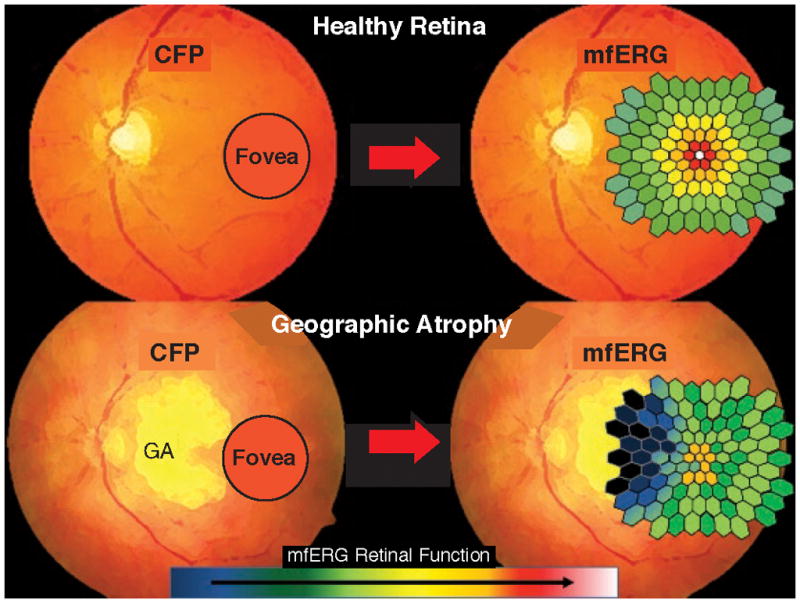
Schematic illustration of the assessment of retinal function using mfERG in healthy retina (top) and in GA (bottom). When the mfERG map is superimposed on the CFP image, the color gradient of the mfERG grid shows the most intense signal in healthy retina at the fovea. In eyes with AMD, decreasing retinal function is shown as darker colors in areas corresponding to GA.
A growing body of literature has described the application of this technique to the study of eyes with AMD. One of the earliest applications of mfERG in AMD demonstrated that this technique can be used to detect differences in retinal electrophysiology in patients with early AMD compared with controls.87 Fifteen eyes with early AMD and drusen were studied with mfERG and compared with both asymptomatic fellow eyes and age-matched controls. Measurable differences in mfERG signals were detected in eyes with early AMD, demonstrating the utility of this technology for early detection of visual defects in patients with AMD.
A key retinal abnormality in patients with GA is the loss of photoreceptors, visible on SD-OCT.1, 75 Retinal function data attainable via mfERG have been compared with SD-OCT abnormalities corresponding to the photoreceptor layer.88 In 29 patients with early AMD, the intensity of the photoreceptor layer on SD-OCT was significantly diminished in eyes with early AMD versus control eyes, and was significantly correlated with mfERG signal. In this study the morphological observation of photoreceptor degradation on SD-OCT was corroborated by loss of retinal function on mfERG, demonstrating the utility of mfERG for the study of retinal pathophysiology in AMD.
Considering the high prevalence of concomitant RPD in eyes with GA, and the potential role of RPD in the pathophysiology of GA, the effects of RPD on retinal function may be important as an early measure of visual function impairment along the AMD disease continuum. Some studies have begun to explore the effects of RPD on visual function using mfERG. Alten et al evaluated the effect of RPD on retinal function as measured by mfERG at baseline and at 12 month follow-up.89, 90 In these two studies, fellow eyes had various manifestations of AMD such as drusen, CNV, or GA, but study eyes had only RPD. The results demonstrated that mfERG sensitivity was not significantly altered by the presence of RPD alone, when compared with healthy control eyes. However, another study found that impaired mfERG sensitivity was detectable in eyes with RPD and concomitant intermediate AMD.91 Univariate and multivariate analyses showed that sensitivity impairment in patients with RPD was detectable in mfERG implicit time, but not in signal amplitude. Considering their results against existing literature, these authors point out the potential confounding effects of instrumentation and methodology on the consistency of mfERG results across studies. Thus, the use of mfERG to evaluate the effects of RPD on retinal function in eyes with AMD remains a subject of ongoing research.
Psychophysical Tests of Visual Function
Electrophysiology is objective, and does not rely on patient cognition, measuring precognitive aspects of the visual system at the level of the retina. Other techniques of function integrate patient cognitive involvement in the measurement process to provide information on visual perception and deficit. Historically, the simplest and most widely used psychometric assessment of visual function has been BCVA. However as noted earlier, in patients with GA, changes may become evident in several measures of visual function before deterioration in BCVA occurs, underlining the importance of multifactorial assessment of visual function. The aim of this section is to describe the recent GA literature regarding other psychometric techniques.
Low Luminance Visual Acuity and Contrast Sensitivity
Another visual acuity metric that has been evaluated in patients with GA is LLVA. In this technique the amount of light transmitted (optical intensity) can be reduced using neutral density filters with a set attenuation placed over the eye to be tested, and the letters seen on a standard illuminated Early Treatment Diabetic Retinopathy Study (ETDRS) visual acuity chart are recorded. Because of the lower luminance created by the filter, LLVA scores are necessarily lower than BCVA and the magnitude of the difference between BCVA and LLVA (defined as the low luminance deficit [LLD]) reveals visual function abnormalities that would not otherwise be apparent by measuring standard BCVA alone. Sunness et al showed that in 91 patients with GA, LLD was a strong predictor of BCVA loss over 2 years, independent of baseline BCVA.92 Even among patients with good baseline BCVA (20/50 Snellen or better), the relative risk of three-line loss of BCVA was 2.88 (95% CI 1.13–7.35) for patients with the worst LLD; 55% of patients with worse LLD lost 3 or more lines of vision at 2 years compared to only 19% with smaller LLD. This study demonstrated that LLVA is an important outcome to be included in clinical trials of patients with GA, and may be a more sensitive measurement for assessing the risk of visual decline than standard BCVA alone.
A similar and related psychometric outcome is contrast sensitivity, often measured using the Pelli-Robson contrast sensitivity chart.93 In this chart, the letters are all the same size, diminishing in contrast from black to grey and further to lighter shades that eventually cannot be distinguished against a white background. Other instruments show alternating black and white lines on a screen (sinusoid gratings).94 In the GA natural history study conducted by Sunness et al, patients with GA and good BCVA (20/50 Snellen or better) had significantly worse contrast sensitivity compared with AMD patients who did not have GA.15 Contrast sensitivity and LLD both may be used to detect abnormal visual function in patients with good BCVA.
Microperimetry
LLVA and contrast sensitivity measure the effect of luminance and contrast on overall visual function, but do not allow for more detailed assessment of function across specific areas of the retina. Because the specific location of GA lesions in the macula or fovea can dictate visual outcomes, this level of detail is important for functional assessments of vision in patients with GA. In recent years, the availability of commercial microperimetry instruments has facilitated the psychometric study of retinal function in greater detail. Akin to mfERG, in microperimetry, specific areas of the retina are stimulated with points of light, and the patient presses a button to acknowledge perception of the stimulus. In addition to identifying functional and nonfunctional areas, stimulus intensity is varied to also identify the relative sensitivity of specific areas of the retina. The fundus is monitored via infrared camera and the fixation point is continuously tracked; thus the sensitivity of the visual field can be mapped to the fundus photo and compared to images obtained with other modalities.
Microperimetry has revealed several key pathophysiologic findings in GA (Figure 5). One study of 18 eyes with GA showed that microperimetric assessment of visual function significantly correlated with progression of the GA lesion area over a 2-year period.95 The number of scotomatous points identified with microperimetry increased over time, and was significantly associated with growth in the GA lesion area. Importantly, this study showed that the sensitivity of functional retina also decreased over time, and this loss of sensitivity was widespread and not limited to areas surrounding GA lesions. Other studies have reported similar findings. For example, although specific measurement of rod function in patients with GA has been relatively unexplored because instrumentation has not been readily available, evidence from histologic studies and rod-targeted perimetry suggests that early loss of rod photoreceptors may be common even at locations far removed from GA lesions.96, 97
Fig 5.
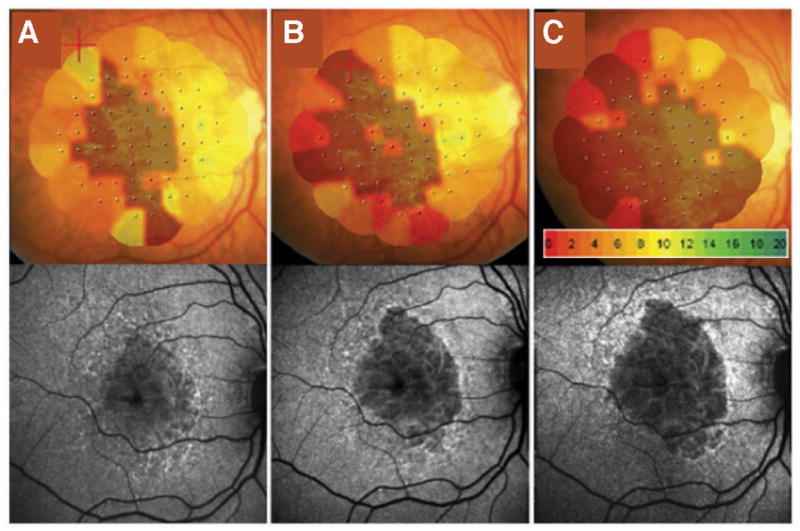
Measurement of retinal function in GA using microperimetry. Color-coded map of retinal sensitivity (top) shows loss of retinal function in darker areas that correspond to GA lesions as assessed by FAF (bottom). Worsening of retinal function is shown over time as lesion area expands from baseline (A), at 12 months (B), and at 24 months (C).
Like mfERG, the utility of microperimetry for assessment of visual function deficits due to the presence of RPD has been reported. Forte et al showed that eyes with only RPD and preserved visual acuity had reduced light sensitivity on microperimetry, compared with control eyes having early AMD.98 Another study evaluated RPD in AMD eyes with small drusen, and also found reduced sensitivity on microperimetry compared with early AMD controls.99 However, RPD did not affect microperimetry sensitivity in eyes with bilateral intermediate AMD. Similar to the application of mfERG for the assessment of retinal function, the role of RPD in AMD is still a key research question. Further studies are needed in patients with AMD to fully understand the effect of RPD on visual function as measured by mfERG and microperimetry. Microperimetry studies have also revealed detail on changes in retinal sensitivity in the pathogenesis of GA. Using microperimetry to assess retinal function in the junctional zone of hyperfluorescence surrounding GA lesions, it has been shown that regions of elevated FAF had significantly lower sensitivity to light stimuli compared with regions of normal FAF.100 Similar results were reported by Scholl et al.101 In this study, authors further differentiated retinal sensitivity in hyperfluorescent regions under photopic and scotopic conditions to selectively probe the sensitivity of rod and cone photoreceptors. Their results demonstrated that scotopic sensitivity loss in hyperfluorescent regions far exceeded photopic loss. Taken together, these data suggest that hyperfluorescent regions of the retina outside of GA lesions demarcate areas of impaired photoreceptor function, and demonstrate the importance of microperimetry in monitoring the development and progression of GA.
Reading Speed
Reading speed can be objectively measured, typically calculated from the number of correctly read words in a paragraph of random words presented for a short, fixed amount of time.102 Two commonly used assessments are the MNREAD and Radner reading charts that have been validated in a number of languages.102–105 The natural history study conducted by Sunness et al showed that even in AMD patients with BCVA ≥20/50, reading speed was significantly poorer in those with GA compared with those having early or intermediate AMD.15, 92 In these patients, poor reading speed was also predictive of future deterioration in BCVA.
Self-Reported Visual Functioning and Quality of Life
Although psychophysical tests (i.e., BCVA, LLVA, contrast sensitivity, microperimetry, reading speed) can reveal specific visual function deficits, they do not capture the entire range of effects that a disease might incur. Therefore patient-centered outcome measures have been developed. These instruments contain a number of items (questions) asking the subject to report the degree of disability experienced, which is recorded on a graded categorical scale. The instruments consist of a variety of domains that explore specific aspects of vision such as near function, distance function, color, etc. Various instruments have been used to examine the effects of visual function deficits on the daily activities of patients with GA.106, 107
A widely used psychometric instrument for assessment of vision-related quality of life is the 25-item Visual Function Questionnaire (VFQ-25) developed by the National Eye Institute.108, 109 Created in 1998 as a 51-item instrument, it has since been refined to 25 items to capture patient-centered vision-related health status among individuals with chronic eye diseases. This questionnaire measures the influence of visual dysfunction on aspects of daily life (e.g., reading the newspaper, finding items on a crowded shelf, driving), as well as broader topics (e.g., emotional well-being, social functioning). While VFQ-25 has been widely implemented in studies involving patients with AMD, the literature has focused on the neovascular AMD population rather than those with GA or GA lesion area worsening. Similarly, other instruments such as the Visual Function Index (VF-14),110 Short Form Health Survey (SF-36),111 and MAC-TSQ have not been well-characterized in the GA population.
Recently a new psychometric instrument for assessment of functional reading has been developed specifically for use in patients with GA. The Functional Reading Independence (FRI) Index is a 7-item questionnaire that evaluates the effect of GA on a patient’s ability to independently perform reading activities. The validation of this instrument was recently reported.112 Among other measures of validity, the FRI Index score correlates with GA lesion size and VFQ-25 score, such that patients with larger GA lesions or lower VFQ-25 scores demonstrate significantly lower mean scores on the FRI Index.112 The FRI Index was also sensitive to increases in GA lesion area.113 Moving forward with the study of functional visual impairment in patients with GA, the FRI Index is currently being implemented in phase 3 GA clinical trials. This instrument is publicly available through Mapi Research Trust. Requests for information or access to the questionnaire may be sent to PROinformation@mapi-trust.org.
Clinical Endpoints in Ongoing GA Trials
For ongoing and future clinical studies of GA, multimodal assessments will facilitate a comprehensive database of information to further our understanding of this disease. The largest ongoing registered phase 3 trials in geographic atrophy are the interventional Chroma and Spectri studies (Genentech/Hoffmann-La Roche). Chroma (NCT02247479) and Spectri (NCT02247531) are evaluating the efficacy and safety of lampalizumab, a monoclonal antibody antigen-binding fragment (Fab) targeting complement Factor D in patients with GA. The primary endpoint of these studies is mean change in GA area assessed by FAF, and as part of a comprehensive assessment these studies will also evaluate potential treatment effect differences using CFP, OCT, microperimetry, reading speed, LLVA, VFQ-25, and the FRI Index.
The ongoing Phase 2b/3 trial SEATTLE (NCT01802866) is evaluating the visual cycle modulator emixustat hydrochloride in patients with GA. This 24-month study will compare the efficacy of emixustat compared with placebo, using a primary endpoint of change from baseline in total GA lesion area. Anatomic endpoints utilized in the phase 2 study included FAF, fundus photography, and FA, thus it is likely these endpoints will be carried forward in SEATTLE. The 24-month Phase 2/3 trial TOGA (NCT01782989) will assess the efficacy of doxycycline versus placebo in GA patients, with a primary outcome of GA enlargement rate. Several other phase 2 studies are also underway (Table), which will evaluate GA lesion area as their primary endpoint. Taken together, these studies will help further our understanding of GA, they will improve characterization of GA and clarify the most sensitive, and appropriate imaging and functional endpoints to monitor disease progression and evaluate potential treatment responses.
Summary
The unique pathologic mechanisms of GA secondary to AMD have important implications for the evaluation of visual function in patients with this disease. As a late-stage manifestation of AMD, GA develops gradually with the formation of scotomas that spare the fovea initially, expanding into the central visual field late in the course of disease.1, 15, 16, 31, 32 The most common assessment of visual function, BCVA, usually fails to reveal the functional deficits experienced by patients with foveal-sparing GA. More appropriate measures of visual function that can topographically map retinal sensitivity and or provide a more global metric of macular function are needed as sensitive outcome measures in GA clinical trials.114
Consequently, a multimodal approach to the assessment of visual function is most appropriate for clinical endpoints in trials involving patients with GA. As highlighted in this review, there have been remarkable advancements in technologies for assessment of GA functional and anatomic deficits, as well as the means of their application. A consensus panel on the quantification of visual acuity has previously suggested that the combined use of measurements such as contrast sensitivity, reading speed, microperimetry, and psychometric questionnaires along with BCVA should be used to more fully assess visual impairment.115 The primary and most rigorous outcomes for tracking disease progression in patients with GA are anatomic endpoints such as CFP, FAF, and OCT. Clinical studies using a multimodal imaging approach will be the most effective means of evaluating the role of RPD in GA, since this approach is best suited to account for the challenges of accurate diagnosis and quantitation of RPD.116
Brief Summary Statement.
Ophthalmologists and retina specialists now have a wide range of functional and anatomic assessments available for the characterization of geographic atrophy in patients with age-related macular degeneration. This review summarizes the recent literature describing the application of modern techniques for the study of geographic atrophy.
Acknowledgments
Third-party writing assistance was furnished by Michael Bennett of Envision Pharma Group, and provided by Genentech, Inc.
Footnotes
Conflict of Interest
SriniVas Sadda has served as a consultant to Genentech, Roche, Allergan, Novartis, Stem Cell Inc, Iconic, Avalanche, Optos, and Carl Zeiss Meditec. Usha Chakravarthy has attended advisory boards for Hoffmann-La Roche and Genentech. Her institution has received grants from Hoffmann-La Roche and she is principal investigator in trials sponsored by Roche. David G. Birch has been a consultant for AGTC, Acucela, Inc., Shire Pharmaceuticals, ISIS/GSK, QLT, and Thrombogenics. Giovanni Staurenghi is principal investigator in trials sponsored by Roche. He is also consultant for Heidelberg Engineering, Quantel Medical, Carl Zeiss Meditec, Alcon, Allergan, Bayer, Boheringer, Genentech, GSK, Novartis, Roche. His institution received grants from Optos, Optovue, Centervue, Heidelberg Engineering, Quantel Medical, Novartis, Carl Zeiss Meditec, Alcon, allergan. He has a patent with Ocular Instruments. Erin Henry is an employee of Genentech, Inc. Christopher Brittain is an employee of F. Hoffmann-La Roche, Ltd.
References
- 1.Sunness JS. The natural history of geographic atrophy, the advanced form of age-related macular degeneration. Mol Vis. 1999;5:25. [PubMed] [Google Scholar]
- 2.Bonilha VL. Age and disease-related structural changes in the retinal pigment epithelium. Clin Ophthalmol. 2008;2:413–424. doi: 10.2147/opth.s2151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Rudnicka AR, et al. Age and gender variations in age-related macular degeneration prevalence in populations of European ancestry: a meta-analysis. Ophthalmology. 2012;119:571–580. doi: 10.1016/j.ophtha.2011.09.027. [DOI] [PubMed] [Google Scholar]
- 4.Wong WL, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health. 2014;2:e106–116. doi: 10.1016/S2214-109X(13)70145-1. [DOI] [PubMed] [Google Scholar]
- 5.Rudnicka AR, et al. Incidence of Late-Stage Age-Related Macular Degeneration in American Whites: Systematic Review and Meta-analysis. American journal of ophthalmology. 2015;160:85–93. e83. doi: 10.1016/j.ajo.2015.04.003. [DOI] [PubMed] [Google Scholar]
- 6.The Age-Related Eye Disease Study system for classifying age-related macular degeneration from stereoscopic color fundus photographs: the Age-Related Eye Disease Study Report Number 6. American journal of ophthalmology. 2001;132:668–681. doi: 10.1016/s0002-9394(01)01218-1. [DOI] [PubMed] [Google Scholar]
- 7.Davis MD, et al. The Age-Related Eye Disease Study severity scale for age-related macular degeneration: AREDS Report No. 17. Arch Ophthalmol. 2005;123:1484–1498. doi: 10.1001/archopht.123.11.1484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Klein R, et al. The five-year incidence and progression of age-related maculopathy: the Beaver Dam Eye Study. Ophthalmology. 1997;104:7–21. doi: 10.1016/s0161-6420(97)30368-6. [DOI] [PubMed] [Google Scholar]
- 9.Finger RP, et al. Reticular pseudodrusen: a risk factor for geographic atrophy in fellow eyes of individuals with unilateral choroidal neovascularization. Ophthalmology. 2014;121:1252–1256. doi: 10.1016/j.ophtha.2013.12.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Marsiglia M, et al. Association between geographic atrophy progression and reticular pseudodrusen in eyes with dry age-related macular degeneration. Invest Ophthalmol Vis Sci. 2013;54:7362–7369. doi: 10.1167/iovs.12-11073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Fleckenstein M, et al. The “diffuse-trickling” fundus autofluorescence phenotype in geographic atrophy. Invest Ophthalmol Vis Sci. 2014;55:2911–2920. doi: 10.1167/iovs.13-13409. [DOI] [PubMed] [Google Scholar]
- 12.Finger RP, et al. Reticular Pseudodrusen and Their Association with Age-Related Macular Degeneration: The Melbourne Collaborative Cohort Study. Ophthalmology. 2015 doi: 10.1016/j.ophtha.2015.10.029. [DOI] [PubMed] [Google Scholar]
- 13.Kovach JL, et al. The Relationship Between Reticular Pseudodrusen and Severity of AMD. Ophthalmology. 2015 doi: 10.1016/j.ophtha.2015.10.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sunness JS, et al. Enlargement of atrophy and visual acuity loss in the geographic atrophy form of age-related macular degeneration. Ophthalmology. 1999;106:1768–1779. doi: 10.1016/S0161-6420(99)90340-8. [DOI] [PubMed] [Google Scholar]
- 15.Sunness JS, et al. Visual function abnormalities and prognosis in eyes with age-related geographic atrophy of the macula and good visual acuity. Ophthalmology. 1997;104:1677–1691. doi: 10.1016/s0161-6420(97)30079-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Schatz H, McDonald HR. Atrophic macular degeneration. Rate of spread of geographic atrophy and visual loss. Ophthalmology. 1989;96:1541–1551. doi: 10.1016/s0161-6420(89)32694-7. [DOI] [PubMed] [Google Scholar]
- 17.Macular Photocoagulation Study Group. Risk factors for choroidal neovascularization in the second eye of patients with juxtafoveal or subfoveal choroidal neovascularization secondary to age-related macular degeneration. Arch Ophthalmol. 1997;115:741–747. doi: 10.1001/archopht.1997.01100150743009. [DOI] [PubMed] [Google Scholar]
- 18.Sunness JS, et al. The development of choroidal neovascularization in eyes with the geographic atrophy form of age-related macular degeneration. Ophthalmology. 1999;106:910–919. doi: 10.1016/S0161-6420(99)00509-6. [DOI] [PubMed] [Google Scholar]
- 19.Fritsche LG, et al. Seven new loci associated with age-related macular degeneration. Nat Genet. 2013;45:433–439. 439e431–432. doi: 10.1038/ng.2578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Fritsche LG, et al. Age-related macular degeneration: genetics and biology coming together. Annual review of genomics and human genetics. 2014;15:151–171. doi: 10.1146/annurev-genom-090413-025610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Black JR, Clark SJ. Age-related macular degeneration: genome-wide association studies to translation. Genetics in medicine : official journal of the American College of Medical Genetics. 2015 doi: 10.1038/gim.2015.70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kawa MP, et al. Complement system in pathogenesis of AMD: dual player in degeneration and protection of retinal tissue. Journal of immunology research. 2014;2014:483960. doi: 10.1155/2014/483960. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Khandhadia S, et al. Age-related macular degeneration and the complement system. Immunobiology. 2012;217:127–146. doi: 10.1016/j.imbio.2011.07.019. [DOI] [PubMed] [Google Scholar]
- 24.Telander DG. Inflammation and age-related macular degeneration (AMD) Seminars in ophthalmology. 2011;26:192–197. doi: 10.3109/08820538.2011.570849. [DOI] [PubMed] [Google Scholar]
- 25.Kleinman ME, Ambati J. Complement Activation and Inhibition in Retinal Diseases. Developments in ophthalmology. 2016;55:46–56. doi: 10.1159/000431141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Whitmore SS, et al. Complement activation and choriocapillaris loss in early AMD: implications for pathophysiology and therapy. Progress in retinal and eye research. 2015;45:1–29. doi: 10.1016/j.preteyeres.2014.11.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kuehn MH, et al. Disruption of the complement cascade delays retinal ganglion cell death following retinal ischemia-reperfusion. Exp Eye Res. 2008;87:89–95. doi: 10.1016/j.exer.2008.04.012. [DOI] [PubMed] [Google Scholar]
- 28.Johnson LV, et al. Complement activation and inflammatory processes in drusen formation and age related macular degeneration. Exp Eye Res. 2001;73:887–896. doi: 10.1006/exer.2001.1094. [DOI] [PubMed] [Google Scholar]
- 29.Yang P, et al. Retinal pigment epithelial cell death by the alternative complement cascade: role of membrane regulatory proteins, calcium, PKC, and oxidative stress. Invest Ophthalmol Vis Sci. 2014;55:3012–3021. doi: 10.1167/iovs.13-13554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Sunness JS, et al. Landmark-driven fundus perimetry using the scanning laser ophthalmoscope. Invest Ophthalmol Vis Sci. 1995;36:1863–1874. [PMC free article] [PubMed] [Google Scholar]
- 31.Sarks JP, Sarks SH, Killingsworth MC. Evolution of geographic atrophy of the retinal pigment epithelium. Eye (Lond) 1988;2(Pt 5):552–577. doi: 10.1038/eye.1988.106. [DOI] [PubMed] [Google Scholar]
- 32.Maguire P, Vine AK. Geographic atrophy of the retinal pigment epithelium. American journal of ophthalmology. 1986;102:621–625. doi: 10.1016/0002-9394(86)90535-0. [DOI] [PubMed] [Google Scholar]
- 33.Wu Z, et al. Low-luminance visual acuity and microperimetry in age-related macular degeneration. Ophthalmology. 2014;121:1612–1619. doi: 10.1016/j.ophtha.2014.02.005. [DOI] [PubMed] [Google Scholar]
- 34.Parisi V, et al. Macular function in eyes with early age-related macular degeneration with or without contralateral late age-related macular degeneration. Retina. 2007;27:879–890. doi: 10.1097/IAE.0b013e318042d6aa. [DOI] [PubMed] [Google Scholar]
- 35.Klein R, et al. The Wisconsin age-related maculopathy grading system. Ophthalmology. 1991;98:1128–1134. doi: 10.1016/s0161-6420(91)32186-9. [DOI] [PubMed] [Google Scholar]
- 36.Bird AC, et al. An international classification and grading system for age-related maculopathy and age-related macular degeneration. The International ARM Epidemiological Study Group. Surv Ophthalmol. 1995;39:367–374. doi: 10.1016/s0039-6257(05)80092-x. [DOI] [PubMed] [Google Scholar]
- 37.Brader HS, et al. New grading criteria allow for earlier detection of geographic atrophy in clinical trials. Invest Ophthalmol Vis Sci. 2011;52:9218–9225. doi: 10.1167/iovs.11-7493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Danis RP, et al. Methods and reproducibility of grading optimized digital color fundus photographs in the Age-Related Eye Disease Study 2 (AREDS2 Report Number 2) Invest Ophthalmol Vis Sci. 2013;54:4548–4554. doi: 10.1167/iovs.13-11804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Ferris FL, 3rd, et al. Clinical classification of age-related macular degeneration. Ophthalmology. 2013;120:844–851. doi: 10.1016/j.ophtha.2012.10.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Sunness JS, et al. Measuring geographic atrophy in advanced age-related macular degeneration. Invest Ophthalmol Vis Sci. 1999;40:1761–1769. [PubMed] [Google Scholar]
- 41.Sunness JS, et al. The long-term natural history of geographic atrophy from age-related macular degeneration: enlargement of atrophy and implications for interventional clinical trials. Ophthalmology. 2007;114:271–277. doi: 10.1016/j.ophtha.2006.09.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.The Age-Related Eye Disease Study Research Group. The Age-Related Eye Disease Study (AREDS): design implications. AREDS report no. 1. Control Clin Trials. 1999;20:573–600. doi: 10.1016/s0197-2456(99)00031-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Kankanahalli S, et al. Automated classification of severity of age-related macular degeneration from fundus photographs. Invest Ophthalmol Vis Sci. 2013;54:1789–1796. doi: 10.1167/iovs.12-10928. [DOI] [PubMed] [Google Scholar]
- 44.Niemeijer M, et al. Automated detection and differentiation of drusen, exudates, and cotton-wool spots in digital color fundus photographs for diabetic retinopathy diagnosis. Invest Ophthalmol Vis Sci. 2007;48:2260–2267. doi: 10.1167/iovs.06-0996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Rapantzikos K, Zervakis M, Balas K. Detection and segmentation of drusen deposits on human retina: potential in the diagnosis of age-related macular degeneration. Med Image Anal. 2003;7:95–108. doi: 10.1016/s1361-8415(02)00093-2. [DOI] [PubMed] [Google Scholar]
- 46.Smith RT, et al. A method of drusen measurement based on the geometry of fundus reflectance. Biomed Eng Online. 2003;2:10. doi: 10.1186/1475-925X-2-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Ramsey DJ, et al. Automated image alignment and segmentation to follow progression of geographic atrophy in age-related macular degeneration. Retina. 2014;34:1296–1307. doi: 10.1097/IAE.0000000000000069. [DOI] [PubMed] [Google Scholar]
- 48.Bearelly S, Cousins SW. Fundus autofluorescence imaging in age-related macular degeneration and geographic atrophy. Advances in experimental medicine and biology. 2010;664:395–402. doi: 10.1007/978-1-4419-1399-9_45. [DOI] [PubMed] [Google Scholar]
- 49.Khanifar AA, et al. Comparison of color fundus photographs and fundus autofluorescence images in measuring geographic atrophy area. Retina. 2012;32:1884–1891. doi: 10.1097/IAE.0b013e3182509778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Schmitz-Valckenberg S, et al. Fundus autofluorescence and progression of age-related macular degeneration. Surv Ophthalmol. 2009;54:96–117. doi: 10.1016/j.survophthal.2008.10.004. [DOI] [PubMed] [Google Scholar]
- 51.Hohn A, Grune T. Lipofuscin: formation, effects and role of macroautophagy. Redox Biol. 2013;1:140–144. doi: 10.1016/j.redox.2013.01.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Terman A, Brunk UT. Oxidative stress, accumulation of biological ‘garbage’, and aging. Antioxid Redox Signal. 2006;8:197–204. doi: 10.1089/ars.2006.8.197. [DOI] [PubMed] [Google Scholar]
- 53.von Ruckmann A, Fitzke FW, Bird AC. Fundus autofluorescence in age-related macular disease imaged with a laser scanning ophthalmoscope. Invest Ophthalmol Vis Sci. 1997;38:478–486. [PubMed] [Google Scholar]
- 54.Deckert A, et al. Automated analysis of digital fundus autofluorescence images of geographic atrophy in advanced age-related macular degeneration using confocal scanning laser ophthalmoscopy (cSLO) BMC ophthalmology. 2005;5:8. doi: 10.1186/1471-2415-5-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Holz FG, et al. Progression of geographic atrophy and impact of fundus autofluorescence patterns in age-related macular degeneration. American journal of ophthalmology. 2007;143:463–472. doi: 10.1016/j.ajo.2006.11.041. [DOI] [PubMed] [Google Scholar]
- 56.Wolf-Schnurrbusch UE, et al. Blue-light versus green-light autofluorescence: lesion size of areas of geographic atrophy. Invest Ophthalmol Vis Sci. 2011;52:9497–9502. doi: 10.1167/iovs.11-8346. [DOI] [PubMed] [Google Scholar]
- 57.Holz FG, et al. Fundus autofluorescence and development of geographic atrophy in age-related macular degeneration. Invest Ophthalmol Vis Sci. 2001;42:1051–1056. [PubMed] [Google Scholar]
- 58.Bearelly S, et al. Use of fundus autofluorescence images to predict geographic atrophy progression. Retina. 2011;31:81–86. doi: 10.1097/IAE.0b013e3181e0958b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Schmitz-Valckenberg S, et al. Correlation between the area of increased autofluorescence surrounding geographic atrophy and disease progression in patients with AMD. Invest Ophthalmol Vis Sci. 2006;47:2648–2654. doi: 10.1167/iovs.05-0892. [DOI] [PubMed] [Google Scholar]
- 60.Bindewald A, et al. Classification of fundus autofluorescence patterns in early age-related macular disease. Invest Ophthalmol Vis Sci. 2005;46:3309–3314. doi: 10.1167/iovs.04-0430. [DOI] [PubMed] [Google Scholar]
- 61.Schmitz-Valckenberg S, et al. Natural History of Geographic Atrophy Progression Secondary to Age-Related Macular Degeneration (Geographic Atrophy Progression Study) Ophthalmology. 2016;123:361–368. doi: 10.1016/j.ophtha.2015.09.036. [DOI] [PubMed] [Google Scholar]
- 62.Wong WT, et al. Treatment of geographic atrophy by the topical administration of OT-551: results of a phase II clinical trial. Investigative ophthalmology & visual science. 2010;51:6131–6139. doi: 10.1167/iovs.10-5637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Sunness JS, Ziegler MD, Applegate CA. Issues in quantifying atrophic macular disease using retinal autofluorescence. Retina. 2006;26:666–672. doi: 10.1097/01.iae.0000236472.56195.e9. [DOI] [PubMed] [Google Scholar]
- 64.Hunter JJ, et al. The susceptibility of the retina to photochemical damage from visible light. Progress in retinal and eye research. 2012;31:28–42. doi: 10.1016/j.preteyeres.2011.11.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Morgan JI, et al. Light-induced retinal changes observed with high-resolution autofluorescence imaging of the retinal pigment epithelium. Invest Ophthalmol Vis Sci. 2008;49:3715–3729. doi: 10.1167/iovs.07-1430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Morgan JI, et al. The reduction of retinal autofluorescence caused by light exposure. Invest Ophthalmol Vis Sci. 2009;50:6015–6022. doi: 10.1167/iovs.09-3643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Sull AC, et al. The evolution of spectral-domain optical coherence tomography. Retina Today. 2008 May-Jun;:39–44. [Google Scholar]
- 68.Bearelly S, et al. Spectral domain optical coherence tomography imaging of geographic atrophy margins. Ophthalmology. 2009;116:1762–1769. doi: 10.1016/j.ophtha.2009.04.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Schmitz-Valckenberg S, et al. Optical coherence tomography and autofluorescence findings in areas with geographic atrophy due to age-related macular degeneration. Invest Ophthalmol Vis Sci. 2011;52:1–6. doi: 10.1167/iovs.10-5619. [DOI] [PubMed] [Google Scholar]
- 70.Fleckenstein M, et al. Tracking progression with spectral-domain optical coherence tomography in geographic atrophy caused by age-related macular degeneration. Invest Ophthalmol Vis Sci. 2010;51:3846–3852. doi: 10.1167/iovs.09-4533. [DOI] [PubMed] [Google Scholar]
- 71.Querques G, et al. Wedge-shaped subretinal hyporeflectivity in geographic atrophy. Retina. 2015 Apr 25; doi: 10.1097/IAE.0000000000000553. Epub ahead of print. [DOI] [PubMed] [Google Scholar]
- 72.Mones J, Biarnes M, Trindade F. Hyporeflective wedge-shaped band in geographic atrophy secondary to age-related macular degeneration: an underreported finding. Ophthalmology. 2012;119:1412–1419. doi: 10.1016/j.ophtha.2012.01.026. [DOI] [PubMed] [Google Scholar]
- 73.Hu Z, et al. Segmentation of the geographic atrophy in spectral-domain optical coherence tomography and fundus autofluorescence images. Invest Ophthalmol Vis Sci. 2013;54:8375–8383. doi: 10.1167/iovs.13-12552. [DOI] [PubMed] [Google Scholar]
- 74.Chen Q, et al. A false color fusion strategy for drusen and geographic atrophy visualization in optical coherence tomography images. Retina. 2014;34:2346–2358. doi: 10.1097/IAE.0000000000000249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Nunes RP, et al. Predicting the progression of geographic atrophy in age-related macular degeneration with SD-OCT en face imaging of the outer retina. Ophthalmic Surg Lasers Imaging Retina. 2013;44:344–359. doi: 10.3928/23258160-20130715-06. [DOI] [PubMed] [Google Scholar]
- 76.Mokwa NF, et al. Grading of age-related macular degeneration: comparison between color fundus photography, fluorescein angiography, and spectral domain optical coherence tomography. J Ophthalmol. 2013;2013:385915. doi: 10.1155/2013/385915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Pece A, et al. Fluorescein angiography and indocyanine green angiography for identifying occult choroidal neovascularization in age-related macular degeneration. Eur J Ophthalmol. 2005;15:759–763. [PubMed] [Google Scholar]
- 78.Landa G, et al. The diagnostic contribution of indocyanine green to fluorescein angiography in fellow drusen eyes of patients with wet age-related macular degeneration. Eur J Ophthalmol. 2007;17:615–619. doi: 10.1177/112067210701700421. [DOI] [PubMed] [Google Scholar]
- 79.Holz FG, et al. Simultaneous confocal scanning laser fluorescein and indocyanine green angiography. American journal of ophthalmology. 1998;125:227–236. doi: 10.1016/s0002-9394(99)80095-6. [DOI] [PubMed] [Google Scholar]
- 80.Bottoni FG, Aandekerk AL, Deutman AF. Clinical application of digital indocyanine green videoangiography in senile macular degeneration. Graefe’s archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle. Ophthalmologie. 1994;232:458–468. doi: 10.1007/BF00195354. [DOI] [PubMed] [Google Scholar]
- 81.Roquet W, et al. Clinical features of drusenoid pigment epithelial detachment in age related macular degeneration. Br J Ophthalmol. 2004;88:638–642. doi: 10.1136/bjo.2003.017632. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Schneider U, et al. Detection of choroidal aneurysms with indocyanine green videoangiography. Graefe’s archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle. Ophthalmologie. 1998;236:193–195. doi: 10.1007/s004170050063. [DOI] [PubMed] [Google Scholar]
- 83.Schneider U, et al. Indocyanine green angiography and transmission defects. Acta Ophthalmol Scand. 1997;75:653–656. doi: 10.1111/j.1600-0420.1997.tb00624.x. [DOI] [PubMed] [Google Scholar]
- 84.Giani A, et al. The dark atrophy with indocyanine green angiography in Stargardt disease. Invest Ophthalmol Vis Sci. 2012;53:3999–4004. doi: 10.1167/iovs.11-9258. [DOI] [PubMed] [Google Scholar]
- 85.Sutter EE, Tran D. The field topography of ERG components in man--I. The photopic luminance response. Vision Res. 1992;32:433–446. doi: 10.1016/0042-6989(92)90235-b. [DOI] [PubMed] [Google Scholar]
- 86.Fish GE, Birch DG. The focal electroretinogram in the clinical assessment of macular disease. Ophthalmology. 1989;96:109–114. doi: 10.1016/s0161-6420(89)32944-7. [DOI] [PubMed] [Google Scholar]
- 87.Li J, Tso MO, Lam TT. Reduced amplitude and delayed latency in foveal response of multifocal electroretinogram in early age related macular degeneration. Br J Ophthalmol. 2001;85:287–290. doi: 10.1136/bjo.85.3.287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Wu Z, et al. Relationship between the second reflective band on optical coherence tomography and multifocal electroretinography in age-related macular degeneration. Invest Ophthalmol Vis Sci. 2013;54:2800–2806. doi: 10.1167/iovs.13-11613. [DOI] [PubMed] [Google Scholar]
- 89.Alten F, et al. Multifocal electroretinography in eyes with reticular pseudodrusen. Invest Ophthalmol Vis Sci. 2012;53:6263–6270. doi: 10.1167/iovs.12-10094. [DOI] [PubMed] [Google Scholar]
- 90.Alten F, et al. Longitudinal structure/function analysis in reticular pseudodrusen. Invest Ophthalmol Vis Sci. 2014;55:6073–6081. doi: 10.1167/iovs.13-13804. [DOI] [PubMed] [Google Scholar]
- 91.Wu Z, et al. Impact of reticular pseudodrusen on microperimetry and multifocal electroretinography in intermediate age-related macular degeneration. Invest Ophthalmol Vis Sci. 2015;56:2100–2106. doi: 10.1167/iovs.14-16210. [DOI] [PubMed] [Google Scholar]
- 92.Sunness JS, et al. Low luminance visual dysfunction as a predictor of subsequent visual acuity loss from geographic atrophy in age-related macular degeneration. Ophthalmology. 2008;115:1480–1488. 1488.e1481–1482. doi: 10.1016/j.ophtha.2008.03.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Pelli DG, Robson JG. The design of a new letter chart for measuring contrast sensitivity. Clin Vision Sci. 1988;2:187–199. [Google Scholar]
- 94.Leat SJ, Woo GC. The validity of current clinical tests of contrast sensitivity and their ability to predict reading speed in low vision. Eye (Lond) 1997;11(Pt 6):893–899. doi: 10.1038/eye.1997.228. [DOI] [PubMed] [Google Scholar]
- 95.Meleth AD, et al. Changes in retinal sensitivity in geographic atrophy progression as measured by microperimetry. Invest Ophthalmol Vis Sci. 2011;52:1119–1126. doi: 10.1167/iovs.10-6075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Curcio CA. Photoreceptor topography in ageing and age-related maculopathy. Eye (Lond) 2001;15:376–383. doi: 10.1038/eye.2001.140. [DOI] [PubMed] [Google Scholar]
- 97.Owsley C, et al. Psychophysical evidence for rod vulnerability in age-related macular degeneration. Invest Ophthalmol Vis Sci. 2000;41:267–273. [PubMed] [Google Scholar]
- 98.Forte R, Cennamo G, de Crecchio G. Microperimetry of subretinal drusenoid deposits. Ophthalmic research. 2014;51:32–36. doi: 10.1159/000354117. [DOI] [PubMed] [Google Scholar]
- 99.Querques G, et al. Impact of reticular pseudodrusen on macular function. Retina. 2014;34:321–329. doi: 10.1097/IAE.0b013e3182993df1. [DOI] [PubMed] [Google Scholar]
- 100.Schmitz-Valckenberg S, et al. Fundus autofluorescence and fundus perimetry in the junctional zone of geographic atrophy in patients with age-related macular degeneration. Invest Ophthalmol Vis Sci. 2004;45:4470–4476. doi: 10.1167/iovs.03-1311. [DOI] [PubMed] [Google Scholar]
- 101.Scholl HP, et al. Photopic and scotopic fine matrix mapping of retinal areas of increased fundus autofluorescence in patients with age-related maculopathy. Invest Ophthalmol Vis Sci. 2004;45:574–583. doi: 10.1167/iovs.03-0495. [DOI] [PubMed] [Google Scholar]
- 102.Legge GE, et al. Psychophysics of reading. VIII. The Minnesota Low-Vision Reading Test. Optometry and vision science : official publication of the American Academy of Optometry. 1989;66:843–853. doi: 10.1097/00006324-198912000-00008. [DOI] [PubMed] [Google Scholar]
- 103.Patel PJ, et al. Test-retest variability of reading performance metrics using MNREAD in patients with age-related macular degeneration. Invest Ophthalmol Vis Sci. 2011;52:3854–3859. doi: 10.1167/iovs.10-6601. [DOI] [PubMed] [Google Scholar]
- 104.Stifter E, et al. Reliability of a standardized reading chart system: variance component analysis, test-retest and inter-chart reliability. Graefe’s archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2004;242:31–39. doi: 10.1007/s00417-003-0776-8. [DOI] [PubMed] [Google Scholar]
- 105.Radner W, Diendorfer G. English sentence optotypes for measuring reading acuity and speed--the English version of the Radner Reading Charts. Graefe’s archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2014;252:1297–1303. doi: 10.1007/s00417-014-2646-y. [DOI] [PubMed] [Google Scholar]
- 106.Crossland MD, Culham LE, Rubin GS. Predicting reading fluency in patients with macular disease. Optometry and vision science : official publication of the American Academy of Optometry. 2005;82:11–17. [PubMed] [Google Scholar]
- 107.Hazel CA, et al. Visual function and subjective quality of life compared in subjects with acquired macular disease. Invest Ophthalmol Vis Sci. 2000;41:1309–1315. [PubMed] [Google Scholar]
- 108.Mangione CM, et al. Psychometric properties of the National Eye Institute Visual Function Questionnaire (NEI-VFQ). NEI-VFQ Field Test Investigators. Arch Ophthalmol. 1998;116:1496–1504. doi: 10.1001/archopht.116.11.1496. [DOI] [PubMed] [Google Scholar]
- 109.Mangione CM, et al. Development of the 25-item National Eye Institute Visual Function Questionnaire. Arch Ophthalmol. 2001;119:1050–1058. doi: 10.1001/archopht.119.7.1050. [DOI] [PubMed] [Google Scholar]
- 110.Riusala A, Sarna S, Immonen I. Visual Function Index (VF-14) in exudative age-related macular degeneration of long duration. American journal of ophthalmology. 2003;135:206–212. doi: 10.1016/s0002-9394(02)01832-9. [DOI] [PubMed] [Google Scholar]
- 111.Mangione CM, et al. Influence of age-related maculopathy on visual functioning and health-related quality of life. American journal of ophthalmology. 1999;128:45–53. doi: 10.1016/s0002-9394(99)00169-5. [DOI] [PubMed] [Google Scholar]
- 112.Tschosik E, et al. Quantifying functional reading independence in geographic atrophy: The FRI Index. Association for Research in Vision and Ophthalmology; Denver, CO: 2015. [Google Scholar]
- 113.Kapre A, et al. Sensitivity of Functional Reading Independence (FRI) Index to change in size of geographic atrophy. International Society for Pharmacoeconomics and Outcomes Research; Philadelphia, PA: 2015. [Google Scholar]
- 114.Ratnam K, et al. Relationship between foveal cone structure and clinical measures of visual function in patients with inherited retinal degenerations. Invest Ophthalmol Vis Sci. 2013;54:5836–5847. doi: 10.1167/iovs.13-12557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Piermarocchi S, et al. Quality of vision: a consensus building initiative for a new ophthalmologic concept. Eur J Ophthalmol. 2006;16:851–860. doi: 10.1177/112067210601600611. [DOI] [PubMed] [Google Scholar]
- 116.Ueda-Arakawa N, et al. Sensitivity and specificity of detecting reticular pseudodrusen in multimodal imaging in Japanese patients. Retina. 2013;33:490–497. doi: 10.1097/IAE.0b013e318276e0ae. [DOI] [PubMed] [Google Scholar]