

ABSTRACT
Background:
The ever-growing elderly population of Iran and their physical and mental consequences put emphasis on the necessity of determining the quality of life (QoL) in this social group. This systematic review and meta-analysis aimed to estimate the mean score of QoL in Iranian elderly citizens.
Methods:
Twenty-one articles that were indexed in Iranian (MagIran and Iran Medex) and international (Scientific Information Database, Google Scholars, Science Direct, PubMed, ProQuest, Scopus) databases were selected. The articles have used the Short Form Health Survey (SF-36) to measure QoL in Iranian elderly. The collected data were analyzed using a random effects model, while heterogeneity of the studies was measured by I2 index. The data analysis was performed by STATA.
Results:
The sample size of the 21 articles was 5318 and the mean score of QoL in the healthy and sick elderly citizens was 53.8 (CI 95%: 49.4-58.2) and 50.6 (CI 95%: 38.4-62.9) respectively. In addition, there was no significant relationship between the score of QoL and the year of publication of the articles. (P=0.748)
Conclusion:
Given that QoL of the studied elderly was almost at an average level, there is a need to codify and implement comprehensive programs through effective training programs toward improving QoL of the elderly.
KEYWORDS: Aging, Elderly, Iran, Quality of life
INTRODUCTION
Aging is a gradual change process, a personal and social experiment and a unique perception of life, which is joyful for some people and for others, it is the start score of the sad and bleak stage of life.1 According to the report of World Health Organization (WHO), aging starts at 65 in the developed countries and 60 in developing countries.2 The latest general census in Iran showed that 7.27% of 75 million population of Iran are older than 60.3 Population projections showed that this rate would reach 10% over 25 years and 25% in 2050.4,5 This demographic change process is so serious that the present century is declared by WHO as the century of the elderly.6 Aging increases the probability of developing mental and physical chronic diseases significantly7,8 so that 80% of the elderly citizens are afflicted with at least one chronic disease and 40% of them suffer from the limitations caused by their chronic diseases.9 Although medical advances have increased life expectancy and the number of elderly citizens, quality of life (QoL) is an important subject for most researchers, rather than length of life.10,11
There are different definitions of Qol; according to the definition of WHO, QoL is one’s perception of his/her standing point in life within the cultural texture and value system of the society regarding purposes, expectations, standards and personal interests.12 In addition, QoL is defined as the extent of physical, psychological and social welfare as perceived by individuals that also indicate one’s satisfaction with life.13 Researches have argued that the QoL is one’s attitude toward the perceived differences between what should be and what actually is.10,14 Despite this variety of definitions, QoL is a dynamic, relative, and more general concept of health, which is described and evaluated by the individual as a function of one’s attitude toward life.15
Nobody questions the merits of increase of life expectancy; however, families and the society incur considerable health and medical costs when the elderly population in the society increases.16 This may in turn result in the decrease of QoL of the elderly.17 Given the importance of QoL, some authors and researchers have argued that health services of the new century must target the improvement of QoL and health. To this end, the first step is to have a wider picture of the QoL of the elderly. Several studies have been carried out in Iran on QoL of the elderly, generating different estimates of QoL.9,10 The purpose of the present study was to achieve a general estimate of QoL in Iranian elderly and survey the general trend of changes in this area.
MATERIALS AND METHODS
The present study was a systematic review and meta-analysis to estimate the score of QoL in Iranian elderly based on the articles indexed in Iranian (MagIran, IranMedex) and international databases (SID, Google Scholar, Science Direct, PubMed, ProQuest, and Scopus). The articles were searched with no time limit based on the keywords “elderly” “quality of life”, “aging” and “Iran” and Farsi equivalent of these terms and also combinations of these terms. Search terms included ((Elderly) OR Aging) AND (quality of life) AND (Iran). To extend the scope of the search, references of the articles found were also reviewed.
Data Extraction
At first, all of the articles on QoL in the Iranian elderly were checked based on the inclusion and exclusion criteria. Exclusion criteria were “irrelevant subject” “ the use of assessment tools other than SF-36”, “repetitive works”, and “unavailability of full-text.” Abstracts of the articles were examined based on the inclusion and exclusion criteria and full text of relevant works were collected. Data extraction form was used in order to collect the data, including the first author’s name, year of publication, place of the study, sample size, and QoL score. Each study was reviewed by two independent researchers and any case of disagreement was sorted by the corresponding author (experienced in meta-analysis study). Primarily, 100 articles were found and 65 were excluded because of these reasons: irrelevancy, not an original study, pilot study, no separate data of QoL, and no separate score of QoL in elderly. The articles indexed in several databases were considered as one. Out of the remaining 35 articles, 14 were removed because the data of some of them had been replicated and also questionnaires other than SF-36 had been used in some of them, so 21 articles entered the final analysis stage.
Statistical Analysis
Given that the score of QoL has a normal distribution, the variance of each article was calculated through normal distribution variance . The weight of each article was relative to its inverse variance. In order to check heterogeneity of the data, Q test and I2 index were used. Heterogeneity index of less than 25% was interpreted as low heterogeneity, 25%-75% as average heterogeneity, and above 75% as high heterogeneity. With I2 equal to 99.8% in this study (high heterogeneity) (P=0.0001, Q=1715), a random effects model was used. To survey the relationship between the score of QoL, year of publication, and sample size, meta-regression analysis was used. In addition, “subgroup analysis” was used to examine the score of QoL based on the target study groups (healthy and patients) and geographical locations. Biased publication was evaluated based on Begg’s Funnel Plot (figure 1), which indicated no bias. Data analyses were performed by SATATA 12.1 (statacorp LP, College Station, TX, USA).
Figure1.
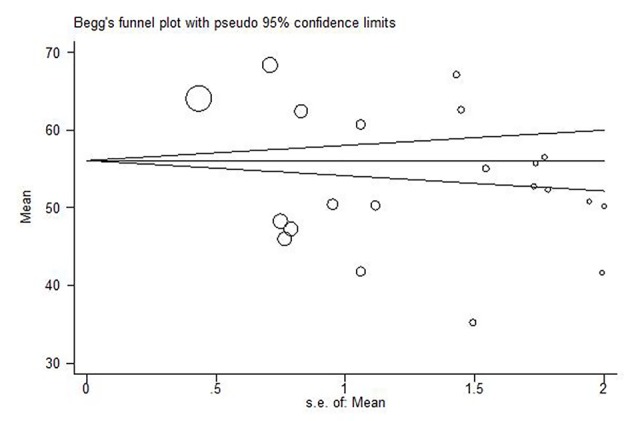
Beggs Funnel Plot with pseudo 95% confidence limits.
Beggs Funnel Plot showed no publishing error (P=0.398). Distribution points of the symmetry axis on the left and right of the graph is the same; it means that the point estimate distribution of several studies around the graph is symmetric.
RESULTS
The primary search yielded 100 articles, out of which 21 articles used in the final analysis stage. Screening process was performed according to PRISMA flow diagram (figure 2). 18
Figure2.

The process of surveying, screening, and selecting the articles for systematic review and meta-analysis mean score of QoL.
Articles used in the final analysis stage had been published between 2004 and 2015 and represented 5318 participants (254 per study). The smallest sample group was in Ghaderi et al.19 with 87 participants and the largest sample group was in Aqamolaei et al.8 with 1000 participants. The highest score of QoL (68.3) was reported by Aqamolaei et al.8 and the lowest score (35.1) was reported by Adib-Hajbaqeri and Abbasinia.14 More details about articles are presented in Table 1.
Table 1.
Specifications of the systematic review and meta-analysis articles about the prevalence of Qol
| Row | First author | Year | Place | Community | Sample size | The mean of QOL | Confidence Interval 95% | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| 1 | Emami Moghaddam et al.9 | 2015 | Mashhad | Blood Pressure | 60 | 50.1 | 46.2 | 54 |
| 2 | Hedayati et al.20 | 2014 | Shiraz | Healthy | 220 | 50.7 | 46.8 | 54.5 |
| 3 | Naseh et al.21 | 2014 | Chahar Mahal | Healthy | 87 | 41.6 | 37.6 | 45.4 |
| 4 | Ghaderi & Mostafaee19 | 2014 | Tabriz | Healthy | 56 | 52.3 | 48.7 | 55.7 |
| 5 | Heravi-Karimooi et al.22 | 2013 | Tehran | Healthy | 180 | 52.6 | 49.2 | 56 |
| 6 | Hekmatpoue et al.10 | 2013 | Arak | Healthy | 271 | 50.2 | 48 | 52.4 |
| 7 | Darvishpoor Kakhki et al.23 | 2013 | Tehran | Healthy | 400 | 48.2 | 46.7 | 49.6 |
| 8 | Aghanuri et al.16 | 2013 | Arak | Healthy | 165 | 55.7 | 52.2 | 59 |
| 9 | Hajihashemi et al.24 | 2013 | Shahryar | Sick | 203 | 54.9 | 51.9 | 57.9 |
| 10 | Mohammadiannia et al.25 | 2013 | Booshehr | Healthy | 173 | 56.4 | 52.9 | 59.8 |
| 11 | SalariLak et al.26 | 2013 | Kamyaran | Healthy | 400 | 60.6 | 58.5 | 62.7 |
| 12 | Abdoli et al.27 | 2012 | Tehran | Healthy | 80 | 67.1 | 64.2 | 69.8 |
| 13 | Abdoli et al.27 | 2012 | Tehran | Osteoporosis | 80 | 62.6 | 64.2 | 69.8 |
| 14 | Salehi et al.28 | 2012 | Tehran | Healthy | 400 | 63.9 | 63.1 | 64.8 |
| 15 | Garousi et al.29 | 2012 | Kerman | Healthy | 383 | 45.9 | 44.4 | 47.4 |
| 16 | Zahmatkeshan et al.30 | 2012 | Booshehr | Healthy | 360 | 47.2 | 45.6 | 48.7 |
| 17 | Jadidi et al.11 | 2011 | Tehran | Healthy | 141 | 50.4 | 48.4 | 52.2 |
| 18 | Adib-Hajbaghery & Abasinia14 | 2010 | Kashan & Qom | Fracture of femur | 70 | 35.1 | 32.2 | 38 |
| 19 | Aghamolaeie et al.8 | 2010 | Bandar-Abbas | Healthy | 1000 | 68.3 | 66.9 | 69.6 |
| 20 | Nejati & Ashayeri31 | 2008 | Kashan | Healthy | 389 | 62.3 | 60.7 | 63.9 |
| 21 | Ahmadi et al.32 | 2004 | Zahedan | Healthy | 200 | 41.7 | 39.6 | 43.7 |
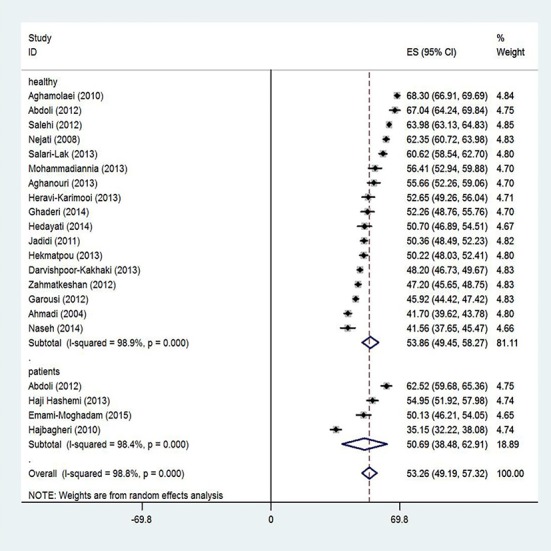
Scores of QoL were analyzed based on random effects model so that for 5318 elderly participants in all the studies, the score of QoL was 53.2 (CI 95%: 49.1-57.3). The model assumes that the differences between the reported results are rooted in differences in sampling process and the obtained scores of the participants. The articles were categorized based on the place of the study and the type of the disease (figure 3).
Figure3.
The mean score of QoL based on the study population; CI of 95% of each article is represented as horizontal lines near the main mean line; dashed line at the mid represents an estimate of the total mean score; and the rhomboid represents CI of the mean score of QoL.
The mean scores of QoL of the healthy and sick elderly based on SF-36 were 53.8 (CI 95%: 49.4-58.2) and 50.6 (CI 95%: 38.4-62.9), respectively. In other words, the healthy elderly enjoyed a higher QoL (Z=23.93 vs. Z=8.13, P<0.001) (figure 4).
Figure4.
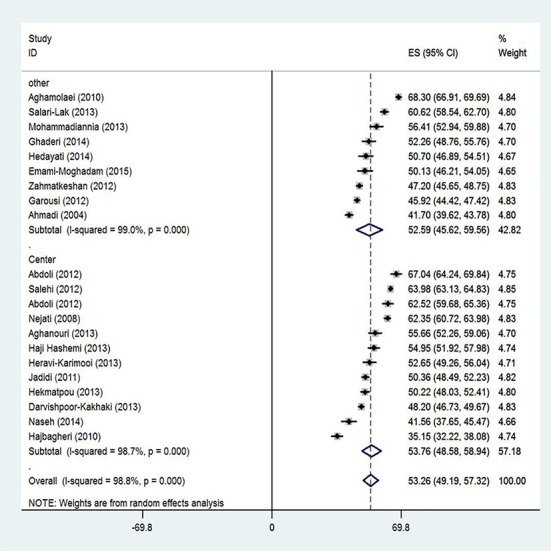
The mean score of QoL based on the place of the study; CI of 95% of each article is represented as horizontal lines near the main mean line; dashed line at the mid represents an estimate of the total mean score; and the rhomboid represents CI of the mean score of QoL.
The mean score of QoL in the elderly was reported to be 53.7 (CI 95%: 48.5-58.9) by the studies conducted in the central regions of the country and 52.5 (CI 95%: 45.6-59.5) by the studies conducted in other regions of the country (Z=20.35 vs. Z=14.79, P<0.001).
Meta-regression analysis (figure 5) indicated that there was no significant relationship between the mean scores of QoL and the year of publication of the articles (P=0.748). It means that the QoL in the elderly has not improved over time. It seems that the factor of year has not been the reason of heterogeneity.
Figure5.
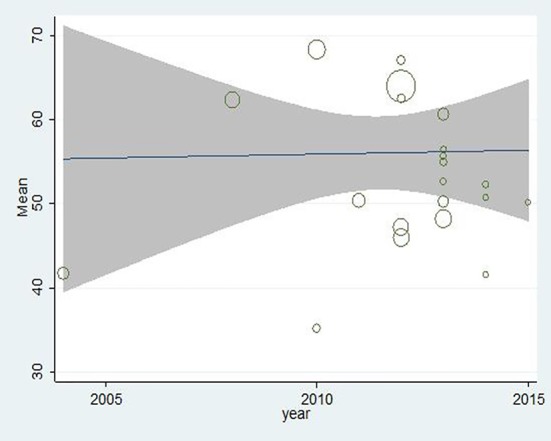
Meta-regression diagram of the mean of QOL in the elderly based on the year of publication.
DISCUSSION
As the results showed, the mean score of QoL in Iranian elderly was 53.2 (CI 95%: 49.1-57.3). Aqanouri believed that because of the absence of norms and standards for QoL in Iranian society, the mean score of QoL of 50 with a standard deviation of 10 is an acceptable mean level of QoL in the elderly.16
Thereby, one might say that Iranian elderly populations have a relatively average QoL. In addition, QoL is a function of one’s perception of his/her life condition based on his/her culture, goals, expectations, standards, priorities and also the value system that he/she live in. Thus, QoL is a personal matter based on an individual’s perception of different aspects of his/her life and not for being measured based on external scales.33
Results of a systematic review and meta-analysis by Cheraghi et al.34 about the QoL among Iranian elderly showed that the elderly gained more than half of the total score of QoL which is consistent with the results of the present study. The difference between the study of Cheraghi and the present study is in the tools used for evaluation of QoL in the elderly; Cheraghi used WHOQOL for evaluating QoL.
Our results showed that the mean score of QoL in healthy Iranian elderly was higher than the sick ones. A cohort study in the UK showed that the mean score of QoL in the healthy elderly in Aberdeen city was 76.1±18.05 and that of two sample groups of the healthy elderly in Herefordshire city was 71.9±18.57 and 75.55±17.6.35 Another study36 reported a mean score of QoL in the elderly domiciled in Rio de Janeiro to be 75.4 and an Australian research37 reported this figure for the healthy elderly equal to 74±25.7. These results indicated that the elderly population in the Western countries enjoys a higher QoL. In two studies conducted in New York38 and France,39 higher mean scores of QoL were reported for the American and French elderly, respectively, than what we have found as the score in QoL of the Iranian elderly. Taking into account that developed countries have a prolonged experience in dealing with the aging population problem, they expectedly have better programs to improve the QoL in the elderly population. Moreover, lower annual income per capita in Iran in comparison to other developed countries and lack of general social, medical and welfare support for the elderly in Iran might explain the lower QoL among Iranian elderly. Researches showed that economic, cultural, and emotional problems, low standards, and unhealthy lifestyle over the last few decades were some of the effective factors on early senescence (at least 15 years earlier than calendar age) among Iranian elderly.2,40 The phenomenon of early senescence leads the individual to a critical stage of life without preparation.40 In a cross-sectional study that was conducted to measure QoL in the healthy Lebanese elderly population, the mean score of QoL was reported to be 52.05, which is similar to that of the Iranian healthy elderly.41 In another cross-sectional study in Turkey,42 the results showed that QoL in the healthy elderly population was 74.55±35.16, which is inconsistent with our results. The inconsistent results could be explained by the differences between the societies and the role and position of the elderly citizens in their family in two countries. Different societies have different behaviors toward the elderly citizens. In some cultures, the elderly lose their roles in the society and the society stops treating them as reliable and responsive individuals. Becoming an elderly citizen in such societies means losing professional roles and responsibilities. Clearly, losing social roles tackles the QoL. Other societies have predicted social works and participation in Non-Governmental Organizations (NGO) to keep the elderly population active and enable them to share their knowledge and experience with other social groups. Through such programs, great losses of human resources in the society are prevented and the elderly are given a chance to improve their social relationship and life.
Our results showed that the mean score of QoL in sick elderly population (50.6) was less than that of the healthy population (53.8). Similar to the result of the present study, the findings of the previous review and meta-analysis studies on the QoL among sick elderly have shown that this group had a lower QoL compared to healthy elderlies.43-45
Also, in a cross-sectional study the QoL in individuals with fibromyalgia and rheumatoid arthritis was significantly less than that of healthy individuals.46 Consistent with our study, Canbaz42 reported that the elderly with chronic diseases in Turkey experienced lower QoL compared to the healthy elderly (P<0.001). Apparently, there is a mutual relationship between having a disease and QoL as physical disorders, and development of physical symptoms has direct effects on all aspects of QoL. The relationship between QoL and diseases is so strong that QoL is always considered as a key index in assessing the patients’ conditions. Moreover, the effectiveness of many health and medical interventions is measured based on QoL.47
The mean score of QoL in the elderly in central regions of the country was 53.7 and in other regions it was 52.5. Apparently, QoL of the elderly doesn’t depend on the area they are living in, but it’s affected by other factors such as culture and access to health services. The undeniable role of common culture (respect for elders), despite ethnical diversity in Iran, growth and development of urbanism, and improvement of quality and quantity of medical health services nationwide are some of the factors that would make the score of QoL to vary in different regions of the country to remain in a thin interval.
Results of meta-regression analysis indicated no change in QoL score over the years. Although technological and scientific advances and achievements of the recent century are not deniable, the effect of these developments on QoL of the elderly has not been notable. In fact, the changes in the importance of land as production tools and rapid social changes have degraded social standing and power of the elderly. Not only the knowledge accumulated in the elderly is no longer considered valuable, but it rather is considered outdated and useless. Consequently, the elderly lose their connections with the society. Garousi believed that any attempt to provide support for the elderly and increase their social relationship may lead to an increase in the QoL in the elderly and life expectancy. 29 According to WHO, while the elderly’s needs for health services are more than any other age group, the services they receive are less than what is provided for other age groups. The majority of health services and interventions provided for the elderly citizens are provided after development of diseases or other health issues and little has been done in the area of prevention. These explain why many personalities and mental aspects of the elderly have remained unknown and many physical and mental problems have remained unsolved despite all technological and medical advances and even the emergence of new fields of expertise such as gerontology. 48 In addition, changes of social structures from wide structure to the core one and the increasing number of women working outside the house have decreased the families’ capacity for supporting and looking after the elderly. Also, the task that was once carried out by the families is the responsibility of societies and the states now.
Reviewing previous systematic review studies revealed that they mostly focused on the tools of QoL evaluation,49,50 conceptualization of QoL in the elderly,51 the relationship between diseases and QoL in the elderly,43,52 and effective physical exercises on QoL,53 none of them has mentioned the score or condition of QoL in the elderly. They mostly evaluated QoL in relation with other variables, so considering their irrelevance with the present study, the results could not be compared with each other.
The strength of this study was that no meta-analysis study about QoL in the elderly has been done before. Our study had some limitations. We could not enroll all of the studies about QoL and we had to exclude some of them because they have used other tools to assess QoL. The other limitation of our study was the variation of diseases and their different effects on QoL, so we could not evaluate different diseases and their effects on QoL separately.
CONCLUSION
The results confirmed that the Iranian elderly population have an average QoL, which is less than that of the developed countries. Therefore, there is a need to codify and implement comprehensive programs and trainings toward improvement and preservation of QoL of the elderly.
ACKNOWLEDGEMENT
We thank all authors of the articles that were used to write this manuscript.
Conflict of Interest:None declared.
REFRENSES
- 1.Bazrafshan MR, Hosseini MA, Rahgozar M, Maddah BS. Quality of women elderly’s life in Shiraz, Jahandidegan club. Salmand. 2008;3:33–41. [In Persian] [Google Scholar]
- 2.Sadeghiyan F, Raei M, Hashemi M, et al. Elderly and health problems: a cross sectional study in the Shahroud township. Iranian Journal of Ageing. 2011;6:26–30. [In Persian] [Google Scholar]
- 3.Sheibani Tazraji F, Pakdaman S, Dadkhah A, Hasanzadeh Tavakoli MR. The effect of music therapy on depression and loneliness in old people. Iranian Journal of Ageing. 2010;5:54–60. [In Persian] [Google Scholar]
- 4.de Silva SA, Scazufca M, Menezes PR. Population impact of depression on functional disability in elderly: results from ‘‘Sao Paulo Ageing & Health Study’’ (SPAH) Eur Arch Psychiatry Clin Neurosci. 2013;263:153–8. doi: 10.1007/s00406-012-0345-4. [DOI] [PubMed] [Google Scholar]
- 5.Bhamani MA, Karim MS, Khan MM. Depression in the elderly in Karachi, Pakistan: a cross sectional study. BMC Psychiatry. 2013;13:181–8. doi: 10.1186/1471-244X-13-181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bahram ME, Pourvaghar MJ, Sadeh MR. Effect of 12 weeks of Chosen Pilates Exercise on the Quality of Iife of Healthy Nonathletic People. Toloo-e-Behdasht. 2014;13:93–103. [In Persian] [Google Scholar]
- 7.Sohrabi MB, Zolfaghari P, Mahdizade F, et al. Evaluation and comparison of cognitive state and depression in elderly admitted in sanitarium with elderly sited in personal home. Knowledge and Health. 2008;3:27–31. [In Persian] [Google Scholar]
- 8.Aghamolaei T, Avafian SS, Zare S. Health related quality of life in elderly people living in Bandar Abbas, Iran: a population- based study. Acta Medica Iranica. 2010;48:185–91. [PubMed] [Google Scholar]
- 9.Emami Moghaddam Z, Khoshraftar Roudi E, Ildarabadi E, Behnam Voshani HR. Quality of life in hypertension elderly patients that referred to health centers in Mashhad. Quarterly Journal of Sabzevar University of Medical Sciences. 2015;22: 444–52. [In Persian] [Google Scholar]
- 10.Hekmatpou D, Jahani F, Behzadi F. Study the quality of life among elderly women in Arak in 2013. Arak Medical University Journal. 2014;17:1–8. [In Persian] [Google Scholar]
- 11.Jadidi A, Farahaninia M, Janmohammadi S, Haghani H. The relationship between spiritual well-being and quality of life among elderly people residing. Holist Nurs Pract. 2015;29:128–35. doi: 10.1097/HNP.0000000000000081. [DOI] [PubMed] [Google Scholar]
- 12.Abnavi F, Rezaei F. The effect of age-related voice changes on the quality of life of the elderly and middle-aged people. J Res Rehabil Sci. 2014;10:549–58. [In Persian] [Google Scholar]
- 13.Panaghi L, Abarashi Z, Mansoori N, Dehghani M. Quality of Life and Related demographic factor of the elderly in Tehran. Salmand. 2010;4:77–87. [In Persian] [Google Scholar]
- 14.Adib-Hajbaghery M, Abasinia M. Assessing Quality of life of elders with femoral neck fractures, using SF36 and EQ5D. Iranian Journal of Nursing Research. 2010;4:71–9. [In Persian] [Google Scholar]
- 15.Mojiri F, Rezaei F, Zibaee F, Mohammadi M. Investigating the relationship between the VHI scores and the acoustic parameters in patients suffering from voice disorder. Journal of research in rehabilitation sciences. 2012;8:1204–12. [Google Scholar]
- 16.Aghanuri A, Mahmoudi M, Asadi M, et al. Quality of life and its relationship with quality of diet among elderly people in urban areas of Markazi province, Iran. Arak Medical University Journal. 2013;15:1–11. [Google Scholar]
- 17.Arastoo A, Ghassemzadeh R, Nasseh H, et al. Factors affecting quality of life in elderly diabetic residents of the Kahrizak geriatric nursing home of Tehran. Iranian Journal of Endocrinology and Metabolism. 2012;14:18–24. [Google Scholar]
- 18.Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535. doi: 10.1136/bmj.b2535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ghaderi D, Mostafaee A. A study on the relationship between religious orientation and quality of life among elderly men living in nursing homes and those living with their families in Tabriz. Salmand. 2014;9:14–21. [In Persian] [Google Scholar]
- 20.Hedayati HR, Hadi N, Mostafavi L, et al. Quality of life among nursing home residents compared with the elderly at home. Shiraz E-Med J. 2014;15:e22718. [Google Scholar]
- 21.Naseh L, Shaikhy RA, Rafii F. Quality of life and its related factors among elders living in nursing homes. Iran Journal of Nursing. 2014;27:67–78. [In Persian] [Google Scholar]
- 22.Heravi-Karimooi M, Rejeh N, Montazeri A. Health-related quality of life among abused and non-abused elderly people: a comparative study. Payesh. 2013;12:479–88. [In Persian] [Google Scholar]
- 23.Darvishpoor Kakhki, A Abed, Saeedi J. Factors related to health- related quality of life (HRQoL) of elderly people in Tehran. J Nurs Midwifery. 2013;23:8–16. [In Persian] [Google Scholar]
- 24.Hajihashemi Z, Vameghi R, Montazeri A, et al. Comparing quality of life among rural and urban elderly outpatients. Payesh. 2013;12:255–62. [Google Scholar]
- 25.Mohammadiannia M, Foroughan M, Rassafiani M, Hosseinzadeh S. Visual functioning and its relations with quality of life in the older people using governmental outpatient clinics services in the City of Boushehr. Salmand. 2013;7:16–26. [In Persian] [Google Scholar]
- 26.SalariLak S, Gorgin Karaji L, Amiri S. Quality of life in elderly population in Kamyaran district, 2009. Urmia Medical Jornal. 2013;24:24–9. [In Persian] [Google Scholar]
- 27.Abdoli B, Modaberi S, Shamsipour P. Comparison of the quality of life for healthy active and sedentary elderly and patients with osteoarthritis. Annals of Biological Research. 2012;3:2343–8. [Google Scholar]
- 28.Salehi L, Salaki S, Alizadeh L. Health-related quality of life among elderly member of elderly centers in Tehran. Iranian Journal of Epidemiology. 2012;8:14–20. [In Persian] [Google Scholar]
- 29.Garousi S, Safizadeh H, Samadian F. The study of relationship between social support and quality of life among elderly people in Kerman. Jundishapur Sci Med J. 2012;11:303–15. [In Persian] [Google Scholar]
- 30.Zahmatkeshan N, Bagherzadeh R, Akaberiyan Sh, et al. Assessing quality of life and related factors in Bushehrs elderly people. Journal of Fasa University of Medical Sciences. 2012;2:253–8. [Google Scholar]
- 31.Nejati V, Ashayeri H. Health related quality of life in the elderly in Kashan. Iranian Journal of Psychiatry and Clinical Psychology. 2008;14:56–61. [In Persian] [Google Scholar]
- 32.Ahmadi F, Salar A, Faghihzadeh S. Quality of life in Zahedan elderly population. Hayat. 2004;10:61–7. [In Persian] [Google Scholar]
- 33.Hasani F, Kamali M, Akbar Fahimi M, Davatgaran K. Factors affecting quality of life of the elderly in the residential homes of Tehran (2009) Journal of Birjand University of Medical Sciences. 2011;18:320–8. [In Persian] [Google Scholar]
- 34.Cheraghi Z, Doosti-Irani A, Nedjat S, et al. Quality of life in elderly Iranian population using the QoL brief questionnaire: a systematic review. Iran J Public Health. 2016;45:978–85. [PMC free article] [PubMed] [Google Scholar]
- 35.Mishra GD, Gale CR, Sayer AA, et al. How useful are the SF-36 sub-scales in older people? Mokken scaling of data from the HALCyon programme. Quality of life Research. 2011;20:1005–10. doi: 10.1007/s11136-010-9838-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Lima MG, Barros MB, César CL, et al. Health related quality of life among the elderly: a population-based study using SF-36 survey. Cadernos de Saude Publica. 2009;25:2159–67. doi: 10.1590/s0102-311x2009001000007. [DOI] [PubMed] [Google Scholar]
- 37.Bartsch LJ, Butterworth P, Byles JE, et al. Examining the SF-36 in an older population: analysis of data and presentation of Australian adult reference scores from the Dynamic Analyses to Optimise Ageing (DYNOPTA) project. Quality of Life Research. 2011;20:1227–36. doi: 10.1007/s11136-011-9864-0. [DOI] [PubMed] [Google Scholar]
- 38.Dickson VV, Howe A, Deal J, McCarthy MM. The relationship of work, self-care and quality of life in a sample of older working adults with cardiovascular disease. Heart & Lung. 2011;41:5–14. doi: 10.1016/j.hrtlng.2011.09.012. [DOI] [PubMed] [Google Scholar]
- 39.Capuron L, Moranis A, Combe N, et al. Vitamin E status and quality of life in the elderly: influence of inflammatory processes. British Journal of Nutrition. 2009;102:1390–4. doi: 10.1017/S0007114509990493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Rostami M, Baraz Pordanjani Sh, Farzianpour F, Rasekh A. Effect of Orem Self-care model on elderly s quality of life in health care centers of Masjed Soleiman in 2007-2008. Journal of Arak University of Medical Sciences. 2009;12:51–9. [In Persian] [Google Scholar]
- 41.Sabbah I, Drouby N, Sabbah S, et al. Quality of life in rural and urban populations in Lebanon using SF-36 health survey. Health and quality of life Outcomes. 2003;1:30. doi: 10.1186/1477-7525-1-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Canbaz S, Sunter AT, Dabak S, Peksen Y. The prevalence of chronic diseases and quality of life in elderly people in Samsun. Turkish Journal of Medical Sciences. 2003;33:335–40. [Google Scholar]
- 43.Gerritsen AE, Allen PF, Witter DJ, et al. Tooth loss and oral health-related quality of life: a systematic review and meta-analysis. Health and quality of life outcomes. 2010;8:126. doi: 10.1186/1477-7525-8-126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Chou CH, Hwang CL, Wu YT. Effect of exercise on physical function, daily living activities, and quality of life in the frail older adults: a meta-analysis. Arch Phys Med Rehabil. 2012;93:237–44. doi: 10.1016/j.apmr.2011.08.042. [DOI] [PubMed] [Google Scholar]
- 45.Mol M, Carpay M, Ramakers I, et al. The effect of perceived forgetfulness on quality of life in older adults; a qualitative review. International Journal of Geriatric Psychiatry. 2007;22:393–400. doi: 10.1002/gps.1686. [DOI] [PubMed] [Google Scholar]
- 46.Salaffi F, Sarzi-Puttini P, Girolimetti R, et al. Health-related quality of life in fibromyalgia patients: a comparison with rheumatoid arthritis patients and the general population using the SF-36 health survey. Clinical & Experimental Rheumatology. 2009;27:S67–74. [PubMed] [Google Scholar]
- 47.Askarpour H, Mohammadi I, Meamariyan R. The effect of self- care management on quality of life of hemophilic adolescents. Daneshvar. 2007;14:1–8. [In Persian] [Google Scholar]
- 48.Ghahremani L, Nazari M, Mosavi MT. Improvement of quality of life in elderly men in Kahrizak nursing home based on educational intervention. Knowledge & Health. 2009;4:18–23. [Google Scholar]
- 49.Hickey A, Barker M, McGee H, O’Boyle C. Measuring health-related quality of life in older patients populations: a review of current approaches. PharmacoEconomics. 2005;23:971–93. doi: 10.2165/00019053-200523100-00002. [DOI] [PubMed] [Google Scholar]
- 50.Haywood KL, Garratt AM, Fitzpatrick R. Older people specific health status and quality of life: a structured review of self-assessed instruments. Journal of Evaluation in Clinical Practice. 2005;11:315–27. doi: 10.1111/j.1365-2753.2005.00538.x. [DOI] [PubMed] [Google Scholar]
- 51.Halvorsrud L, Kalfoss M. The conceptualization and measurement of quality of life in older adults: a review of empirical studies published during 1994–2006. European Journal of Ageing. 2007;4:229–46. doi: 10.1007/s10433-007-0063-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Marengoni A, Angleman S, Melis R, et al. Aging with multimorbidity: a systematic review of the literature. Ageing Research Reviews. 2011;10:430–9. doi: 10.1016/j.arr.2011.03.003. [DOI] [PubMed] [Google Scholar]
- 53.de Vries NM, va Ravensberg CD, Hobbelen JS, et al. Effects of physical exercise therapy on mobility, physical functioning, physical activity and quality of life in community-dwelling older adults with impaired mobility, physical disability and/or multi-morbidity: a meta-analysis. Ageing Research Reviews. 2012;11:136–49. doi: 10.1016/j.arr.2011.11.002. [DOI] [PubMed] [Google Scholar]