

Abstract
Background:
This report describes the findings of the survey conducted by South African Depression and Anxiety Group (SADAG) in a cohort of disadvantaged South African adolescent scholars in which PHQ-9 teen version was modified and adapted (PHQ-9M) to improve the response rate.
Method:
PHQ-9M was administered to 2025 secondary students of 35 schools over 2 years in Gauteng Province, South Africa.
Results:
The mean age was 15.8 years. 23% of respondents scored 9 or above, 26.7% reported suicidal ideations in last month, 21.8% reported lifetime suicide attempts and 9.3% had severe functional impairment. PHQ-9M showed a fair internal consistency and face validity in this study.
Conclusion:
The PHQ-9M could be useful in conducting surveys in settings of low mental health literacy after further evaluation of its psychometric properties. The high rates of suicidal ideations, suicide attempts, and functional impairment in this population suggest the need for preventive interventions.
Keywords: Adolescents, Patient Health Questionnaire-9 teen version, South Africa
INTRODUCTION
Adolescent depression is a disabling mental health disorder, with a prevalence of 5.7% in 13–18-year-old and significant personal and societal costs if untreated.[1] There is a risk of recurrence, interruption of developmental milestones, a cluster of adverse health risk behaviors and suicide. Many scientific guidelines such as preventive US task force recommendations suggest the use of screening tools for an early detection and treatment of depression in 12–18 years old in primary care settings.[2] One such widely used screening instrument for depression is Patient Health Questionnaire-9 (PHQ-9) with proven validity in adolescents and vulnerable population.[3,4] In this paper, we describe the adaptation and validation of teen version of PHQ-9,[5] in a socioeconomically disadvantaged population of South African adolescents.
South African Depression and Anxiety Group (SADAG) is a registered nongovernmental organization working in the area of patient advocacy, education, and de-stigmatization of mental illness in the South Africa. A preventive initiative called suicide should not be a secret (SSS) was designed by SADAG to target the most vulnerable, and difficult to reach groups in the community. SSS aimed at training the educators and providing psychoeducation to adolescents about depression and suicide. In this report, we are presenting the findings from the survey conducted in rural, semi-rural, and impoverished areas of Gauteng province. The objective of the survey was to test the adapted teen version of PHQ-9 in a cohort of South African adolescents and assess the functional impairment due to depressive symptoms. A part of this survey has been published elsewhere.[6]
METHODOLOGY
SADAG conducted a school-based survey during which the teen version of PHQ-9 was administered to 100 school going adolescents from secondary schools in impoverished regions of Gauteng province in a pilot, with an extremely poor response rate of <10%. The various reasons for the poor response rate were explored, and several measures were implemented to improve it.
Presentations were made on depression of 60 min duration to improve the awareness and understanding of the concept and the questions, delivered by trained presenters with experience in dealing with depression in youth. These presentations were delivered to the target population of secondary students from 35 schools in rural/semirural/impoverished regions of Gauteng province and covered topics ranging from: The pressures faced by teenagers today; signs and symptoms of depression in young people; identification of early warning signs; common myths associated with depression; practical strategies for offering support; resources to get help; and how to communicate with someone they are worried about.
Furthermore, the surveyors decided to test the improvement in the response rate by simplifying the questionnaire by reducing the number of points in the scale. The 4-point scale of PHQ-9 teen version (0 = not at all; 1 = several days; 2 = more than half the days; and 3 = nearly every day) was reduced to a 3-point scale (0 = not at all; 1 = sometimes; and 2 = most of the time). Subsequent to the presentations, the abovementioned modification of PHQ-9 teen version (PHQ-9M) was administered to 2025 adolescent participants from 35 schools over 2 years.
RESULTS
The response rate with the implemented measures improved to over 90%. There were 1999 valid questionnaires and 26 questionnaires with inadequate responses (51.8% males and 48.2% females). The mean age of the participants was 15.8 (standard deviation [SD] = 1.8 years). Scores on the PHQ-9 teen version range from 0 to 27. On the PHQ-9M in this study, the scores range from 0 to 18. A total of 456 respondents (23%) scored an arbitrary cutoff score of 9 or above on PHQ-9M.
One of the four additional questions on PHQ-9 teen version measures functional impairment due to the symptoms in the past year. In our survey, using PHQ-9M, 1287 adolescents (64%) reported some functional impairment and 187 (9.3%) reported severe functional impairment due to the symptoms. The mean PHQ score of adolescents with functional impairment was 7.05 (SD = 3.28). This was significantly higher than the scores in the group without any functional impairment (mean difference = 2.21, 95% confidence interval [CI] = 1.904–2.509, χ2 = 0.133) [Table 1]. Furthermore, about 60% of those reporting severe functional impairment due to symptoms scored 9 or above on PHQ-AM.
Table 1.
Mean Patient Health Questionnaire-9 M scores and standard deviation
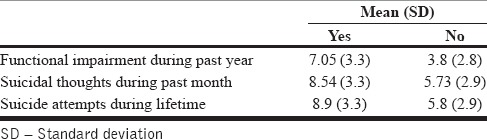
In response to the other additional questions, 535 adolescents (26.7%) reported suicidal ideations during the previous month and 436 (21.8%) reported lifetime suicide attempts. An independent-samples t-test showed significantly higher scores for those reporting suicidal ideations compared to those without suicidal ideations (mean difference = 2.81, 95% CI = 3.13–2.5) and those with suicide attempts compared to those without suicide attempts (mean difference = 3.096, 95% CI = 3.44–2.75) [Table 1].
DISCUSSION
The internal consistency of PHQ-9M was fair with a Cronbach alpha coefficient of 0.64 as compared to a Cronbach alpha coefficient of 0.89 of PHQ-9.[7] We could not assess the criterion validity of the modified version by comparing scores to the original, due to extremely poor response rates on the original version. We can assume the face validity of PHQ-9 M as a valid screen of depression in adolescents when compared with the standard version, as the questions on the modified version are the same.
In this report, use of presentations to create awareness and increase literacy about depression and the modification of a standard scale was successfully utilized to improve the response rates. It might have been easier for the participants to respond to a 3-point scale because of the limited understanding of the psychological concepts and poor mental health (and general) literacy in this largely disadvantaged group. According to Raaijmakers,[8] midpoints are necessary for the respondents with the limited knowledge about the survey concepts, to reduce the nonresponse rate by selecting the midpoint to indicate the sense of “undecided” or “don’t know.” Further studies are required for a comprehensive assessment of the psychometric properties and utility of the modified version, in the context of the literature showing the greatest effect on the psychometric properties of the scale when the response points reduced from 3 to 2.[9]
The rate of severe functional impairment of 9.3% is higher when compared to rates of impairment due to depression in other prevalence studies in adolescent population.[1] Furthermore, the rates of suicidal ideations and suicide attempts were also much higher compared to the estimated lifetime prevalence of suicidal ideations (9.1%) and suicide attempts (2.9%) found in nationally representative South African Stress and Health study.[10] Both the findings could be due to the nonrepresentative nature of our sample and the socio-demographics of the population in this study. Our survey was conducted in the disadvantaged adolescents from remote areas in Johannesburg with possible socio-economic difficulties impacting upon their general stress levels. Recent findings from Saving and Empowering Young Lives in Europe study highlight the importance of early identification of not only threshold but subthreshold depression and anxiety to minimize functional impairment and suicide in adolescents.[11]
A high proportion (23%) of adolescents scored 9 or above on the PHQ-9M, indicating the possible presence of depressive symptoms. SADAG is currently trying to improve mental health literacy and awareness about depression in adolescents in this region, and the mental health literacy campaign findings are described in a separate paper.[6] To conclude, the PHQ-9M could be a useful tool in conducting surveys in low mental health literacy settings, after further psychometric evaluation. The findings also highlight the need for preventive measures to target the high rates of suicidal ideations, suicide attempts, and functional impairment due to depressive symptoms in this population.
Limitations
This is a preliminary study to evaluate the adaptation of PHQ teen version in a specific cohort of South African adolescents. Further studies are required to test its psychometric properties and generalizability to the other adolescent populations.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Jane Costello E, Erkanli A, Angold A. Is there an epidemic of child or adolescent depression? J Child Psychol Psychiatry. 2006;47:1263–71. doi: 10.1111/j.1469-7610.2006.01682.x. [DOI] [PubMed] [Google Scholar]
- 2.Williams SB, O’Connor EA, Eder M, Whitlock EP. Screening for child and adolescent depression in primary care settings: A systematic evidence review for the US Preventive Services Task Force. Pediatrics. 2009;123:e716–35. doi: 10.1542/peds.2008-2415. [DOI] [PubMed] [Google Scholar]
- 3.Maurer DM. Screening for depression. Am Fam Physician. 2012;85:139–44. [PubMed] [Google Scholar]
- 4.Richardson LP, McCauley E, Grossman DC, McCarty CA, Richards J, Russo JE, et al. Evaluation of the patient health questionnaire-9 item for detecting major depression among adolescents. Pediatrics. 2010;126:1117–23. doi: 10.1542/peds.2010-0852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Richardson LP, Katon W, Russo JE, Rockhill C, McCarty C, Richards J, et al. Honolulu, HI: 2009. Screening Characteristics and Validity of the Patient Health Questionnaire-9 (PHQ-9) Among Adolescents. Poster Presented at the 56th Annual Meeting of the American Academy of Child and Adolescent Psychiatry. [Google Scholar]
- 6.Aggarwal S, Berk M, Taljard L, Wilson Z. South African adolescents’ beliefs about depression. Int J Soc Psychiatry. 2016;62:198–200. doi: 10.1177/0020764015618226. [DOI] [PubMed] [Google Scholar]
- 7.Kroenke K, Spitzer RL, Williams JB. The PHQ-9: Validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Raaijmakers QA. Adolescents’ midpoint responses on likert-type scale items: Neutral or missing values? Int J Public Opin Res. 2000;12:209–17. [Google Scholar]
- 9.Lee J, Paek I. In search of the optimal number of response categories in a rating scale. J Psychoeduc Assess. 2014;32:663–73. [Google Scholar]
- 10.Tomlinson M, Grimsrud AT, Stein DJ, Williams DR, Myer L. The epidemiology of major depression in South Africa: Results from the South African stress and health study. S Afr Med J. 2009;99(5 Pt 2):367–73. [PMC free article] [PubMed] [Google Scholar]
- 11.Balázs J, Miklósi M, Keresztény A, Hoven CW, Carli V, Wasserman C, et al. Adolescent subthreshold-depression and anxiety: Psychopathology, functional impairment and increased suicide risk. J Child Psychol Psychiatry. 2013;54:670–7. doi: 10.1111/jcpp.12016. [DOI] [PubMed] [Google Scholar]