

Abstract
Here, we report a fetus with a rare aortic arch anomaly with left aortic arch and right ductus arteriosus, which has not been reported so far. In this condition, the aorta extends to the left of the trachea as in normal, while the ductus arteriosus extends to the right of the trachea and joins the descending aorta posterior to the trachea, with a cross-ribbon sign.
Keywords: Aortic arch, anomaly, prenatal diagnosis, right ductus arteriosus
Introduction
Inclusion of outflow tracts and three vessel trachea in fetal echocardiography has improved the prenatal diagnosis of anomalies of aortic arch. Prenatal sonographic features of newer patterns of these anomalies are being described. Here, we report the features of one such pattern with left aortic arch and right ductus arteriosus.
Case Report
A 23-year-old low risk pregnant woman, gravida 1, Para 0 presented for the routine anomaly scan at 28 weeks. The biometry corresponded to menstrual age. There was polyhydramnios. The axial sweep of the fetal heart revealed the normal four chamber view and left ventricular outflow tract [Figure 1A]. The main pulmonary artery was directed towards the right [Figure 1B]. The aortic arch was to the left of the trachea [Figure 1C]. After the origin of branch pulmonary arteries, the ductus arteriosus extended to the right of the trachea and joined the descending aorta behind the trachea to form a complete vascular ring. This mimicked a cross ribbon [Figure 1D; Video 1]. There was indentation on trachea by the vascular ring on sagittal scan. The patient reported loss of fetal movements at 32 weeks and sonography revealed intrauterine fetal death.
Figure 1 (A-E).
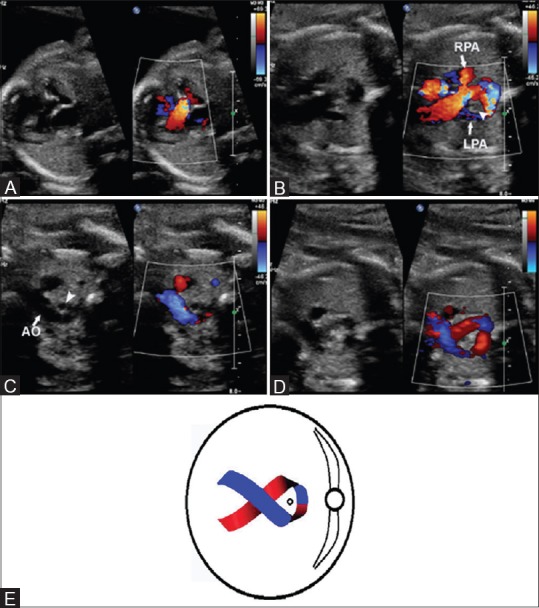
(A) Left ventricular outflow tract view showing the normal origin of aorta from the left ventricle and directed towards the right shoulder. (B) Section just cephalic to A showing the origin of the main pulmonary artery from right ventricle and extending to the right and giving off the branches of right (RPA) and left (LPA) pulmonary arteries and continues to the right of the trachea (arrow head) as ductus arteriosus. (C) Section just cephalic to B shows the aortic arch (AO) extending to the left of the trachea (arrow head). (D) Slightly oblique scan showing the aortic arch to the right and the ductus arteriosus to the left of the trachea and joining together behind the trachea giving a cross-ribbon appearance (E) Line diagram showing the cross ribbon sign
Discussion
Aortic arch anomalies refer to a variety of congenital abnormalities of the position or branching pattern or both of the aortic arch.[1,2,3,4] They may be associated with congenital cardiac defects, chromosomal anomalies, or present as incidental findings in asymptomatic infants. Some anomalies of the aortic arch, particularly those with aberrant branching, may form vascular rings, causing clinical symptoms from tracheal or esophageal compression.[5,6] Various types of congenital aortic arch abnormalities have been described; however, most have been reported in the pediatric or radiological literature using magnetic resonance imaging (MRI) and spiral computed tomography (CT).[7,8,9] Although aortic arch anomalies are not uncommon, there are few reports on their prenatal diagnosis.[10,11,12,13] Normal and abnormal development of the aortic arch can be easily understood by reference to the hypothetical double aortic arch model described by Dr. Jesse E. Edwards [Figure 2A].[4,14,15,16] The model illustrates a fairly late stage of development. An aortic arch connects the ascending aorta to the descending aorta, and a ductus arteriosus (ductus) connects the ipsilateral pulmonary artery to the descending aorta, on each side of the trachea and esophagus, forming a complete vascular ring. Each aortic arch gives rise to a common carotid artery and a subclavian artery. Normally, the left aortic arch and left ductus persist, and the right aortic arch distal to the origin of the right subclavian artery and the right ductus regress. Most of the aortic arch anomalies are assumed to result from abnormal persistence of a part or parts that should have regressed and/or abnormal regression of a part or parts that should have persisted. The left or right-sidedness of the aortic arch refers to the position of the aortic arch relative to the trachea. It does not refer to which side of the midline the aorta ascends.[2] The left and right-sidedness of the ductus can also be defined by its position relative to the trachea.[11] This relationship is best seen in the three vessel trachea (3VT) view of the fetal heart, as described by Yagel et al.[17] Normally, both the aortic arch and ductus arteriosus are scanned as a “V” to the left of the trachea with the apex pointing posteriorly. In the right aortic arch, with mirror image branching and right ductus arteriosus, left aortic arch distal to the origin of the left subclavian artery and the left ductus arteriosus regress. In this condition, the aortic arch and ductus arteriosus are seen to the right of the trachea on fetal echo, and seen as a “V” on the right side.[18] In right aortic arch with left ductus arteriosus, the left aortic arch between common carotid and subclavian arteries and right ductus arteriosus regress. On fetal echo, there is U sign with aortic arch to the right of the trachea and ductus arteriosus to the left of the trachea.[16,19] In double aortic arch, aortic arch of both the sides persists and right ductus arteriosus regresses.
Figure 2 (A-C).
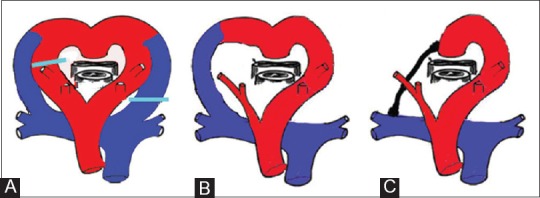
(A) Hypothetical double aortic arch model described by Edwards JE (modified from reference) and the developmental model of the anomaly described in this case report showing the segments of the right aortic arch and left ductal arch that regress. (B) Fetal circulation in this anomaly. (C) Postnatal circulation when the right ductus remains as the ligamentum ductus
In the fetus described here, there was left aortic arch with right ductus arteriosus. This results from regression of the right aortic arch distal to subclavian artery and the left ductus arteriosus [Figure 2]. In left ventricular outflow tract view, the ascending aorta is directed to the right and then turns to the left and extends to the left of trachea. The main pulmonary artery and the ductus arteriosus are seen to extend to the right of the trachea. The aortic arch and ductus arteriosus unite behind the trachea to form a complete vascular ring around the trachea and esophagus. Consequently, the aorta and ductus arteriosus are in the form of a cross ribbon. Because of a complete vascular ring, the trachea and esophagus may be compressed and result in polyhydramnios. To our knowledge, this pattern of anomaly of aortic and ductal arches has not been reported so far.
Video Available on: www.ijri.org
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Moes CAF. Vascular rings and related conditions. In: Freedom RM, Mawson JB, Yoo SJ, Benson LN, editors. Congenital Heart Disease. Textbook of Angiocardiograph. Armonk, NY: Futura Publishing Co; 1997. pp. 947–83. [Google Scholar]
- 2.Weinberg PM. Aortic arch anomalies. In: Emmanouilides GC, Allen HD, Riemenschneider TA, Gutgesell HP, editors. Heart Disease in Infants, Children, and Adolescents. Baltimore, MD: Williams & Wilkins; 1995. pp. 810–37. [Google Scholar]
- 3.Park SC, Zuberbuhler JR. Vascular ring and pulmonary sling. In: Anderson RH, Macartney FJ, Shinebourne EA, Tynan M, editors. Pediatric Cardiology. Edinburgh, UK: Churchill Livingstone; 1987. pp. 1123–36. [Google Scholar]
- 4.Edwards JE. Vascular rings and slings. In: Moller JH, Neal WA, editors. Fetal, Neonatal, and Infant Cardiac Disease. Norwalk, CT: Appleton and Lange; 1990. pp. 745–54. [Google Scholar]
- 5.Goor DA. Congenital Malformations of the Heart. Embryology, Anatomy and Operative Considerations. New York: Grune & Stratton; 1975. [Google Scholar]
- 6.Knight L, Edwards JE. Right aortic arch. Types and associated anomalies. Circulation. 1974;50:1047–51. doi: 10.1161/01.cir.50.5.1047. [DOI] [PubMed] [Google Scholar]
- 7.Hopkins KL, Patrick LE, Simoneaux SF, Bank ER, Parks WJ, Smith SS. Pediatric great vessel anomalies: Initial clinical experience with spiral CT angiography. Radiology. 1996;200:811–5. doi: 10.1148/radiology.200.3.8756937. [DOI] [PubMed] [Google Scholar]
- 8.Kersting-Sommerhoff BA, Sechtem UP, Fisher MR, Higgins CB. MR imaging of congenital anomalies of the aortic arch. AJR Am Roentgenol. 1987;149:9–13. doi: 10.2214/ajr.149.1.9. [DOI] [PubMed] [Google Scholar]
- 9.Katz M, Konen E, Rozenman J, Szeinberg A, Itzchak Y. Spiral CT and 3D reconstruction of vascular rings and associated tracheobronchial anomalies. J Comput Assist Tomogr. 1995;19:564–8. doi: 10.1097/00004728-199507000-00011. [DOI] [PubMed] [Google Scholar]
- 10.Bronshtein M, Lorber A, Berant M, Auslander R, Zimmer EZ. Sonographic diagnosis of fetal vascular rings in early pregnancy. Am J Cardiol. 1998;81:101–3. doi: 10.1016/s0002-9149(97)00864-3. [DOI] [PubMed] [Google Scholar]
- 11.Yoo SJ, Lee YH, Kim ES, Ryu HM, Kim MY, Yang JH, et al. Tetralogy of Fallot in the fetus: Findings at targeted sonography. Ultrasound Obstet Gynecol. 1999;14:29–37. doi: 10.1046/j.1469-0705.1999.14010029.x. [DOI] [PubMed] [Google Scholar]
- 12.Yoo SJ, Lee YH, Cho KS, Kim DY. Sequential segmental approach to fetal congenital heart disease. Cardiol Young. 1999;9:430–44. doi: 10.1017/s1047951100005266. [DOI] [PubMed] [Google Scholar]
- 13.Hornberger LK. Aortic arch anomalies. In: Allan L, Hornberger L, Sharland G, editors. Textbook of Fetal Cardiology. London, UK: Greenwich Medical Media; 2000. pp. 305–21. [Google Scholar]
- 14.Edwards JE. “Vascular rings” related to anomalies of the aortic arches. Mod Concepts Cardiovasc Dis. 1948;17:19–20. [PubMed] [Google Scholar]
- 15.Edwards JE. Malformation of the aortic arch system manifested as “vascular rings”. Lab Invest. 1953;2:56–75. [PubMed] [Google Scholar]
- 16.Yoo SJ, Min JY, Lee YH, Roman K, Jaeggi E, Smallhorn J. Fetal sonographic diagnosis of aortic arch anomalies. Ultrasound Obstet Gynecol. 2003;22:535–46. doi: 10.1002/uog.897. [DOI] [PubMed] [Google Scholar]
- 17.Yagel S, Arbel R, Anteby EY, Raveh D, Achiron R. The three vessels and trachea view (3VT) in fetal cardiac scanning. Ultrasound Obstet Gynecol. 2002;20:340–5. doi: 10.1046/j.1469-0705.2002.00801.x. [DOI] [PubMed] [Google Scholar]
- 18.Iliescu DG, Comanescu AC, Tudorache S, Cernea N. Right aortic arch with patent right ductus arteriosus and normal heart. Ultrasound Obstet Gynecol. 2012;40:115–6. doi: 10.1002/uog.10076. [DOI] [PubMed] [Google Scholar]
- 19.Achiron R, Rotstein Z, Heggesh J, Bronshtein M, Zimand S, Lipitz S, et al. Anomalies of the fetal aortic arch: A novel sonographic approach to in utero diagnosis. Ultrasound Obstet Gynecol. 2002;20:553–7. doi: 10.1046/j.1469-0705.2002.00850.x. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.