

Abstract
Background:
Value added services (VAS) are an innovative dispensing system created to provide an alternative means of collecting partial drug supply from our hospital. This in turn was projected to reduce the necessity for patient to visit pharmacy counter and thus reduce the burden of prescription handling.
Objective:
To evaluate the impact of increased VAS uptake following promotional campaign towards patient waiting time and to explore factors that may affect patient waiting time at the Ambulatory Pharmacy, Queen Elizabeth Hospital.
Methods:
A quasi experimental study design was conducted from September 2014 till June 2015 at the Ambulatory Pharmacy. During pre-intervention phase, baseline parameters were collected retrospectively. Then, VAS promotional campaign was carried out for six months and whilst this was done, the primary outcome of patient waiting time was measured by percentage of prescription served less than 30 minutes. A linear regression analysis was used to determine the impact of increased VAS uptake towards patient waiting time.
Results:
An increased in percentage of VAS registration (20.9% vs 35.7%, p<0.001) was observed after the promotional campaign. The mean percentage of prescription served less than 30 minutes increased from 83.2% SD=15.9 to 90.3% SD=11.5, p=0.001. After controlling for covariates, it was found that patient waiting time was affected by number of pharmacy technicians (b=-0.0349, 95%CI-0.0548 : -0.0150, p=0.001), number of pharmacy counters (b=0.1125, 95%CI 0.0631 : 0.1620, p<0.001), number of prescriptions (b=0.0008, 95%CI 0.0004 : 0.0011, p<0.001), and number of refill prescriptions (b=0.0004, 95%CI 0.0002 : 0.0007, p<0.001). The increased in percentage of VAS registration was associated with reduction in number of refill prescription (b=-2.9838, 95%CI -4.2289 : -1.7388, p<0.001).
Conclusions:
Patient waiting time at the Ambulatory Pharmacy improved with the increased in VAS registration. The impact of increased VAS uptake on patient waiting time resulted from reduction in refill prescriptions. Patient waiting time is influenced by number of pharmacy technicians, number of pharmacy counters, number of prescriptions and number of refill prescriptions.
Keywords: Appointments and Schedules, Pharmaceutical Services, Professional Practice, Pharmacy Service, Hospital, Ambulatory Care, Pharmacists, Malaysia
INTRODUCTION
Medication accessibility and continuous supply of medicine are essential for patient with chronic diseases, to maintain their quality of life and reduce healthcare cost.1 Since 2011, the Ministry of Health in Malaysia has implemented a policy in which prescriptions with a duration of more than one month will be supplied on a monthly basis.2,3 This was to enable pharmacists to monitor patient compliance to medication and reduce medication wastage.2 However, this has led to an increase patient load at the Ambulatory Pharmacy and hence prolonged patient waiting time.
We conducted a root-cause analysis and found that the causes of long patient waiting time at the Ambulatory Pharmacy were multifactorial. Inexperienced personnel with non-familiarity of dispensing workflow and drug arrangements would delay dispensing processes. Insufficient manpower was also identified to have caused long patient waiting time. High burden of prescriptions when multiple clinics were in operation also led to congestion. Handling prescription errors would propel a longer processing time. Extra steps in dispensing procedure including counter checking of filled medications before dispensing will slow down dispensing process but this is regarded as an essential process to ensure medication safety in dispensing. Prescription which contains controlled items like Psychotropic substances required longer patient waiting time as compared to standard medications because it requires mandatory recording. Improvising patient waiting time became an important element for the Ambulatory Pharmacy Services as it can negatively affect patient’s satisfaction and also because it is a measureable performance indicator under the Ministry of Health Malaysia, that 95% of prescriptions should be dispensed in less than 30 minutes.4
Various methods have been proposed in other countries to reduce patient waiting time. Some of these include automated dispensing system, manpower scheduling plan, electronically delivered prescription and redesign of pharmacy workflow.4,5,6,7,8 In Malaysia, one of the methods adopted was implementation of Value Added Services (VAS). VAS was created to ease patient on refilling chronic prescription. VAS is a collective of innovative dispensing system which provides patient with alternative means of collecting partial drug supply.3 In general, it consists of Integrated Drug Dispensing System (SPUB), Drive Through Pharmacy, Courier Service, and SMS and Take Service.
Several studies have investigated usage and patient satisfaction on VAS. Survey conducted in a Malaysia government hospital revealed that 96% of their subjects were satisfied with the SMS and Take service quality.9. A study on drive-through pharmacy in Taiwan also showed a high patient satisfaction of up to 90% with increased usage after implementation of the service. Most of these patients found the service more convenient and effective compared to traditional pharmacy service.10 Despite the positive feedback from literatures, we did not find any literature that consists of an evaluation on the impact of VAS in reducing patient waiting time in the Ambulatory Pharmacy. Therefore, the objectives of our study are to evaluate impact of VAS towards patient waiting time in the Ambulatory Pharmacy and to explore the factors associated with patient waiting time when VAS registrations were increased.
METHODS
Study setting
The study was performed in the Ambulatory Pharmacy of Queen Elizabeth Hospital, a tertiary care hospital with over 700 beds in Kota Kinabalu, Sabah, Malaysia. The Ambulatory Pharmacy provides medication dispensing services to both inpatient and outpatient clinics from 7.30am to 10.00pm daily including public holidays. The workflow of conventional medication dispensing in the Ambulatory Pharmacy is represented in Figure 1.
Figure 1.
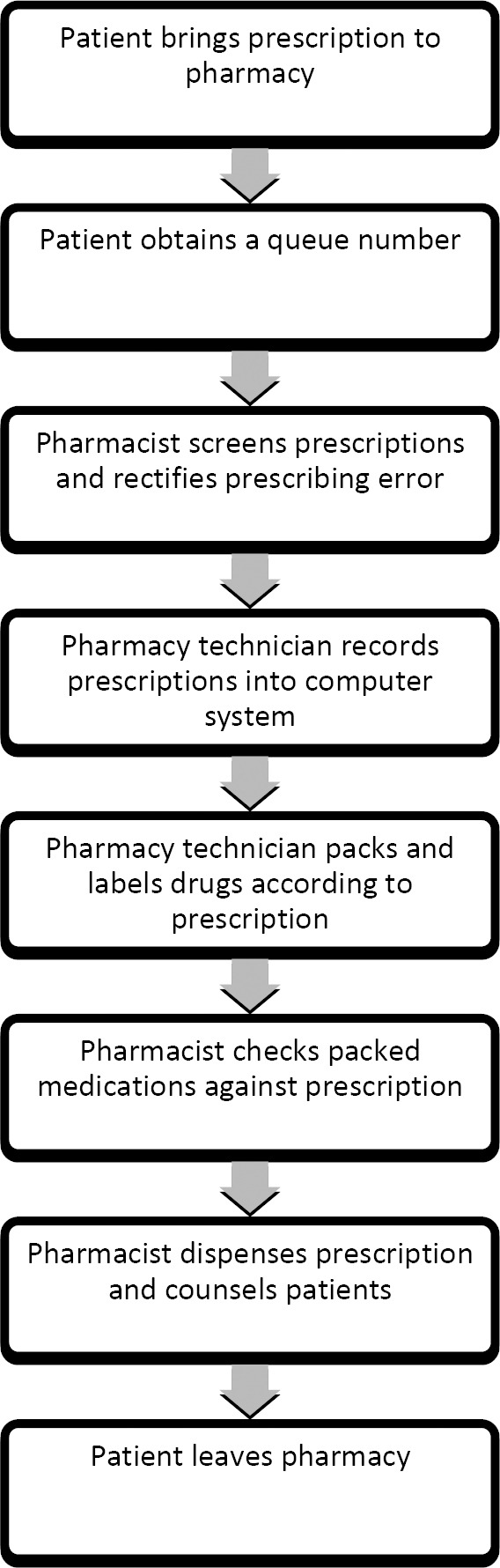
Workflow of conventional medication dispensing.
Study design
A quasi experimental study was performed to measure the impact of increased VAS uptake on patient waiting time in the Ambulatory Pharmacy. During the pre-intervention phase, baseline data was collected retrospectively from September till December 2014. During this period, there was no active promotion for the use of VAS to patients. However, some pharmacists may have inadvertently informed the patients on the availability of VAS at the dispensing counter. Starting from December 2014, activation of promotional campaign was carried out to increase uptake of VAS by patients. The promotional campaign was carried out continuously until June 2015. In post-intervention phase, impact of increased VAS uptake was evaluated. All prescriptions received during office hours (7am – 5pm, Monday to Friday) were included to the study while prescription received after office hour (5pm-7am, weekends and public holidays), one-off prescriptions, walk-in prescriptions and prescriptions with last supply were excluded.
Ethical approval
The study was registered with National Medical Research Register (NMRR-14-1808-23656) and approved by Medical Research Ethics Committee in Malaysia. Consent form was not required for this study because no individual identifiable data was obtained from patients.
Description of intervention
In this study, intervention consists of increased VAS uptake with promotional campaign. With this, we estimated that the increased VAS uptake following promotional campaign will reduce patient waiting time in the Ambulatory Pharmacy. The promotional campaign consisted of seven strategies to increase patient’s awareness on VAS. These include: 1) VAS promotional brochure with VAS selection application form for every patient with refill prescription at receiving counter, 2) active promotion by pharmacist over the dispensing counter, 3) VAS promotional posters, 4) VAS video shows at patient waiting area, (5) promotional advertisement in local newspapers, 6) and radio station, and 7) active promotion during bedside dispensing when patients were discharged from hospital. All pharmacists and pharmacy technicians in the Ambulatory Pharmacy were briefed and trained on the promotional campaign before it started. Training on promotional campaign was done periodically to ensure everyone was aware of the ongoing promotional campaign in the pharmacy. A specific counter was created to handle VAS registrations.
Outcome measurement and data collection
The primary outcome was impact of increased VAS uptake following VAS promotional campaign on patient waiting time, which is measured in terms of percentage of prescription served less than 30 minute. The patient waiting time data can be generated through a computerized Queue Management System. Secondary outcome measured was to explore the factors that affect patient waiting time at the Ambulatory Pharmacy. A customized data collection form was designed by researchers and used to collect data on outcomes of interest. Data collectors were recruited and trained to collect data. Data was collected using a customized form and then transferred onto computer database for analysis.
Statistical analysis
Data was recorded in Microsoft Excel 2013 and analysed by using SPSS 17.0. Independent T and Mann-Whitney test were used to test the difference in outcome variables before and after intervention. All potential variables that might have any influences on the patient waiting time were identified using simple linear regression analysis. These variables were then used to form a model in multiple linear regression to determine the strength of association with patient waiting time. Log transformation was used when the outcome variables of waiting time was not normally distributed. Descriptive data were reported as mean or median. A p value less than 0.05 was considered significant.
RESULTS
A total of 118,379 prescriptions (average of 550 prescriptions per day) were included for analysis throughout the study period. Of these prescriptions, 71658 (60.5%) and 46721 (39.5%) were refill prescriptions and one-off prescriptions respectively. From these refill prescriptions, those that have registered for VAS consisted of 26.7% while 73.3% did not registered for VAS.
As compared to pre-intervention phase, the number of prescriptions, number of dispensing counters and number of pharmacy technicians were significantly lower in post-intervention phase (p < 0.001; Table 1). The number of queries pertaining to prescriptions received and number of pharmacists was notably higher in post-intervention phase. However, it did not confer significance in terms of number of pharmacists on duty (p=0.063).
Table 1.
Differences of variables pre and post-intervention phase (n=215).
| Variables | Before intervention | After intervention | z-statistica | P valuea |
|---|---|---|---|---|
| Num. of prescription | 654.5 (174) | 513 (168) | -6.693 | <0.001 |
| Num. of query | 3.5 (6) | 11 (12) | -7.497 | <0.001 |
| Num. of dispensing counter | 7 (0) | 5 (2) | -6.941 | <0.001 |
| Num. of pharmacist | 21 (4) | 23 (5) | -1.861 | 0.063 |
| Num. of pharmacy technician | 17 (3) | 16 (3) | -2.481 | 0.013 |
Mann-Whitney Test
Effect of intervention on VAS uptake
The effect of promotional campaign on VAS was shown in Table 2. This was to determine the extent of VAS uptake following the heightened awareness. Both the average number of prescriptions registered for VAS (71 vs 103.5; p<0.001) and the percentage of VAS registration (20.9% vs 35.7%, p<0.001) increased significantly with promotional campaign. Among the different types of VAS, SPUB remains the favourite among VAS users comprised of 84.8% of all VAS registration, followed by drive-through pharmacy (12.9%), SMS and take service (1.1%) and courier service (1.1%). Similarly, we saw significant improvement in percentage of prescription served less than 30 minutes (83.2; SD=15.9 vs 90.3; SD=11.5; p=0.001) and a reduction in average waiting time (21.2; SD=7.1 vs 17.7; SD=12.9; p=0.033).
Table 2.
Effect of VAS promotional campaign on pharmacy activities (n=215).
| Variables | Before intervention | After intervention | t-statistic (df)b | p-valueb |
|---|---|---|---|---|
| Number of Refill prescriptions Median (IQR) | 391 (301) | 276 (172) | -4.475c | <0.001c |
| VAS registration (%) Mean; SD | 20.9; 16.9 | 35.7; 19.3 | 5.636 (201) | <0.001 |
| Prescription served less than 30 minutes (%) Mean; SD | 83.2; 15.9 | 90.3; 11.5 | 3.431 (138.9) | 0.001 |
| Average waiting time (min) Mean; SD | 21.2; 7.1 | 17.7; 12.9 | -2.143 (203) | 0.033 |
Independent t Test;
Z-statistic, Mann-Whitney Test
Impact of factors towards pharmacy waiting time
When the factors were further analysed by linear regression analysis, the number of pharmacy technicians, number of pharmacy counters, number of prescriptions and number of refill prescriptions were found to be significant (Table 3 and 4). The model fitted fairly and accounted for 44.6% of variation in waiting time (R-sq=0.446). Percentage of prescription served less than 30 minutes was primarily affected by number of pharmacy technicians (b=-0.0349, 95%CI: -0.0548 : -0.0150, p=0.001), number of pharmacy counters (b=0.1125, 95%CI 0.0631:0.1620, p<0.001), number of prescriptions (b=0.0008, 95%CI: 0.0004 : 0.0011, p<0.001), and number of refill prescriptions (b=0.0004, 95%CI: 0.0002 : 0.0007, p<0.001). When other variables were held constant, increase of pharmacy technician by 1 unit would increase the percentage by 0.1352%. When pharmacy counter was increased by 1 unit, the percentage of prescription served less than 30 minutes would reduce by 0.5191% (p<0.001). When pharmacy technician is increased by 1 unit, the percentage would increase by 0.1352%. Increase of total daily prescription by 1 would reduce the percentage by 0.004% (p<0.001). Refill prescription also significantly associated with waiting time but the association was weak as compared to other factors. When number of refill prescription was increased by 1, the patient waiting time would reduce by 0.0004% (p<0.001).
Table 3.
Simple linear regression analysis evaluating the impact of factors towards percentage of prescription served less than 30 minutes (n=215).
| Variable (x) | Simple linear regression | p-value | ||
|---|---|---|---|---|
| Log (101-y) | % change in y for every increase in 1 unit x | |||
| b | 95%CI | |||
| Num. of pharmacists | 0.0044 | -0.0142, 0.0231 | -0.0679 | 0.6394 |
| Num. of pharmacy Technicians | 0.0009 | -0.0230, 0.0248 | -0.0207 | 0.9392 |
| Num. of pharmacy counters | 0.1841 | 0.1444, 0.2238 | -0.3639 | <0.001 |
| Num. of queries | 0.0041 | -0.0036, 0.0117 | -0.0790 | 0.2966 |
| Num. of prescriptions | 0.0014 | 0.0011, 0.0017 | -0.0031 | <0.001 |
| Num. of refill prescriptions | 0.0007 | 0.0005, 0.0011 | -0.0143 | <0.001 |
| ŦPost-intervention | -0.2376 | -0.3472, -0.1281 | 5.6711 | <0.001 |
y=Percentage prescription with waiting time less than 30 minutes
b= crude regression coefficient
Post intervention=1, Pre intervention=0
Table 4.
Multiple linear regression analysis evaluating the impact of factors towards percentage of prescription served less than 30 minutes (n=215).
| Variable (x) | Multiple linear regressiona | p value | ||
|---|---|---|---|---|
| Log (101-y) | % change in y for every increase in 1 unit x | |||
| Adj. b | 95%CI | |||
| No. of pharmacy technicians | -0.0349 | -0.0548, -0.0150 | 0.1352 | 0.001 |
| No. of pharmacy counters | 0.1125 | 0.0631, 0.1620 | -0.5191 | <0.001 |
| No. of prescriptions | 0.0008 | 0.0004, 0.0011 | -0.0040 | <0.001 |
| No. of refill prescriptions | 0.0004 | 0.0002, 0.0007 | -0.0004 | <0.001 |
Adj. b=adjusted regression coefficient
R2=0.446; the model reasonably fits well; model assumptions are met; there is no interaction detected; there is no multicollinearity problems
Final Model: Log10 (101 – y) = 0.239 – (0.035*Pharmacy technician) + (0.113*pharmacy counter) + (0.001*total prescription) + (0.0001*refill prescription)
Impact of VAS registration towards refill prescription
The extent of the effect of VAS registration on number of refill prescription at the Ambulatory Pharmacy was determined. Simple linear regression analysis showed that an increased in VAS uptake was significantly associated with the reduction in number of refill prescriptions (b=-2.9838, 95%CI -4.2289 : -1.7388, p<0.001). With an increase of VAS registration by 1 unit, it would have reduced the number of refill prescriptions by 3. Result of simple linear regression was presented in Table 5.
Table 5.
Simple regression analysis between percentage of VAS registration and number of refill prescriptions (n = 215).
| Variable (x) | Simple Linear Regression | ||
|---|---|---|---|
| b | 95% CI | p-value | |
| Percentage of VAS registration | -2.9838 | -4.2289,-1.7388 | <0.001 |
y = Refill prescription
b = crude regression coefficient
aR2= 0.100; the model reasonably fits well; model assumptions are met; there is no multicollinearity problems
DISCUSSION
The objectives of this study were to investigate the impact of increased in VAS uptake and to explore the factors associated with patient waiting time at the Ambulatory Pharmacy. Through an active promotional campaign, VAS registration increased significantly from 20.9% to 35.7% (p<0.001). Meanwhile, percentage of prescription served less than 30 minutes also improved from 83.2% to 90.3% (p=0.001). From this study, it was found that patient waiting time was significantly associated with number of pharmacy technicians, number of pharmacy counters, number of prescriptions and number of refill prescriptions.
In our hospital, one of the most commonly used VAS is SPUB. This service allows patients to refill prescription freely from any government healthcare facilities that are conveniently located to their home, office and villages. This is particularly useful for our patients who majority comes from remote areas in Sabah. Drive-through pharmacy is another service whereby monthly partial drug supplies are delivered via the drive through counter on given appointment date. This is initiated to increase patient’s convenience and relieve congested parking spaces in busy hospitals. However, unclear location of Drive Through counter and traffic congestion at the Drive Through lane were among the negative experiences reported by the patients. Courier service is another VAS offered by our hospitals. Main advantage of this service is delivery of partial drug supplies to patient’s doorstep with minimal postal fee being imposed to the patient. Geriatric patients benefited most from this service as most of them have difficulties replenishing medicines in hospitals and clinics due to transport issues. However, delay postal delivery, concern of medication error and additional postal fee were barriers that impede usage of the service. SMS and Take is another service that falls under VAS. It requires patients to send short messages about their details and desired time of collections to pharmacy hotline. Upon receiving the messages, patients’ prescriptions will be filled in advance. Patients only need to show their prescription numbers and collect their medicines without having to queue. However, elderly or illiterate patients who don’t know how to use a mobile phone might not be able to utilise this service.
Patient waiting time at the Ambulatory Pharmacy has consistently been a factor in determining quality of pharmaceutical care services provided. Therefore, shortening this waiting time has been a well-established and important goal of Ambulatory Pharmacy. An in-depth meeting with senior pharmacists from the Ambulatory Pharmacy revealed a few factors which they felt could be causing prolonged patient waiting time. As shown in table 6, these factors can be grouped into four major categories, including insufficient staff, excessive number of patients, increasing number of prescription errors and a questionable dispensing workflow. VAS can potentially overcome these by reducing the number of incoming refill prescriptions during peak hours. Apart from that, it also enables a more flexible workload management because refill prescriptions under VAS can be filled during off-peak hours. Although VAS is being perceived to be time-, effort- and fuel-saving, arising from convenience in drug collection, little is known about its impact on patient waiting time in the Ambulatory Pharmacy. With this study, at least we could perceive the extent of VAS in improving patient waiting time at the counter.
In our literature review, we notice that studies were conducted to examine public perception towards VAS and to identify barriers that prevent patients from adopting VAS.11,12 None has actually evaluated the impact of VAS in shortening patient waiting time. Few studies have reported improvement in patient waiting time by using other interventions. Chou and colleagues suggested that reengineering the prescription-filling process that involves reorganizing dispensing units, opening of extra dispensing window and relocation of drug arrangement can reduce outpatients’ waiting time and enhance the quality and competitiveness of their Hospital’s medical treatment.13 A study done in Abu Dhabi also showed a reduction in average patient waiting time when a fast track dispensing window was introduced to dispense prescription with 3 items or less.14 However, Tan and colleagues who studied the impact of automating the prescription filling function using a prototype has failed to improve the waiting time target. They concluded that automation was still a useful and low cost method to improve waiting time but the speed of the system needs to be upgraded.5 Our study indicates that an increased in VAS registration will result in shorter patient waiting time. However, a comparison in terms of magnitude in improvement of waiting time between these studies is not possible as different settings possess different dispensing workflow and different methods were employed. Apart from that, parameters used to measure patient waiting time in other studies also varied. Nevertheless, the results of our study have offered an insight on how VAS has an impact onto the patient waiting time for dispensing of medications at the Ambulatory Pharmacy in our hospital.
Results of the regression analysis showed that higher number of pharmacy technicians was associated with higher percentage of prescription served less than 30 minutes. This may appear self-evident as pharmacy technician plays an important role in medication dispensing activity, assisting in recording, packaging and labelling of medications. This also suggests the presence of bottleneck at the stage of prescription filling. Insufficient number of pharmacy technicians can cause the prescriptions to pile up while waiting to be dispensed.5 Ideal ratio of pharmacy technician to prescriptions should be further studied in order to overcome this bottleneck. One might assume that higher number of dispensing counter may lead to shorter patient waiting time. However, our study showed that higher number of dispensing counter was associated with longer patient waiting time. This could be due to the interior layout of the Ambulatory Pharmacy whereby pharmacy staff needs to travel further to dispatch prescriptions when there is more operating pharmacy counter. Apart from that, higher number of dispensing counters caused manpower to scatter across the Ambulatory Pharmacy. As a result, pharmacy staff tends to spend their time on non-productive activities. Higher number of prescriptions and refill prescriptions were inversely associated with patient waiting time. The increased amount of workload with same amount of pharmacy staff causes the Ambulatory Pharmacy to work above its capacity. Inability to solve this problem will compromise patient care and cause overcrowding in the Ambulatory Pharmacy especially during clinic hours.
Higher amount of prescriptions received by Ambulatory Pharmacy, regardless of total or refill prescriptions, is associated with prolonged patient waiting time. Our regression model found that VAS can significantly reduce number of refill prescriptions at the pharmacy counter during office hours and hence shorten the patient waiting time, but the impact was very marginal. This could be attributed to the attainment of percentage of VAS registration. We postulate that a VAS registration of more than 30% is needed to provide a better achievement to reduce patient waiting time. An attempt is in place to request for administration level in our hospital to adopt a policy for refill prescriptions to use VAS services. However, this may be inundated with a few problems concerning perceptions of the public, as studied by CLH Tan et al on the patients understanding, beliefs and experiences with using VAS. In this study, it was reported that concerns pertaining to delay of postal deliver, concern over medication errors, traffic congestion at drive-through lane, unwillingness to pay for postal fee, lack of knowledge and awareness, and lack of personal motivation were the common feedbacks.11 Policy makers or providers alike should look into these concerns before develop interventions to improve the services.
Strength and limitation
Large sample size and long period of follow up were the major strengths of this study. A total of 118379 prescriptions were included for analysis and the patient waiting time in the Ambulatory Pharmacy was followed up for up to 6 months in post-intervention phase. Measurement of patient waiting time using the computerised Queue Management System ensured a standardised approach and consistent data collection throughout the study period. Furthermore, possible confounding variables on patient waiting time were also controlled and taken into consideration during the study analysis. This study does, however, have some limitations. Although we have taken into consideration some of the confounding variables affecting patient waiting time, other possible factors such as staff productivity and experience, and number of items in prescription were not being studied. Apart from that, our results have yet to reflect full impact of VAS on patient waiting time as the percentage of VAS registration was not maximised. In terms of study design, head to head comparison with a control arm consisting of an Ambulatory Pharmacy without VAS implementation would have provided a better estimate on impact of VAS. However, this is not possible in our setting as most Ministry of Health-affiliated healthcare facilities have started implementing VAS before our study was conducted. Changes of patient waiting time over a period would be a better indicator of VAS impact as compared to comparison of mean before and after intervention. This requires more advanced statistical method such as interrupted time series analysis. Lastly, our findings might not be generalizable to other Ambulatory Pharmacy in other hospitals because the medical services are only for adult patients and also the differences in dispensing workflow.
Implications of findings and future research
Results of our study showed that promotional campaign can increase the enrolment rate of VAS through improved patients’ awareness. Hence, this method can be implemented in other hospitals with low VAS enrolment rate to increase usage of VAS among patients. However, VAS usage was yet to be maximised despite the promotional campaign. This showed the presence of other barriers is limiting the usage of VAS apart from patients’ awareness. Future studies should embark to study other possible limiting factors. Data from this study will also serve as a baseline data or reference for policymaker to study new performance indicator for the services. Our study also provides additional understanding on how patient waiting time varies in different pharmacy setting. A follow-up study to further improve patient waiting time can be conducted by optimising these factors. Our findings suggested that VAS was able to reduce burden of prescription in the Ambulatory Pharmacy and improve patient waiting time but the impact was only marginal.
CONCLUSIONS
Increased VAS registration has resulted in improvement in percentage of prescription served less than 30 minutes and reduction in average patient waiting time. Patient waiting time was found to be associated with the number of dispensing counters, number of pharmacy technicians, number of prescriptions and number of refill prescriptions. Although VAS is effective in reducing the number of refill prescriptions, percentage of VAS registration need to be further increased in order to detect a practically significant improvement in patient waiting time.
ACKNOWLEDGEMENT
We would like to thank the Director General of Health Malaysia for permission to publish the results of this study.
Footnotes
CONFLICT OF INTEREST
The authors declare no conflict of interest in this study.
FUNDING
None.
Contributor Information
Benjamin C. Loh, BPharm. Pharmacy Department, Queen Elizabeth Hospital. Kota Kinabalu, Sabah (Malaysia). uraws87@gmail.com
Kheng F. Wah, BPharm. Pharmacy Department, Queen Elizabeth Hospital. Kota Kinabalu, Sabah (Malaysia). Khengfui.wah@gmail.com
Carolyn A. Teo, BPharm. Pharmacy Department, Queen Elizabeth Hospital. Kota Kinabalu, Sabah (Malaysia). aili_lyn88@hotmail.com
Nadia M. Khairuddin, BPharm. Pharmacy Department, Queen Elizabeth Hospital. Kota Kinabalu, Sabah (Malaysia). nadiakhairudin@gmail.com
Fairenna B. Fairuz, BPharm. Pharmacy Department, Queen Elizabeth Hospital. Kota Kinabalu, Sabah (Malaysia). fairenna@gmail.com
Jerry E. Liew, MPharm (Clin), BCPS. Pharmacy Department, Queen Elizabeth Hospital. Kota Kinabalu, Sabah (Malaysia). jerliew@gmail.com
References
- 1.Wiedenmayer K, Summers RS, Mackie CA, Gous AG, Everard M, Tromp D. Developing pharmacy practice: a focus on patient care. The Hague: WHO-FIP; 2006. [Google Scholar]
- 2.Rahman DEA. Why Medications Given on Monthly Basis. Malaysia: The Star Online; 2011. [accesed 2011 21 July]. Available from: http://www.mps.org.my/newsmaster.cfm?&menuid=36&action=view&retrieveid=3465 . [Google Scholar]
- 3.Ahmad A, Hassan Y, Aziz N, Hashim R, Bahrin NLZ. Pharmacy dispensing value-added services: determination of patients enrolment rate and factors influencing. 4th International Conference on Pharmaceuticals, Nutraceuticals and Cosmetic Science; Selangor (Malaysia): Jul 1 2015. doi: 10.13140/RG.2.1.4748.1689. [Google Scholar]
- 4.Bahadori M, Mohammadnejhad SM, Ravangard R, Teymourzadeh E. Using queuing theory and simulation model to optimize hospital pharmacy performance. Iran Red Crescent Med J. 2014;16(3):e16807. doi: 10.5812/ircmj.16807. doi: 10.5812/ircmj. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Tan WS, Chua SL, Yong KW, Wu TS. Impact of pharmacy automation on patient waiting time: an application of computer simulation. Ann Acad Med Singapore. 2009;38(6):501–507. [PubMed] [Google Scholar]
- 6.Choon OH, Leng CW, Ai WJ, Chai TM. Evaluation of manpower scheduling strategies at outpatient pharmacy with discrete-event simulation. OR Insight. 2013;26(1):71–84. doi: 10.1057/ori.2012.9. [Google Scholar]
- 7.Fernando TJ, Nguyen DD, Baraff LJ. Effect of electronically delivered prescriptions on compliance and pharmacy wait time among emergency department patients. Acad Emerg Med. 2012;19(1):102–105. doi: 10.1111/j.1553-2712.2011.01249.x. doi: 10.1111/j.1553-2712.2011.01249.x. [DOI] [PubMed] [Google Scholar]
- 8.Pierce R, Rogers E, Sharp M, Musulin M. Outpatient pharmacy redesign to improve work flow, waiting time, and patient satisfaction. Am J Hosp Pharm. 1990;47(2):351–356. [PubMed] [Google Scholar]
- 9.Othman MI, Huzaifah A, Zaini N, Nordini W, Ismail HW, Sulaiman S, Razali WN, Isa H. Comparison of Patients’ Waiting Time between SMS (Short Message Service) and Conventional Methods in an Out-patient Pharmacy. ASEAN Conference on Scientific and Social Science Research 2011; Penang, Malaysia, 22 - 23 June: 2011. [Google Scholar]
- 10.Lin YF, Lin YM, Sheng LH, Chien HY, Chang TJ, Zheng CM, Lu HP. First drive-through pharmacy services in Taiwan. J Chin Med Assoc. 2013;76(1):37–41. doi: 10.1016/j.jcma.2012.10.001. doi: 10.1016/j.jcma.2012.10.001. [DOI] [PubMed] [Google Scholar]
- 11.Tan CLH, Hassali MA, Saleem F, Shafie AA, Aljadhay H, Gan VB. Building intentions with the theory of planned behaviour: a qualitative assessment of salient beliefs about pharmacy value added services in Malaysia. Health Expect. 2016;19(6):1215–1225. doi: 10.1111/hex.12416. doi: 10.1111/hex.12416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Tan CL, Hassali MA, Saleem F, Shafie AA, Aljadhey H, Gan VB. Development, test-retest reliability and validity of the Pharmacy Value-Added Services Questionnaire (PVASQ) Pharm Pract (Granada) 2015;13(3):598. doi: 10.18549/PharmPract.2015.03.598. doi: 10.18549/PharmPract.2015.03.598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Chou YC, Chen BY, Tang YY, Qiu ZJ, Wu MF, Wang SC, Lin HS, Chuang WC. Prescription-filling process reengineering of an outpatient pharmacy. J Med Syst. 2012;36(2):893–902. doi: 10.1007/s10916-010-9553-5. doi: 10.1007/s10916-010-9553-5. [DOI] [PubMed] [Google Scholar]
- 14.Shaat M. Improving pharmacy dispensing performance through time management. [Masters thesis] Royal College of Surgeons in Ireland. 2011 [Google Scholar]