

Abstract
A warming climate is anticipated to increase the future heat-related total mortality in urban areas. However, little evidence has been reported for cause-specific mortality or nonurban areas. Here we assessed the impact of climate change on heat-related total and cause-specific mortality in both urban and rural counties of Jiangsu Province, China in the next five decades. To address the potential uncertainty in projecting future heat-related mortality, we applied localized urban- and nonurban-specific exposure response functions, six population projections including a no population change scenario and five Shared Socioeconomic Pathways (SSPs), and 42 temperature projections from 21 global climate models and two Representative Concentration Pathways (RCPs). Results showed that projected warmer temperatures in 2016–2040 and 2041–2065 will lead to higher heat-related mortality for total non-accidental, cardiovascular, respiratory, stroke, ischemic heart disease (IHD), and chronic obstructive pulmonary disease (COPD) causes occurring annually during May to September in Jiangsu Province, China. Nonurban residents in Jiangsu will suffer from more excess heat-related cause-specific mortality in 2016–2065 than urban residents. Variations across climate models and RCPs dominated the uncertainty of heat-related mortality estimation whereas population size change only had limited influence. Our findings suggest that targeted climate change mitigation and adaptation measures should be taken in both urban and nonurban areas of Jiangsu Province. Specific public health interventions should be focused on the leading causes of death (stroke, IHD, and COPD), whose health burden will be amplified by a warming climate.
Keywords: Heat, Mortality, Projection, Climate change
Graphical abstract

1. Introduction
Heat exposure has been associated with increases in both total non-accidental mortality and cause-specific mortality from cardiovascular and respiratory diseases (Basu, 2009; Bobb et al., 2014; Curriero et al., 2002; Hajat and Kosatky, 2010; Yang et al., 2013). A warming climate is projected to increase future heat-related total non-accidental mortality across developed countries (Ballester et al., 2011; Guo et al., 2016; Huang et al., 2011; Kingsley et al., 2016; Li et al., 2013; Petkova et al., 2013; Vardoulakis et al., 2014). However, few studies have estimated the impact of climate change on heat-related specific causes of death, such as cardiovascular mortality and respiratory mortality (Li et al., 2015). Anticipating changes in future cause-specific mortality is crucial to understanding and reducing future population vulnerability to climate change. In addition, many of these studies have focused on urban areas due to the urban heat island effect and high density of susceptible population (Huang et al., 2011; Li et al., 2013). However, there is emerging evidence supporting high risk of heat-related health impacts in nonurban areas (Bennett et al., 2014; Chen et al., 2016; Madrigano et al., 2015; Sarofim et al., 2016; Sheridan and Dolney, 2003). Less is known about how total and cause-specific mortality will change in response to changes in projected heat exposure in nonurban areas. Moreover, limited studies have specifically assessed climate change impacts on heat-related mortality in developing countries such as China where socioeconomic and demographic conditions differ from those in developed counties. To date in China, only limited evidence of climate change impacts on heat-related mortality were found in Beijing, China, leading to considerable uncertainty as to whether the single city result can be applied to larger regions of China (Li et al., 2015).
Projecting heat-related mortality under a changing climate requires information on the exposure response function (ERF) for temperature-related mortality, projected changes in temperature, baseline rates of cause-specific mortality, and the size of the exposed population (Huang et al., 2011), all of which contribute uncertainties. The choice of ERF contributes a large part of the variations in estimating future temperature-related mortality (Benmarhnia et al., 2014; Wu et al., 2014). As the ERF of heat-related mortality can vary substantially within countries (Bennett et al., 2014; Ma et al., 2015), a region-specific ERF instead of a single ERF covering different regions or countries is critically important in evaluating the impact of climate change on regional heat-related mortality. Another source of uncertainty lies in the projected temperature, based on both scenarios of future ‘forcing’ associated with greenhouse gas concentrations and from climate model response to those greenhouse gas concentrations. The latter varies due to different model formulations, representation of processes and initial states (Flato et al., 2013), so a multi-model ensemble approach is required to address this uncertainty (Li et al., 2013). In addition, population growth would also affect the impact of climate change on heat-related health effects by increasing exposed population, which has not been well considered in many previous studies (Jones et al., 2015).
In this study, we aimed to assess the impact of climate change on heat-related total and cause-specific mortality in both urban and rural counties of Jiangsu Province, China. We applied urban-specific and nonurban-specific ERFs for heat-related total, cardiovascular (including more specific causes of stroke and ischemic heart disease (IHD)), and respiratory (including chronic obstructive pulmonary disease (COPD)) mortality from our previous analysis (Chen et al., 2016) to multiple climate and population projections to estimate the climate change-induced heat-related health burdens in 104 counties of Jiangsu Province, China.
2. Methods
This study was conducted in 104 counties of Jiangsu Province, China with a total population of 78.2 million people in 2010. Jiangsu Province is located along the eastern coast of China and is the most densely populated province in China. Situated in the transition belt from a subtropical to temperate zone, Jiangsu Province has a typical monsoonal climate with an average daily mean temperature of 15.7 °C and four distinct seasons. Jiangsu Province is one of the most developed regions in China and has the second largest Gross Domestic Product (GDP) among Chinese provinces in 2015.
2.1 Temperature projections
Daily maximum and minimum temperatures for the historical period 1980–2005 and the future period 2011–2070 under two Representative Concentration Pathway (RCP) climate scenarios were obtained from the NASA Earth Exchange (NEX) Global Daily Downscaled Projections (GDDP) dataset. The NEX-GDDP dataset includes downscaled daily climate projections at a high spatial resolution of 0.25° × 0.25° from 21 global-scale general circulation models (GCMs) conducted under the Coupled Model Intercomparison Project Phase 5 (CMIP5) (Thrasher et al., 2012). Detailed information about the 21 models can be found in Supplementary Table A1. These GCM runs were developed for the Intergovernmental Panel on Climate Change Fifth Assessment Report (IPCC AR5) (Flato et al., 2013). The NEX-GDDP dataset consists of CMIP5 GCM outputs bias corrected against the Global Meteorological Forcing Dataset (GMFD) (Sheffield et al., 2006), a historical reanalysis dataset based on meteorological station data, using the Bias-Correction Spatial Disaggregation method. This quantile-mapping approach corrects biases between the GCMs and GMFD data over the historical period (1980–2005) for each quantile individually, allowing for non-constant bias across the temperature domain. All 21 CMIP5 GCMs available through NEX under RCP4.5 and RCP8.5 were used in this study, resulting in 42 temperature projections. RCP8.5 is a high-emission business-as-usual scenario in absence of climate mitigation policies, resulting the highest radiative forcing among the total set of RCPs (Riahi et al., 2011). RCP4.5 is a medium-low climate mitigation scenario that stabilizes radiative forcing at 4.5 watts per square meter (W/m2) in the year 2100 without ever exceeding that value (Thomson et al., 2011). Thus, using RCP4.5 and RCP8.5 can provide a range of possible future climate conditions in this study.
The daily temperature projections in the geographic region (116.875°E–121.125°E, 30.875°N–35.125°N) that covers 104 counties of Jiangsu Province (see Supplementary Fig.A1) were selected in this study. Daily average temperature projections were computed as the average of daily minimum temperature and maximum temperature for each grid cell. County-level daily average temperature projections were calculated by taking the area-weighted mean daily average temperature of each grid cell that fell fully or partially within a certain county boundary in Jiangsu Province. The weights that represented the approximate fraction of each cell covered by the county polygon were normalized so that they added up to one. In order to keep consistent with the 25-year baseline period from 1981–2005, two 25-year future periods from 2016–2040 and 2041–2065 were used in this analysis.
2.2 Population projections
To isolate the climate-only effect on heat-related mortality, a no population change scenario was first used in this study by assuming the future population is the same as the baseline population in Jiangsu, China. County-level population data based on the 2010 Population Census of China was used as the baseline population. To account for the future demographic changes, population projections at 0.125° × 0.125° resolution under five shared socioeconomic pathways (SSPs) in Jiangsu Province from 2010 to 2060 were applied (Jones and O’Neill, 2016). The SSPs describe a set of plausible alternative futures of societal development without considering the effects of climate change and new climate policies over the 21st century (O’Neill et al., 2014). In SSP population projections, the assumptions of Chinese population changes are low fertility, low mortality, medium migration, and high education for SSP1; medium fertility, medium mortality, medium migration, and medium education for SSP2; high fertility, high mortality, low migration, and low education for SSP3; high fertility, high mortality, medium migration, and polarized education for SSP4; low fertility, low mortality, high migration, and high education for SSP5 (KC and Lutz, 2014).
County-level population projections were calculated by summing the populations of each grid cell that fell within a certain county boundary in Jiangsu Province. Since SSP population projections were based on the 2000 population, the potential biases between SSP population projections and Census 2010 population were corrected using a scaling factor (Census 2010 population divided by SSP 2010 population projections) for each county.
2.3 Health impact assessment
We computed the attributable daily deaths (ADD) to heat exposure for each county as follows:
| [1] |
where ADD represents the estimated county-level daily heat-related deaths; Yb is the county-level baseline daily mortality rate for cause-specific (total non-accidental, cardiovascular, respiratory, stroke, IHD, and COPD) deaths; Tmean is the county-level daily average temperature projections from 21 GCMs for the baseline period (1981–2005) and the future periods (2016–2040 and 2041–2065); ERF is the daily percentage change in county-level mortality for a given Tmean relative to the 75th percentile (24.13 °C); POP is the county-level population.
The ERF, which represents the heat effect on daily mortality for a given daily Tmean, was defined as follows:
| [2] |
where RR is the cumulative relative risk of Tmean relative to 24.13 °C, which is derived from the pooled results of ERF in 102 counties of Jiangsu Province as described in our previous work (Chen et al., 2016). Briefly, using observation-derived temperatures and cause-specific mortality, a distributed lag non-linear model was first applied to estimate the heat-related mortality risk in each county during 2009 to 2013. All counties were divided into two groups on the basis of urban fraction: urban counties (percentage of urban population ≥ median percentage, i.e., 57.11%) and nonurban counties (percentage of urban population < 57.11%). A Bayesian hierarchical model was then used to pool the county-specific estimates for urban and nonurban counties. As different ERFs were previously found for urban and nonurban counties, we used the urban-specific and nonurban-specific ERFs for each cause of death to estimate the county-level heat-related deaths (see Supplementary Fig.A2). In sensitivity analysis, an overall ERF for all counties was also applied in the health impact assessment.
Total and cause-specific daily baseline mortality rates for all ages and both sex were obtained from the Jiangsu Provincial Center for Disease Prevention and Control. Specifically, daily mortality data during 2009–2013 were used to calculate the baseline daily mortality rates for 99 counties in Jiangsu Province. For another five counties in Jiangsu Province, no complete death certificate data before 2014 was available. Thus, the 2014 daily mortality data was used to compute the baseline daily mortality rates for these remaining five counties. We held the baseline mortality rate during 2009–2014 in Jiangsu Province constant in both the historical period and future periods. To reduce the inter-annual variations and intra-month fluctuations of daily mortality rates on a certain calendar day, we computed the averaged monthly mortality rates for each cause of death during 2009–2014 and then converted the monthly mortality rates evenly to daily rates within a certain month.
For each of the 21 GCMs, we computed the heat-related daily deaths using Equation [1] for each RCP scenario (RCP4.5 and RCP8.5), each period (1981–2005, 2016–2040 and 2041–2065), and each population scenario (no change and SSP1–SSP5). Then we calculated the annual average heat-related deaths during the warm season (May–September) in each period. Finally, the changes in future annual average heat-related deaths during the warm season were calculated as the differences between the baseline period (1981–2005) and the future periods (2016–2040 and 2041–2065).
To explore the sensitivity of heat-related mortality projections to different factors (i.e., 2 RCPs, 21 GCMs, 6 population projections, and 3 ERF coefficients (mean, upper and lower estimates of the 95% CI)), we conducted a variance component analysis using a ANOVA-type estimation to determine the contribution of each factor in the total variance of overall heat-related mortality estimates (Li et al., 2016). We performed the uncertainty analysis for each cause of death and each future period, respectively.
All analyses were conducted in R 2.15.0 (R Foundation for Statistical Computing, Vienna, Austria) and ArcGIS (version 10.0; ESRI, Redlands, CA).
3. Results
Fig.1 (a) shows the multi-model simulated time series of annual warm season (May to September) mean daily average temperature during the historical and future periods. Compared to the historical period 1980–2005, projected ambient temperatures will continually increase in 2016–2070 under both the RCP4.5 and RCP8.5 scenarios. In general, RCP8.5 yielded higher daily average temperatures than RCP4.5; and this difference becomes larger over time. Under RCP4.5, the projected 21-GCMs mean daily average temperature during the warm season increased by 1.1 °C and 2.0 °C in 2016–2040 and 2041–2065, respectively compared with 1981–2005 (see Supplementary Table A2). Larger increases relative to 1981–2005 were observed under RCP8.5, with a 1.3 °C increment in 2016–2040 and 2.7 °C increment in 2041–2065, respectively.
Fig.1.
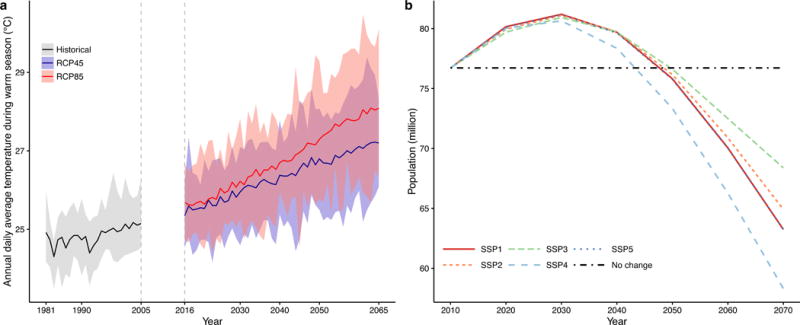
Temperature and population changes in the 104 counties of Jiangsu Province. (a) multi-model simulated time series of annual warm season (May to September) mean daily average temperature during the historical period (1981–02005) and future periods (2016–2065). Time series of mean projections and a measure of uncertainty (shading, minimum-maximum range from 21 CMIP5 GCMs) are shown for RCP4.5 (blue) and RCP8.5 (red). Black (grey shading) is the modelled historical daily average temperature. See Supplementary Table A1 for summary information on each model. (b) The total population projections during 2010–2070 under six population scenarios (No change and SSP1-SSP5).
Under the SSPs, population size in the 104 counties of Jiangsu Province will first increase from 2010 to 2030, then decrease from 2030 to 2070 (Fig.1 (b)). The trajectories of five SSPs stay close to each other until around 2030. Visible differentiation occurs among SSPs after 2050 with the highest population in SSP3 and the lowest in SSP4. Compared with the no population change scenario (76.7 million), population sizes are generally larger from 2010 to 2040 under SSPs with SSP3 reaching 81.2 million in 2030. After 2050, SSPs projected population sizes are smaller than the no population change scenario, with SSP4 reaching 58.3 million in 2070.
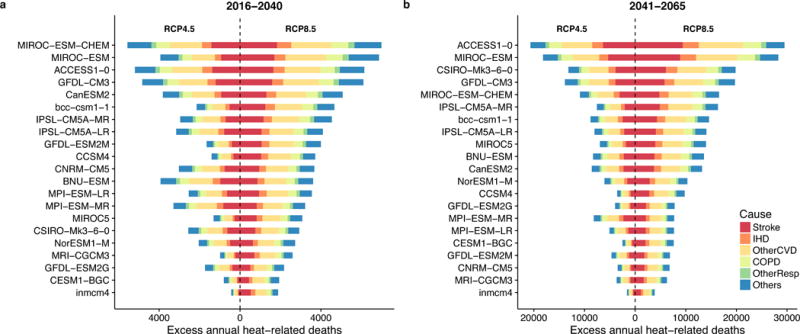
Future changes in projected temperature under both RCP scenarios will cause stroke, IHD, other cardiovascular diseases (OtherCVD), COPD, other respiratory diseases (OtherResp), and other non-accidental (Others) deaths to increase in 2016–2040 and 2041–2065 relative to 1981–2005 in Jiangsu Province under a no population change assumption (Fig.2). The projected excess (future period – baseline period) heat-related deaths varied greatly among the 21 GCMs. From 1981–2005 to 2041–2065, the highest estimates of excess heat-related total deaths were from the ACCESS1–0 model, which were one order of magnitude bigger than the lowest estimates from the INMCM4 model. The variation of excess heat-related mortality across the 21 GCMs increases over time, as its range in 2041–2065 is much larger than that in 2016–2040.
Fig.2.

Changes in heat-related cause-specific deaths occurring annually between May and September in 2016–2040 and 2041–2065 versus 1981–2005 for 21 models under the RCP4.5 and RCP8.5 climate scenarios with a no population change assumption in Jiangsu Province, China. Cause-specific deaths include deaths due to stroke, ischemic heart disease (IHD), other cardiovascular disease (OtherCVD), chronic obstructive pulmonary disease (COPD), other respiratory disease (OtherResp), and other causes of non-accidental disease (Others). Urban- and nonurban-specific ERFs for each cause of death were used in the calculation.
Under RCP4.5, the Jiangsu population in 2010 would have 2730 (95%CI: 2591–2871) and 7992 (95%CI: 7542–8454) excess heat-related total deaths annually between May and September if experiencing the multi-model mean projected temperatures in 2016–2040 and 2041–2065 (Table 1). Likewise, there would be 1713 (95%CI: 1612–1817) and 5314 (95%CI: 4958–5686) excess heat-related cardiovascular deaths, 452 (95%CI: 411–494) and 1286 (95%CI: 1167–1411) excess heat-related respiratory deaths, 667 (95%CI: 641–694) and 2217 (95%CI: 2105–2334) excess heat-related stroke deaths, 237 (95%CI: 176–300) and 787 (95%CI: 653–927) excess heat-related IHD deaths, and 323 (95%CI: 287–361) and 964 (95%CI: 859–1073) excess heat-related COPD deaths in 2016–2040 and 2041–2065, respectively. More excess heat-related cause-specific deaths are projected under RCP8.5 than RCP4.5, as presented in Table 1.
Table 1.
Changes in 21-GCM-averaged heat-related cause-specific deaths occurring annually between May and September if the Jiangsu 2010 population in urban and nonurban counties were exposed to the daily average temperatures in 2016–2040 and 2041–2065 under the RCP4.5 and RCP8.5 climate scenarios compared to those in 1981–2005 (Mean and 95% confidence intervalsa).
| RCP Scenario | Cause of Death | 2016–2040 | 2041–2065 | ||||
|---|---|---|---|---|---|---|---|
|
| |||||||
| All | Urban | Nonurban | All | Urban | Nonurban | ||
| RCP4.5 | Total | 2730 (2591–2871) | 823 (765–882) | 1907 (1826–1989) | 7992 (7542–8454) | 2055 (1942–2169) | 5937 (5599–6285) |
| Cardiovascular | 1713 (1612–1817) | 449 (411–487) | 1264 (1201–1330) | 5314 (4958–5686) | 1186 (1104–1269) | 4128 (3854–4416) | |
| Respiratory | 452 (411–494) | 146 (128–165) | 306 (283–329) | 1286 (1167–1411) | 355 (314–398) | 931 (853–1013) | |
| Stroke | 667 (641–694) | 151 (134–167) | 516 (506–527) | 2217 (2105–2334) | 426 (390–463) | 1791 (1715–1872) | |
| IHD | 237 (176–300) | 52 (39–66) | 185 (138–234) | 787 (653–927) | 137 (106–170) | 649 (547–757) | |
| COPD | 323 (287–361) | 84 (71–98) | 239 (216–263) | 964 (859–1073) | 217 (188–247) | 747 (671–827) | |
| RCP8.5 | Total | 3982 (3776–4191) | 1107(1036–1180) | 2874 (2740–3011) | 13069 (12265–13899) | 3160 (3004–3318) | 9910 (9261–10582) |
| Cardiovascular | 2568 (2413–2728) | 618 (570–667) | 1949 (1843–2060) | 8951 (8286–9652) | 1876 (1753–2000) | 7076 (6533–7652) | |
| Respiratory | 648 (591–708) | 194 (171–218) | 454 (420–490) | 2082 (1874–2303) | 539 (476–605) | 1543 (1398–1698) | |
| Stroke | 1031 (988–1076) | 213 (192–235) | 818 (796–841) | 3821 (3593–4061) | 692 (639–746) | 3129 (2954–3315) | |
| IHD | 372 (293–455) | 73 (55–91) | 300 (238–364) | 1362 (1165–1569) | 216 (170–265) | 1145 (995–1303) | |
| COPD | 473 (421–526) | 114 (97–131) | 359 (325–395) | 1586 (1406–1777) | 339 (297–383) | 1246 (1109–1393) | |
The 95% confidence intervals were derived from the estimates of heat-mortality ERFs in (Chen et al., 2016).
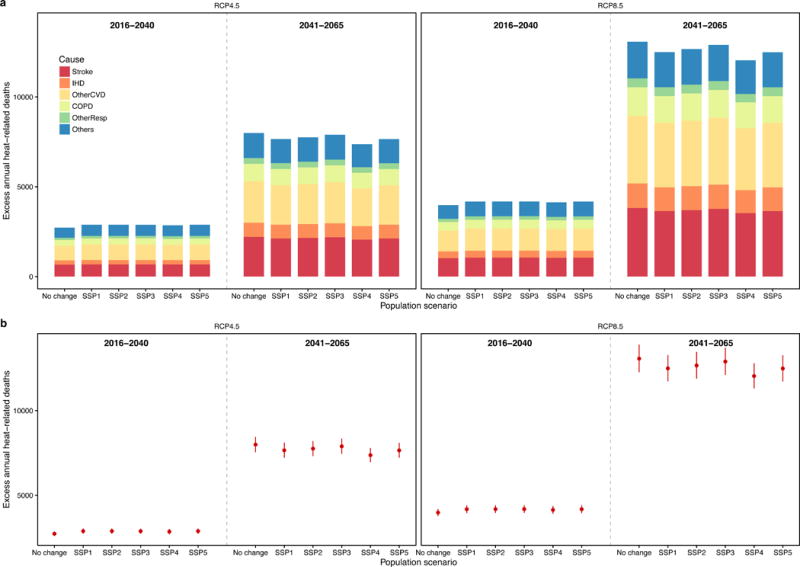
Fig.3 summarizes the changes in heat-related cause-specific deaths under the six different population growth scenarios in Jiangsu Province. In general, for both RCP emission scenarios, compared to the historical period 1981–2005, all five SSPs generate slightly more excess heat-related deaths than the no population change scenario in 2016–2040 and less excess heat-related deaths in 2041–2065. Among all population projections under SSPs, the SSP3 scenario generally leads to the highest heat-related deaths, whereas the SSP4 scenario results in the lowest estimates. Though population will likely decrease in 2041–2065 (Fig.1b), due to higher temperatures, the estimated excess heat-related deaths would still be much higher than those in 2016–2040 for all five SSPs. For all population scenarios, cardiovascular deaths (Stroke + IHD + OtherCVD) account for more than 60% of heat-related total deaths (Fig.3a). Variations of heat-related total deaths among different population scenarios are generally within the range of 95%CI induced by ERFs (Fig.3b), which is also observed for other cause-specific deaths (see Supplementary Fig.A3).
Fig.3.
Multi-model mean changes in heat-related cause-specific (a) and total (b) deaths occurring annually between May and September in 2016–2040 and 2041–2065 versus 1981–2005 for 21 GCMs under the RCP4.5 and RCP8.5 climate scenarios with six population scenarios (2010 population and SSP1 –SSP5 projected populations) in Jiangsu Province, China. Cause-specific deaths include deaths due to stroke, ischemic heart disease (IHD), other cardiovascular disease (OtherCVD), chronic obstructive pulmonary disease (COPD), other respiratory disease (OtherResp), and other causes of non-accidental disease (Others). Vertical lines in (b) show uncertainty of estimates from the 95% CI of ERFs for total non-accidental death.
We applied the urban- and rural-specific ERFs (see Supplementary Fig.A2) to estimate the changes in heat-related deaths in the future periods compared with the historical period. Nonurban counties generally have higher heat effects for temperature > 24.13 °C on daily total non-accidental, cardiovascular, respiratory, stroke, IHD, and COPD mortality than urban counties (see Supplementary Fig.A2). If an overall ERF was used for all urban and nonurban counties in the health impact assessment, the excess heat-related total deaths would be overestimated for urban counties and underestimated for nonurban counties (Fig.4). On average, excess heat-related total deaths in urban counties would be overestimated by 12.3% under RCP4.5 and 15.4% under RCP8.5 during 2016–2040, and 20.6% under RCP4.5 and 24.5% under RCP8.5 during 2041–2065, respectively. On the contrary, average excess heat-related total deaths in nonurban counties would be underestimated by 17.3% under RCP4.5 and 18.9% under RCP8.5 during 2016–2040, and 20.6% under RCP4.5 and 21.8% under RCP8.5, respectively. Estimates from the other five specific causes of heat-related deaths led to similar validation results that argue for using both urban- and nonurban-specific ERFs (as opposed to a single ERF; results not shown).
Fig.4.
Relationships between estimated multi-model mean changes in heat-related total non-accidental deaths occurring annually between May and September in 2016–2040 and 2041–2065 versus 1981–2005 for 21 GCMs using the overall exposure response function (ERF) and those using the urban-specific and nonurban-specific ERFs for the 2010 population and the RCP4.5 and RCP8.5 climate scenarios in Jiangsu Province, China. The blue and red lines with grey shadings are the linear regression lines and the 95% confidence regions for urban and nonurban counties, respectively. The black line is the 1:1 line.
Using the urban- and nonurban-specific ERFs, the uncertainty attributable to ERFs were generally quite small (<5%) except for the heat-related IHD deaths in 2016–2040 (17%) (see Supplementary Fig.A4). In the future five decades, the choice of climate models contributed the most uncertainty in estimating heat-related mortality (62–70%), followed by RCPs (about 25%). Population size had limited influence on the uncertainty of heat-related mortality estimation (<1%).
The future warming impacts on mortality varied substantially across the 104 counties in Jiangsu Province (see Supplementary Fig.A5). Compared with southern counties, increases in heat-related total mortality relative to the 1981–2005 are much larger in middle and northern counties, most of which are nonurban areas. Under RCP8.5 with a no population change assumption, 89.5% of counties with more than 150 excess heat-related total deaths in 2041–2065 were located in nonurban areas (34/38 counties). Under RCP4.5 with a no population change assumption, all 12 counties with more than 150 excess heat-related deaths in 2041–2065 were located in nonurban areas.
4. Discussion
Under both RCP scenarios, projected warmer temperatures in the 2016–2040 and 2041–2065 periods will lead to higher heat-related mortality for total non-accidental, cardiovascular, respiratory, stroke, IHD, and COPD causes occurring annually during May to September in Jiangsu Province, China. Nonurban residents in Jiangsu will suffer from more excess heat-related cause-specific mortality in 2016–2065 than urban residents. Climate models and scenarios dominate the estimation uncertainty of future heat-related mortality while population size contributes only quite limited uncertainty.
Our findings of increasing future heat-related mortality are broadly consistent with previous assessments (Guo et al., 2016; Kingsley et al., 2016; Li et al., 2015; Petkova et al., 2013; Schwartz et al., 2015; Vardoulakis et al., 2014), though direct comparison of the effect estimates is difficult as different climate models, scenarios, downscaling methods, time periods, ERFs, and population growth scenarios were used in those previous studies. To allow a rough comparison between this study and previous studies, we computed the future changes in heat-related deaths per 100,000 people under the no population change scenario. We found that in Jiangsu Province, the mean increases in heat-related total mortality occurring annually during May to September relative to 1981–2005 was 3.5 per 100,000 people in 2016–2040 and 10.2 per 100,000 people in 2041–2065 under RCP4.5, and 5.1 per 100,000 people in 2016–2040 and 16.6 per 100,000 people in 2041–2065 under RCP8.5, respectively. Similarly, a recent study using the GFDL-CM3 model showed that increases in heat-related deaths during April to September relative to 1976–2005 were 6.2 per 100,000 people in 2016–2045 and 8.1 per 100,000 people in 2036–2065 under RCP6.0 scenario in 209 U.S. cities (Schwartz et al., 2015). Under the RCP4.5 and RCP8.5 scenarios, similar increments in heat-related all-cause deaths per 100,000 people relative to 1971–2000 were also found in New York City (5.4 and 6.3 in 2010–2039, and 10.6 and 15.2 in 2040–2069), Philadelphia (3.5 and 4.3 in 2010–2039, and 7.7 and 11.5 in 2040–2069), and Boston (3.0 and 3.6 in 2010–2039, 5.9 and 8.8 in 2040–2069) (Petkova et al., 2013). Using daily maximum temperature as the exposure metric, projected increases in annual heat-related all-cause mortality per 100,000 people during the warm months (April to October) in 2046–2053 relative to 2005–2012 in Rhode Island, U.S. were 2.7 under RCP4.5 and 3.6 and under RCP8.5, respectively (Kingsley et al., 2016), which is comparable with our estimates.
For cause-specific mortality, far few studies have assessed the impacts of climate change on heat-related cause-specific mortality (Li et al., 2015). The mean increase in annual cardiovascular mortality during May to September relative to 1981–2005 in Jiangsu Province was 2.2 per 100,000 in 2016–2040 and 6.8 per 100,000 in 2041–2065 under RCP4.5, and 3.3 per 100,000 in 2016–2040 and 11.4 per 100,000 in 2041–2065 under RCP8.5, respectively. In accordance with our findings, projected median increases in annual heat-related cardiovascular mortality relative to 1971–2000 in Beijing were 4.2 per 100,000 in 2010–2039 and 5.8 per 100,000 in 2040–2069 under RCP4.5, and 4.0 per 100,000 in the 2010–2039 and 6.5 per 100,000 in the 2040–2069 under RCP8.5, respectively (Li et al., 2015).
We found that nonurban counties will experience higher excess heat-related mortality in the future five decades than urban counties in Jiangsu Province. To the best of our knowledge, this is the first study to quantify the impact of climate change on heat-related mortality in nonurban areas using multi-model climate models and RCP scenarios. A recent study also found comparable cardiorespiratory deaths in rural and urban areas of England and Wales by assuming temperature increased by 2°C instead of using climate model projections (Bennett et al., 2014). Previous projection studies only focused on urban areas because urban residents were generally assumed to be more vulnerable due to the high density of susceptible people and the higher temperatures associated with the urban heat island effect (Guo et al., 2016; Li et al., 2013). Though evidence on significant heat-related health impacts in rural areas is emerging, these studies are often hindered by quantitative challenges due to low population density and dispersed weather stations in rural areas (Sarofim et al., 2016). This study benefits from our previous attempt to use fine-scale interpolated temperatures to quantify the mortality effect of heat exposure in both urban and rural residents of Jiangsu Province, where more residents are in nonurban areas than in urban areas (Chen et al., 2016). In our previous study, nonurban areas in Jiangsu Province were found to have significant heat-related mortality risks due to their high heat-related vulnerability (Chen et al., 2016). Nonurban areas in Jiangsu Province generally had higher percentages of older people, higher percentages of people with lower education level, lower prevalence of air conditioning, and insufficiency of hospital infrastructure, which were all associated with increased heat-related mortality risks. Using an overall ERF instead of urban- and nonurban-specific ERFs results in an overestimation of 12.3%–24.5% excess heat-related total deaths in urban areas and an underestimation of 17.3%–21.8% excess heat-related total deaths in nonurban areas (Fig.4). This implies that further studies assessing the impact of climate change on heat-related health effects in rural areas should apply a rural-specific ERF, rather than using ERF from urban areas. Nonurban counties were found to have higher heat-related mortality risks and more daily death counts than urban counties in Jiangsu Province (Chen et al., 2016), which contributes to the higher estimates of nonurban excess heat-related deaths in Jiangsu Province. The high projected heat-related mortality burden in nonurban areas of Jiangsu indicates that effective adaptive measures should be taken in nonurban areas, which throughout the world have received less attention than urban areas in heat mitigation efforts, to reduce the potential adverse health impacts attributable to warming temperatures.
In Jiangsu Province with a no population change assumption, more than half of the excess heat-related total deaths were derived from cardiovascular mortality (Table 1 and Fig.3). The larger increment in cardiovascular mortality than that in respiratory mortality was also observed in a previous study in Beijing, China (Li et al., 2015). This is mainly due to the high percentage of baseline cardiovascular mortality, which contributes to about 44.6% of total non-accidental deaths in China in 2013 (Zhou et al., 2016). Stroke, IHD, and COPD are the three most common non-communicable diseases in China in 2013, accounting for about 23.0%, 16.7%, and 10.9% of total non-accidental deaths (Zhou et al., 2016). In the future five decades (2016–2065), these three causes will contribute about 48.5% and 50.7% of the heat-related total deaths under RCP4.5 and RCP8.5, respectively (Table 1). Thus, future interventions to reduce the burden of these three leading causes should also include measures to reduce heat-related vulnerability.
Projecting heat-related mortality under a changing climate inherently involves large uncertainties related to baseline ERF, baseline mortality rate, climate models, and population changes (Huang et al., 2011). Several of these uncertainties were addressed in this study by utilizing a localized ERF for Jiangsu residents, 21 climate models, and six population size growth scenarios. Uncertainty from climate models dominated the estimation of future heat-related mortality with an increasing trend from 2016–2040 to 2041–2065 (Fig.2 and Fig.A4). Our findings indicate that the choice of climate models reflects the greatest source of uncertainty in heat-related mortality projections in Jiangsu Province, China. This might be because GCMs’ intra-annual variance, in conjunction with the magnitude of summer-mean warming (see Supplementary Table A2), could generate order of magnitude differences in heat-related mortality changes, due to the nonlinear ERF at high temperatures tails (see Supplementary Fig.A2). Future research could look into the relative role of projected temperature variance changes compared with mean changes in driving heat-related mortality increase. Improved and more robust projections of future climate will enhance the health impact assessment of heat exposure under climate change. The contribution of population size growth to future changes in heat-related mortality is relatively small in Jiangsu (see Supplementary Fig.A4). Compared with a no population change assumption and for a given amount of warming, projected future population size will cause heat-related cause-specific mortality to slightly increase in 2016–2040 and to slightly decrease in 2041–2065. For example, compared with using the 2010 population, using SSP3 projected population yielded 5.1% higher estimates in 2016–2040 and 1.3% lower estimates in 2041–2065 under RCP8.5 (Fig.3). On the contrary, considering both population size growth and population ageing in the demographic changes could result in substantial increases in future heat-related mortality (Lee and Kim, 2016; Vardoulakis et al., 2014; Voorhees et al., 2011), as elderly people are more vulnerable to heat-related mortality (Bell et al., 2008; Benmarhnia et al., 2015; Hajat et al., 2007). Therefore, the no population change scenario and SSP population size growth scenarios used in this study provide conservative projections of possible future heat-related mortality due to climate change (Knowlton et al., 2007).
Our study has several limitations. First, our projections of heat-related mortality under climate change did not account for population acclimatization to heat stress. Recent studies comparing the temperature optimum (i.e., the temperature with minimum mortality) in different countries revealed that populations could adapt to their local climates to some extent (Guo et al., 2014; Todd and Valleron, 2015). People may adapt to heat stress through modifications in activities, increased use of air conditioning, and alternative building designs (Kinney et al., 2008). Projecting future mortality effects of climate change on heat exposure without consideration of heat adaptation may lead to substantial overestimates (Petkova et al., 2014). Second, we did not consider changes in demographic structure such as population ageing, which may lead to underestimation of heat-related mortality due to climate change (Lee and Kim, 2016). Population ageing may amplify future heat-related health burdens by increasing the proportion of vulnerable elderly population (Huang et al., 2011; Li et al., 2016; Vardoulakis et al., 2014). Third, the county-level baseline cause-specific mortality rates were held constant in the health impact assessment as no such projection data are available in Jiangsu Province. Fourth, the findings of this study were derived from only one province of China, which may not be applicable to other regions with different climates and socio-economic statuses in China. Finally, the total warming, as well as the magnitude, intensity, and duration of heat events specifically could change in ways not captured by the GCMs and RCPs (Horton et al., 2016).
Strengths of our study include the use of downscaled daily climate projections from 21 climate models under two RCP scenarios for the projection of heat-related mortality. Additionally, differences in heat-related mortality projections between urban and nonurban areas were addressed by applying urban- and nonurban-specific ERF in the health impact assessment. Furthermore, non-linear cause-specific ERFs were used to model the health impacts associated with future heat exposure, allowing for more flexible temperature-mortality relationships than linear ERFs.
5. Conclusion
In summary, we found that warming temperatures projected for 2016–2040 and 2041–2065 could lead to higher heat-related mortality in Jiangsu Province, China. Nonurban residents will suffer from more heat-related death burden than urban residents in the future five decades. The results argue for targeted climate change mitigation and adaptation measures tailored to both urban and nonurban areas of Jiangsu Province. Specific public health interventions could be focused on the leading causes of death, whose health burden will be amplified by a warming climate.
Supplementary Material
Capsule.
A warming climate in the next five decades will lead to increased burden of heat-related total and cause-specific mortality in Jiangsu, China, especially in nonurban areas.
Highlights.
A warming climate will amplify heat-related cause-specific mortality in Jiangsu.
Nonurban residents are more vulnerable to climate change than urban residents.
Climate models contribute the largest uncertainty in health impact assessment.
Acknowledgments
This work was supported by the China National Natural Science Foundation (grant number: 71433007), the China National Key Research & Development Program (grant number: 2016YFC0207600), the US National Institute of Environmental Health Sciences (grant numbers: ES009089 and T32ES023770), the Shanghai Tongji Gao Tingyao Environmental Science & Technology Development Foundation (STGEF). Climate scenarios used were from the NEX-GDDP dataset, prepared by the Climate Analytics Group and NASA Ames Research Center using the NASA Earth Exchange and distributed by the NASA Center for Climate Simulation (NCCS). We acknowledge the World Climate Research Program’s Working Group on Coupled Modeling, which is responsible for CMIP, and we thank the climate modeling groups for producing and making available their model output.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflict of interest: The authors declare that they have no conflict of interest.
References
- Ballester J, Robine JM, Herrmann FR, Rodo X. Long-term projections and acclimatization scenarios of temperature-related mortality in Europe. Nat Commun. 2011;2:358. doi: 10.1038/ncomms1360. [DOI] [PubMed] [Google Scholar]
- Basu R. High ambient temperature and mortality: a review of epidemiologic studies from 2001 to 2008. Environ Health. 2009;8:40. doi: 10.1186/1476-069X-8-40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bell ML, O’Neill MS, Ranjit N, Borja-Aburto VH, Cifuentes LA, Gouveia NC. Vulnerability to heat-related mortality in Latin America: a case-crossover study in Sao Paulo, Brazil, Santiago, Chile and Mexico City, Mexico. Int J Epidemiol. 2008;37:796–804. doi: 10.1093/ije/dyn094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Benmarhnia T, Deguen S, Kaufman JS, Smargiassi A. Vulnerability to heat-related mortality: a systematic review, meta-analysis, and meta-regression analysis. Epidemiology. 2015;26:781–793. doi: 10.1097/EDE.0000000000000375. [DOI] [PubMed] [Google Scholar]
- Benmarhnia T, Sottile MF, Plante C, Brand A, Casati B, Fournier M, Smargiassi A. Variability in temperature-related mortality projections under climate change. Environ Health Perspect. 2014;122:1293–1298. doi: 10.1289/ehp.1306954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bennett JE, Blangiardo M, Fecht D, Elliott P, Ezzati M. Vulnerability to the mortality effects of warm temperature in the districts of England and Wales. Nat Clim Chang. 2014;4:269–273. [Google Scholar]
- Bobb JF, Peng RD, Bell ML, Dominici F. Heat-related mortality and adaptation to heat in the United States. Environ Health Perspect. 2014;122:811–816. doi: 10.1289/ehp.1307392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen K, Zhou L, Chen X, Ma Z, Liu Y, Huang L, Bi J, Kinney P. Urbanization level and vulnerability to heat-related mortality in Jiangsu Province, China. Environ Health Perspect. 2016 doi: 10.1289/EHP204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Curriero FC, Heiner KS, Samet JM, Zeger SL, Strug L, Patz JA. Temperature and mortality in 11 cities of the eastern United States. Am J Epidemiol. 2002;155:80–87. doi: 10.1093/aje/155.1.80. [DOI] [PubMed] [Google Scholar]
- Flato G, Marotzke J, Abiodun B, Braconnot P, Chou SC, Collins W, Cox P, Driouech F, Emori S, Eyring V, Forest C, Gleckler P, Guilyardi E, Jakob C, Kattsov V, Reason C, Rummukainen M. Evaluation of Climate Models. In: Stocker TF, Qin D, Plattner G-K, Tignor M, Allen SK, Boschung J, Nauels A, Xia Y, Bex V, Midgley PM, editors. Climate Change 2013: The Physical Science Basis Contribution of Working Group I to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change. Cambridge University Press; Cambridge, United Kingdom and New York, NY, USA: 2013. pp. 741–866. [Google Scholar]
- Guo Y, Gasparrini A, Armstrong B, Li S, Tawatsupa B, Tobias A, Lavigne E, de Sousa Zanotti Stagliorio Coelho M, Leone M, Pan X, Tong S, Tian L, Kim H, Hashizume M, Honda Y, Guo YLL, Wu CF, Punnasiri K, Yi SM, Michelozzi P, Saldiva PHN, Williams G. Global variation in the effects of ambient temperature on mortality: A systematic evaluation. Epidemiology. 2014;25:781–789. doi: 10.1097/EDE.0000000000000165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guo Y, Li S, Liu DL, Chen D, Williams G, Tong S. Projecting future temperature-related mortality in three largest Australian cities. Environ Pollut. 2016;208(Part A):66–73. doi: 10.1016/j.envpol.2015.09.041. [DOI] [PubMed] [Google Scholar]
- Hajat S, Kosatky T. Heat-related mortality: a review and exploration of heterogeneity. J Epidemiol Community Health. 2010;64:753–760. doi: 10.1136/jech.2009.087999. [DOI] [PubMed] [Google Scholar]
- Hajat S, Kovats RS, Lachowycz K. Heat-related and cold-related deaths in England and Wales: who is at risk? Occup Environ Med. 2007;64:93–100. doi: 10.1136/oem.2006.029017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Horton RM, Mankin JS, Lesk C, Coffel E, Raymond C. A review of recent advances in research on extreme heat events. Curr Clim Change Rep. 2016:1–18. [Google Scholar]
- Huang C, Barnett AG, Wang X, Vaneckova P, FitzGerald G, Tong S. Projecting future heat-related mortality under climate change scenarios: a systematic review. Environ Health Perspect. 2011;119:1681–1690. doi: 10.1289/ehp.1103456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones B, O’Neill BC. Spatially explicit global population scenarios consistent with the Shared Socioeconomic Pathways. Environmental Research Letters. 2016;11:084003. [Google Scholar]
- Jones B, Oneill BC, McDaniel L, McGinnis S, Mearns LO, Tebaldi C. Future population exposure to US heat extremes. Nat Clim Chang. 2015;5:652–655. [Google Scholar]
- KC S, Lutz W. The human core of the shared socioeconomic pathways: Population scenarios by age, sex and level of education for all countries to 2100. Glob Environ Change. 2014 doi: 10.1016/j.gloenvcha.2014.06.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kingsley SL, Eliot MN, Gold J, Vanderslice RR, Wellenius GA. Current and projected heat-related morbidity and mortality in Rhode Island. Environ Health Perspect. 2016;124:460–467. doi: 10.1289/ehp.1408826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kinney PL, O’Neill MS, Bell ML, Schwartz J. Approaches for estimating effects of climate change on heat-related deaths: challenges and opportunities. Environ Sci Policy. 2008;11:87–96. [Google Scholar]
- Knowlton K, Lynn B, Goldberg RA, Rosenzweig C, Hogrefe C, Rosenthal JK, Kinney PL. Projecting heat-related mortality impacts under a changing climate in the New York City region. American Journal of Public Health. 2007;97:2028–2034. doi: 10.2105/AJPH.2006.102947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee JY, Kim H. Projection of future temperature-related mortality due to climate and demographic changes. Environment International. 2016 doi: 10.1016/j.envint.2016.06.007. [DOI] [PubMed] [Google Scholar]
- Li T, Ban J, Horton RM, Bader DA, Huang G, Sun Q, Kinney PL. Heat-related mortality projections for cardiovascular and respiratory disease under the changing climate in Beijing, China. Sci Rep. 2015;5 doi: 10.1038/srep11441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li T, Horton RM, Bader DA, Zhou M, Liang X, Ban J, Sun Q, Kinney PL. Aging will amplify the heat-related mortality risk under a changing climate: Projection for the elderly in Beijing, China. Sci Rep. 2016;6:28161. doi: 10.1038/srep28161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li T, Horton RM, Kinney PL. Projections of seasonal patterns in temperature-related deaths for Manhattan, New York. Nat Clim Chang. 2013;3:717–721. doi: 10.1038/nclimate1902. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ma W, Wang L, Lin H, Liu T, Zhang Y, Rutherford S, Luo Y, Zeng W, Zhang Y, Wang X, Gu X, Chu C, Xiao J, Zhou M. The temperature–mortality relationship in China: An analysis from 66 Chinese communities. Environ Res. 2015;137:72–77. doi: 10.1016/j.envres.2014.11.016. [DOI] [PubMed] [Google Scholar]
- Madrigano J, Jack D, Anderson GB, Bell ML, Kinney PL. Temperature, ozone, and mortality in urban and non-urban counties in the northeastern United States. Environ Health. 2015;14:3. doi: 10.1186/1476-069X-14-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- O’Neill BC, Kriegler E, Riahi K, Ebi KL, Hallegatte S, Carter TR, Mathur R, van Vuuren DP. A new scenario framework for climate change research: the concept of shared socioeconomic pathways. Clim Change. 2014;122:387–400. [Google Scholar]
- Petkova EP, Gasparrini A, Kinney PL. Heat and mortality in New York City since the beginning of the 20th century. Epidemiology. 2014;25:554–560. doi: 10.1097/EDE.0000000000000123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Petkova EP, Horton RM, Bader DA, Kinney PL. Projected heat-related mortality in the US urban northeast. Int J Environ Res Public Health. 2013;10:6734–6747. doi: 10.3390/ijerph10126734. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Riahi K, Rao S, Krey V, Cho C, Chirkov V, Fischer G, Kindermann G, Nakicenovic N, Rafaj P. RCP 8.5—A scenario of comparatively high greenhouse gas emissions. Clim Change. 2011;109:33–57. [Google Scholar]
- Sarofim MC, Saha S, Hawkins MD, Mills DM, Hess J, Horton R, Kinney P, Schwartz J, St Juliana AA. Ch 2: Temperature-Related Death and Illness, The Impacts of Climate Change on Human Health in the United States: A Scientific Assessment. U.S. Global Change Research Program; Washington, DC: 2016. pp. 43–68. [Google Scholar]
- Schwartz JD, Lee M, Kinney PL, Yang S, Mills D, Sarofim MC, Jones R, Streeter R, Juliana AS, Peers J. Projections of temperature-attributable premature deaths in 209 US cities using a cluster-based Poisson approach. Environmental Health. 2015;14:85. doi: 10.1186/s12940-015-0071-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheffield J, Goteti G, Wood EF. Development of a 50-year high-resolution global dataset of meteorological forcings for land surface modeling. J Climate. 2006;19:3088–3111. [Google Scholar]
- Sheridan SC, Dolney TJ. Heat, mortality, and level of urbanization: measuring vulnerability across Ohio, USA. Clim Res. 2003;24:255–265. [Google Scholar]
- Thomson AM, Calvin KV, Smith SJ, Kyle GP, Volke A, Patel P, Delgadoarias S, Bondlamberty B, Wise MA, Clarke LE. RCP4.5: a pathway for stabilization of radiative forcing by 2100. Clim Change. 2011;109:77–94. [Google Scholar]
- Thrasher B, Maurer EP, McKellar C, Duffy PB. Technical Note: Bias correcting climate model simulated daily temperature extremes with quantile mapping. Hydrol Earth Syst Sci. 2012;16:3309–3314. [Google Scholar]
- Todd N, Valleron AJ. Space–time covariation of mortality with temperature: A systematic study of deaths in France, 1968–2009. Environ Health Perspect. 2015;123:659–664. doi: 10.1289/ehp.1307771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vardoulakis S, Dear K, Hajat S, Heaviside C, Eggen B. Comparative assessment of the effects of climate change on heat- and cold-related mortality in the United Kingdom and Australia. Environ Health Perspect. 2014;122:1285–1292. doi: 10.1289/ehp.1307524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Voorhees AS, Fann N, Fulcher C, Dolwick P, Hubbell B, Bierwagen B, Morefield P. Climate change-related temperature impacts on warm season heat mortality: a proof-of-concept methodology using BenMAP. Environmental Science & Technology. 2011;45:1450–1457. doi: 10.1021/es102820y. [DOI] [PubMed] [Google Scholar]
- Wu J, Zhou Y, Gao Y, Fu JS, Johnson BA, Huang C, Kim YM, Liu Y. Estimation and uncertainty analysis of impacts of future heat waves on mortality in the eastern United States. Environ Health Perspect. 2014;122:10–16. doi: 10.1289/ehp.1306670. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yang J, Liu HZ, Ou CQ, Lin GZ, Zhou Q, Shen GC, Chen PY, Guo Y. Global climate change: Impact of diurnal temperature range on mortality in Guangzhou, China. Environ Pollut. 2013;175:131–136. doi: 10.1016/j.envpol.2012.12.021. [DOI] [PubMed] [Google Scholar]
- Zhou M, Wang H, Zhu J, Chen W, Wang L, Liu S, Li Y, Wang L, Liu Y, Yin P, Liu J, Yu S, Tan F, Barber RM, Coates MM, Dicker D, Fraser M, González-Medina D, Hamavid H, Hao Y, Hu G, Jiang G, Kan H, Lopez AD, Phillips MR, She J, Vos T, Wan X, Xu G, Yan LL, Yu C, Zhao Y, Zheng Y, Zou X, Naghavi M, Wang Y, Murray CJL, Yang G, Liang X. Cause-specific mortality for 240 causes in China during 1990–2013: a systematic subnational analysis for the Global Burden of Disease Study 2013. Lancet. 2016;387:251–272. doi: 10.1016/S0140-6736(15)00551-6. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.