

Abstract
Background
Lifestyle interventions targeting weight loss, such as those delivered through the Diabetes Prevention Program, reduce the risk of developing type 2 diabetes. Technology-mediated interventions may be an option to help overcome barriers to program delivery, and to disseminate diabetes prevention programs on a larger scale.
Objective
We conducted a meta-analysis to evaluate the effect of such technology-mediated interventions on weight loss.
Methods
In this meta-analysis, six databases were searched to identify studies reporting weight change that used technology to mediate diet and exercise interventions, and targeted individuals at high risk for developing type 2 diabetes. Studies published between January 1, 2002 and August 4, 2016 were included.
Results
The search identified 1196 citations. Of those, 15 studies met the inclusion criteria and evaluated 18 technology-mediated intervention arms delivered to a total of 2774 participants. Study duration ranged from 12 weeks to 2 years. A random-effects meta-analysis showed a pooled weight loss effect of 3.76 kilograms (95% CI 2.8-4.7; P<.001) for the interventions. Several studies also reported improved glycemic control following the intervention. The small sample sizes and heterogeneity of the trials precluded an evaluation of which technology-mediated intervention method was most efficacious.
Conclusions
Technology-mediated diabetes prevention programs can result in clinically significant amounts of weight loss, as well as improvements in glycaemia in patients with prediabetes. Due to their potential for large-scale implementation, these interventions will play an important role in the dissemination of diabetes prevention programs.
Keywords: diabetes mellitus, type 2; weight reduction programs; technology; meta-analysis; prediabetic state
Introduction
Over 29 million Americans (approximately 9% of the US population) have diabetes, and an additional 86 million Americans have prediabetes, an asymptomatic condition associated with an increased risk of developing type 2 diabetes [1]. In 2002, the landmark Diabetes Prevention Program (DPP) demonstrated that improved diet, regular exercise, and weight loss lead to a 58% reduction in the 3-year incidence of type 2 diabetes, compared to a placebo control arm, in patients at risk for the disease [2]. Importantly, this reduction was sustained over the long-term; specifically, 10-year follow-up analysis demonstrated the incidence of type 2 diabetes in the lifestyle intervention group was reduced by 34% compared with placebo [3].
The remarkable success of the DPP generated nationwide efforts to translate the results of the original trial intervention into practice [4,5]. The National Diabetes Prevention Program (NDPP) was established in 2010 as a congressionally-authorized initiative to support the dissemination of diabetes prevention programs across the United States [6]. NDPP-recognized diabetes prevention programs consist of 16 weekly sessions (core phase) followed by 6 monthly sessions (postcore phase) delivered by a trained lifestyle coach following the curriculum of the original DPP.
Systematic review of in-person group-based DPP programs demonstrates that they can effectively promote weight loss [7]. Although community-based DPP translations are more accessible, scalable, and financially sustainable than one-on-one interventions used during the original DPP study [4,6], there are barriers to participation. These barriers include transportation, distance, work schedules, aversion to group settings, and child care needs [8-11]. To address these issues, several pilot studies have used technology-mediated interventions to promote weight loss in participants at risk for type 2 diabetes. To date, a systematic review of these studies has not been performed.
The primary purpose of this meta-analysis is to assess the effect of technology-mediated lifestyle interventions on weight loss in those at risk for developing type 2 diabetes. We also discuss reported glycemic changes associated with these interventions.
Methods
Study Selection
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement guidelines for conducting and reporting this meta-analysis (Multimedia Appendix 1) [12]. We examined studies evaluating interventions that used technology to disseminate diet and exercise lifestyle programs, with the aim to achieve weight loss and improve glycemic control in adult patients with prediabetes. A systematic review was performed on the literature published between January 1, 2002 and August 4, 2016. Only studies published after the 2002 DPP study were included. We searched 6 databases to identify relevant studies, including PubMed, EMBASE, SportDiscus, CINAHL, PyschINFO, and Web of Science. Search terms to assess lifestyle intervention and use of technology were used, including the combination of MeSH and Emtree headings and subheadings, free-text keywords, and study design filters (eg, prediabetic state, weight loss, weight reduction programs, prediabet*, diabetes prevent*, telemedicine, telephone, web, technolog*, randomized controlled trial, and controlled clinical trial). We manually searched reference lists of review articles, and experts in the field were contacted to include all possible studies. Studies targeting individuals younger than 18 years of age, pregnant patients, or patients with a diagnosis of type 2 diabetes mellitus were excluded (see Multimedia Appendix 2 for search strategy).
Article titles and abstracts were screened to determine relevance and possible inclusion in the study. Full texts of the resulting articles were then read to determine eligibility based on the inclusion criteria. Authors were contacted directly to request missing weight change data, or clarify intervention methods and participant criteria when necessary.
Studies considered for inclusion had to satisfy three criteria. First, the primary objective of the study was to deliver diet and exercise lifestyle interventions using technology (digital versatile disc [DVD], computer-based program, phone, or text messaging) with the aim to achieve weight loss. Second, the study had to target patients with a diagnosis of prediabetes, or a body mass index (BMI) >24 kilograms per meter squared (kg/m2; or >22 kg/m2 if Asian) and at least one additional risk factor for diabetes (prior gestational diabetes, central adiposity, or metabolic syndrome); these criteria were based on those employed in the NDPP criteria [13]. Third, the study had to be either a randomized controlled trial (RCT) or prospective cohort study—with or without comparison groups—published in an academic journal and reported in English.
Outcomes
The primary outcome was absolute weight change following the intervention. Glycemic changes (as measured by changes in oral glucose tolerance test results, fasting blood glucose levels, hemoglobin A1c levels, prediabetes prevalence, or incidence of diabetes over the intervention period) were also reported, if available.
Studies that included a core intervention phase, as well as a postcore maintenance phase, had data extracted and used for this analysis directly after the core phase was completed. This approach served to reduce heterogeneity between studies that did and did not include a maintenance phase. We assessed absolute weight change effect of technology-mediated interventions, and compared results between those interventions modeled on the DPP with those using a different curriculum. We also examined the influence of intervention duration on weight change. Average percent weight change was also reported, if available. Program attrition was also assessed by comparing the number of enrolled participants with the number of program completers.
Data Analyses
Weight change outcomes in the core phase of each intervention were assessed using a meta-analysis. These outcomes were either directly reported in the study results, calculated by determining the within-person difference between reported weights before and after the intervention, or obtained from the authors. The focus of our study was to observe the effect of technology-mediated interventions on weight change, and since the control groups across the different papers were significantly disparate, we excluded the data reported for control arms and only extracted data from the groups receiving an intervention delivered by technology. Each treatment group (or cohort) was analyzed as one pre/postintervention study. All weights were converted to kg units. Using the standard deviation (SD) of within-person weight change outcomes was necessary for calculating the relative study-influences for the meta-analysis. Studies that did not directly report this value had SDs calculated using either the P-value or the CI associated with average weight change.
Heterogeneity between studies was assessed by Cochran’s Q statistic, which is the weighted sum of squared deviations of the study-specific estimates from the overall one, and is distributed approximately as a chi-squared random variable with k -1 degrees of freedom (k being the number of studies in the analysis) [14]. We further measured the I2 statistic, defined as I2=100%*(Q-k+1)/Q, that quantifies the proportion of heterogeneity in the trial results beyond chance. Higher I2 is indicative of greater heterogeneity. Based on the observation of significant heterogeneity across studies, study estimates were pooled using a random-effects model that allowed for some random variability between studies, as well as sampling error. Publication bias between studies was assessed visually using a funnel plot. The visual effect is supplemented by the more formal Egger’s test [15], which is essentially a significance test of intercept in a weighted least-squares fit of study-specific standardized effect on precision (reciprocal of standard error). A significant intercept is indicative of publication bias. Rosenthal’s fail-safe N, based on the aggregated standardized effect size, was used to estimate the number of additional (potentially unpublished) studies required to convert a significant result into a nonsignificant one. A fail-safe N>5k+10 is indicative of lack of potential publication bias [16]. An influence analysis was carried out to assess the influence of each study by recalculating the pooled estimate after deleting the study.
The included studies were of varied types—ranging from observational to blinded and unblinded randomized trials (with or without control)—making a fixed protocol for quality scoring impractical. Instead we performed an indirect quality-adjusted analysis via a meta-regression, adjusting for study duration, examining whether the analysis used intention-to-treat methods, and whether the intervention incorporated DPP material. Statistical analyses were carried out in STATA 13 (StataCorp LP, College Station, Texas) and R 3.3.0 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Results of Systematic Literature Search
After eliminating duplicates, a total of 1024 publications were identified through the databases; one additional publication was identified from searching reference lists and through consultation with experts. Each publication was screened by title and abstract. The resulting 52 publications were reviewed in full, 37 of which were excluded because they did not meet inclusion criteria. The final systematic review included 15 publications that reported outcomes for a total of 18 intervention arms (Figure 1).
Figure 1.
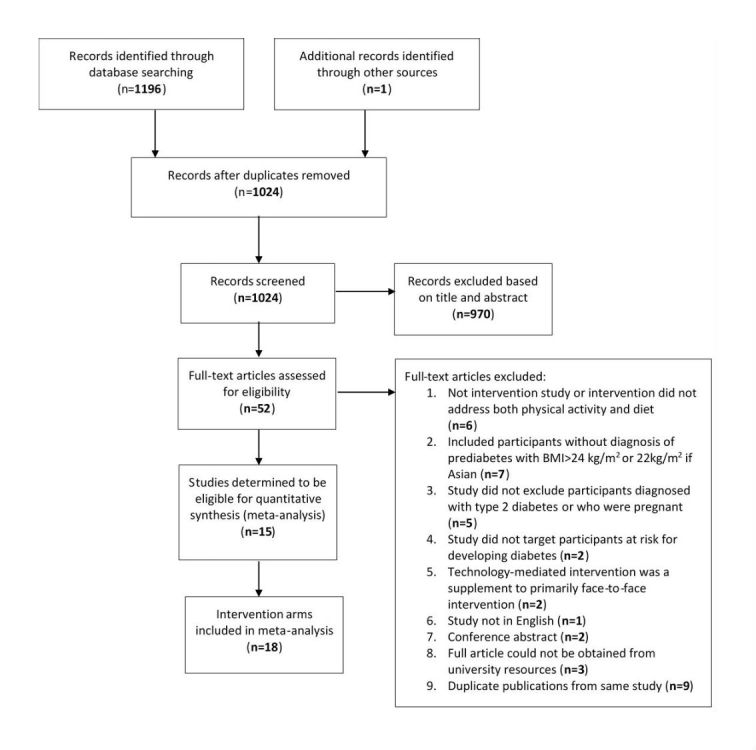
Flowchart showing results of systematic search strategy and selection process. BMI: body mass index.
Study Characteristics
Of the 15 studies included: 6 were RCTs in which the technology-mediated treatment arm was compared to standard care or a face-to-face intervention; 2 included control arms but assigned treatment conditions by community and without randomization; 3 randomly assigned participants to different technology-mediated intervention arms; 1 included parallel interventions arms assigned by community and without randomization; 2 were prospective cohort studies; and 1 allowed participants to self-select into the treatment arm. Multimedia Appendix 3 describes each cohort, and Table 1 shows key outcomes.
Table 1.
Weight change outcomes. DVD: digital versatile disk; kg: kilogram; NA: not available or not applicable; SD: standard deviation.
| Study Cohort (Year): Intervention | Attrition | Level of Utilization | Mean weight change, kg (SD) | % weight change (SD) |
| Aguiar et al (2016): DVD [17] | 19% | NA | -4.98 (4.2)a | -4.85 (4.1) |
| Block et al (2015): Interactive voice response, email, text message, mobile app [18] | 14% | After 6 months, intervention participants interacted with online program in a median of 17 of 24 weeks. | -3. 1 (3.6)a | -3.60 (NA) |
| Sakane et al (2015): Telephone [19] | 18% | Mean responses to telephone calls during 1-year period: 2.8 (SD 0.6; Group A), 5.2 (SD 1.9; Group B), 8.2 (SD 3.5; Group C) | -1.1 (3.4)a | NA |
| Cha et al (2014): Internet and telephone [20] | 13% | NA | -2.9 (4.3) | NA |
| Nicklas et al (2014): Internet [21] | 11% | Median 9 videos watched | -2.6 (5.5)a, at 6 months | NA |
| Sepah et al (2014): Internet [22] | 15% | 85% (187/220) completed at least 4 of the 16 core lessons | -5.0 (3.6) | -5.0 (NA) |
| Betzlbacher et al (2013): Telephone [23] | 0% | All calls completed | -3.3 (4.3) | -3.7 (NA) |
| Ma et al (2013): DVD and email [24] | 10% | NA | -4.5 (7.2)a | -4.9 (7.2) |
| Piatt et al (2013): DVD [25] | 43% | Average attendance for DVD debriefing sessions 2.9/4 | -5.5 (4.0)a | -5.7 (4.0) |
| Piatt et al (2013): Internet and e-counseling [25] | 57% | Average 6.8 of 12 videos viewed | -6.2 (5.1)a | -6.3 (4.5) |
| Ramachandran et al (2013): Text message [26] | 4% | Average number of text messages dropped from 18 to 12 messages a month | -0.1 (2.7) | NA |
| Weinstock et al (2013): Individual telephone [27] | 43% | Average 9 of 16 sessions attended across 2 intervention cohorts | -4.6 (17.6) | -4.2 (16.9) |
| Weinstock et al (2013): Group telephone [27] | 38% | Average 9 of 16 sessions attended across 2 intervention cohorts | -4.9 (17.7) | -4.5 (20.3) |
| Kramer et al (2010): DVD [28] | 14% | Average 10.2 of 12 calls completed | -5.4 (5.2)a | -5.6 (NA) |
| Vadheim et al (2010): Video conference [29] | 12% | Average 14.2 of 16 weeks of participation | -6.7 (3.7) | NA |
| Estabrooks and Smith-Ray (2008): Interactive voice response [30] | 28% | 10% did not complete any calls | -2.2 (2.7) | -2.6 (3.1) |
| Tate et al (2003): Internet only [31] | 15% | NA | -2.0 (5.7)a | -2.2 (NA) |
| Tate et al (2003): Internet and e-counseling [31] | 17% | NA | -4.4 (6.2)a | -4.8 (NA) |
aresults reported for intention-to-treat analysis
Participant Characteristics
A total of 2774 participants were enrolled in the technology-mediated interventions, of whom 2247 had follow-up data included in the final meta-analysis. Averaged across studies, enrolled participants were 49 years old and had a starting BMI of 29 (excluding 1 study that did not report baseline BMI [30]). Thirty-nine percent of the participants were female (excluding 1 study that did not report the gender composition of the intervention cohort [28]), and 34% were white (excluding 4 studies that did not report the number of white participants in the intervention cohorts [28,29]). Four studies were conducted outside of the United States [17,19,26,32] and 2 were undertaken in rural communities [25,29].
Treatment Characteristics
The duration of the interventions ranged from 12 weeks to 2 years. Half of the studies were modeled on the DPP [18,21,22,24,25,27-29]. The technologies employed by the 18 intervention arms included DVDs and e-videos [17,21,24,25,28], Web-based resources [18,20-22,31], videoconferencing [29], telephone (individual and conference calls) [19,20,25,27,28], interactive voice response [18,30], text messages [26], e-counseling [21,24,25,31], email [18,24,25,31], and online group forums [22]. Supplementary print materials, such as diet and physical activity log books [17,19,23,25,28,29] and in-person group DPP [25,29], were also utilized. The lessons and messages delivered via the technology-enabled interventions centered on educating participants on how to achieve a healthy diet and exercise to reduce the risk of type 2 diabetes, and enabling behavioral changes through goal setting, self-monitoring, and logging of diet and physical activity. Video, text message, or Web-based lessons often introduced diet and physical activity concepts, while the personalized or automated phone, text message, and email messages would reinforce concepts, goals, and self-monitoring behavior.
Publication Bias
The funnel plot in Figure 2 was found to be statistically significant (P=.002) using Egger’s test, indicating a potential for publication bias. However, Rosenthal’s fail-safe N was above 4000 (more than 40 times the 5k+10 threshold) suggesting the potential threat from such bias to be quite small. For this reason, no corrective action was undertaken.
Figure 2.
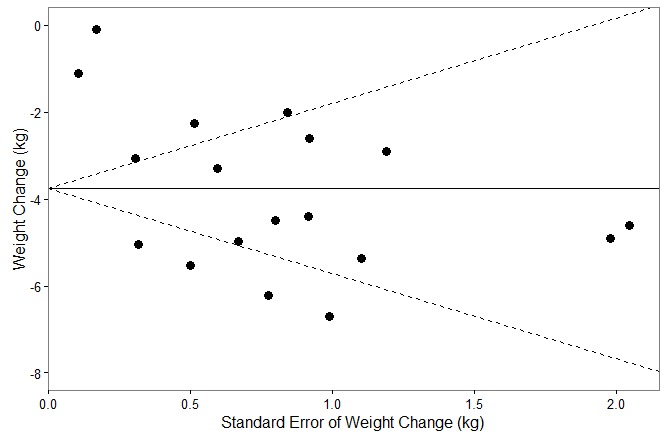
Funnel plot for publication bias analysis.
Change in Weight
Given significant heterogeneity across studies (I2=96.1%, P<.001), a random-effects meta-analysis of the change in weight was performed utilizing 18 cohorts from the 15 studies. Figure 3 displays the change in weight and CIs for each intervention, stratified by whether the intervention was modeled from the DPP. Figure 3 also presents a pooled estimate of mean weight change using a random-effects model combining data from all 18 cohorts. These results demonstrate that technology-based interventions are effective at decreasing weight by an average of 3.76 kg (95% CI 2.8-4.7; P<.001). The DPP-based interventions resulted in marginally higher (P=.074) average weight loss (mean 4.81 kg, 95% CI 3.9-5.7) than non-DPP interventions (mean 2.44 kg, 95% CI 1.5-3.4). The contribution of each study to the overall effect ranged from 3.2-6.6%. Furthermore, the influence plot in Figure 4 indicates that no single point had exceptional influence, and the exclusion of any single cohort did not appreciably change the results of the overall estimate.
Figure 3.
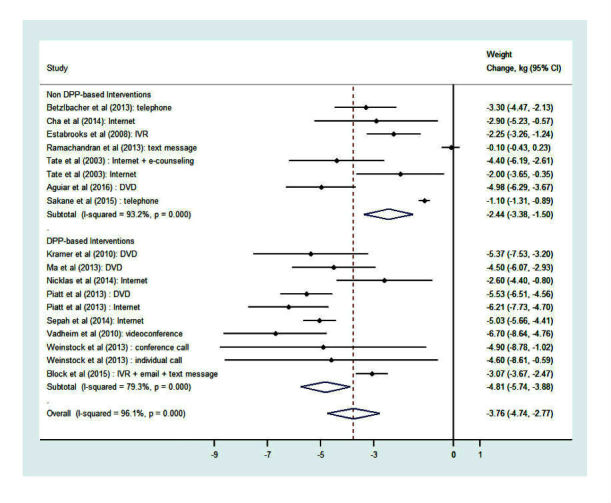
Forest plot of weight change from random-effects meta-analysis outcomes. DPP: Diabetes Prevention Program; DVD: digital versatile disk; IVR: interactive voice response.
Figure 4.
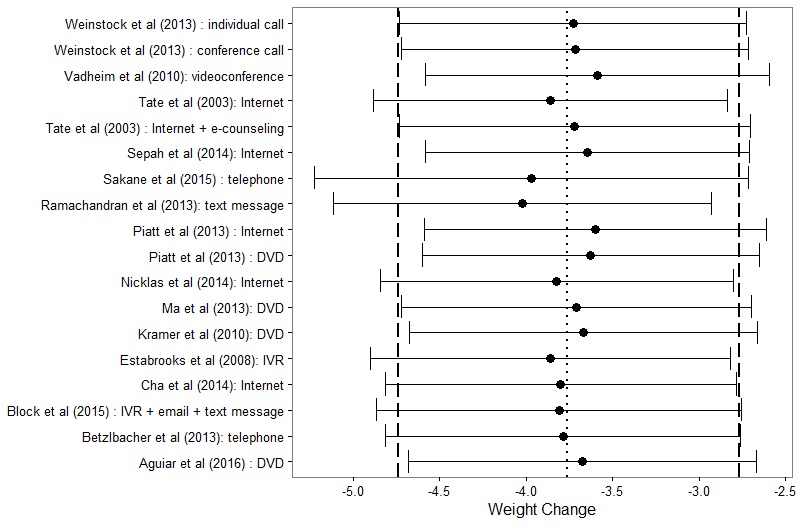
Influence plot of random-effects meta-analysis. DVD: digital versatile disk; IVR: interactive voice response.
Change in Glycaemia and Follow-Up Weight Outcomes
Eight studies reported a change in glycaemia over the course of the intervention [17,18,20,22-25,28]. Multimedia Appendix 4 shows the particular measure(s) used—oral glucose tolerance test, fasting blood glucose, and hemoglobin A1c—as well as baseline and postintervention mean values. Multimedia Appendix 4 also shows the reduction in prediabetes prevalence among participants. All 5 of the studies that reported baseline and postintervention prediabetes prevalence measurements reported decreases in prevalence [17,18,20,23,25]. Of the 4 cohorts reporting conversion from prediabetes to diabetes during the intervention period, rates ranged from 0-18% [21,23,24,26]. The 2 cohorts with the longest intervention durations reported the largest conversion rates [23,26].
Multimedia Appendix 5 presents change in weight measured in follow-up or maintenance periods, which were documented 8 to 36 months after the initial postcore intervention measurements. Follow-up or maintenance period durations varied by study, ranging from 12 to 48 months after baseline measurements. Some cohorts followed their core interventions with less intensive and/or optional maintenance interventions [21,22,24,27,33], while others included follow-up measurements without postcore maintenance interventions [23,25,34,35]. The relationship between follow-up time and weight change was mixed, with some shorter time frames observing a larger change, and some longer time frames observing a smaller change.
Discussion
This meta-analysis shows that technology-mediated interventions lead to clinically significant weight loss (mean 3.76 kg, 95% CI 2.8-4.7 kg; P<.001) in individuals at risk for diabetes. Additionally, as evidenced by our finding that 8 of 18 intervention arms [19,22,24,25,27,32-35] reported sustained weight loss outcomes at least one-year postintervention, the weight loss achieved through technology-mediated interventions may be sustainable. Moreover, the finding that several of the studies [17,18,20,23-25,28] reported improved glycaemia further supports the argument that these interventions are effective methods to prevent the development of diabetes.
Among American adults, there is widespread adoption of cell phones (92%) and smartphones (67%) [36]. These usage levels indicate that placing technology-mediated interventions in the hands of patients is becoming easier than ever. Moreover, from a clinical standpoint, we may soon live in a world where provider referrals to technology-mediated interventions to promote lifestyle and behavior change are commonplace. However, the marketplace is currently filled with a patchwork of technology-mediated solutions that vary widely in terms of quality, particularly in terms of health-related apps. This market is filled with products whose development often lacks professional content-expertise, theoretical underpinnings, and an appropriate evidence base to support use [37,38]. Given that we have demonstrated that quality technology-mediated interventions are effective at promoting and sustaining weight loss, more should be done to promote their use within clinical practice, so that consumers may succeed with high quality applications, as opposed to fail with poorly conceptualized, designed, and implemented tools.
Two design components that were of particular interest in this meta-analysis were: (1) studies based on the DPP curriculum, and (2) study duration. While not quite achieving statistical significance, there was a strong trend toward more weight loss in the intervention arms that were based on the DPP curriculum. Studies investigating the efficacy of technology-based interventions often rely on short-term follow-up, which is commonly seen as a limitation of the existing body of literature. Our analysis shows no effect of intervention duration on weight loss outcomes, which is not consistent with previously reported literature [7]. It is possible that this finding is due to the heterogeneity of the technologies utilized, or the fact that some interventions included maintenance phase components while others did not.
Limitations
One limitation of our meta-analysis was the inability to compare intervention and control weight change results within the studies. This issue arose because only four studies were RCTs with a nontechnology control arm. To demonstrate whether technology-mediated interventions have comparable weight loss outcomes to in-person interventions, future studies are needed that directly compare these two cohorts. There was wide heterogeneity in intervention type, duration, population, and study attrition. Furthermore, none of the included studies had large sample sizes. Thus, conclusions could not be drawn about which method would be most efficacious. The variety of reported glycaemia changes limited our ability to perform a meta-analysis of these results. There was a fair amount of heterogeneity across the studies when examining study populations, as well as interventions used. This heterogeneity raises concerns for the statistical pooling of study results, but it strengthens the generalizability of the conclusions drawn from this systematic review, and provides important implications for the implementation of diabetes prevention programs.
Quality assessment was difficult, given the variety of study designs. Even in those studies that were RCTs, several standard quality criteria were not applicable. For example, complete blinding cannot be achieved within behavioral intervention studies. Instead, we chose three quality criteria that were relevant across studies (intention-to-treat analysis, intervention duration, and whether the study was modeled after the DPP) and included them as independent predictors in the meta-regression.
Future Directions
Those technology-mediated interventions that were modeled after the DPP tended to result in greater weight loss compared to the non-DPP modeled interventions, although this difference was not statistically significant at the .05 level. Further research is needed to test the hypothesis that weight loss outcomes can be optimized by incorporating the DPP curriculum.
Several studies investigated the effect of technology-mediated interventions on specific populations, such as younger populations or those in rural settings. Further investigation is needed using large methodologically sound comparative-effect research trials to determine which interventions are most efficacious in facilitating weight loss and glycemic improvement in specific demographic categories of participants at risk for developing diabetes. Such categories include specific age ranges, BMIs, and genders, as well as social, economic, and ethnic backgrounds. It has been shown that the success of a lifestyle intervention is largely affected by the participant’s ability to choose the intervention modality [25], but factors that make an intervention more efficacious among target populations need to be explored, especially as technology allows intervention delivery to be individualized. Future studies should also evaluate whether technology should be coupled with some degree of in-person contact.
Studies are needed to examine how accessible these interventions are in low-income urban populations. For technology-mediated diabetes prevention interventions to expand the reach of diabetes prevention to a greater number of individuals at high risk for developing diabetes, research is needed with respect to intervention cost and payment models.
The inconsistency between using fasting blood glucose and hemoglobin A1c to measure metabolic control made it difficult to determine the extent to which technology-mediated interventions affected glycemic improvement. Weight loss was instead used as a direct health outcome measure. Some interventions may not result in weight loss but may improve glycemic control. Ideally, studies would include both weight loss and glycemic control (which would be measured using both fasting glucose and hemoglobin A1c) as a standardized evaluation methodology.
While a few of the studies in this analysis compared different forms of technology, further analysis is required to understand the advantages that each technology contributes to intervention outcome. In addition, the efficacy of maintenance phase interventions needs to be adequately assessed by comparing the weight loss outcomes and glycaemia of those who choose to stay in maintenance phase and those who decide to drop out. Understanding of such factors could guide the establishment of technology-mediated interventions as a potential correlate to the NDPP’s current program.
Conclusion
Our meta-analysis showed that technology-mediated diabetes prevention interventions resulted in weight loss and lead to significant improvements in glycaemia. These results suggest that technology-mediated interventions could be an alternative to in-person diabetes prevention programs. The option of using technology-mediated delivery can potentially overcome barriers of access and allow expanded dissemination of such interventions.
Acknowledgments
Funding for this research was provided through the Michigan Diabetes Research Center (grant P30DK020572) as well as the Training Program in Endocrinology and Metabolism (grant T32DK007245) through the National Institutes of Health/National Institute of Diabetes, Digestive, and Kidney Disease. The funders had no role in study design, data collection, data analysis, decision to publish, or preparation of the manuscript.
Abbreviations
- BMI
body mass index
- DPP
Diabetes Prevention Program
- DVD
digital versatile disc
- k
number of studies in the analysis
- kg
kilogram
- NDPP
National Diabetes Prevention Program
- RCT
randomized controlled trial
- SD
standard deviation
Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist.
Search strategy.
Published studies of technology-mediated diabetes prevention interventions.
Change in glycaemia.
Follow-up weight outcomes.
Footnotes
Conflicts of Interest: NK is Chief Medical Officer of Canary Health (formerly DPS Health). None of the other authors declare any conflicts of interest. CRR has collaborated on research with Omada Health but has not received any financial compensation from this organization.
References
- 1.Centers for Disease Control and Prevention . National Diabetes Statistics Report. Atlanta, GA: U.S. Department of Health and Human Services; 2014. [2015-05-04]. Estimates of Diabetes and Its Burden in the United States http://www.cdc.gov/diabetes/data/statistics/2014StatisticsReport.html . [Google Scholar]
- 2.Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA, Nathan DM, Diabetes Prevention Program Research Group Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002 Feb 07;346(6):393–403. doi: 10.1056/NEJMoa012512. http://europepmc.org/abstract/MED/11832527 .346/6/393 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Diabetes Prevention Program Research Group. Knowler WC, Fowler SE, Hamman RF, Christophi CA, Hoffman HJ, Brenneman AT, Brown-Friday JO, Goldberg R, Venditti E, Nathan DM. 10-year follow-up of diabetes incidence and weight loss in the Diabetes Prevention Program Outcomes Study. Lancet. 2009 Nov 14;374(9702):1677–86. doi: 10.1016/S0140-6736(09)61457-4. http://europepmc.org/abstract/MED/19878986 .S0140-6736(09)61457-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Vojta D, Koehler TB, Longjohn M, Lever JA, Caputo NF. A coordinated national model for diabetes prevention: linking health systems to an evidence-based community program. Am J Prev Med. 2013 Apr;44(4 Suppl 4):S301–6. doi: 10.1016/j.amepre.2012.12.018.S0749-3797(13)00026-3 [DOI] [PubMed] [Google Scholar]
- 5.Yoon U, Kwok LL, Magkidis A. Efficacy of lifestyle interventions in reducing diabetes incidence in patients with impaired glucose tolerance: a systematic review of randomized controlled trials. Metabolism. 2013 Feb;62(2):303–14. doi: 10.1016/j.metabol.2012.07.009.S0026-0495(12)00272-7 [DOI] [PubMed] [Google Scholar]
- 6.Albright AL, Gregg EW. Preventing type 2 diabetes in communities across the U.S.: the National Diabetes Prevention Program. Am J Prev Med. 2013 Apr;44(4 Suppl 4):S346–51. doi: 10.1016/j.amepre.2012.12.009.S0749-3797(13)00016-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ali MK, Echouffo-Tcheugui J, Williamson DF. How effective were lifestyle interventions in real-world settings that were modeled on the Diabetes Prevention Program? Health Aff (Millwood) 2012 Jan;31(1):67–75. doi: 10.1377/hlthaff.2011.1009. http://content.healthaffairs.org/cgi/pmidlookup?view=long&pmid=22232096 .31/1/67 [DOI] [PubMed] [Google Scholar]
- 8.Venditti EM, Wylie-Rosett J, Delahanty LM, Mele L, Hoskin MA, Edelstein SL, Diabetes Prevention Program Research Group Short and long-term lifestyle coaching approaches used to address diverse participant barriers to weight loss and physical activity adherence. Int J Behav Nutr Phys Act. 2014 Feb;11:16. doi: 10.1186/1479-5868-11-16. http://www.ijbnpa.org/content/11//16 .1479-5868-11-16 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Laws RA, Fanaian M, Jayasinghe UW, McKenzie S, Passey M, Davies GP, Lyle D, Harris MF. Factors influencing participation in a vascular disease prevention lifestyle program among participants in a cluster randomized trial. BMC Health Serv Res. 2013 May;13:201. doi: 10.1186/1472-6963-13-201. http://www.biomedcentral.com/1472-6963/13/201 .1472-6963-13-201 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ackermann RT. Working with the YMCA to implement the Diabetes Prevention Program. Am J Prev Med. 2013 Apr;44(4 Suppl 4):S352–6. doi: 10.1016/j.amepre.2012.12.010.S0749-3797(13)00017-2 [DOI] [PubMed] [Google Scholar]
- 11.McTigue KM, Conroy MB, Hess R, Bryce CL, Fiorillo AB, Fischer GS, Milas NC, Simkin-Silverman LR. Using the internet to translate an evidence-based lifestyle intervention into practice. Telemed J E Health. 2009 Nov;15(9):851–8. doi: 10.1089/tmj.2009.0036. [DOI] [PubMed] [Google Scholar]
- 12.Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA, PRISMA-P Group Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015 Jan;4:1. doi: 10.1186/2046-4053-4-1. http://www.systematicreviewsjournal.com/content/4//1 .2046-4053-4-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Centers for Disease Control and Prevention Diabetes Prevention Recognition Program: Standards and Operating Procedures. 2015. [2015-05-04]. http://www.cdc.gov/diabetes/prevention/recognition .
- 14.Cochran WG. The combination of estimates from different experiments. Biometrics. 1954 Mar;10(1):101. doi: 10.2307/3001666. [DOI] [Google Scholar]
- 15.Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997 Sep 13;315(7109):629–34. doi: 10.1136/bmj.315.7109.629. http://europepmc.org/abstract/MED/9310563 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Rosenthal R. Combining results of independent studies. Psychol Bull. 1978;85(1):185–193. [Google Scholar]
- 17.Aguiar EJ, Morgan PJ, Collins CE, Plotnikoff RC, Young MD, Callister R. Efficacy of the Type 2 Diabetes Prevention Using LifeStyle Education Program RCT. Am J Prev Med. 2016 Mar;50(3):353–64. doi: 10.1016/j.amepre.2015.08.020.S0749-3797(15)00510-3 [DOI] [PubMed] [Google Scholar]
- 18.Block G, Azar KM, Romanelli RJ, Block TJ, Hopkins D, Carpenter HA, Dolginsky MS, Hudes ML, Palaniappan LP, Block CH. Diabetes prevention and weight loss with a fully automated behavioral intervention by email, web, and mobile phone: a randomized controlled trial among persons with prediabetes. J Med Internet Res. 2015 Oct 23;17(10):e240. doi: 10.2196/jmir.4897. http://www.jmir.org/2015/10/e240/ v17i10e240 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Sakane N, Kotani K, Takahashi K, Sano Y, Tsuzaki K, Okazaki K, Sato J, Suzuki S, Morita S, Oshima Y, Izumi K, Kato M, Ishizuka N, Noda M, Kuzuya H. Effects of telephone-delivered lifestyle support on the development of diabetes in participants at high risk of type 2 diabetes: J-DOIT1, a pragmatic cluster randomised trial. BMJ Open. 2015 Aug 19;5(8):e007316. doi: 10.1136/bmjopen-2014-007316. http://bmjopen.bmj.com/cgi/pmidlookup?view=long&pmid=26289448 .bmjopen-2014-007316 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Cha E, Kim KH, Umpierrez G, Dawkins CR, Bello MK, Lerner HM, Narayan KM, Dunbar SB. A feasibility study to develop a diabetes prevention program for young adults with prediabetes by using digital platforms and a handheld device. Diabetes Educ. 2014 Jun;40(5):626–37. doi: 10.1177/0145721714539736.0145721714539736 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Nicklas JM, Zera CA, England LJ, Rosner BA, Horton E, Levkoff SE, Seely EW. A web-based lifestyle intervention for women with recent gestational diabetes mellitus: a randomized controlled trial. Obstet Gynecol. 2014 Sep;124(3):563–70. doi: 10.1097/AOG.0000000000000420.00006250-201409000-00013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Sepah SC, Jiang L, Peters AL. Translating the Diabetes Prevention Program into an online social network: validation against CDC standards. Diabetes Educ. 2014 Jul;40(4):435–443. doi: 10.1177/0145721714531339.0145721714531339 [DOI] [PubMed] [Google Scholar]
- 23.Betzlbacher A, Grady K, Savas L, Cotterill S, Boaden R, Summers L, Gibson M. Behaviour change among people with impaired glucose tolerance: comparison of telephone-based and face-to-face advice. J Health Serv Res Policy. 2013 Apr;18(1 Suppl):2–6. doi: 10.1177/1355819612473582.18/1_suppl/2 [DOI] [PubMed] [Google Scholar]
- 24.Ma J, Yank V, Xiao L, Lavori PW, Wilson SR, Rosas LG, Stafford RS. Translating the Diabetes Prevention Program lifestyle intervention for weight loss into primary care: a randomized trial. JAMA Intern Med. 2013 Jan 28;173(2):113–21. doi: 10.1001/2013.jamainternmed.987. http://europepmc.org/abstract/MED/23229846 .1485081 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Piatt GA, Seidel MC, Powell RO, Zgibor JC. Comparative effectiveness of lifestyle intervention efforts in the community: results of the Rethinking Eating and ACTivity (REACT) study. Diabetes Care. 2013 Feb;36(2):202–9. doi: 10.2337/dc12-0824. http://europepmc.org/abstract/MED/22966092 .dc12-0824 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ramachandran A, Snehalatha C, Ram J, Selvam S, Simon M, Nanditha A, Shetty AS, Godsland IF, Chaturvedi N, Majeed A, Oliver N, Toumazou C, Alberti KG, Johnston DG. Effectiveness of mobile phone messaging in prevention of type 2 diabetes by lifestyle modification in men in India: a prospective, parallel-group, randomised controlled trial. Lancet Diabetes Endocrinol. 2013 Nov;1(3):191–8. doi: 10.1016/S2213-8587(13)70067-6.S2213-8587(13)70067-6 [DOI] [PubMed] [Google Scholar]
- 27.Weinstock RS, Trief PM, Cibula D, Morin PC, Delahanty LM. Weight loss success in metabolic syndrome by telephone interventions: results from the SHINE Study. J Gen Intern Med. 2013 Dec;28(12):1620–8. doi: 10.1007/s11606-013-2529-7. http://europepmc.org/abstract/MED/23843020 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kramer MK, Kriska AM, Venditti EM, Semler LN, Miller RG, McDonald T, Siminerio LM, Orchard TJ. A novel approach to diabetes prevention: evaluation of the Group Lifestyle Balance program delivered via DVD. Diabetes Res Clin Pract. 2010 Dec;90(3):e60–3. doi: 10.1016/j.diabres.2010.08.013.S0168-8227(10)00403-1 [DOI] [PubMed] [Google Scholar]
- 29.Vadheim LM, McPherson C, Kassner DR, Vanderwood KK, Hall TO, Butcher MK, Helgerson SD, Harwell TS. Adapted diabetes prevention program lifestyle intervention can be effectively delivered through telehealth. Diabetes Educ. 2010 Aug;36(4):651–6. doi: 10.1177/0145721710372811.0145721710372811 [DOI] [PubMed] [Google Scholar]
- 30.Estabrooks PA, Smith-Ray RL. Piloting a behavioral intervention delivered through interactive voice response telephone messages to promote weight loss in a pre-diabetic population. Patient Educ Couns. 2008 Jul;72(1):34–41. doi: 10.1016/j.pec.2008.01.007.S0738-3991(08)00015-3 [DOI] [PubMed] [Google Scholar]
- 31.Tate DF, Jackvony EH, Wing RR. Effects of Internet behavioral counseling on weight loss in adults at risk for type 2 diabetes: a randomized trial. JAMA. 2003 Apr 9;289(14):1833–6. doi: 10.1001/jama.289.14.1833.289/14/1833 [DOI] [PubMed] [Google Scholar]
- 32.Begg CB, Berlin JA. Publication bias and dissemination of clinical research. J Natl Cancer Inst. 1989 Jan 18;81(2):107–15. doi: 10.1093/jnci/81.2.107. [DOI] [PubMed] [Google Scholar]
- 33.Trief PM, Weinstock RS, Cibula D, Delahanty LM. Sustained weight loss one year after group telephone intervention: 3-year results from the SHINE study. Diabetes Res Clin Pract. 2014 Dec;106(3):e74–8. doi: 10.1016/j.diabres.2014.09.032.S0168-8227(14)00432-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Savas LA, Grady K, Cotterill S, Summers L, Boaden R, Gibson JM. Prioritising prevention: implementation of IGT Care Call, a telephone based service for people at risk of developing type 2 diabetes. Prim Care Diabetes. 2015 Feb;9(1):3–8. doi: 10.1016/j.pcd.2014.07.003.S1751-9918(14)00079-5 [DOI] [PubMed] [Google Scholar]
- 35.Piatt GA, Seidel MC, Powell RO, Zgibor JC. Influence of patient-centered decision making on sustained weight loss and risk reduction following lifestyle intervention efforts in rural Pennsylvania. Diabetes Educ. 2016 Jun;42(3):281–90. doi: 10.1177/0145721716636962.0145721716636962 [DOI] [PubMed] [Google Scholar]
- 36.Rainie L, Zickuhr K. Pew Research Center. 2015. [2016-11-21]. Americans' views on mobile etiquette http://www.pewinternet.org/2015/08/26/americans-views-on-mobile-etiquette/
- 37.Subhi Y, Bube SH, Rolskov BS, Skou Thomsen AS, Konge L. Expert involvement and adherence to medical evidence in medical mobile phone apps: a systematic review. JMIR Mhealth Uhealth. 2015 Jul 27;3(3):e79. doi: 10.2196/mhealth.4169. http://mhealth.jmir.org/2015/3/e79/ v3i3e79 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Nikolaou CK, Lean ME. Mobile applications for obesity and weight management: current market characteristics. Int J Obes (Lond) 2017 Jan;41(1):200–202. doi: 10.1038/ijo.2016.186.ijo2016186 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist.
Search strategy.
Published studies of technology-mediated diabetes prevention interventions.
Change in glycaemia.
Follow-up weight outcomes.