

Abstract
Clinically, pure spermatic-cord lipoma has not been recognized as a disease entity but regarded as an incidental finding at the time of hernia repair, because it presents groin symptoms and clinical findings indistinguishable from those of inguinal hernia. We report the successful treatment of case of huge pure spermatic-cord lipoma originally misdiagnosed as inguinal hernia. The patients had tumor excision without orchiectomy. Symptoms improved without any complication. In patients with inguinal hernia symptoms, pure spermatic-cord lipoma should be recognized as a significant clinical entity, and differential diagnosis should be achieved using ultrasonography and computed tomography to avoid unnecessary hernia repair.
Keywords: Diagnosis, Herniorrhaphy, Inguinal hernia, Misdiagnosis, Spermatic cord lipoma
Introduction
Spermatic cord lipoma is a clinical entity widely regarded as an incidental finding at the time of hernia repair. A former study even described the term lipoma as a misnomer, as it was believed that spermatic cord lipoma was an extension and indirect herniation of the retroperitoneal fat.1 In another study, only the lipoma confined to the inguinal canal, with no connection to the extraperitoneal fat, can be considered a true lipoma of the spermatic cord.2 Although the reported incidence of spermatic cord lipoma was low prior to the development of laparoscopic repair, especially for lipomas not accompanied with an inguinal hernia sac, the prevalence of such findings was later revealed to be higher than expected.3 Spermatic cord lipoma can present with groin symptoms and clinical findings indistinguishable from those of inguinal hernia, which can lead to preoperative misdiagnosis of lipomas. We experienced successful treatment of two cases with pure spermatic cord lipoma, originally misdiagnosed as inguinal hernia and will present one of the two cases.
Case report
A 33-year-old man had undergone laparoscopic right herniorrhaphy at another hospital 1 month ago, presented to our clinic with right scrotal swelling, without postoperative symptomatic improvement. He was unable to visit the urologist immediately after the operation due to his busy schedule. On physical examination, the right scrotum was the size of an adult fist, and a non-tender mass was noted. On scrotal sonography, a homogenous hyperechoic mass was noted, while both testes were intact (Fig. 1). On abdominopelvic CT, a club-shaped enlarged fatty component of the spermatic cord was noted in right inguinal canal and right scrotal sac (Fig. 2). Through the inguinal incision, the surgical findings showed no connection to the peritoneum and no herniation. The tumor was severely adhered to the spermatic cord and epididymis. The right vas deferens couldn't be identified and had to be resected. The dissected testis and the epididymis at the distal area were preserved. And the size of the dissected tumor was 10 × 7.5 × 5 cm (Fig. 3). Histopathology indicated spermatic cord lipoma. At the 6-month follow-up, US and abdominopelvic CT showed no specific findings.
Figure 1.
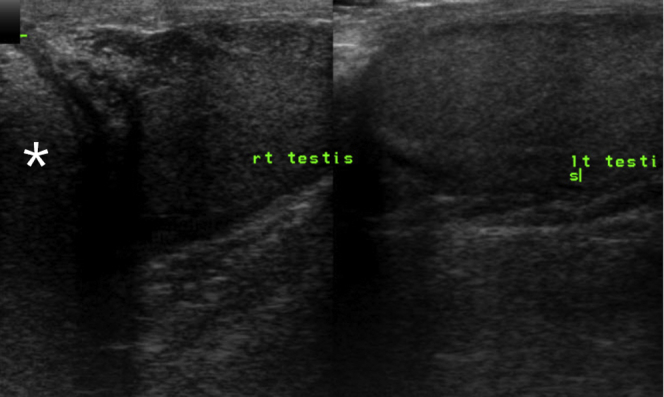
On scrotal sonography, a homogenous hyperechoic mass was noted, while both testes were intact. Axis, vertical cephalad; *, lipoma.
Figure 2.

Preoperative computed tomography revealed a club-shaped, enlarged fatty component of the spermatic cord in the right inguinal canal and right scrotal sac. Yellow arrows, both testes.
Figure 3.

The tumor had a size of 10 × 7.5 × 5 cm, ovoid shape, and consisted of a hard and well-encapsulated mass. On cut surface, the mass had yellowish appearance and appeared to have collected fluid.
Discussion
There have been several reports describing the etiology of incidental spermatic cord lipoma, with one mentioning it may represent the associated herniated fat,1 while another stating that spermatic cord lipoma should only be diagnosed when confined to the spermatic cord, without communication to the peritoneum.2 We are in favor of the later point of view. Spermatic cord lipoma can cause hernia's symptoms in the absence of a true hernia associated with a peritoneal defect; if overlooked at the time of laparoscopic hernia repair, unsatisfactory results of the repair may be reported. Moreover, it is believed that pure spermatic cord lipoma may infiltrate the internal ring and cause dilation, indirectly resulting in hernia. Thus, limiting the treatment to hernia repair does no resolve spermatic cord lipoma.4 They are many reasons why the pre- or intra-operative diagnosis of spermatic cord lipoma was not well made. Firstly, some study reported that about over half of the pure spermatic cord lipoma patients were diagnosed by US and the others were misdiagnosed as a hernia without any further investigation, furthermore asymptomatic small lipoma couldn't be detected, but it was eventually identified by MRI.1 Next, it has been reported that spermatic lipoma tends to be missed in the open or laparoscopic operation if surgeons do not sort through with careful attention, at open operation, the traction on the cord could tent a fold of peritoneum through the deep ring to mimic a small hernia.3 In addition, even it has been reported that there was a case about a missing hernia only to discover a persistent swelling postoperatively, which identified as a cord lipoma at subsequent open operation.4 Finally, in general, lipoma of the cord receives little clinical attention and wasn't well defined as an independent clinical entity to general surgeons. It was mentioned as an unimportant differential diagnosis of inguinal swelling. Concerning preoperative modalities of investigation, even if the symptoms of spermatic cord lipoma mimic those of inguinal hernia, we should consider the further investigation including abdominopelvic CT and MRI when the tumor presents with such symptoms as slowly growing, non-reducible, fixed, relatively hard and non-tender mass. We believe that ultrasonographic evaluation is effective in differentiating testicular cancer from lipoma but alone is insufficient to diagnose spermatic cord lipoma. If the sonographic findings are unclear, CT or MRI is highly recommended. The pure spermatic cord lipoma has no communication to peritoneum. On CT, especially below the level of the external inguinal ring, its fat content may be difficult to differentiate from mesenteric fat-containing inguinal hernia. However, it was known that spermatic cord lipoma could be discernable in coronal view, as it has a well demarcated superior wall with no opening to the peritoneum laterally to the inferior epigastric vessels, while the mesenteric fat accompanying hernias extend up either medially or laterally to the inferior epigastric vessels, toward the mesentery, without recognizable superior walls.5 For the open approach, the inguinal incision is mandatory to observe whether there is peritoneal connection or not.
Conclusion
In the treatment and diagnosis of patients with inguinal hernia symptoms, we suggest that pure spermatic cord lipoma should be recognized as a significant clinical entity, and urologic differential diagnosis should be performed. Exact preoperative diagnosis is important to avoid unnecessary hernia repair.
Conflict of interest
None.
Acknowledgment
None.
References
- 1.Lilly M.C., Arregui M. Lipoma of the cord and round ligament. Ann Surg. 2000;235:586–590. doi: 10.1097/00000658-200204000-00018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Fawcett A.N., Rooney P.S. Inguinal cord lipoma. Br J Surg. 1997;84:1168–1169. [PubMed] [Google Scholar]
- 3.Nasr Ayman O., Tormey S., Walsh T.N. Lipoma of the cord and round ligament: an overlooked diagnosis? Hernia. 2005;9:245–247. doi: 10.1007/s10029-005-0335-9. [DOI] [PubMed] [Google Scholar]
- 4.McDonnell C.O., Walsh T.N. A hernia sac cannot be found at operation. Br J Surg. 2000;87:521–522. doi: 10.1046/j.1365-2168.2000.01406-14.x. [DOI] [PubMed] [Google Scholar]
- 5.Fataar Shadley. CT of inguinal canal lipomas and fat-containing inguinal hernias. J Med Imaging Radiat Oncol. 2011;55:485–492. doi: 10.1111/j.1754-9485.2011.02288.x. [DOI] [PubMed] [Google Scholar]