

Abstract
This paper reviews the evolution of the Oregon model of family behavior therapy over the past four decades. Inspired by basic research on family interaction and innovation in behavior change theory, a set of intervention strategies were developed that were effective for reducing multiple forms of problem behavior in children (e.g., Patterson, Chamberlain, & Reid, 1982). Over the ensuing decades, the behavior family therapy principles were applied and adapted to promote children’s adjustment to address family formation and adaptation (Family Check-Up model), family disruption and maladaptation (Parent Management Training–Oregon model), and family attenuation and dissolution (Treatment Foster Care–Oregon model). We provide a brief overview of each intervention model and summarize randomized trials of intervention effectiveness. We review evidence on the viability of effective implementation, as well as barriers and solutions to adopting these evidence-based practices. We conclude by proposing an integrated family support system for the three models applied to the goal of reducing the prevalence of severe problem behavior, addiction, and mental problems for children and families, as well as reducing the need for costly and largely ineffective residential placements.
Keywords: parent training, treatment foster care, prevention, developmental models, peers
In the late 1950S, the effectiveness of treating children’s behavior problems with even intensive residential interventions was called into question. Despite gains during treatment, returning children back into pathogenic environments meant losing treatment gains (Redl & Wineman, 1957). At the same time, a new science of behavior was taking hold (Skinner, 1954) with a strong emphasis on the observation of reinforcement for problem behavior in the natural environment. The application of reinforcement principles to improving the family environment of children with problem behavior was a promising application. There were four groups within the United States that led this effort using a coordinated set of strategies (Patterson, 2002): Sidney Bijou (Bijou & Baer, 1966), Connie Hanf (1968), Robert Wahler (Wahler, Winkel, Peterson, & Morrison, 1965), and Gerald Patterson (Patterson, 1965). These interacting research groups generated a set of core principles that remain central in today’s parent training programs: (a) parents, not therapists, serve as the treatment agents; (b) parents learn to track and record behavior; and (c) parents apply contingency management with their children using positive reinforcement for positive child behavior and mild negative sanctions to discourage problem behavior.
In the most recent compendium of evidence-based psychotherapies (Weisz & Kazdin, 2010), all eight of the treatments for “externalizing disorders” have their roots in behavior family therapy innovations emerging from these four groups in the 1960s, and the following were directly derived: The Incredible Years (Webster-Stratton & Reid, 2010), Parent Management Training (Kazdin, 2010), Parent-Child Interaction Therapy (Zisser & Eyberg, 2010), Triple P Positive Parenting (Sanders & Murphy-Brennan, 2010), Parent Management Training–Oregon model (Forgatch & Patterson, 2010), and Treatment Foster Care, Oregon model (Smith & Chamberlain, 2010). In addition, family-based treatment for oppositional behavior by McMahon and Forehand (2005) is based on these basic behavior change principles applied to families. A search of Google Scholar for the term “behavioral parent training” yielded 1,520,000 scholarly articles on this topic.
The application of reinforcement principles to improving family life, in general, and children’s mental health, in particular, is the major success story of behavior science in the 20th century. Of interest is the potential for a systematic integration of advances in behavioral family interventions to improve the mental health and well-being of children and adolescents in communities, especially those most vulnerable to pathogenic environments. This review provides an overview of the evolution of research within the Oregon group since the seminal publication by Patterson, Chamberlain, and Reid (1982) in addressing the unique needs of children and families across the spectrum of family disruption and contexts. Randomized trials are reviewed, as well as implementation success and failures. Reflection on the findings from these coordinated programs of research suggests next steps for applying behavior change principles to improve the lives of youth and families at the population level.
Oregon Studies of Child Aggression
In the mid-1960s, the Oregon group studied primarily families seeking help to improve children’s aggressive and disruptive behavior. This initiated a series of case studies focused on children with behavior problems. Over the next decade, the studies became more ambitious, with pre/post and follow-up data, larger samples, replications, and randomized controlled trials (Arnold, Levine, & Patterson, 1975; Fleischman & Szykula, 1981; Forgatch & Toobert, 1979; Patterson, 1974; Patterson et al., 1982; Patterson & Reid, 1970). Success in treating aggressive behavior in children fueled new efforts to apply the same behavioral principles to family intervention to treat multiple offender adolescents (Bank, Marlowe, Reid, Patterson, & Weinrott, 1991; Reid, 1976) and families referred for child abuse (Reid, 1986). The application of behavior therapy to families referred for chronic delinquency and child abuse, however, gave pause to the group, and suggested the need for a developmental model that provided an account for challenges of clinical work with these populations, as well as to guide improved treatment strategies. Incidental to the analysis of family contributions to the severity of problem behavior was the increasing realization within the group and the field (Capaldi & Patterson, 1991; Forgatch, Patterson, & Skinner, 1988; Patterson, 1982) that family dissolution and change were integral to children’s progression from problem behavior to severe forms of delinquency, antisocial behavior, depression, and drug abuse in adolescence.
Family interaction had long been of interest to sociologists concerned with predicting which children would eventually be arrested for criminal behavior in adolescence; many of the criminology studies began in the 1930s (Loeber & Dishion, 1983). Interestingly, when home visitors described families of children who later became delinquent, they reported both overly harsh discipline as well as lax supervision as highly predictive. These early observations from a sociological perspective fit well with the direct observations of research that led to the formulation of the coercion model (Patterson, 1982). The coercion model provides a developmental perspective on how both harsh parenting as well as lax supervision might co-occur. As youth become more problematic, parents disengage from parenting (Patterson, DeBaryshe, & Ramsey, 1989; Patterson, Reid, & Dishion, 1992) and fail to track or monitor youth behavior in the community. Thus, the same parent can be both lax, and overly harsh, often after discovering a child’s most recent escapade (e.g., stealing). Longitudinal research began to fill in the gaps as well as accounting for seemingly paradoxical findings of both clinical research and sociological research on delinquency.
Several research groups converged on an understanding of the longitudinal development and changes observed from childhood through adolescence (see Dishion & Patterson, in press, for a recent review). Longitudinal models emerged that described the cascade of relatively minor problem behavior (often in early childhood) to more serious forms of deviance, including violence, sexual risk taking, and drug abuse. As shown in Figure 1, poor self-regulation and problem behavior in early childhood disrupts a child’s entry into school. Poor relationships with peers and slow academic progress are associated with peer interactions that lead to growth in antisocial behavior in childhood (see Snyder et al., 2006). Such behavior can further undermine school adjustment and family engagement, which leads to more involvement in deviant peer groups (Dishion, Patterson, Stoolmiller, & Skinner, 1991). Deviant peer involvement is the strongest proximal predictor of escalations in multiple forms of problem behavior in adolescence. Adolescent self-organization within deviant peer groups often co-occurs with the waning of parent’s ability to influence positive change (Dishion & Tipsord, 2011).
FIGURE 1.
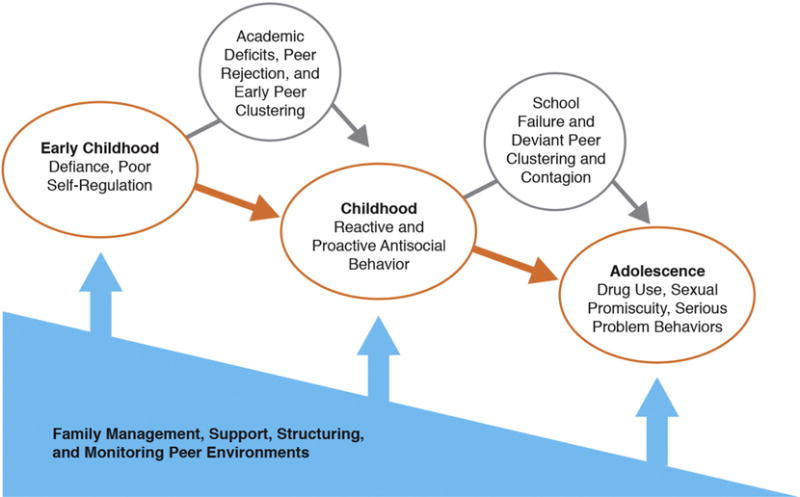
The Cascade Model. Developmental outcomes of early problem behavior and family management as a countervailing force.
A Model-Based Family Intervention Model
A critical feature of the Oregon intervention model is the emphasis on supporting the behavior management skills of caregiving adults, including both daily social interaction processes (e.g., reinforcement patterns) but also improving tracking and monitoring of children’s behavior. The term family management was used to describe a broader set of parenting behaviors than originally targeted in behavior management training (Patterson, 1982; Patterson et al., 1992). Figure 1 summarizes a vast body of evidence indicating that family management is a countervailing force to the cascading evolution towards more serious adjustment problems.
The cascade developmental model has strong implications for the design of interventions that are effective in reducing problem behavior at each stage of development. The covariation of disrupted family management with increasing levels of child and adolescent problem behavior is a unidirectional, recursive process. Family disruption is a dynamic process (Dishion, Forgatch, Van Ryzin, & Winter, 2012), and entails daily social interactions among multiple family members. Children and adolescents can disrupt family environments (Block, Block, & Gjerde, 1986; Forgatch & Stoolmiller, 1994). Children with multiple challenging behaviors “fail” many foster care placements, which in turn exacerbates behavior and well-being (Chamberlain et al., 2006).
It is critical to appreciate that parents often struggle with their own adversities, emotional adjustment, and relationships, and this can impact the caregiving environment they provide. The simple number of caregiver transitions (divorces, breakups, new partners, remarriages, etc.) has a strong linear correlation with the severity of emotional and behavioral adjustment problems (Capaldi & Patterson, 1991). Parent substance use and other problematic and addictive behavior disrupt parenting across generations (Pears, Capaldi, & Owen, 2007).
As the Oregon group began the process of applying the behavior parent training principles to new populations that were mandated to treatment (child abuse, delinquent offending), we observed that the level of intactness of the family covaried with the severity of the clinical presentation. Over the past 30 years, since the publication of one of the earliest randomized trials on parent management training (Patterson et al., 1982), the Oregon group self-organized into three groups, each developing expertise in families at various stages of formation and disruption.
Figure 2 provides an overview of stages of disruption of family systems over time. It has often been observed that stress is a change agent in families, always related to change, some of which increases resilience, and others lead to family disruption and potential dissolution (caregiving environment changes, parents unavailable, foster care, etc.). Family formation includes the early stages of families that co-evolve with the birth and development of a child, or may involve the formation of a step-family following a divorce. Families in this stage are able to mobilize to address stressors, and often make changes on their own to improve the well-being of family members and children. At times, when stressors are left unattended, specific patterns of maladaption might occur, such as patterns of coercive conflict, marital conflict, betrayal or avoidance and dissatisfaction. Families experiencing repeated difficulties, disruption, and maladaptation often benefit from structure approaches to behavior change, and perhaps would be less responsive to interventions with a lighter touch. Finally, over time, families become weak, caregivers leave, become incarcerated, and are forced to give up their children, or the child and adolescent leave the home. When families attenuate and dissolve, family approaches to behavior parent training are less viable, primarily because of the correlated chaos and lack of a stable caregiving environment.
FIGURE 2.
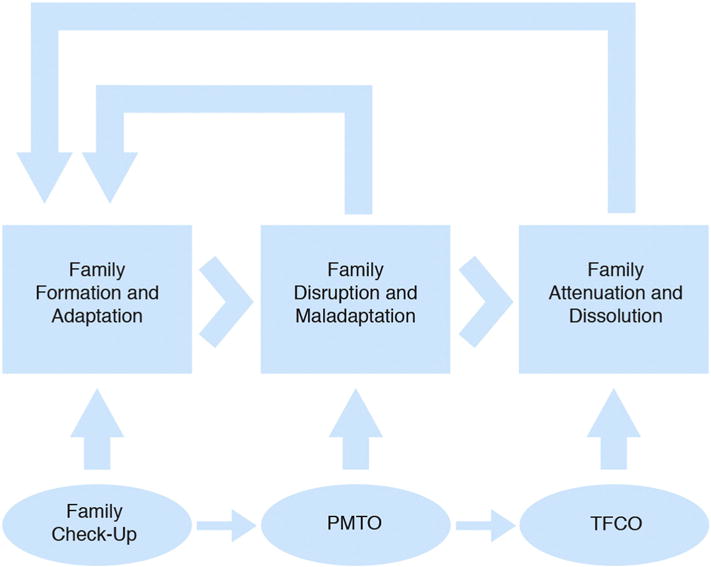
Innovations of behavioral parenting interventions addressing family disruption and reformation.
As shown in Figure 2, the Oregon group organized around families’ needs, with the Family Check-Up addressing the needs of intact families, some of whom may change with minimal support. Parent management training was most appropriate for disrupted or maladapting families, and treatment foster care was most appropriate to address the needs of children and families that are attenuated and dissolving, with the eventual goal of placing a child and adolescent back into the family origin or other permanent, safe, and secure caregiving environment. As shown in Figure 2, we see the link between optimal intervention strategies, family disruption, and youth adjustment as potentially dynamic, with the explicit goal of interventions returning families to adaptive homeostasis in which daily social interactions are minimally coercive and optimally positive and supportive. Note that all three intervention models described below are based on a common core of behavior change principles and strategies. We briefly describe each intervention in turn, and summarize the key outcome studies involving randomization that link the intervention to improved social interactions in the caregiving environment, which in turn improves the behavior and adjustment of youth and family members.
THE FAMILY CHECK-UP
The Family Check-Up (FCU) was designed to support parents during key developmental transitions that are vulnerable to disrupted family management, child problem behavior, and emotional distress. This FCU is designed as both a preventive tool as well as an initial step (i.e., an intake process) for families seeking treatment. The FCU was initially developed at the Oregon Social Learning Center (OSLC) as a selected intervention for families of young adolescents in middle school (Dishion, Kavanagh, & Kiesner, 1999). Modeled after the Drinker’s Check-Up (Miller & Rollnick, 2002), the FCU service model involves two to three sessions, including the following three components: (a) an initial interview, (b) the family assessment, and (c) a feedback session (see Dishion & Kavanagh, 2003; Dishion & Stormshak, 2007, for a review).
Within the initial interview, the parent consultant engages the caregiver in a reflective discussion of the current status of their family and their child’s adjustment, providing opportunities for parent’s discussion of hopes, need for change, as well as motivating engagement in a family assessment. The assessment phase includes brief questionnaires on child adjustment at home and school, parent adjustment, family context, and direct observations of parent-child interaction. All assessment data are automatically scored based on norms and summarized within a user-friendly “rainbow sheet” for easy interpretation by parents. The rainbow sheet summarizes the strengths and domains that need attention: Green suggests a domain, which is an area of strength (low alcohol use and substance use of parent); yellow suggests some concerns (marital satisfaction in the marginal range); and red suggests an area that needs attention. The feedback session focuses on parenting and family strengths and problem behaviors that were observed and linking the assessment to the parents’ original concerns.
Motivational interviewing is the key therapist skill used to engage caregivers in change talk with respect to parenting. The FCU is also a key strategy for motivating and engaging caregivers in more intensive parent management training, especially when contact with parents comes through service settings like services for Women, Infants and Children (WIC), pediatric care, and schools, situations in which parents are not requesting intervention services. The FCU is also a useful tool for parents when receiving children home for residential treatment (e.g., Slavet et al., 2005), or for parents in treatment with their own mental health or substance use concerns (e.g., Uebelacker, Hecht, & Miller, 2006), considering their caregiving practices and need for additional parenting supports. The FCU is especially helpful for engaging families in evidence-based parent management sessions, groups (e.g., Dishion, Stormshak, & Kavanagh, 2011), or other evidence-based interventions for the child or parent. For instance, if a family is concerned about the opposition behavior of their 7-year-old son, as well as the depression of their 16-year-old adolescent, intervention services might focus on parent management of problem behavior, as well as problem solving with adolescents and cognitive behavioral therapy for the adolescent within individual sessions. In this sense, the results of the family assessment guide as well as motivate engagement in services following the feedback session.
The FCU model has been most empirically tested within the context of randomized trials to young families engaged in WIC, public school settings in early adolescence, community mental health agencies, and emergency room (ER) settings (see Table 1 for summary). The strength of the model is the ability to use it within service settings with large populations of children and families not seeking treatment. However, the challenge of evaluating the preventative impact of the intervention is that many of the families served do not require large changes. Table 1 summarizes the results to longitudinal randomized studies published in peer review journals, with a focus on linking the FCU to the prevention of the development of future problem behaviors, as well as the mediation of change through improvements in social interaction in the family.
Table 1.
Intervention Outcome Studies for Family Check-Up
| Authors | Targeted Population | Sample Size | Length of Follow-up | Randomized Comparison Group | Measurement Strategies | Analytic Framework | Mediating Variable | Effect Size on DV |
|---|---|---|---|---|---|---|---|---|
| Dishion et al., 2002 | 90% of three public middle schools | 672 | 3 years | Controls (no intervention) | Student survey report of drug use | ITT | Small to medium | |
| Dishion et al., 2003 | 90% of three public middle schools | 72 | 3 years | Controls (no intervention) | Self-report drug use, observed monitoring at age 12 & 14 | ITT | Improved parental monitoring | Medium to large |
| Slavet et al., 2005 | Incarcerated adolescents | 10 | Immediate | N/A (feasibility trial) | Adolescents’ confidence in ability to resist drug use, parents’ confidence in ability to impact adolescents’ risky behaviors | N/A | Medium | |
| Shaw et al., 2006 | Children of families in WIC at risk for future conduct problems at age 2 | 120 | 3 years | Controls (no intervention) | Parent report child problem behavior, observed parenting | ITT | Improved parental monitoring | Medium |
| Uebelacker et al., 2006 | Community sample | 32 | 3 months | N/A (feasibility trial) | Parent report of family functioning and depression | N/A | Medium | |
| Connell et al., 2007 | 90% of three public middle schools | 998 | 5 years | Controls (no intervention) | Adolescent report, court records of youth drug use and problem behavior | ITT, CACE | Medium to very large | |
| Gardner et al., 2007 | Children of families in WIC at risk for future conduct problems at age 2 | 120 | 1 year | Controls (no intervention) | Observation of proactive parenting and parent report child problem behavior | ITT | Improved proactive parenting | Small |
| Connell et al., 2008 | Children of families in WIC at risk for future conduct problems at age 2 | 731 | 1 year | Controls (no intervention) | Parent report of externalizing and internalizing: co-morbidity | ITT | Small | |
| Connell & Dishion, 2008 | 90% of three public middle schools | 106 | 2 years | Controls (no intervention) | Adolescent report CDI depression | ITT, CACE | Medium to very large | |
| Dishion et al., 2008 | Children of families in WIC at risk for future conduct problems at age 2 | 731 | 3 years | Controls (no intervention) | Observation of parent positive behavior support and parent report child problem behavior | ITT | Improved positive behavior support | Small to medium |
| Connell, 2009 | 90% of three public middle schools | 998 | 11 years | Controls (no intervention) | Self-reported tobacco use | CACE | Small to very large | |
| Shaw et al., 2009 | Children of families in WIC at risk for future conduct problems at age 2 | 731 | 3 years | Controls (no intervention) | Parent report of child problem behavior maternal depression | ITT | Reduced maternal depressive symptoms | Small |
| Stormshak, Connell, & Dishion, 2009 | 90% of three public middle schools | 998 | 5 years | Controls (no intervention) | School records of attendance and grades for academic classes | CACE | Very large | |
| Stormshak et al., 2010 | 80% of three public middle schools | 377 | 4 years | Controls (no intervention) | Youth report of self-regulation (effortful control) | ITT | Improved self-regulation | Very small |
| Spirito et al., 2011 | Adolescents treated in an emergency department after an alcohol-related event | 125 | 1 year | Individual Motivational Interviewing for adolescent only | Youth report of alcohol use | ITT | Medium | |
| Stormshak et al., 2011 | 80% of three public middle schools | 593 | 2 years | Controls (no intervention) | Youth report of deviant peers, alcohol, and antisocial behavior | CACE | Large to very large | |
| Van Ryzin & Dishion, 2012 | 90% of three public middle schools | 998 | 7 years | Controls (no intervention) | Youth report conflict, antisocial behavior, deviant peers, and direct observation of family conflict | ITT | Reduced parent-child conflict | Medium to large |
| Fosco, Frank, Stormshak, & Dishion, 2013 | 80% of three public middle schools | 593 | 3 years | Controls (no intervention) | Youth report of self-regulation, antisocial behavior, drug use | ITT | Self-regulation | Very small |
| McEachern et al., 2013 | Children of families in WIC at risk for future conduct problems at age 2 | 435 | 3 years | Controls (no intervention) | Parent report of life satisfaction and child problem behavior | ITT | Reduced child behavior problems | Small |
| Caruthers, Ryzin, & Dishion, 2014 | 90% of three public middle schools | 998 | 5 years | Controls (no intervention) | Youth report of parent relationships, monitoring, high-risk sexual behavior and deviant peer involvement | ITT | Improved parent relationships and monitoring | Small |
| Chang, Shaw, Dishion, Gardner, & Wilson, 2014 | Children of families in WIC at risk for future conduct problems at age 2 | 731 | 5 years | Controls (no intervention) | Observation of parent positive behavior support and parent report inhibitory control | ITT | Increased inhibitory control | Small |
| Dishion et al., 2014 | Children of families in WIC at risk for future conduct problems at age 2 | 731 | 5 years | Controls (no intervention) | Parent and teacher report of problem behavior | ITT, CACE | Small to large | |
| Nelson, Van Ryzin, & Dishion, 2015 | 90% of three public middle schools | 998 | 12 years | Controls (no intervention) | Youth report of tobacco, cannabis, and alcohol use | ITT | Small to medium | |
| Sitnick et al., 2014 | Children of families in WIC at risk for future conduct problems at age 2 | 731 | 3 years | Controls (no intervention) | Observation of parent-child coercion and positive engagement at 2, 3, 4, and 5 years | ITT | Reduced parent-child coercion | Very small |
| Smith et al., 2014 | Combined two prevention trials in public middle schools | 1193 | 2 years | Controls (no intervention) | Youth report of ethnicity, family conflict, and antisocial behavior | ITT | Reduced family conflict | Small |
| Leijten et al., 2014 | Children of families in WIC at risk for future conduct problems at age 2 | 731 | 5 years | Controls (no intervention) | Parent report of service utilization at age 7 | ITT | Small | |
| Reuben, Shaw, Brennan, Dishion, & Wilson, 2015 | Children of families in WIC at risk for future conduct problems at age 2 | 731 | 6 years | Controls (no intervention) | Maternal report of depression and child behavior problems, observed coercion | ITT | Reduced maternal depressive symptoms | Very small |
| Veronneau, et al., in press | 90% of three public middle schools | 998 | 12–13 years | Controls (no intervention) | Self-reported tobacco, alcohol, and cannabis use | ITT, CACE | Medium to very large |
As shown in Table 1, the effect sizes of the FCU model with high-risk families involved in WIC range between small (i.e., for children’s inhibitory control) and large (parent reported oppositional and aggressive behavior). These studies also suggest improvements in family involvement (Shaw, Dishion, Supplee, Gardner, & Arnds, 2006) with high-risk families living in a large metropolitan area (N = 120, 2-year-old males only). Similarly, a larger prevention trial (N = 731, males and females) involving three unique communities (suburban, rural, and metropolitan) also screened as at risk within WIC revealed moderate effect sizes in the reduction of problem behavior between ages 2 and 4, and these effects were mediated by improvements in positive behavior support (Dishion et al., 2008). A follow-up study of the 2-year-olds to age 7.5 revealed that teachers reported intervention youth to be less oppositional in school, parents continue to rate fewer behavior problems, and effect sizes increased from small to large, depending on the number of years participants engaged in the yearly FCU intervention service (Dishion et al., 2014).
In an intensive analysis of observed family interaction as a mediator of long-term outcomes, Sitnick et al. (2014) found that long-term reductions in children’s aggressive and oppositional behavior was mediated by yearly improvements in parents’ observed positive behavior support as well as coercive conflict. Finally, Shaw also found moderate effects on reductions in maternal depression in early childhood, in both studies (Shaw et al., 2006; Shaw, Connell, Dishion, Wilson, & Gardner, 2009). It is worth noting that similar effect sizes were observed in the first study by Shaw and colleagues (Shaw et al., 2006) as the larger multisite trial, yet the latter study also offered follow-up parent training sessions for 70% of the families. In addition, we found that coercive family interactions in the WIC families did not change, unless they were provided with videotaped feedback on their interaction practices (Smith et al., 2014). These findings suggest that the FCU model on its own, without parent management training, may have limitations with respect to improving more entrenched, coercive family interaction dynamics. Videotaped feedback and rehearsal are key components of several versions of parent management training (Forgatch & Patterson, 2010; Zisser & Eyberg, 2010).
The results to two independent randomized trials in public middle school involve young adolescents and their families representing over 90% of the school population in high-risk neighborhoods (summarized in Table 1). The first (Dishion & Kavanagh, 2003) involved 998 sixth-grade students who were randomized to middle school as usual, versus middle school with family support. Family support was offered at multiple levels, with the FCU as the selected intervention delivered within a Family Resource Center in the school building. As shown in Table 1, we found that at age 14, random assignment of the high-risk students to receive the FCU showed reductions in drug use from ages 11 to 14 (Dishion, Kavanagh, Schneiger, Nelson, & Kaufman, 2002). In this study, we developed an observational measure of parent monitoring. Between the ages of 12 and 14, improvements in observations of parent monitoring significantly mediated intervention effects on adolescent drug use (Dishion, Nelson, & Kavanagh, 2003). Youth were followed to age 26–27, and we recently reported reductions in marijuana, alcohol, and tobacco use (Véronneau, Dishion, Connell, & Kavanagh, in press). In this study, both intention to treat (ITT) and complier average causal effect (CACE) modeling (Jo, 2002) were used. In the ITT framework, 12-year follow-ups showed reduced use of marijuana. When engagement in the FCU was incorporated into the prevention models, moderate effects were found for reductions in young adult alcohol, marijuana, and tobacco use.
Van Ryzin and Dishion (2012) examined the long-term effects of the FCU model on antisocial behavior by age 18–19 using youth report as the outcome. Like above, an ITT effect was found on the reduction of antisocial behavior from ages 11 to 18 (small effect size), and both self-reported and observed conflict mediated the long-term changes in adolescence.
Based on the initial positive results on parent monitoring and substance use, a new randomized trial was initiated in public middle schools to replicate and extend the findings. In this study, 593 ethnically diverse sixth-grade students were randomly assigned to the FCU or middle school as usual (see Stormshak, Fosco, & Dishion, 2010; Stormshak et al., 2011). In this study, the only intervention activity was the FCU, and the potential for follow-up parent training sessions and universal classroom-based family supports were not provided. In this trial, an effort was made to match the ethnicity of the parent consultant with that of the families to increase engagement. Engagement was increased from 25% to 38% (Stormshak et al., 2010). An analysis of FCU engagement using CACE modeling revealed statistically reliable reductions in antisocial behavior, deviant peer involvement, family conflict, and alcohol use (Stormshak et al., 2011; Van Ryzin & Dishion, 2012).
A study of the FCU model as implemented in a community mental health setting was studied by randomizing 40 therapists to being trained in the FCU model, and then following up with their clients and comparing those to therapists without such training. This study reports reductions in conduct problems among youth with therapists trained in the FCU (Smith, Stormshak, & Kavanagh, 2014).
Finally, in a randomized trial of motivational interviewing with 125 adolescents admitted to the ER for alcohol-related issues, youth were randomized to individual motivational interviewing, or individual motivation interviewing with an FCU (Spirito et al., 2011). The FCU condition was implemented in the home setting following the ER admission. Examining outcomes over three follow-up probes include 3, 6, and 1 year. Both conditions resulted in reductions in drinking, and the addition of the FCU was linked to reductions in “high volume” drinking at the 3-month follow-up probe, over and above motivational interviewing with the adolescent.
PARENT MANAGEMENT TRAINING–OREGON MODEL (PMTO)
PMTO is the core intervention underlying all of the Oregon models, originally summarized by Patterson and colleagues (Patterson & Reid, 1975) and tested using a randomized comparison sample (Patterson et al., 1982). This family of evidence-based programs ranges in focus from preventive interventions with at-risk samples to clinical treatment for serious behavior problems for youngsters from preschool through adolescence. In PMTO programs, parents serve as the primary agents of change; thus, therapists focus their efforts on parents rather than working directly with the children, although children are included in sessions as relevant. Programs focus on preventing or reducing outcomes related to youngsters’ externalizing and internalizing behavior problems, including antisocial, academic, and conduct problems; delinquency; and depression. Children’s mental health systems employ PMTO to address these issues. Because the programs intervene primarily with parents to decrease coercive parenting and increase positive parenting practices, PMTO interventions are also provided by the child welfare system for birth parents whose children have been removed for abuse/neglect (for reviews, see Forgatch & Domenech Rodríguez, 2015; Forgatch & Patterson, 2010; Forgatch, Patterson, & Gewirtz, 2013).
The iterative process employed by the OSLC group integrating theory has led to an expansion of the basic set of behavioral principles. The earliest programs focused on contingent positive reinforcement, negative sanctions for misbehavior, and careful tracking of specific behaviors. In the 21st century, the core components of PMTO programs comprise skill encouragement (also called contingent positive reinforcement), limit setting/discipline (also called negative sanctions), monitoring/supervision (an expansion of tracking), interpersonal problem solving, and positive involvement. An additional set of skills empowers these core components. These supporting skills include: clear directions, emotion identification and regulation, and communication skills. All intervention components are strength-based in that therapists help parents recognize and build on positive qualities already present in their families. For a more detailed description, see Forgatch and Domenech Rodríguez (2015).
PMTO can be delivered in a variety of formats: individual family treatment delivered in families’ homes or in agency settings, parent groups in agency or community settings, and telehealth delivery by phone or video. The number of sessions averages 25 individual family sessions for clinical cases; parent groups and telehealth sessions range from 6 to 14 sessions. Typical procedures call for weekly meetings with a midweek call to troubleshoot issues with home practice assignments.
One aspect that may differentiate PMTO from other parent training approaches is an emphasis on clinical change skills of the therapist to reduce resistance to change. This emphasis grew out of a series of studies conducted during the 1980s in which video recordings of therapy sessions were scored using an observational system that coded exchanges between therapists and families (Patterson & Chamberlain, 1988; Patterson & Forgatch, 1985; Stoolmiller, Duncan, Bank, & Patterson, 1993). Findings indicated that both client characteristics and therapist behavior may evoke client resistance. For example, when therapists teach or confront parents, they increase the likelihood that the client’s next response will be resistant; when they combine teach with confront, resistance increases sevenfold (Patterson & Forgatch, 1985). This finding led to efforts to shape clinical processes to provide more support and to replace didactic teaching by engaging parents in the teaching/learning process, consistent with motivational enhancement strategies applied to substance use treatment (Miller & Rollnick, 2002). In sessions we actively engage parents in the teaching-learning process through the use of role-play and interactive problem solving. For a brief review of the therapy process studies and their incorporation into the intervention, see Forgatch and Domenech Rodríguez (2015).
Outcomes for PMTO prevention and treatment programs are based on randomized controlled trials, multiple-method and -agent assessment, and follow-up periods from 1 to 9 years (see Table 2 for a summary). Benefits have been reported for the youngsters and for the parents, mediated by observed changes in key family interaction dynamics. Positive outcomes for youngsters include the following: reductions in observed noncompliance, deviant behavior, family aggression, and playground aggression; fewer police reports of nonstatus offenses; reduction in early police arrests; less growth in number of police arrests and less time incarcerated; teacher ratings of improved adaptive functioning in school and reduction in delinquency; and reduced self-reported depression, deviant peer association, tobacco use, and illicit drug use. See Forgatch and Patterson (2010) for details of these studies.
Table 2.
Intervention Outcome Studies for Parent Management Training, Oregon
| Authors | Targeted Population | Sample Size | Length of Follow-up | Randomized Comparison Group | Measurement Strategies | Analytic Framework | Mediating Variable | Effect Size on DV |
|---|---|---|---|---|---|---|---|---|
| Amlund Hagen et al., 2011 & Ogden & Amlund Hagen, 2008 | Families in Norway with child ages 4–12 displaying at least onecf disruptive behavior disorder symptom, recruited to the study via existing child services agencies | 112 | 12 months | Controls (treatment as usual) | Observed parental discipline, teacher ratings of social skills, parent ratings of externalizing behavior | ITT | Effective discipline, family cohesion | Small to medium |
| Kjøbli, Hukkelberg, & Ogden, 2013 | Families in Norway with child ages 3–12 either at an early-stage / developed conduct problems, recruited from those who had contacted an agency for these issues | 137 | 6 months | Controls (treatment as usual) | Self-reported parenting practices, parent and teacher ratings of social competence | ITT | N/A | Small to large |
| Kjøbli & Bjørnebekk, 2013 | Families in Norway with child ages 3–12 either at an early-stage / developed conduct problems, recruited from those who had contacted an agency for these issues | 216 | 6 months | Controls (treatment as usual) | Self-reported parenting practices, externalizing behavior | ITT | N/A | Small to medium |
| Bjorknes et al., 2012 | Somali and Pakistani immigrant families in Norway with child ages 3–9 at risk for the development of conduct problems | 96 | Pre-Post | Controls (wait-list) | Self-reported parenting practices, externalizing behavior | ITT | Harsh discipline, positive parenting | Small to medium |
| Sigmarsdóttir, Thorlacius, Guðmundsdóttir, & DeGarmo, 2015 | Families in Iceland with child ages 5–12 displaying current behavior problems at school or home | 102 | Pre-Post | Controls (treatment as usual) | Child adjustment construct using child, parent, and teacher reports | ITT | N/A | Small to medium |
| Sigmarsdóttir & Björnsdóttir, 2012 | A community in Iceland | ~930 | 10 years | N/A (quasi-experimental) | Referrals for services | N/A | N/A | Small to medium |
| Parra-Cardona et al., 2012 | Two-parent families recruited from the community | 24 | Pre-Post | N/A (qualitative analysis) | Engagement, retention, satisfaction | N/A | N/A | N/A |
| Gewirtz & Taylor, 2009 | Mothers and children residing in shelters or transitional housing | 10 | Pre-Post | N/A (feasibility trial) | Engagement, retention, satisfaction | N/A | N/A | N/A |
| Gewirtz et al., 2015 | Formerly homeless families in supportive housing settings | 161 | 2 years | Controls (treatment as usual) | Parent self-efficacy, observed parenting, child self-report of depression, teacher and parent report of child strengths | ITT | N/A | Medium to large |
| Wieling et al., 2015 | Ugandan mothers drawn form a larger observational study and reporting significant difficulty parenting at least one child | 14 | 5 months | N/A (feasibility trial) | Engagement, retention, satisfaction, observed positive parenting, self-reported discipline practices | N/A | N/A | Medium |
| Gewirtz et al., 2014 | Families with a child ages 4–12 and at least one parent who had deployed recently (i.e., Iraq or Afghanistan) | 42 | Pre-Post | N/A (feasibility trial) | Participation, satisfaction | N/A | N/A | |
| Forgatch et al., 2005 | Recently married biological mother and stepfather families with child in grades K-3, recruited from community | 110 | 24 months | Controls (no intervention) | Observed parenting practices, parent report of home behavior, teacher report of internalizing and externalizing behavior | ITT | Parenting practices, noncompliance, home behavior | Medium to large |
| DeGarmo & Forgatch, 2007 | Recently married biological mother and stepfather families with child in grades K-3, recruited from community | 111 | 25 months | Controls (no intervention) | Observed stepfather parenting | ITT | N/A | Medium |
| Bullard et al., 2010 | Recently married biological mother and stepfather families with child in grades K-3, recruited from community | 112 | 26 months | Controls (no intervention) | Observed parenting practices, observed marital relationship, self-reported marital satisfaction | ITT | Observed parenting practices | Medium |
| Wachlarowicz, Snyder, Low, Forgatch, & DeGarmo, 2012 | Recently married biological mother and stepfather families with child in grades K-3, recruited from community | 113 | 27 months | Controls (no intervention) | Coercive and positive parenting | ITT | N/A | Small to medium |
| Forgatch & DeGarmo, 2007 | Recently separated single mothers and their sons in grades 1–3, recruited from the community | 238 | 30 months | Controls (no intervention) | Rise out of poverty, financial stress, income-to-needs ratio | ITT | Income-to-needs ratio | Small to medium |
| Martinez & Forgatch, 2001 | Recently separated single mothers and their sons in grades 1–3, recruited from the community | 238 | 30 Months | Controls (no intervention) | Observed parenting practices, observed noncompliance | ITT | Positive parenting, coercive discipline | Small to medium |
| Forgatch et al., 2009 | Recently separated single mothers and their sons in grades 1–3, recruited from the community | 238 | 9 years | Controls (no intervention) | Observed parenting practices, teacher report of delinquency, self-reported deviant peer association, (early) arrests | ITT | Deviant peer association | Small to medium |
| DeGarmo et al., 2004 | Recently separated single mothers and their sons in grades 1–3, recruited from the community | 238 | 30 months | Controls (no intervention) | Observed parenting practices, teacher report of externalizing and internalizing behavior, maternal depression | ITT | Child externalizing and internalizing problems | Small to medium |
| Forgatch & DeGarmo, 1999 | Recently separated single mothers and their sons in grades 1–3, recruited from the community | 238 | 12 months | Controls (no intervention) | Observed parenting practices, teacher and child report of school adjustment | ITT | Effective parenting | Small to medium |
| Chamberlain et al., under review | Families served by private agencies in child welfare system | ~2000 | Pre-Post | N/A (quasi-experimental) | Reunification, placement stability | N/A | N/A | Small |
| Akin et al., 2014 | Families swith a child with severe emotional disturbance in foster care | 60 | Pre-Post | Controls (treatment as usual) | Attrition, reunification | ITT | N/A | N/A |
Benefits for parents include the following: reductions in observed coercive parenting and ineffective discipline, increased or sustained positive parenting practices, improved marital interaction, self-reported rise out of poverty, increased per capita annual income, increased socioeconomic status (education, occupation, income), decreased maternal depression, increased marital satisfaction, and fewer police reports of arrests (Bullard et al., 2010; DeGarmo, Patterson, & Forgatch, 2004; Forgatch & DeGarmo, 2007; Forgatch & Patterson, 2010; Patterson, Forgatch, & DeGarmo, 2010).
Several studies conducted ITT mediational modeling to test the theoretical perspective that the mechanisms of change are reduction in coercion and improved positive parenting practices. The findings have supported the hypothesis. Intervention benefits to parenting practices mediated intervention effects on youth and maternal police arrests, teacher-reported delinquency, children’s reports of depression and drug and tobacco use, parents’ reports of maternal improvements in SES, and observations of quality of marital interaction (Bullard et al., 2010; DeGarmo, Eddy, Reid, & Fetrow, 2009; DeGarmo & Forgatch, 2007; DeGarmo et al., 2004; Forgatch, DeGarmo, & Beldavs, 2005; Forgatch, Patterson, DeGarmo, & Beldavs, 2009; Patterson et al., 2010). An analysis of the divorce study with 9 years of data tested the model using longitudinal sequencing of the constructs and found that intervention effects on reducing coercive parenting from baseline to 1 year mediated the intervention effects on growth in positive parenting from 1 year to 3 years; growth in positive parenting served as the most proximal mediator for benefits to child outcomes (i.e., reduced number of police arrests and teacher ratings of delinquency) and benefits to socioeconomic status (Forgatch, Beldavs, Patterson, & DeGarmo, 2008).
The PMTO preventive approach has been adapted for a wide variety of contexts and cultures within the U.S., including mothers living in supportive housing (Gewirtz, DeGarmo, Lee, Morrell, & August, 2015) and shelters because of domestic violence or homelessness (Gewirtz, 2007; Gewirtz & Taylor, 2009), military staff reintegrating home from war (Gewirtz, Pinna, Hanson, & Brockberg, 2014), Latino immigrant families (Parra-Cardona et al., 2012), step-families (Forgatch et al., 2005), single mothers (Forgatch & DeGarmo, 1999), and families living in high crime neighborhoods (Reid, Eddy, Fetrow, & Stoolmiller, 1998).
The late 1990s marked the beginning of wide-scale PMTO implementations. The first site, Norway, set the stage for the manner in which the PMTO purveyor group conducts implementations. The approach that was developed is full transfer to the adopting community, in which a fully trained implementation site becomes licensed to conduct the program independently within its site, training their own clinicians, coaches, trainers, and fidelity raters (see Forgatch et al., 2013). To ensure sustained fidelity to the model, each site maintains a team of fidelity raters who are trained to reliability on the Fidelity of Implementation Rating System (FIMP; Knutson, Forgatch, Rains, & Sigmarsdóttir, 2009). Reliability is maintained with monthly reliability checks within the site’s team and an annual reliability test with scores provided by the purveyor fidelity team. This approach has resulted in extending the reach of the program within sites. A study of effect sizes across generations of PMTO practitioners in Norway following scale-up several years after the original implementation shows sustained fidelity to the model and maintenance of effect sizes in outcomes (Tømmeraas & Ogden, 2015). In the 15 years since the Norwegian implementation, they have tailored the program to extend its reach with adaptations for use within the health care system, ethnic minority groups, and other preventive applications. Each adaptation has been tested with an RCT (see Amlund Hagen, Ogden, & Bjørnebekk, 2011; Bjørknes, Kjøbli, Manger, & Jakobsen, 2012; Kjøbli & Bjørnebekk, 2013; Kjøbli, Hukkelberg, & Ogden, 2013; Kjøbli & Ogden, 2012; Ogden & Amlund Hagen, 2008).
Other wide-scale PMTO implementations include the following: statewide programs within the child mental health system in Michigan; a statewide program within child welfare in Kansas; city/countywide programs in Detroit/Wayne County, Michigan; and nationwide in Iceland, The Netherlands, and Denmark. Mexico City conducted a small RCT, and a pilot program is under way in Northern Uganda. A program for birth parents in the child welfare system in New York City is ongoing in collaboration with KEEP for the foster parents (Chamberlain, Feldman, Wulczyn, Saldana, & Forgatch, 2015). See Forgatch and Domenech Rodríguez (2015) and Forgatch et al. (2013) for more information on implementations.
TREATMENT FOSTER CARE–OREGON MODEL (TFCO)
The TFCO model (formerly Multidimensional Treatment Foster Care) was specifically designed to address the needs of families and youth with serious problem behavior and correlated family disruption and dissolution. Specifically, TFCO focuses on children and adolescents who have been removed or are slated to be removed from their family homes because of serious antisocial behavior (by juvenile justice), severe emotional problems (mental health systems), or because of having experienced severe child abuse and neglect (child welfare systems). Versions of TFCO have been developed for preschoolers in foster care (TFCO-P; Fisher, Stoolmiller, Mannering, & Chamberlain, 2011), latency age children (TFCO-C; Smith, Stormshak, Chamberlain, & Bridges Whaley, 2001), and adolescents (TFCO-A; Chamberlain, 2003). In addition, the model was expanded to provide preventive services to regular state foster care homes in child welfare systems to stem the tide of foster care placement disruptions and increase child well-being outcomes. The preventive version of TFCO is called KEEP (keeping foster and kinship parents supported and trained). KEEP, described in detail elsewhere (Chamberlain, Price, Leve, Laurent, Landsverk, & Reid, 2008), contains the core elements of TFCO, yet is less intensive and costly to implement.
In TFCO, youth are placed singly in specially trained and supported foster homes as an alternative to congregate care settings. For adolescents, TFCO-A serves as an alternative to group homes, residential correctional settings, or inpatient residential treatment. For younger children, TFCO-C serves as an alternative to regular foster care for preschoolers with behavior/mental health problems (TFCO-P). Foster parents are intensively trained, supervised, and supported to provide positive adult support, nurturing and mentoring, close supervision, and consistent limit setting. TFCO placements typically last 6 to 9 months and involve coordinated interventions in the home, with peers, in educational settings, and with the youth’s biological family members or other long-term placement resource. Close consultation, training, and support of the foster parents form the cornerstone of the TFCO model. Program supervisors with small caseloads (10 families each) maintain daily contact with TFCO parents to collect data on youth adjustment and to provide ongoing consultation, support, and crisis intervention. Many of the youth served have unfortunately developed advanced skills in undermining adult efforts to set healthy limits and monitor daily activities. In TFCO, daily consultations that are data-based and supportive provide a critical venue for problem- solving strategies to socialize youth into more healthy lifestyles (e.g., attending school, doing homework, chores, participating in family activities, and reducing unsupervised time with peers).
The basic components of the model include: (a) daily (M–F) telephone contact with foster parents using the Parent Daily Report checklist (PDR; Chamberlain & Reid, 1987); (b) weekly foster parent group meetings led by the program supervisor focused on supervision, training in parenting practices, and support; (c) an individualized behavior management program implemented daily in the home by the foster parent; (d) individual therapy for the youth, (e) individual skills training/coaching for the youth; (f) PMTO-informed family therapy (for biological/adoptive/relative family of the youth) focused on parent management strategies; (g) close monitoring of school attendance, performance, and homework completion; (h) case management to coordinate the TFCO family, peer, and school settings; (i) 24-hour on-call staff availability to foster and biological parents; and (j) psychiatric consultation as needed. Like the FCU and PMTO models, the TFCO intervention embodies a strong focus on strength-building and positive reinforcement, and specific intervention components are tailored to the child’s age and developmental level. Additional information on the basic TFCO model is described in detail elsewhere (Chamberlain, 2003).
TFCO-A trials (see Table 3 for summary) in the U.S. have indicated its effectiveness in reducing arrest rates and deviant peer affiliations for boys and girls, placement disruption and parenting for boys, and pregnancy rates and school engagement for girls (Chamberlain & Reid, 1998; Kerr, Leve, & Chamberlain, 2009; Leve, Fisher, & Chamberlain, 2009). For example, between baseline and a 12-month follow-up, TFCO youth had spent 53 (boys) and 22 (girls) days in lockup (e.g., a detention facility), whereas control youth had spent 129 and 56 days, respectively; and in the 24 months following baseline, 26.9% of TFCO girls had a new pregnancy vs. 46.9% of control girls. International replication trials of TFCO have also shown positive results. A trial in Sweden indicated significant reductions in youth-reported externalizing and internalizing behavior relative to the treatment services-as-usual (TAU) control group (Westermark, Hansson, & Olsson, 2010). Depression scores were twice as high for TAU control youth as compared to TFCO-A youth at the 2-year follow-up. A recent 3-year follow-up in Sweden found that compared to youth assigned to TAU, those in TFCO-A spent two-thirds fewer days in locked settings and had significantly lower rates of violent crime (Bergström & Höjman, 2015).
Table 3.
Intervention Outcome Studies for Treatment Foster Care, Oregon
| Authors | Targeted Population | Sample Size | Length of Follow-up | Randomized Comparison Group | Measurement Strategies | Analytic Framework | Mediating Variable | Effect Size on DV |
|---|---|---|---|---|---|---|---|---|
| Leve, Chamberlain, & Reid, 2005 | Girls referred by juvenile court judges for out-of-home care due to chronic delinquency | 81 | 12 months | Control (treatment-as-usual: group care setting) | Days in locked settings, recidivism and criminal activity | ITT | N/A | Small to medium |
| Leve & Chamberlain, 2005 | Male and female adolescents referred by juvenile court judges for out-of-home care due to chronic delinquency | 153 | 12 months | Control (treatment-as-usual: group care setting) | Delinquent peer affiliations | ITT | Delinquent peer association during intervention | Small |
| Leve & Chamberlain, 2007 | Female adolescents referred by juvenile court judges for out-of-home care due to chronic delinquency | 81 | 12 months | Control (treatment-as-usual: group care setting) | School attendance, homework completion | ITT | N/A | Small |
| Chamberlain, Leve, & DeGarmo, 2007 | Female adolescents referred by juvenile court judges for out-of-home care due to chronic delinquency | 81 | 24 months | Control (treatment-as-usual: group care setting) | Delinquency, criminal referrals, days in locked settings | ITT | N/A | Small to medium |
| Kerr et al., 2009 | Female adolescents referred by juvenile court judges for out-of-home care due to chronic delinquency | 166 | 24 months | Control (treatment-as-usual: group care setting) | Pregnancies | ITT | N/A | Medium |
| Harold et al., 2013 | Female adolescents referred by juvenile court judges for out-of-home care due to chronic delinquency | 166 | 24 months | Control (treatment-as-usual: group care setting) | Depressive symptoms and diagnosis | ITT | N/A | Small to medium |
| Poulton et al., 2014 | Female adolescents referred by juvenile court judges for out-of-home care due to chronic delinquency | 166 | 24 months | Control (treatment-as-usual: group care setting) | Psychotic symptoms | ITT | N/A | Medium |
| Fisher, Gunnar, Chamberlain, & Reid, 2000 | Children referred for placement in foster home by child welfare system because of one or more placement disruptions and/or highly disruptive behavior | 30 | 3 months | N/A (pilot study) | Parenting strategies, parent/foster stress, child behavior problems and salivary cortisol levels | N/A | N/A | Medium to large |
| Eddy & Chamberlain, 2000 | Male adolescents referred by juvenile court judges for out-of-home care due to chronic delinquency | 79 | 24 months | Control (treatment-as-usual: group care setting) | Antisocial behavior construct | ITT | Family management skills, deviant peer association | Medium |
| Chamberlain, Moreland, & Reid, 1992 | Children placed in foster care for at least three months | 72 | 24 months | Control (treatment-as-usual) | Retention of foster families, disruption in placements, child behavior problems, staff impression of parenting practices | ITT | N/A | Small to medium |
| Chamberlain & Reid, 1998 | Male adolescents referred by juvenile court judges for out-of-home care due to chronic delinquency | 79 | 12 months | Control (treatment-as-usual: group care setting) | Official records and self-report of criminal referrals, reunification with family members days in locked settings | ITT | N/A | Medium to large |
| Chamberlain et al., 2008 | Children being placed in foster care for the first time, being moved due to disruptive behavior, or returning to foster care from another setting | 700 | 5 months | Control (treatment-as-usual) | Child behavior problems, positive reinforcement practices by parents | ITT | N/A | Small |
| Rhoades, Leve, Harold, Kim, & Chamberlain, 2014 | Female adolescents referred by juvenile court judges for out-of-home care due to chronic delinquency | 166 | 9 years | Control (treatment-as-usual: group care setting) | Self-report of illicit drug use | ITT | N/A | Small to medium |
| Smith et al., 2012 | Female adolescents referred by court for out-of-home care due to chronic delinquency, with at least one traumatic experience | 30 | 12 months | Control (treatment-as-usual: group care setting) | Trauma-related mental health symptoms, delinquency, days spent in locked settings | ITT | N/A | Medium |
| Smith, Chamberlain, & Eddy, 2010 | Male adolescents referred by juvenile court judges for out-of-home care due to chronic delinquency | 79 | 18 months | Control (treatment-as-usual: group care setting) | Adolescent self-report of drug and alcohol use | ITT | N/A | Small to medium |
For children experiencing abuse and neglect, there is a myriad of cascading effects, including attenuated attachment and trust of adults, stress reactivity, as well as the potential for repeated placements in caregiving environments. As discussed above, progression in mental health and problem behavior symptoms is a linear function of repeated changes and failures in the caregiving environment. TFCO-P has been shown to produce positive attachment outcomes: Children in the intervention condition showed increases in secure behavior and decreases in avoidant behavior relative to children in regular foster care services, with small effect sizes; children in TFCO-P had a 10% increase in rates of secure behavior over a 12-month period, whereas control children had a 6% decrease in secure behavior over the same time period (Fisher & Kim, 2007). In addition, TFCO-P outcomes include significant influences on stress response systems: the intervention effectively prevented TFCO-P children from having blunted diurnal HPA axis function, with medium effect sizes (Fisher, Stoolmiller, Gunnar, & Burraston, 2007) and produced reductions in caregiver stress (Fisher & Stoolmiller, 2008). Further, the intervention improved placement stability outcomes across a 2-year period and mitigated the risk of multiple prior foster care placements on children’s subsequent placement failures (Fisher, Burraston, & Pears, 2006). Compared to TFCO-P children, children receiving regular foster care services were not only 3.6 times more likely to have a permanent placement failure, but children with three or more prior placement failures were at a heightened risk of a permanent placement failure. The probability of a failed permanent placement was approximately three times larger for children in the control condition.
Each of the interventions described here emphasizes the important role of caregiving adults in supervising, nurturing, and managing child and adolescent behavioral, emotional, and functional adjustment. In the case of TFCO, foster parents are in the critical role of providing this support and skill building. Mediational modeling studies have been conducted to verify the theoretical perspective underlying the TFCO model and to demonstrate that specific TFCO program elements act as drivers or mechanisms of change on major intervention targets. For example, Eddy and Chamberlain (2000) found that association with delinquent peers and the availability of parents as supports and mentors predicted subsequent levels of youth delinquent and antisocial behavior regardless of intervention condition (TFCO-A experimental or Group Care control). That is, those youth who were prevented from hanging out unsupervised with delinquent peers and who experienced positive parenting had significantly lower levels of delinquency in follow-up. Unsupervised time with peers occurred less frequently for the youth TFCO-A model than for those in the Group Care (control group) setting, and youth in TFCO-A spent higher quality and more time with mentoring adults. These components partially (and significantly) accounted for the positive treatment effects observed for youth placed in TFCO-A relative to those placed in Group Care settings.
In another example, Leve and Chamberlain (2007) found that girls in TFCO-A spent more time doing homework than girls in Group Care during treatment and that this homework time and school engagement scores significantly predicted the number of days girls spent in locked settings 12 months postbaseline. In other words, keeping girls engaged in school prevented additional criminal behavior and therefore time incarcerated in follow-up.
The TFCO began being implemented in the U.S. and in Europe in the early 1990s (see www.TFCO.com for a list of sites). Large-scale implementations with multiple TFCO sites have occurred in England, Sweden, and New York City. In 2000, we partnered with the California Institute for Mental Health (CIMH) to decrease the number of children and adolescents placed in group home settings in California. Group home placements had been shown to be expensive and to result in poor outcomes (Marsenich, 2002). CIMH obtained foundation funding to pay for 10 counties to receive training in TFCO as an alternative to placing youth in-group homes. Our experiences working with these counties, who were well resourced and experienced with innovation, encouraged us to think about how we could engage and motivate non–early adopting counties to implement. At the same time, CIMH was looking for ways to provide technical assistance and support to counties implementing EBPs with the goal of increasing the reach, fidelity, and sustainability of EBPs in California. To do this, they developed a peer-to-peer learning model called the Community Development Team (CDT). The CDT operates through multicounty development team meetings where a group of six to seven counties share experiences and engage in problem solving about implementation barriers together. Key stakeholders from each of the counties participate in CDT meetings. Stakeholders are drawn from multiple levels (system leaders, organization/agency directors, practitioners) to participate in the CDT meetings (Sosna & Marsenich, 2006). Next, with funding from NIMH, we tested the effectiveness of implementing TFCO using the CDT model compared to “implementation as usual” (with counties implementing TFCO singly) in 51 counties in California and Ohio. Counties were randomly assigned to implementation condition (CDT or implementing singly). We found that CDT had advantages in that it resulted in the eventual placements of more than double the number of youth in to TFCO programs (Brown et al., 2014).
An Integrative Public Health Framework
As the science of behavioral family interventions improved over the past four decades, there was a gradual increase in the demand for implementing in real-world service settings with a focus on reducing problem behavior. This transition from program development to real-world implementation, however, has been a serious challenge for the field in general. For example, it is estimated that about 10% of the providers in settings that serve children and families are adopted with the fidelity intended by the original program developers (O’Connell, Boat, & Warner, 2009; Biglan, 2015). Based on our research as well as that of the field, we suggest progress for large-scale reductions in the prevalence of child and adolescent problem behavior (antisocial behavior, substance use, delinquency, and violence) will benefit from deep integration of family-based prevention and treatment strategies in the context of child welfare, juvenile justice, and the public education system. We suggest the application of three basic behavioral science principles that could be applied to this end.
The first is the contagion principle, which specifies that children and adolescents often escalate problem behaviors in the company of peers in settings without skillful adult leadership (Dishion & Tipsord, 2011, for review). Direct observations of children on the public school playground as early as age 5 (Snyder et al., 2006) as well as within adolescent friendships (Dishion & Patterson, 1996) revealed a process of deviancy training involving peer reinforcement for deviant talk that leads to escalations in problem behavior and violence (see Dishion, in press; Piehler, in press). A lack of awareness of the contagion principle can lead to the unfortunate outcome of spending resources on programs and intervention strategies that inadvertently increase the problem behaviors that potentially undermine youth development (see Dodge, Dishion, & Lansford, 2006, for a review).
The contagion principle is most compelling when considering conventional rehabilitation strategies within juvenile justice and child welfare. For example, in studies reviewed above, the effectiveness of TFCO-A in reducing repeat offending among multiple offenders was mediated by youths’ exposure to unsupervised peer settings in group homes and residential treatment (see Leve & Chamberlain, 2005). This finding is consistent with early work on juvenile correction facilities, showing the ratio of positive reinforcement of peers compared to adults in the institution was 9 to 1 (Buehler, Patterson, & Furniss, 1966). It is challenging in many residential settings to adequately establish an environment where the good intentions of staff compete with the tendency of youth in peer groups to reinforce and learn new forms of problem behavior. Careful longitudinal studies that collected data on children before they committed offenses have confirmed suspicions that juvenile correction facilities (institutions, lock ups, group homes) do more harm than good. For example, research by Gatti, Tremblay, and Vitaro (2009) following youth in the Montreal prevention trial revealed that there was an iatrogenic effect of juvenile correction facilities, in that youth who spent time in juvenile corrections were more likely to reoffend with serious offenses in adulthood, controlling for their differences in their problem behavior in adolescence. Moreover, systematic studies of youth in Florida juvenile corrections revealed youth tended to reoffend with the same crime as their inmate peers after released, controlling for their behavior at entry (Bayer, Hjalmarsson, & Pozen, 2009). Clearly youth learn behaviors within institutions that contribute to the chronicity of their problem behavior, which further undermines opportunities for dropping out of criminal behavior as well as drug-using and selling lifestyles.
In this sense, larger units (e.g., states) are in a position of reducing and possibly eliminating expensive residential facilities that aggregate high-risk youth in public schools, child welfare, and juvenile justice. Correctional facilities would be needed far less if more effective family-centered prevention and intervention strategies like FCU, PMTO, and TFCO were adopted. In the context of randomized trials these interventions find decreases in arrests, changes in placements, and reduced time in locked-down facilities through adolescence. Reduction of time in juvenile corrections predicts reduced time in the very expensive adult prison system.
The second principle is data-based monitoring and decision-making, a cornerstone of behavioral approaches to treatment in general, but behavior family therapy in particular (Chamberlain & Reid, 1998; Kolko, 1996). At a larger scale, optimizing organizational and community strategies for improving youth lives and reducing problem behaviors benefits from data-driven decision-making with periodic monitoring (see also Fixsen, Blase, Metz & Van Dyke, 2013; Mrazek, Biglan, Hawkins, & Cody, 2007). In our collective work, well-intentioned implementations may fail if the appropriate leadership structure is not in place. In an implementation study of the FCU model in 41 public middle schools, engagement of high-risk families within the public middle school context was not supported at the district level. Therefore, the efforts of school principals to monitor and support the use of parenting supports in schools went unnoticed, and therefore, often languished. A monthly report of the proportion of high-risk students with each school with family behavior support would likely improve leadership support as well as student outcomes (Dishion et al., under review). Alternatively, the experiences described above in Norway, Sweden, Michigan, California, and New York had strong leadership support, periodic monitoring of implementation outcomes, and accordingly, have progressed with respect to increasing the number of providers using the evidence-based practices as well as child outcomes.
The third key principle is shaping competent adherence to the evidence-based practices. Shaping involves the differential reinforcement for successive approximations of a skill, commonly used with clinical success in behavioral interventions. However, shaping is less often used in the context of professional development of advanced skill sets. The early work on client resistance described above suggested that the clinical skill of the provider is critical to the change process. Direct observations of therapists’ competent adherence in sessions predicts changes in parenting practices, which in turn predicts improvement in youth outcomes in both FCU and PMTO (Forgatch et al., 2013; Forgatch & DeGarmo, 2011; Smith et al., 2014). This finding has two implications. The first is that competent adherence requires motivation and effort of the provider, and as such, shaping successive approximations when coaching this skill set is critical to therapists becoming fluid in a behavioral model. If clinician competence is assumed or neglected through lack of training and support, effect sizes will suffer, especially working with families with children showing problem behavior (Ogden, Forgatch, Askeland, Patterson, & Bullock, 2005; Weiss, Catron, Harris, & Phung, 1999). Second, therapists and supervisors who use evidence-based practices benefit from professional support in terms of acknowledgement and salary for mastering a skill-set that is conducive to family change. Most evidence-based practices require more than a modicum of patience and skill to effectively deliver, as well as study, practice, role-play and openness to supervisory feedback. It is likely that the supervisory context is one among several pillars that support the implementation of evidence-based practices for children and families (Dishion & Stormshak, 2007) and these support systems need to be in place to deliver and sustain effective prevention and treatment services that are scientifically derived.
INTEGRATED FAMILY SUPPORT WITHIN PUBLIC SCHOOLS
So far we have reviewed a history of divergent development since the publication of Patterson, Chamberlain, and Reid (1982). Although the FCU, PMTO, and TFC-O arose within the Oregon group, the intervention models were tested and refined independently. At this juncture, it is beneficial to consider the benefits of integrating the models within one service system within a community to reduce the prevalence of problem behavior and to promote healthy development. The public school system is a promising venue for integration, as all children are ostensibly served and educated, despite their involvement in child welfare, juvenile justice, community mental health, and foster care.
At present, school district leadership typically adopt evidence-based intervention programs for high-risk children and families in an uncoordinated approach, and depending on the structure of the school district, each school can shop for the program that best fits the needs of the staff as well as the perceived needs of the students and parents. Often schools have multiple programs running at the same time. Therefore, school staff have difficulty tracking the procedures and processes of each evidence-based program. Staff meetings are often held in the “program graveyard,” including stacks of previously adopted and abandoned intervention programs, many of which are evidence based. The problem is not the availability of interventions that are evidence based, it is one of coordination of intervention strategies in such a way as to not disrupt the workflow of the educational environment.
To scaffold decisions on evidence-based adoption, training, and implementation, some alternative approaches have emerged. Exemplary is the PROSPER diffusion model for EBI’s for children and families (see Spoth, Redmond, Shin, & Azevedo, 2004). Within the PROSPER framework, the Cooperation Extension System (CES) serves as a venue for seed-funding initial efforts to initiate program adoption, training, and implementation over time, resulting in sustainable efforts to promote evidence-based family-centered prevention programs within schools. For example, the Strengthening Families parent groups were disseminated within schools within the CES venue and found to be a cost-effective prevention strategy (Crowley, Jones, Greenberg, Feinberg, & Spoth, 2012). However, this approach focuses purely on primary prevention within the context of public schools. Thus, universal support for parents is provided in parent groups that meet after school, often involving a select group of families willing to attend regularly. Despite the limited reach, this approach has been found to produce robust prevention effects on multiple forms of substance use (e.g., Spoth, Redmond, Hockaday, & Shin, 1996).
The focus on family support within school systems is synergistic to effective school practices such as Positive Behavior Intervention Support (Crone & Horner, 2003) or the Good Behavior Game (Poduska et al., 2008). Effective family support, however, requires engagement of families of high-risk students as well as integration into other student support services (Dishion, 2011). It is noteworthy that about 50% of the juvenile offences are committed by 5% of the youth and families (Farrington, Loeber, & Van Kammen, 1990). Similarly, the vast majority of the discipline contacts in schools involve only 5% to 10% of the student population (Crone & Horner, 2003). Invitations to parent groups are unlikely to engage the families most in need of services (Szapocznik et al., 1988). For example, in one community sample of youth, less than half of the persistent juvenile offenders had sought help by age 18 for the problem behavior, despite the long history of juvenile justice offenses and behavior problems in school and in the community (Stouthamer-Loeber & Loeber, 2002). By extension based on the prevalence of community service settings using EBIs (O’Connell, Boat, & Warner, 2009), less than 5% of the persistent juvenile offenders likely had exposure to an evidence-based family intervention. In this sense, the failure to coordinate and track youth within a public school venue means a lost opportunity for prevention and treatment. In this sense, it is precisely the highest risk youth who may slip through the cracks, eventually cascading to more serious levels of problem behavior.
THE AIM FAMILY SUPPORT SYSTEM
There is clear and dire need for an integrated approach to prevention and treatment of student problem behavior as well as emotional stress with family support in public schools. There are three functions that need to be addressed to provide effective support to the children and families on the risk continuum. The first is systematic and cost-effective assessment and screening. It is relatively simple to screen for antisocial behavior and emotional distress in children and adolescents. Several researchers have built on the multistage assessment strategies originally formulated by Cronbach and Gleser (1965). A multiple gating strategy was suggested (Loeber, Dishion & Patterson, 1984) and later refined for elementary school (Walker & Severson, 1990). In these multistage approaches, teachers and parents are administered brief screens to identify youth at low risk for problem behavior or persistent emotional distress (depression, anxiety). The remaining group is then reassessed by another agent (parent or teacher) and again, youth at low risk are screened out. This procedure of systematically ruling out low-risk youth is often referred to as multiple gating, and has shown to be quite effective in identifying a very small subgroup with high rates of problem behavior and substance use (Dishion & Patterson, 1993).
The second function of a family support system is to provide the appropriate level of intervention support for the youth and families. Although assessment protocols can be useful to identify those most in need of intervention support, it is often the case that the risk status of a family may change quickly. Thus a team of intervention staff is needed to navigate multiple risk needs of families (see Figure 2) and minimize the need for seeking referrals with agencies. In the most severe form of family disruption, treatment foster care may be necessary, providing youth with a safe and effective treatment context while also providing parenting support with the family caregivers. Rather than hope that there is an evidence-based treatment foster care service available, the integrated service team can respond without outside referrals.
The third function of an integrated service system is monitoring intervention progress and decreasing or increasing support based on response to the intervention (Fuchs & Fuchs, 2006). In our early work, we used parents’ daily telephone reports as a tool for monitoring intervention progress (Chamberlain & Reid, 1991). The three functions—assessment, intervention and monitoring—can be coordinated with the AIM Family Support System, combining FCU, PMTO, and TFC-O, as shown in Figure 3. Seamless integration of the FCU, PMTO, and TFC-O within a school district potentiates substantial benefits over deploying the three models independently. The following are the list of potential benefits:
Redundancy in the behavior support strategies at all tiers of the family service.
Accurate and rapid assorting of families into the appropriate level of support, making it less likely that parents are receiving too brief or too intensive an intervention.
Continuity of educational engagement and school retention, by minimizing the need for disruptions due to residential treatment.
Reduce the likelihood of placement into programs or school settings that aggregate high-risk students, which, under some conditions, may lead to problem behavior contagion.
Reduce need to change schools due to temporary treatment foster care reduces disruption of educational progress.
Parents would be less likely to fall out of contact with services during the referral process (e.g., from PMTO to TFC-O). For example, completers of TFC-O that may still need support at a lower level could be seamlessly transitioned to continuing PMTO, and completers of PMTO could be transitioned to annual FCUs to monitor for possible deterioration in skills.
The development of parenting skills across different levels of need and support services could be seamlessly tracked to refine intervention strategies and promote data-based monitoring and decision-making.
Substantially reduced implementation costs due to training, quality of implementation oversight, training and retraining as well as a unified tracking and billing.
FIGURE 3.
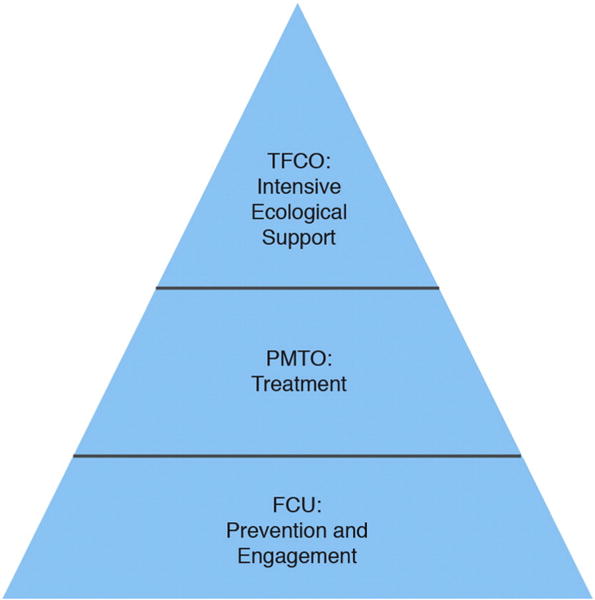
Towards a cost-effective, coordinated, comprehensive community support system for children and families.
In summary, efforts to systemically link effective behavioral interventions within service settings that serve an entire school district are likely to be more effective, less costly, and more sustainable than any single intervention delivered individually (**Chamberlain, Wolf-Feldman, Wulczyn, Saldana & Forgatch, under review). In this sense, we are perhaps ready to move beyond our previous focus on clinical outcomes to a broader focus on community well-being (Biglan, 2015). The AIM Family Support System is an example of a service system that is accountable for improving outcomes but also provides efficient coordination of behavioral interventions for families most likely to succeed. The progress in behavioral family therapy over the past three decades is remarkable. A clinically effective but narrowly defined intervention for outpatient clinics serving families with children with manifest problem behavior has evolved into a range of complementary interventions that can be embedded in service systems that reach thousands of youth and families. Early models for the development of problem behavior served as a useful guide to intervention design and testing. What is now needed are models for implementation that can bring about systemic change to reduce the prevalence of child and adolescent problem behavior and eliminate ineffective, expensive, or iatrogenic prevention and treatment services.
Acknowledgments
This research was supported in part from the Oregon Youth Authority and from the following grants: R01 DA007031-21A1, R01 DA036832-01A1, P50 DA035763, and R01 DA032634 from the National Institute on Drug Abuse; RO1 DA 16097 from the Prevention Research Branch, NIDA, U.S. PHS; and RO1 MH 38318 and RO1 MH 54703 from the Child and Adolescent Treatment and Preventive Intervention Research Branch, DSIR, NIMH, U.S. PHS. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Drug Abuse, Child and Adolescent Treatment and Preventive Intervention Research Branch, or the National Institutes of Health.
Footnotes
Conflict of Interest Statement
Dr. Chamberlain is a partner in TFC Consultants, which disseminates TFCO.
Contributor Information
Thomas Dishion, ASU REACH Institute, Arizona State University.
Marion Forgatch, Implementation Sciences International Inc., and Oregon Social Learning Center.
Patricia Chamberlain, Oregon Social Learning Center.
William E. Pelham, III, ASU REACH Institute, Arizona State University.
References
- Akin BA, Testa MF, McDonald TP, Melz H, Blase KA, Barclay A. Formative Evaluation of an Evidence-Based Intervention to Reduce Long-Term Foster Care: Assessing Readiness for Summative Evaluation. Journal of Public Child Welfare. 2014;8(4):354–374. http://dx.doi.org/10.1080/15548732.2014.939250. [Google Scholar]
- Amlund Hagen K, Ogden T, Bjørnebekk G. Treatment outcomes and mediators of parent management training: A one-year follow-up of children with conduct problems. Journal of Clinical Child & Adolescent Psychology. 2011;40:165–178. doi: 10.1080/15374416.2011.546050. http://dx.doi.org/10.1080/15374416.2011.546050. [DOI] [PubMed] [Google Scholar]
- Arnold JE, Levine AG, Patterson GR. Changes in sibling behavior following family intervention. Journal of Consulting and Clinical Psychology. 1975;43:683–688. doi: 10.1037//0022-006x.43.5.683. http://dx.doi.org/10.1037/0022-006x.43.5.683. [DOI] [PubMed] [Google Scholar]
- Bank L, Marlowe JH, Reid JB, Patterson GR, Weinrott MR. A comparative evaluation of parent-training interventions for families of chronic delinquents. Journal of Abnormal Child Psychology. 1991;19:15–33. doi: 10.1007/BF00910562. http://dx.doi.org/10.1007/bf00910562. [DOI] [PubMed] [Google Scholar]
- Bayer P, Hjalmarsson R, Pozen D. Building criminal capital behind bars: Peer effects in juvenile corrections. Quarterly Journal of Economics. 2009;124:105–147. http://dx.doi.org/10.3386/w12932. [Google Scholar]
- Bergström M, Höjman L. Is multidimensional treatment foster care (MTFC) more effective than treatment as usual in a three-year follow-up? Results from MTFC in a Swedish setting. European Journal of Social Work. 2015:1–17. Online first 10 April. http://dx.doi.org/10.1080/13691457.2015.1030361.
- Biglan A. The nurture effect: How the science of human behavior can improve our lives and our world. Oakland, CA: New Harbinger Publications; 2015. [Google Scholar]
- Bijou SW, Baer DM. Operant behavior:areas of research and application. New York: Appleton-Century-Crofts; 1966. Operant methods in child behavior and development; pp. 718–789. [Google Scholar]
- Bjørknes R, Kjøbli J, Manger T, Jakobsen R. Parent training among ethnic minorities: Parenting practices as mediators of change in child conduct problems. Family Relations: An Interdisciplinary Journal of Applied Family Studies. 2012;61:101–114. http://dx.doi.org/10.1111/j.1741-3729.2011.00683.x. [Google Scholar]
- Block JH, Block J, Gjerde PF. The personality of children prior to divorce: A prospective study. Child Development. 1986;57:827–840. doi: 10.1111/j.1467-8624.1986.tb00249.x. http://dx.doi.org/10.2307/1130360. [DOI] [PubMed] [Google Scholar]
- Brown CH, Chamberlain P, Saldana L, Padgett C, Wang W, Cruden G. Evaluation of two implementation strategies in 51 child county public service systems in two states: Results of a cluster randomized head-to-head implementation trial. Implementation Science. 2014;9:1–15. doi: 10.1186/s13012-014-0134-8. http://dx.doi.org/10.1186/s13012-014-0134-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buehler RE, Patterson GR, Furniss JM. The reinforcement of behavior in institutional settings. Behavior Research & Therapy. 1966;4:157–167. doi: 10.1016/0005-7967(66)90002-7. http://dx.doi.org/10.1016/0005-7967(66)90002-7. [DOI] [PubMed] [Google Scholar]
- Bullard L, Wachlarowicz M, DeLeeuw J, Snyder J, Low S, Forgatch MS, DeGarmo DS. Effects of the Oregon Model of Parent Management Training (PMTO) on marital adjustment in new stepfamilies: A randomized trial. Journal of Family Psychology. 2010;24:485–496. doi: 10.1037/a0020267. http://dx.doi.org/10.1037/a0020267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Capaldi DM, Patterson GR. Relation of parental transitions to boys’ adjustment problems: I. A linear hypothesis. II. Mothers at risk for transitions and unskilled parenting. Developmental Psychology. 1991;27:489–504. http://dx.doi.org/10.1037//0012-1649.27.3.489. [Google Scholar]
- Caruthers AS, Ryzin MJV, Dishion TJ. Preventing High-Risk Sexual Behavior in Early Adulthood with Family Interventions in Adolescence: Outcomes and Developmental Processes. Prevention Science. 2014;15(1):59–69. doi: 10.1007/s11121-013-0383-9. http://dx.doi.org/10.1007/s11121-013-0383-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chamberlain P. Treating chronic juvenile offenders: Advances made through the Oregon multidimensional treatment foster care model. Washington, DC: American Psychological Association; 2003. http://dx.doi.org/10.1037/10596-000. [Google Scholar]
- Chamberlain P, Reid JB. Parent observation and report of child symptoms. Behavioral Assessment. 1987;9:97–109. [Google Scholar]
- Chamberlain P, Reid JB. Using a specialized foster care community treatment model for children and adolescents leaving the state mental hospital. Journal of Community Psychology. 1991;19(3):266–276. http://dx.doi.org/10.1002/1520-6629(199107)19:3<266::AID-JCOP2290190310>3.0.CO;2-5. [Google Scholar]
- Chamberlain P, Reid JB. Comparison of two community alternatives to incarceration for chronic juvenile offenders. Journal of Consulting and Clinical Psychology. 1998;66:624–633. doi: 10.1037//0022-006x.66.4.624. http://dx.doi.org/10.1037/0022-006x.66.4.624. [DOI] [PubMed] [Google Scholar]
- Chamberlain P, Feldman SW, Wulczyn F, Saldana L, Forgatch MS. Implementation and evaluation of linked parenting models in the New York City child welfare system. 2015 doi: 10.1016/j.chiabu.2015.09.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chamberlain P, Leve LD, DeGarmo DS. Multidimensional treatment foster care for girls in the juvenile justice system: 2-year follow-up of a randomized clinical trial. Journal of Consulting and Clinical Psychology. 2007;75(1):187–193. doi: 10.1037/0022-006X.75.1.187. http://dx.doi.org/10.1037/0022-006X.75.1.187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chamberlain P, Moreland S, Reid K. Enhanced services and stipends for foster parents: effects on retention rates and outcomes for children. Child Welfare. 1992;71(5):387–401. 15p. [PubMed] [Google Scholar]
- Chamberlain P, Price JM, Reid JB, Landsverk J, Fisher PA, Stoolmiller M. Who disrupts from placement in foster and kinship care? Child Abuse and Neglect. 2006;30:409–424. doi: 10.1016/j.chiabu.2005.11.004. http://dx.doi.org/10.1016/j.chiabu.2005.11.004. [DOI] [PubMed] [Google Scholar]
- Chamberlain P, Price J, Leve LD, Laurent H, Landsverk JA, Reid JB. Prevention of behavior problems for children in foster care: Outcomes and mediation effects. Prevention Science. 2008;9:17–27. doi: 10.1007/s11121-007-0080-7. http://dx.doi.org/10.1007/s11121-007-0080-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chamberlain P, Wolf-Feldman S, Wulczyn F, Saldana L, Forgatch M. Prevention Science under review. [Google Scholar]
- Chang H, Shaw DS, Dishion TJ, Gardner F, Wilson MN. Direct and Indirect Effects of the Family Check-Up on Self-Regulation from Toddlerhood to Early School-Age. Journal of Abnormal Child Psychology. 2014;42(7):1117–1128. doi: 10.1007/s10802-014-9859-8. http://dx.doi.org/10.1007/s10802-014-9859-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Connell AM. Employing Complier Average Causal Effect Analytic Methods to Examine Effects of Randomized Encouragement Trials. The American Journal of Drug and Alcohol Abuse. 2009;35(4):253–259. doi: 10.1080/00952990903005882. http://dx.doi.org/10.1080/00952990903005882. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Connell AM, Dishion TJ. Reducing depression among at-risk early adolescents: Three-year effects of a family-centered intervention embedded within schools. Journal of Family Psychology. 2008;22(4):574–585. doi: 10.1037/0893-3200.22.3.574. http://dx.doi.org/10.1037/0893-3200.22.3.574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Connell A, Dishion TJ, Yasui M, Kavanagh K. An adaptive approach to family intervention: Linking engagement in family-centered intervention to reductions in adolescent problem behavior. Journal of Consulting and Clinical Psychology. 2007;75:568–579. doi: 10.1037/0022-006X.75.4.568. [DOI] [PubMed] [Google Scholar]
- Connell A, Bullock BM, Dishion TJ, Shaw DS, Wilson M, Gardner F. Family intervention effects on co-occurring early childhood behavioral and emotional problems: A latent transition analysis approach. Journal of Abnormal Child Psychology. 2008;36:1211–1225. doi: 10.1007/s10802-008-9244-6. http://dx.doi.org/10.1007/s10802-008-9244-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cronbach LJ, Gleser GC. Psychological tests and personnel decisions. Oxford, England: U. Illinois Press; 1965. [Google Scholar]
- Crone DA, Horner RH. Building positive behavior support systems in schools: Functional behavioral assessment. New York, NY: Guildford Press; 2003. [Google Scholar]
- Crowley DM, Jones DE, Greenberg MT, Feinberg ME, Spoth RL. Resource consumption of a diffusion model for prevention programs: The PROSPER delivery system. Journal of Adolescent Health. 2012;50(3):256–263. doi: 10.1016/j.jadohealth.2011.07.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeGarmo DS, Forgatch MS. Efficacy of parent training for stepfathers: From playful spectator and polite stranger to effective stepfathering. Parenting: Science and Practice. 2007;7:1–25. doi: 10.1080/15295190701665631. http://dx.doi.org/10.1080/15295190701665631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeGarmo DS, Eddy JM, Reid JB, Fetrow RA. Evaluating mediators of the impact of the Linking the Interests of Families and Teachers (LIFT) multimodal preventive intervention on substance use initiation and growth across adolescence. Prevention Science. 2009;10:208–220. doi: 10.1007/s11121-009-0126-0. http://dx.doi.org/10.1007/s11121-009-0126-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeGarmo DS, Patterson GR, Forgatch MS. How do outcomes in a specified parent training intervention maintain or wane over time? Prevention Science. 2004;5:73–89. doi: 10.1023/b:prev.0000023078.30191.e0. http://dx.doi.org/10.1023/B:PREV.0000023078.30191.e0. [DOI] [PubMed] [Google Scholar]
- Dishion TJ. Promoting academic competence and behavioral health in public schools: A strategy of systemic concatenation of empirically based intervention principles [Special Issue] School Psychology Review. 2011;40(4):590–597. [Google Scholar]
- Dishion TJ. An evolutionary framework for understanding coercion and aggression. In: Dishion TJ, Snyder J, editors. Oxford handbook of coercive relationship dynamics: Basic mechanisms, developmental processes, and intervention applications. New York, NY: Oxford University Press; (in press) [Google Scholar]
- Dishion TJ, Kavanagh K. The Adolescent Transitions Program: A family-centered prevention strategy for schools. In: Reid JB, Snyder JJ, Patterson GR, editors. Antisocial behavior in children and adolescents: A developmental analysis and the Oregon model for intervention. Washington, DC: American Psychological Association; 2003. pp. 257–272. http://dx.doi.org/10.1037/10468-013. [Google Scholar]
- Dishion TJ, Patterson GR. Childhood screening for early adolescent problem behavior: A multiple gating strategy. In: Singer M, Singer L, Anglin TM, editors. Handbook for screening adolescents at psychosocial risk. New York, NY: Lexington Books; 1993. pp. 375–399. [Google Scholar]
- Dishion TJ, Patterson GR. The development and ecology of problem behavior: Linking etiology, prevention, and treatment. In: Cicchetti D, editor. Handbook for developmental psychopathology. (in press) [Google Scholar]
- Dishion TJ, Patterson SG. Preventive parenting with love, encouragement, and limits: The preschool years. Eugene, OR: Castalia; 1996. [Google Scholar]
- Dishion TJ, Stormshak EA. Intervening in children’s lives: An ecological, family-centered approach to mental health care. Washington, DC: American Psychological Association; 2007. [Google Scholar]
- Dishion TJ, Tipsord JM. Peer contagion in child and adolescent social and emotional development. Annual Review of Psychology. 2011;62:189–214. doi: 10.1146/annurev.psych.093008.100412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dishion TJ, Brennan LM, Shaw DS, McEachern AD, Wilson MN, Jo B. Prevention of problem behavior through annual Family Check-Ups in early childhood: Intervention effects from home to early elementary school. Journal of Abnormal Child Psychology. 2014;42:343–354. doi: 10.1007/s10802-013-9768-2. http://dx.doi.org/10.1007/s10802-013-9768-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dishion TJ, Forgatch MS, Van Ryzin MJ, Winter C. The nonlinear dynamics of family problem solving in adolescence: The predictive validity of a peaceful resolution attractor. Nonlinear Dynamics, Psychology, and Life Sciences. 2012;16:331–352. [PMC free article] [PubMed] [Google Scholar]
- Dishion TJ, Kavanagh K, Kiesner J. Prevention of early adolescent substance use among high-risk youth: A multiple gating approach to parent intervention. In: Ashery RS, editor. Research meeting on drug abuse prevention through family interventions. Washington, DC: U.S.: Government Printing Office; 1999. pp. 208–228. (NIDA Research Monograph No. 177). [Google Scholar]
- Dishion TJ, Kavanagh K, Schneiger A, Nelson S, Kaufman N. Preventing early adolescent substance use: A family-centered strategy for public middle school. [Special issue] Prevention Science. 2002;3:191–201. doi: 10.1023/a:1019994500301. [DOI] [PubMed] [Google Scholar]
- Dishion TJ, Nelson SE, Kavanagh K. The Family Check-Up with high-risk young adolescents: Preventing early-onset substance use by parent monitoring [Special issue] Behavior Therapy. 2003;34:553–571. [Google Scholar]
- Dishion TJ, Patterson GR, Stoolmiller M, Skinner ML. Family, school, and behavioral antecedents to early adolescent involvement with antisocial peers. Developmental Psychology. 1991;27:172–180. http://dx.doi.org/10.1037/0012-1649.27.1.172. [Google Scholar]
- Dishion TJ, Seeley J, Garbacz A, Kim H, Stormshak E, Gau J, Smolkkowski K. Translational research on evidence-based parenting support within public schools: Strategies, findings, implementation challenges and systemic solutions. School Psychology Review (under review) [Google Scholar]
- Dishion TJ, Shaw DS, Connell AM, Gardner F, Weaver CM, Wilson MN. The Family Check-Up with high-risk indigent families: Preventing problem behavior by increasing parents’ positive behavior support in early childhood. Child Development. 2008;79:1395–1414. doi: 10.1111/j.1467-8624.2008.01195.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dishion TJ, Stormshak EA, Kavanagh K. Everyday parenting: A professional’s guide to building family management skills. Champaign, IL: Research Press; 2011. [Google Scholar]
- Dodge KA, Dishion TJ, Lansford JE. Deviant peer influences in intervention and public policy for youth. Social Policy Report. 2006;20:3–19. [Google Scholar]
- Eddy JM, Chamberlain P. Family management and deviant peer association as mediators of the impact of treatment condition on youth antisocial behavior. Journal of Consulting and Clinical Psychology. 2000;68:857–863. doi: 10.1037/0022-006X.68.5.857. http://dx.doi.org/10.2307/1129726. [DOI] [PubMed] [Google Scholar]
- Farrington DP, Loeber R, Van Kammen WB. Long-term criminal outcomes of hyperactivity–impulsivity–attention deficit and conduct problems in childhood. In: Robins LN, Rutter M, editors. Straight and devious pathways from childhood to adulthood. New York: Cambridge University Press; 1990. pp. 62–81. [Google Scholar]
- Fisher PA, Kim HK. Intervention effects on foster preschoolers’ attachment-related behaviors from a randomized trial. Prevention Science. 2007;8:161–170. doi: 10.1007/s11121-007-0066-5. http://dx.doi.org/10.1007/s11121-007-0066-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fisher PA, Stoolmiller M. Intervention effects on foster parent stress: Associations with child cortisol levels. Development and Psychopathology. 2008;20:1003–1021. doi: 10.1017/S0954579408000473. http://dx.doi.org/10.1017/s0954579408000473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fisher PA, Burraston B, Pears KC. Permanency in foster care: Conceptual and methodological issues. Child Maltreatment. 2006;11:92–94. http://dx.doi.org/10.1177/1077559505283357. [Google Scholar]
- Fisher PA, Gunnar MR, Chamberlain P, Reid JB. Preventive Intervention for Maltreated Preschool Children: Impact on Children’s Behavior, Neuroendocrine Activity, and Foster Parent Functioning. Journal of the American Academy of Child & Adolescent Psychiatry. 2000;39(11):1356–1364. doi: 10.1097/00004583-200011000-00009. http://dx.doi.org/10.1097/00004583-200011000-00009. [DOI] [PubMed] [Google Scholar]
- Fisher PA, Stoolmiller M, Gunnar MR, Burraston B. Effects of a therapeutic intervention for foster preschoolers on diurnal cortisol activity. Psychoneuroendocrinology. 2007;32:892–905. doi: 10.1016/j.psyneuen.2007.06.008. http://dx.doi.org/10.1016/j.psyneuen.2007.06.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fisher PA, Stoolmiller M, Mannering AM, Chamberlain P. RCT intervention effects on foster placement disruptions associated with problem behavior. Journal of Consulting and Clinical Psychology. 2011;79:481–487. doi: 10.1037/a0024313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fixsen D, Blase K, Metz A, Van Dyke M. Statewide implementation of evidence-based programs. Exceptional Children. 2013;79:213–230. http://dx.doi.org/10.1177/001440291307900206. [Google Scholar]
- Fleischman MJ, Szykula SA. A community setting replication of a social learning treatment for aggressive children. Behavior Therapy. 1981;12:115–122. http://dx.doi.org/10.1016/s0005-7894(81)80112-8. [Google Scholar]
- Forgatch MS, DeGarmo DS. Parenting through change: An effective prevention program for single mothers. Journal of Consulting and Clinical Psychology. 1999;67:711–724. doi: 10.1037//0022-006x.67.5.711. http://dx.doi.org/10.1037/0022-006X.67.5.711. [DOI] [PubMed] [Google Scholar]
- Forgatch MS, DeGarmo DS. Accelerating recovery from poverty: Prevention effects for recently separated mothers. Journal of Early and Intensive Behavior Intervention. 2007;4(4):681–702. doi: 10.1037/h0100400. http://dx.doi.org/10.1037/h0100400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Forgatch MS, DeGarmo DS. Sustaining fidelity following the nationwide PMTO implementation in Norway. Prevention Science. 2011;12:235–246. doi: 10.1007/s11121-011-0225-6. http://dx.doi.org/10.1007/s11121-011-0225-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Forgatch MS, Domenech Rodríguez MM. Interrupting coercion: The iterative loops among theory, science, and practice. In: Dishion TJ, Snyder JJ, editors. Oxford Handbook of Coercive Relationship Dynamics (Online first, May) New York, NY: Oxford University Press; 2015. http://dx.doi.org/10.1093/oxfordhb/9780199324552.013.17. [Google Scholar]
- Forgatch MS, Patterson GR. Parent Management Training - Oregon Model: An intervention for antisocial behavior in children and adolescents. In: Weisz JR, Kazdin AE, editors. Evidence-based psychotherapies for children and adolescents. New York, NY: Guilford Press; 2010. pp. 159–178. [Google Scholar]
- Forgatch MS, Stoolmiller M. Emotions as contexts for adolescent delinquency. Journal of Research on Adolescence. 1994;4:601–614. http://dx.doi.org/10.1207/s15327795jra0404_10. [Google Scholar]
- Forgatch MS, Toobert DJ. A cost-effective parent training program for use with normal preschool children. Journal of Pediatric Psychology. 1979;4:129–145. http://dx.doi.org/10.1093/jpepsy/4.2.129. [Google Scholar]
- Forgatch MS, Beldavs ZG, Patterson GR, DeGarmo DS. From coercion to positive parenting: Putting divorced mothers in charge of change. In: Kerr M, Stattin H, Engels R, editors. What can parents do? New insights into the role of parents in adolescent problem behavior. London: Wiley; 2008. pp. 191–209. http://dx.doi.org/10.1002/9780470774113.ch8. [Google Scholar]
- Forgatch MS, DeGarmo DS, Beldavs Z. An efficacious theory-based intervention for stepfamilies. Behavior Therapy. 2005;36:357–365. doi: 10.1016/s0005-7894(05)80117-0. http://dx.doi.org/10.1016/S0005-7894(05)80117-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Forgatch MS, Patterson GR, Gewirtz AH. Looking forward: The promise of widespread implementation of parent training programs. Perspectives on Psychological Science. 2013;8:682–694. doi: 10.1177/1745691613503478. http://dx.doi.org/10.1177/1745691613503478. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Forgatch MS, Patterson GR, Skinner ML. A mediational model for the effect of divorce on antisocial behavior in boys. In: Hetherington EM, Arasteh JD, editors. Impact of divorce, single parenting, and step-parenting on children. Hillsdale, NJ: Erlbaum; 1988. pp. 135–154. [Google Scholar]
- Forgatch MS, Patterson GR, DeGarmo DS, Beldavs ZG. Testing the Oregon delinquency model with 9-year follow-up of the Oregon Divorce Study. Development and Psychopathology. 2009;21:637–660. doi: 10.1017/S0954579409000340. http://dx.doi.org/10.1017/S0954579409000340. [DOI] [PubMed] [Google Scholar]
- Fosco GM, Frank JL, Stormshak EA, Dishion TJ. Opening the “Black Box”: Family Check-Up intervention effects on self-regulation that prevents growth in problem behavior and substance use. Journal of School Psychology. 2013;51(4):455–468. doi: 10.1016/j.jsp.2013.02.001. http://doi.org/10.1016/j.jsp.2013.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fuchs D, Fuchs LS. Introduction to response to intervention: What, why, and how valid is it? Reading Research Quarterly. 2006;41(1):93–99. http://doi.org/10.1598/RRQ.41.1.4. [Google Scholar]
- Gardner F, Shaw D, Dishion TJ, Burton J, Supplee L. Randomized prevention trial for early conduct problems: Effects on proactive parenting and links to toddler disruptive behavior. Journal of Family Psychology. 2007;21(3):398–406. doi: 10.1037/0893-3200.21.3.398. http://dx.doi.org/10.1037/0893-3200.21.3.398. [DOI] [PubMed] [Google Scholar]
- Gatti U, Tremblay RE, Vitaro F. Iatrogenic effect of juvenile justice. Journal of Child Psychology and Psychiatry. 2009;50:991–998. doi: 10.1111/j.1469-7610.2008.02057.x. http://dx.doi.org/10.1111/j.1469-7610.2008.02057.x. [DOI] [PubMed] [Google Scholar]
- Gewirtz AH. Promoting children’s mental health in family supportive housing: A community-university partnership for formerly homeless children and families. The Journal of Primary Prevention. 2007;28:359–374. doi: 10.1007/s10935-007-0102-z. http://dx.doi.org/10.1007/s10935-007-0102-z. [DOI] [PubMed] [Google Scholar]
- Gewirtz AH, Taylor T. Participation of homeless and abused women in a parent training program: Science and practice converge in a battered women’s shelter. In: Hindsworth MF, Lang TB, editors. Community participation and empowerment. Hauppage, NY: Nova Science Publishers; 2009. pp. 97–114. [Google Scholar]
- Gewirtz AH, DeGarmo DS, Lee S, Morrell N, August G. Two-year outcomes of the Early Risers prevention trial with formerly homeless families residing in supportive housing. Journal of Family Psychology. 2015;29:242–252. doi: 10.1037/fam0000066. http://dx.doi.org/10.1037/fam0000066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gewirtz AH, Pinna KLM, Hanson SK, Brockberg D. Promoting parenting to support reintegrating military families: After deployment, adaptive parenting tools. Psychological Services. 2014;11:31–40. doi: 10.1037/a0034134. http://dx.doi.org/10.1037/a0034134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hanf C. Modification of mother child controlling behavior during mother-child interactions in a controlled laboratory setting. Paper presented at the regional meeting of the Association for Advancement of Behavior Therapy; Olympia, WA. 1968. [Google Scholar]
- Harold GT, Kerr DCR, Ryzin MV, DeGarmo DS, Rhoades KA, Leve LD. Depressive Symptom Trajectories Among Girls in the Juvenile Justice System: 24-month Outcomes of an RCT of Multidimensional Treatment Foster Care. Prevention Science. 2013;14(5):437–446. doi: 10.1007/s11121-012-0317-y. http://dx.doi.org/10.1007/s11121-012-0317-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jo B. Estimation of intervention effects with noncompliance: Alternative model specifications. Journal of Educational and Behavioral Statistics. 2002;27(4):385–409. [Google Scholar]
- Kazdin AE. Problem-solving skills training and parent management training for oppositional defiant disorder and conduct disorder. In: Weisz JR, Kazdin AE, editors. Evidence-Based Psychotherapies for Children and Adolescents. Second. New York, NY: Guilford Press; 2010. pp. 211–226. [Google Scholar]
- Kerr DCR, Leve LD, Chamberlain P. Pregnancy rates among juvenile justice girls in two randomized controlled trials of multidimensional treatment foster care. Journal of Consulting and Clinical Psychology. 2009;77:588–593. doi: 10.1037/a0015289. http://dx.doi.org/10.1037/a0015289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kjøbli J, Bjørnebekk G. A randomized effectiveness trial of brief parent training: Six-month follow-up. Research on Social Work Practice. 2013;23:603–612. http://dx.doi.org/10.1177/1049731513492860. [Google Scholar]
- Kjøbli J, Ogden T. A randomized effectiveness trial of brief parent training in primary care settings. Prevention Science. 2012;13:616–626. doi: 10.1007/s11121-012-0289-y. http://dx.doi.org/10.1007/s11121-012-0289-y. [DOI] [PubMed] [Google Scholar]
- Kjøbli J, Hukkelberg S, Ogden T. A randomized trial of group parent training: Reducing child conduct problems in real-world settings. Behaviour Research and Therapy. 2013;51:113–121. doi: 10.1016/j.brat.2012.11.006. http://dx.doi.org/10.1016/j.brat.2012.11.006. [DOI] [PubMed] [Google Scholar]
- Knutson NM, Forgatch MS, Rains LA, Sigmarsdóttir M. Fidelity of Implementation Rating System (FIMP): The manual for PMTO™. Eugene, OR: Implementation Sciences International, Inc.; 2009. [Google Scholar]
- Kolko DJ. Clinical monitoring of treatment course in child physical abuse: Psychometric characteristics and treatment comparisons. Child Abuse & Neglect. 1996;20(1):23–43. doi: 10.1016/0145-2134(95)00113-1. [DOI] [PubMed] [Google Scholar]
- Leijten P, Shaw DS, Gardner F, Wilson MN, Matthys W, Dishion TJ. The Family Check-Up and Service Use in High-Risk Families of Young Children: A Prevention Strategy with a Bridge to Community-Based Treatment. Prevention Science. 2014;16(3):397–406. doi: 10.1007/s11121-014-0479-x. http://dx.doi.org/10.1007/s11121-014-0479-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leve LD, Chamberlain P. The effects of gender and intervention context on delinquency for youth in the juvenile justice system. Journal of Abnormal Psychology. 2005;33(3):339–347. doi: 10.1007/s10802-005-3571-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leve LD, Chamberlain P. A randomized evaluation of Multidimensional Treatment Foster Care: Effects on school attendance and homework completion in juvenile justice girls. Research on Social Work Practice. 2007;17:657–663. doi: 10.1177/1049731506293971. http://dx.doi.org/10.1177/1049731506293971. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leve LD, Chamberlain P, Reid JB. Intervention outcomes for girls referred from juvenile justice: Effects on delinquency. Journal of Consulting and Clinical Psychology. 2005;73(6):1181–1184. doi: 10.1037/0022-006X.73.6.1181. http://dx.doi.org/10.1037/0022-006X.73.6.1181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leve LD, Fisher PA, Chamberlain P. Multidimensional treatment foster care as a preventive intervention to promote resiliency among youth in the child welfare system. Journal of Personality. 2009;77:1869–1902. doi: 10.1111/j.1467-6494.2009.00603.x. http://dx.doi.org/10.1111/j.1467-6494.2009.00603.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Loeber R, Dishion T. Early predictors of male delinquency: A review. Psychological Bulletin. 1983;94:68–99. http://dx.doi.org/10.1037/0033-2909.94.1.68. [PubMed] [Google Scholar]
- Loeber R, Dishion TJ, Patterson GR. Multiple gating: A multistage assessment procedure for identifying youths at risk for delinquency. Journal of Research in Crime and Delinquency. 1984;21:7–32. [Google Scholar]
- Marsenich L. Evidence-based practices in mental health services for foster youth. Sacramento, CA: California Institute for Mental Health; 2002. Mar, [Google Scholar]
- Martinez CR, Forgatch MS. Preventing problems with boys’ noncompliance: Effects of a parent training intervention for divorcing mothers. Journal of Consulting and Clinical Psychology. 2001;69(3):416–428. doi: 10.1037//0022-006x.69.3.416. http://dx.doi.org/10.1037/0022-006X.69.3.416. [DOI] [PubMed] [Google Scholar]
- McEachern AD, Fosco GM, Dishion TJ, Shaw DS, Wilson MN, Gardner F. Collateral benefits of the family check-up in early childhood: Primary caregivers’ social support and relationship satisfaction. Journal of Family Psychology. 2013;27(2):271–281. doi: 10.1037/a0031485. http://dx.doi.org/10.1037/a0031485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McMahon RJ, Forehand RL. Helping the Noncompliant Child: Family-Based Treatment for Oppositional Behavior. New York, NY: Guilford Press; 2005. [Google Scholar]
- Miller WR, Rollnick S. Motivational interviewing: Preparing people for change. 2nd. New York: Guilford Press; 2002. [Google Scholar]
- Mrazek P, Biglan A, Hawkins JD, Cody C. Community monitoring systems: Tracking and improving the well-being of America’s children and adolescents. Falls Church, VA: Society for Preventive Research; 2007. [Google Scholar]
- Nelson SE, Van Ryzin MJ, Dishion TJ. Alcohol, marijuana, and tobacco use trajectories from age 12 to 24 years: Demographic correlates and young adult substance use problems. Development and Psychopathology. 2015;27:253–277. doi: 10.1017/S0954579414000650. Special Issue 01. http://dx.doi.org/10.1017/S0954579414000650. [DOI] [PubMed] [Google Scholar]
- O’Connell ME, Boat T, Warner KE, editors. Preventing mental, emotional, and behavioral disorders among young people: Progress and possibilities. Washington, DC: National Academies Press; 2009. http://dx.doi.org/10.17226/12480. [PubMed] [Google Scholar]
- Ogden T, Amlund Hagen K. Treatment effectiveness of parent management training in Norway: A randomized controlled trial of children with conduct problems. Journal of Consulting and Clinical Psychology. 2008;76:607–621. doi: 10.1037/0022-006X.76.4.607. http://dx.doi.org/10.1037/0022-006X.76.4.607. [DOI] [PubMed] [Google Scholar]
- Ogden T, Forgatch MS, Askeland E, Patterson GR, Bullock BM. Implementation of parent management training at the national level: The case of Norway. Journal of Social Work Practice. 2005;19:319–331. http://dx.doi.org/10.1080/02650530500291518. [Google Scholar]
- Parra-Cardona JR, Domenech Rodríguez MM, Forgatch MS, Sullivan C, Bybee D, Holtrop K, Bernal G. Culturally adapting an evidence-based parenting intervention for Latino immigrants: The need to integrate fidelity and cultural relevance. Family Process. 2012;51:56–72. doi: 10.1111/j.1545-5300.2012.01386.x. http://dx.doi.org/10.1111/j.1545-5300.2012.01386.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patterson GR. An application of conditioning techniques to the control of a hyperactive child. In: Ullmann LP, Krasner L, editors. Case studies in behavior modification. New York: Holt, Rinehart & Winston; 1965a. pp. 370–375. [Google Scholar]
- Patterson GR. A basis for identifying stimuli which control behaviors in natural settings. Child Development. 1974;45:900. http://dx.doi.org/10.2307/1128075. [PubMed] [Google Scholar]
- Patterson GR. A social learning approach: Coercive family process. Eugene, OR: Castalia; 1982. [Google Scholar]
- Patterson GR. The early development of coercive family process. In: Reid JB, Patterson GR, Snyder J, editors. Antisocial behavior in children and adolescents: A developmental analysis and model for intervention. Washington, DC: American Psychological Association; 2002. pp. 25–44. [Google Scholar]
- Patterson GR, Chamberlain P. Treatment process: A problem at three levels. In: Wynne LC, editor. The state of the art in family therapy research: Controversies and recommendations. New York, NY: Family Process Press; 1988. pp. 189–223. http://dx.doi.org/10.1037/e386842004-001. [Google Scholar]
- Patterson GR, Forgatch MS. Therapist behavior as a determinant for client noncompliance: A paradox for the behavior modifier. Journal of Consulting and Clinical Psychology. 1985;53:846–851. doi: 10.1037//0022-006x.53.6.846. http://dx.doi.org/10.1037/0022-006X.53.6.846. [DOI] [PubMed] [Google Scholar]
- Patterson GR, Reid JB. Reciprocity and coercion: Two facets of social systems. In: Neuringer C, Michael JI, editors. Behavior modification in clinical psychology. New York: Appleton-Century-Crofts; 1970. pp. 133–177. [Google Scholar]
- Patterson GR, Chamberlain P, Reid JB. A comparative evaluation of a parent-training program. Behavior Therapy. 1982;13:638–650. doi: 10.1016/j.beth.2016.11.004. http://dx.doi.org/10.1016/s0005-7894(82)80021-x. [DOI] [PubMed] [Google Scholar]
- Patterson GR, DeBaryshe BD, Ramsey E. A developmental perspective on antisocial behavior. American Psychologist. 1989;44:329–335. doi: 10.1037//0003-066x.44.2.329. http://dx.doi.org/10.1037/0003-066X.44.2.329. [DOI] [PubMed] [Google Scholar]
- Patterson GR, Forgatch MS, DeGarmo DS. Cascading effects following intervention. Development & Psychopathology. 2010;22:949–970. doi: 10.1017/S0954579410000568. http://dx.doi.org/10.1017/S0954579410000568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patterson GR, Reid JB. Families with Aggressive Children. Eugene, OR: Castalia Pub; 1975. [Google Scholar]
- Patterson GR, Reid JB, Dishion TJ. Antisocial Boys. Vol. 4. Eugene, OR: Castalia; 1992. [Google Scholar]
- Pears K, Capaldi DM, Owen LD. Substance use risk across three generations: The roles of parent discipline practices and inhibitory control. Psychology of Addictive Behaviors. 2007;21:373–386. doi: 10.1037/0893-164X.21.3.373. http://dx.doi.org/10.1037/0893-164x.21.3.373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piehler TF. Coercion and contagion in child and adolescent peer relationships. In: Dishion TJ, Snyder J, editors. Oxford handbook of coercive relationship dynamics: Basic mechanisms, developmental processes, and intervention applications. New York, NY: Oxford University Press; pp. 129–139. (in press) [Google Scholar]
- Poduska JM, Kellam SG, Wang W, Brown CH, Ialongo NS, Toyinbo P. Impact of the Good Behavior Game, a universal classroom-based behavior intervention, on young adult service use for problems with emotions, behavior, or drugs or alcohol. Drug & Alcohol Dependence. 2008;95:29–44. doi: 10.1016/j.drugalcdep.2007.10.009. http://dx.doi.org/10.1016/j.drugalcdep.2007.10.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Poulton R, Van Ryzin MJ, Harold GT, Chamberlain P, Fowler D, Cannon M, Leve LD. Effects of Multidimensional Treatment Foster Care on Psychotic Symptoms in Girls. Journal of the American Academy of Child & Adolescent Psychiatry. 2014;53(12):1279–1287. doi: 10.1016/j.jaac.2014.08.014. http://dx.doi.org/10.1016/j.jaac.2014.08.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Redl F, Wineman D. The aggressive child. New York: The Free Press; 1957. [Google Scholar]
- Reid JB. A social approach to family intervention in delinquent behavior patterns. In: Browning P, editor. Rehabilitation and the retarded offender. Springfield, IL: Thomas; 1976. pp. 194–206. [Google Scholar]
- Reid JB. Social-interactional patterns in families of abused and nonabused children. In: Waxler CZ, Cummings EM, Iannotti R, editors. Altruism and aggression: Biological and social origins. New York, NY: Cambridge University Press; 1986. pp. 238–255. [Google Scholar]
- Reid JB, Eddy JM, Fetrow RA, Stoolmiller M. Three year outcomes from a randomized, universal, prevention trial for conduct disorder. Paper presented at the Annual meetings of the Society for Prevention Research; Park City, UT. 1998. [Google Scholar]
- Reuben JD, Shaw DS, Brennan LM, Dishion TJ, Wilson MN. A Family-Based Intervention for Improving Children’s Emotional Problems Through Effects on Maternal Depressive Symptoms. Journal of Consulting and Clinical Psychology. 2015 doi: 10.1037/ccp0000049. http://dx.doi.org/10.1037/ccp0000049. [DOI] [PMC free article] [PubMed]
- Rhoades KA, Leve LD, Harold GT, Kim HK, Chamberlain P. Drug Use Trajectories After a Randomized Controlled Trial of MTFC: Associations With Partner Drug Use. Journal of Research on Adolescence. 2014;24(1):40–54. doi: 10.1111/jora.12077. http://dx.doi.org/10.1111/jora.12077. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sanders MR, Murphy-Brennan M. The international dissemination of the Triple P–Positive Parenting Program. In: Weisz JR, Kazdin AE, editors. Evidence-Based Psychotherapies for Children and Adolescents. Second. New York, NY: Guilford Press; 2010. pp. 519–537. [Google Scholar]
- Shaw DS, Connell A, Dishion TJ, Wilson MN, Gardner F. Improvements in maternal depression as a mediator of intervention effects on early childhood problem behavior. Development and Psychopathology. 2009;21(2):417–439. doi: 10.1017/S0954579409000236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shaw DS, Dishion TJ, Supplee L, Gardner F, Arnds K. Randomized trial of a family-centered approach to the prevention of early conduct problems: 2-year effects of the Family Check-Up in early childhood. Journal of Consulting and Clinical Psychology. 2006;74:1–9. doi: 10.1037/0022-006X.74.1.1. http://dx.doi.org/10.1037/0022-006x.74.1.1. [DOI] [PubMed] [Google Scholar]
- Sigmarsdóttir M, Björnsdóttir A. Community implementation of PMTO ™: Impacts on referrals to specialist services and schools. Scandinavian Journal of Psychology. 2012;53(6):506–511. doi: 10.1111/j.1467-9450.2012.00974.x. http://dx.doi.org/10.1111/j.1467-9450.2012.00974.x. [DOI] [PubMed] [Google Scholar]
- Sigmarsdóttir M, Thorlacius Ö, Guðmundsdóttir EV, DeGarmo DS. Treatment Effectiveness of PMTO for Children’s Behavior Problems in Iceland: Child Outcomes in a Nationwide Randomized Controlled Trial. Family Process. 2015;54(3):498–517. doi: 10.1111/famp.12109. http://dx.doi.org/10.1111/famp.12109. [DOI] [PubMed] [Google Scholar]
- Sitnick SL, Shaw DS, Gill A, Dishion TJ, Winter C, Waller R, Wilson M. Parenting and the Family Check-Up: Changes in observed parent-child interaction following early childhood intervention. Journal of Clinical Child & Adolescent Psychology, Online first, 18 August. 2014:1–15. doi: 10.1080/15374416.2014.940623. http://dx.doi.org/10.1080/15374416.2014.940623. [DOI] [PMC free article] [PubMed]
- Skinner B. The science of learning and the art of teaching. Harvard Educational Review. 1954;24:86–97. [Google Scholar]
- Slavet JD, Stein LAR, Klein JL, Colby SM, Barnett NP, Monti PM. Piloting the Family Check-Up with incarcerated adolescents and their parents. Psychological Services. 2005;2(2):123–132. doi: 10.1037/1541-1559.2.2.123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith DK, Chamberlain P. Multidimensional treatment foster care for adolescents: Processes and outcomes. In: Weisz JR, Kazdin AE, editors. Evidence-based psychotherapies for children and adolescents. 2nd. New York, NY: Guilford Press; 2010. pp. 243–258. [Google Scholar]
- Smith DK, Chamberlain P, Eddy JM. Preliminary Support for Multidimensional Treatment Foster Care in Reducing Substance Use in Delinquent Boys. Journal of Child & Adolescent Substance Abuse. 2010;19(4):343–358. doi: 10.1080/1067828X.2010.511986. http://dx.doi.org/10.1080/1067828X.2010.511986. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith DK, Stormshak E, Chamberlain P, Bridges Whaley R. Placement disruptions in treatment foster care. Journal of Emotional and Behavioral Disorders. 2001;9:200–205. http://dx.doi.org/10.1177/106342660100900306. [Google Scholar]
- Smith JD, Dishion TJ, Shaw DS, Wilson MN, Winter CC, Patterson GR. Coercive family process and early-onset conduct problems from age 2 to school entry. Development and Psychopathology. 2014;26:917–932. doi: 10.1017/S0954579414000169. http://dx.doi.org/10.1017/S0954579414000169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith JD, Stormshak EA, Kavanagh K. Results of a pragmatic effectiveness-implementation hybrid trial of the Family Check-Up in community mental health agencies. Administration and Policy in Mental Health and Mental Health Services Research. 2014;42(3):265–278. doi: 10.1007/s10488-014-0566-0. http://dx.doi.org/10.1007/s10488-014-0566-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Snyder JJ, Reid JB, Stoolmiller M, Howe GW, Brown CH, Dagne GA, Cross W. The role of behavioral observation in measurement systems for ran-domized prevention trials. Prevention Science. 2006;6:1–14. doi: 10.1007/s11121-005-0020-3. http://dx.doi.org/10.1007/s11121-005-0020-3. [DOI] [PubMed] [Google Scholar]
- Sosna T, Marsenich L. Community development team model: Supporting the model adherent implementation of programs and practices. Sacramento, CA: California Institute for Mental Health; 2006. [Google Scholar]
- Spirito A, Sindelar-Manning H, Colby SM, Barnett NP, Lewander W, Rohsenow DJ, Monti PM. Individual and family motivational interventions for alcohol-positive adolescents treated in an emergency department: Results of a randomized clinical trial. Archives of Pediatrics & Adolescent Medicine. 2011;165(3):269–274. doi: 10.1001/archpediatrics.2010.296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spoth RL, Redmond C, Shin C, Azevedo K. Brief family intervention effects on adolescent substance initiation: School-level growth curve analyses 6 years following baseline. Journal of Consulting and Clinical Psychology. 2004;72(3):535–542. doi: 10.1037/0022-006X.72.3.535. http://dx.doi.org/10.1037/0022-006X.72.3.535. [DOI] [PubMed] [Google Scholar]
- Spoth R, Redmond C, Hockaday C, Shin CY. Barriers to participation in family skills preventive interventions and their evaluations: A replication and extension. Family Relations. 1996;45(3):247–254. [Google Scholar]
- Stoolmiller M, Duncan TE, Bank L, Patterson GR. Some problems and solutions in the study of change: Significant patterns of client resistance. Journal of Consulting and Clinical Psychology. 1993;61:920–928. doi: 10.1037//0022-006x.61.6.920. http://dx.doi.org/10.1037/0022-006X.61.6.920. [DOI] [PubMed] [Google Scholar]
- Stormshak EA, Connell AM, Véronneau MH, Myers MW, Dishion TJ, Kavanagh K, Caruthers AS. An ecological approach to promoting early adolescent mental health and social adaptation: Family centered intervention in public middle schools. Child Development. 2011;82(1):209–225. doi: 10.1111/j.1467-8624.2010.01551.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stormshak EA, Connell A, Dishion TJ. An Adaptive Approach to Family-Centered Intervention in Schools: Linking Intervention Engagement to Academic Outcomes in Middle and High School. Prevention Science. 2009;10(3):221–235. doi: 10.1007/s11121-009-0131-3. http://dx.doi.org/10.1007/s11121-009-0131-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stormshak EA, Fosco GM, Dishion TJ. Implementing interventions with families in schools to increase youth school engagement: The Family Check-Up model. School Mental Health. 2010;2:82–92. doi: 10.1007/s12310-009-9025-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stouthamer-Loeber M, Loeber R. Lost opportunities for intervention: undetected markers for the development of serious juvenile delinquency. Criminal Behaviour & Mental Health. 2002;12(1):69. doi: 10.1002/cbm.487. [DOI] [PubMed] [Google Scholar]
- Szapocznik J, Perez-Vidal A, Brickman AL, Foote FH, Santisteban D, Hervis O. Engaging adolescent drug abusers and their families in treatment: A strategic structural systems approach. Journal of Consulting and Clinical Psychology. 1988;56(4):552–557. doi: 10.1037//0022-006x.56.4.552. [DOI] [PubMed] [Google Scholar]
- Tømmeraas T, Ogden T. Is there a scale-up penalty? Testing behavioral change in the scaling up of parent management training in Norway. 2015 doi: 10.1007/s10488-015-0712-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Uebelacker LA, Hecht J, Miller IW. The Family Check-Up: A pilot study of a brief intervention to improve family functioning in adults. Family Process. 2006;45(2):223–236. doi: 10.1111/j.1545-5300.2006.00092.x. [DOI] [PubMed] [Google Scholar]
- Van Ryzin MJ, Dishion TJ. The impact of a family-centered intervention on the ecology of adolescent antisocial behavior: Modeling developmental sequelae and trajectories during adolescence. Development and Psychopathology. 2012;24:1139–1155. doi: 10.1017/S0954579412000582. http://dx.doi.org/10.1017/s0954579412000582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Véronneau M-H, Dishion TJ, Connell AM, Kavanagh K. A randomized, controlled trial of the Family Check-Up model in public secondary schools: Linking parent engagement to substance use progressions from early adolescence to adulthood. Journal of Consulting and Clinical Psychology. doi: 10.1037/a0040248. (in press) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wachlarowicz M, Snyder J, Low S, Forgatch M, DeGarmo D. The Moderating Effects of Parent Antisocial Characteristics on the Effects of Parent Management Training-Oregon (PMTO™) Prevention Science. 2012;13(3):229–240. doi: 10.1007/s11121-011-0262-1. http://dx.doi.org/10.1007/s11121-011-0262-1. [DOI] [PubMed] [Google Scholar]
- Wahler RG, Winkel GH, Peterson RF, Morrison DC. Mothers as behavior therapists for their own children. Behaviour Research and Therapy. 1965;3:113–124. doi: 10.1016/0005-7967(65)90015-x. http://dx.doi.org/10.1016/0005-7967(65)90015-x. [DOI] [PubMed] [Google Scholar]
- Walker HM, Severson H. Systematic Screening for Behavior Disorders (SSBD): A Multiple Gating Procedure. Longmont, CO: Sopris West; 1990. [Google Scholar]
- Webster-Stratton CH, Reid MJ. The Incredible Years parents, teachers, and children training series: a multifaceted treatment approach for young children with conduct disorders. In: Weisz JR, Kazdin AE, editors. Evidence-Based Psychotherapies for Children and Adolescents. Second. New York, NY: Guilford Press; 2010. pp. 194–210. [Google Scholar]
- Weiss B, Catron T, Harris V, Phung TM. The effectiveness of traditional child psychotherapy. Journal of Consulting and Clinical Psychology. 1999;67:82–94. doi: 10.1037//0022-006x.67.1.82. [DOI] [PubMed] [Google Scholar]
- Weisz JR, Kazdin AE. The present and future of evidence-based psychotherapies for children and adolescents. In: Weisz JR, Kazdin AE, editors. Evidence-based psychotherapies for children and adolescents. New York, NY: Guilford Press; 2010. pp. 557–572. [Google Scholar]
- Westermark PK, Hansson K, Olsson M. Multidimensional treatment foster care (MTFC): results from an independent replication. Journal of Family Therapy. 2010;33:20–41. http://dx.doi.org/10.1111/j.1467-6427.2010.00515.x. [Google Scholar]
- Wieling E, Mehus C, Yumbul C, Möllerherm J, Ertl V, Laura A, Catani C. Preparing the Field for Feasibility Testing of a Parenting Intervention for War-Affected Mothers in Northern Uganda. Family Process. 2015 doi: 10.1111/famp.12189. n/a–n/a. http://dx.doi.org/10.1111/famp.12189. [DOI] [PubMed]
- Zisser A, Eyberg SM. Parent-child interaction therapy and the treatment of disruptive behavior disorders. In: Weisz JR, Kazdin AE, editors. Evidence-based psychotherapies for children and adolescents. New York, NY: Guilford Press; 2010. pp. 179–193. [Google Scholar]