

Abstract
Background
β-D-glucan (BDG) is a helpful diagnostic marker for many invasive fungal infections, but not for nocardiosis. Here, we reported the first case of nocardial infection with high serum level of BDG.
Case presentation
A 73-year-old man was hospitalized because of fever, headache, and appetite loss after 10 months of steroid and immunosuppressive therapy for cryptogenic organizing pneumonia. With a diagnosis of bacterial pneumonia, treatment with ampicillin/sulbactam was initiated. There was improvement on chest radiograph, but fever persisted. Further work-up revealed multiple brain abscesses on cranial magnetic resonance imaging (MRI). Serum galactomannan and BDG were elevated at 0.6 index and 94.7 pg/ml, respectively. Voriconazole was initiated for presumed aspergillus brain abscess. However, fever persisted and consciousness level deteriorated. Drainage of brain abscess was performed; based on the Gram stain and Kinyoun acid-fast stain, disseminated nocardiosis was diagnosed. Voriconazole was then shifter to trimethoprim/sulfamethoxazole. The presence of Nocardia farcinica was confirmed by the 16S rRNA gene sequence. Treatment course was continued; BDG level normalized after 1 month and cranial MRI showed almost complete improvement after 2 months.
Conclusion
BDG assay is widely used to diagnose invasive fungal infection; therefore, clinicians should be aware that Nocardia species may show cross-reactivity with BDG assay on serum.
Keywords: Nocardial infection, β-D-glucan, Cross-reactivity, Serum
Background
Nocardia species is a gram-positive, branching, filamentous bacillus that may cause localized and disseminated infections in humans, including pulmonary infection, subcutaneous infection, brain abscess, and bacteremia. β-D-glucan (BDG) is a polysaccharide glucose polymer that is found in a broad range of fungal agents, but not in the cell wall of Nocardia species. Therefore, BDG is not thought to be useful in diagnosing nocardiosis. However, Koncan et al. reported a case of Nocardia abscessus brain abscess that showed elevated level of BDG on cerebrospinal fluid [1]. They also described that Nocardia species showed cross-reactivity with BDG assay. Here, we presented the first reported case of nocardial infection with elevated serum BDG level.
Case presentation
A 73-year-old man, Asian, and ex-smoker presented to our department with complaints of fever, headache and appetite loss after 10 months of steroid and immunosuppressive therapy for cryptogenic organizing pneumonia. Physical examination revealed a heart rate of 88 beats/min, blood pressure of 142/74 mmHg, respiratory rate of 20 breaths/min, temperature of 38.5 °C, and oxygen saturation of 95% on room air. Chest examination revealed coarse crackles on right lower lung field. Chest radiograph and computed tomography showed infiltrates on the right middle lobe (Figs. 1 and 2). The white blood cell count, C-reactive protein, and procalcitonin levels were 15,100 /μl, 5.73 mg/dl, and 0.221 ng/ml, respectively. Test for human immunodeficiency virus (HIV) infection was negative. Expectorated sputum smears were negative for bacteria and acid-fast bacilli. Urinary antigen test (Binax NOW; Binax, Inc., Portland, ME) for Streptococcus pneumoniae and Legionella pneumophila were negative. Although it was difficult to determine the causative bacteria, a presumptive diagnosis of community-acquired pneumonia was made, and treatment with ampicillin/sulbactam (ABPC/SBT) 1.5 g intravenously every 6 h was initiated. On day 8, white blood cell count normalized and chest radiograph showed improvement; however, fever persisted. Due to a suspicion of drug fever, ABPC/SBT was discontinued. However, fever persisted even after 4 days of ABPC/SBT discontinuation. To search for the source of infection, cranial magnetic resonance imaging (MRI) was done and showed multiple masses (Fig. 3); brain abscess was diagnosed. Serum Quantiferon test (QuantiFERON-TB Gold In-Tube; Cellestis, Chadstone, Australia), cryptococcus antigen and toxoplasma antibody were negative. Galactomannan (Platelia Aspergillus Ag; Bio-Rad, Marnes-la-Coquette, France) and β-D-glucan (Wako; Wako Pure Chemical Industries, Ltd., Tokyo, Japan) were elevated at 0.6 index, and 94.7 pg/ml, respectively. On day 11, voriconazole (VRCZ) 200 mg intravenously every 12 h was initiated for presumed aspergillus brain abscess. However, after 5 days of treatment, fever continued and consciousness level deteriorated. On day 16, drainage of brain abscess was performed; Gram stain revealed many neutrophils and gram-positive rods with branching, filamentous hyphae (Fig. 4a). Kinyoun acid-fast stain of the gram-positive rods was positive (Fig. 4b). On the basis of these findings, disseminated nocardiosis was diagnosed, and VRCZ was shifted to intravenous trimethoprim/sulfamethoxazole (TMP/SMX) 240 mg/1200 mg every 8 h. The cultured strain was sent to Department of Laboratory medicine of Nagasaki University Hospital, where the presence of Nocardia farcinica was confirmed by 16S rRNA gene sequence. Treatment course was continued. BDG level normalized after 1 month, therefore intravenous TMP/SMX was shifted to oral TMP/SMX 240 mg/1200 mg every 8 h. Cranial MRI showed almost complete improvement after 2 months. Unfortunately, the patient died from aspiration pneumonia after 6 months of treatment.
Fig. 1.
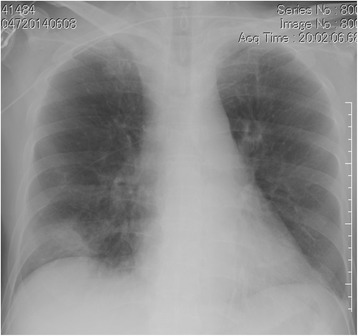
Chest radiography on admission showed infiltration shadow in the right lower lung field
Fig. 2.
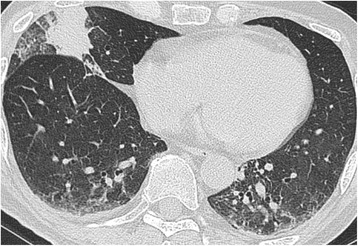
Chest CT on admission showed infiltration shadow in the right middle lobe and ground glass opacity in both lower lobes
Fig. 3.
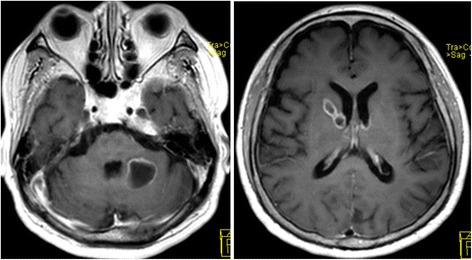
Cranial MRI showed multiple masses
Fig. 4.
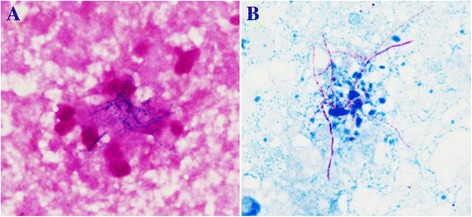
a Gram stain of abscess (×1000) showed a cluster of branching, filamentous Gram-positive rods. b Modified acid fast Kinyoun staining of abscess (×1000) showed filamentous red-stained partially acid-fast rods
Discussion
Nocardia infections are rare, but potentially fatal conditions that are typically more problematic in patients with cell-mediated immunosuppression [2], but may occasionally affect immunocompetent patients as well [3]. Nocardia species is a ubiquitous, gram-positive, actinomycete saprophyte that lives in soil, organic matter and water. Human infection usually arises from direct inoculation of the skin or by inhalation. It is considered an opportunistic pathogen that affects patients with impaired cell-mediated immunity. Most of the patients with Nocardia infection have predisposing factors, such as hematologic malignancies, treatment with corticosteroids, solid tumors, bone marrow or solid organ transplantation, HIV infection or chronic pulmonary or renal disease [2]. The most common clinical presentation is subacute pneumonia with nodules, necrosis, cavitary disease, lung abscess, effusion, and/or empyema [4–6]. Nocardial brain abscess is a rare clinical finding, most of which originate from a primary focus, such as the lungs, skin, or elsewhere in the body [7]. Central nervous system involvement was recognized in over 44% of all cases of systemic nocardiosis [8]. Moreover, nocardial brain abscess carries the highest mortality rate among all bacterial cerebral abscesses [9].
Due to the nonspecific clinical and radiologic manifestations, including irregular nodules, cavitation, reticulonodular shadow, infiltration and pleural effusion, pulmonary nocardiosis is easily misdiagnosed as bacterial pneumonia, tuberculosis, mycosis or actinomycosis [10]. Furthermore, nocardial brain abscess is often mistaken for aspergillosis, tuberculosis, or malignancy because of the similar clinical manifestations [11]. Therefore, helpful diagnostic markers, such as Quantiferon test, cryptococcus antigen, galactomannan, and β-D-glucan (BDG) are very useful. BDG is a polysaccharide glucose polymer that is found in a broad range of commonly encountered fungal agents, including Candida spp., Aspergillus spp., and Pneumocystis jirovecii, with notable exception of cryptococci, zygomycetes, and Blastomyces dermatitidis. BDG is helpful for the diagnosis of invasive fungal infections. This test is a chromogenic, quantitative enzyme immunoassay designed to detect BDG using purified, lysed amebocytes (Limulus amebocyte lysate). These cells contain components of the Limulus clotting cascade, including factors C and G, which initiate coagulation in the presence of bacterial lipopolysaccharide and BDG, respectively. By removing factor C from the lysate, the manufacturers limit activation of the cascade to BDG alone. However, false-positive results with certain hemodialysis filters [12], fungal derived antibiotics [13], immunoglobulins [14], Alcaligenes faecalis and Stretococcus pneumoniae infection [15], and bacteremia caused by Pseudomonas aeruginosa [16] have been described. Koncan et al. reported a case of Nocardia abscessus brain abscess with BDG level that was elevated in the cerebrospinal fluid, but negative in serum [1]. To our best knowledge, nocardial infection with high serum level of BDG has not been reported previously. Our case was the first English article about nocardial infection with elevated BDG level on serum. All known causes of false-positive BDG assay, including invasive fungal disease, hemodialysis treatment using cellulose membrane filter, and use of fungal-derived antibiotics and immunoglobulins, were not present in this patient. Metan et al. reported that clinical administration of intravenous ABPC/SBT caused false-positive BDG assay, although not statistically significant [17]. On the other hand, Marty et al. reported that ABPC/SBT tested negative for BDG at the drug-infusate concentration or at maximum plasma concentration [18]. In our patient, BDG level was examined 4 days after ABPC/SBT discontinuation; we think that ABPC/SBT administration did not cause a false-positive BDG assay. In this patient, because the bacterial suspension of the clinical isolate of Nocardia farcinica was positive for BDG, environmental contamination was unlikely the cause of the positive serum BDG assay. We tested with BDG assay both a strain of N. farcinica isolated from brain pus sample in this case and pure blood agr as negative control used Wako assay (Wako; Wako Pure Chemical Industries, Ltd., Tokyo, Japan). The positive cut off was 11 pg/ml. The strain was cultured on blood agr plate for 24 h at 37 °C. The bacteria were suspended in glucan free sterile saline and harvested by centrifugation (3000×g, 4 °C, 5 min). The organisms were resuspended in glucan free sterile saline and diluted from 1 × 108 to 2 × 108 CFU/ml as estimated by turbidimetry. Pure blood agar as negative control were always negative, but BDG levels of N. farcinica were mildly elevated to about 20 pg/ml.
Pulmonary nocardiosis and nocardial brain abscess can be easily misdiagnosed clinically. Moreover, culture of Nocardia species is difficult because of the slow growth of the bacteria and the presence of normal flora in the culture. Microbiologic diagnosis of nocardiosis and identification of nocardia clinical isolates by conventional methods are difficult and time-consuming [19]. Additionally, cross-reactivity of Nocardia species with serum BDG assay makes the diagnosis of nocardiosis difficult. Because BDG assay is widely used to diagnose invasive fungal infection, clinicians should take into consideration the fact that Nocardia species may show cross-reactivity with BDG assay on serum. Clinicians should aim to detect the causative microbes without excessively depending on helpful serologic tests, such as BDG.
Conclusion
In conclusion, the first case of nocardial infection with high serum level of BDG was described. Clinicians should be aware of the possibility that Nocardia species may show cross-reactivity with BDG on serum.
Acknowledgement
The authors wish to acknowledge the patient.
Funding
The authors declare that funding was not utilized for the preparation of this manuscript.
Availability of data and materials
All available data is presented in the main paper.
Authors’ contributions
TS managed the patient and reviewed the literature. TN contributed to the collection of patient data. SY and NM analyzed the radiologic findings. SY and KY performed microbiological tests. TS was the main writer of the manuscript. NS and HM moderated the manuscript. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Written informed consent was obtained from the patient’s daughter for publication of this case report and any accompanying images. A copy of the written consent has been submitted for review by the Editor of this journal.
Ethics approval and consent to participate
Our ethics committee waived the requirement of ethics approval because all medical and laboratory procedures are routinely carried out and do not affect decisions concerning treatment.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Abbreviations
- ABPC/SBT
Ampicillin/sulbactam
- BDG
β-D-glucan
- TMP/SMX
Trimethoprim/sulfamethoxazole
- VRCZ
Voriconazole
Contributor Information
Toyomitsu Sawai, Phone: +81 (95) 822-3251, Email: toyosawai@yahoo.co.jp.
Takumi Nakao, Email: tkm790.nc.crux@gmail.com.
Shota Yamaguchi, Email: yamaguchi-shota@ncho.jp.
Sumako Yoshioka, Email: ysumako@yahoo.co.jp.
Nobuko Matsuo, Email: nobumaru1024@gmail.com.
Naofumi Suyama, Email: naika-suyama@nmh.jp.
Katsunori Yanagihara, Email: k-yanagi@nagasaki-u.ac.jp.
Hiroshi Mukae, Email: hmukae@nagasaki-u.ac.jp.
References
- 1.Koncan R, Favuzzi V, Ligozzi M, Sorrentino A, Cornaglia G, Lo cascio G. Cross-reactivity of Nocardia spp. in the fungal (1-3)-β-D-glucan aperformed on cerebral spinal fluid. Diagn Microbiol Infect Dis. 2015;81:94–95. doi: 10.1016/j.diagmicrobio.2014.11.002. [DOI] [PubMed] [Google Scholar]
- 2.Matulionyte R, Rohner P, Uckay I, Lew D, Garbino J. Secular trends of Nocardia infection over 15 years in a tertiary care hospital. J Clin Pathol. 2004;57:807–812. doi: 10.1136/jcp.2004.016923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Budzik JM, Hosseini M, Mackinnon AC, Jr, Taxy JB. Disseminated Nocardia farcinica: literature review and fatal outcome in an immunocompetent patient. Surg Infect. 2012;13:163–170. doi: 10.1089/sur.2011.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.De La lglesia P, Viejo G, Gomez B, De Miguel D, Del Valle A, Otero L. Fatal pulmonary Nocardia farcinica infection. J Clin Microbiol. 2002;40:1098–1099. doi: 10.1128/JCM.40.3.1098-1099.2002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mari B, Monton C, Mariscal D, Lujan M, Sala M, Domingo C. Pulmonary nocardiosis: clinical experience in ten cases. Respiration. 2001;68:382–388. doi: 10.1159/000050531. [DOI] [PubMed] [Google Scholar]
- 6.Babayigit A, Olmez D, Sozmen C, Makay B, Uzuner N, Karaman O, Anal O, Gulay Z. Infection caused by Nocardia farcinica mimicking pulmonary metastasis in an adolescent girl. Pediatr Emerg Care. 2010;26:203–205. doi: 10.1097/PEC.0b013e3181d1e3f7. [DOI] [PubMed] [Google Scholar]
- 7.Menku A, Kurtsoy A, Tucer B, Yildiz O, Akdemir H. Nocardia brain abscess mimicking brain tumor in immunocompetent patients: report of two cases and review of the literature. Acta Neurochir. 2004;146:411–414. doi: 10.1007/s00701-004-0263-y. [DOI] [PubMed] [Google Scholar]
- 8.Beaman L, Beaman BL. Nocardia species: host-parasite relationships. Clin Microbiol Rev. 1994;7:213–264. doi: 10.1128/CMR.7.2.213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ntziora F, Falagas ME. Linezolid for the treatment of patients with central nervous system infection. Ann Pharmacother. 2007;41:296–308. doi: 10.1345/aph.1H307. [DOI] [PubMed] [Google Scholar]
- 10.Agterof MJ, van der Bruggen T, Tersmette M, ter Borg EJ, van den Bosch JMM, Biesma DH. Nocardiosis: a case series and a mini review of clinical and microbiological features. Neth J Med. 2007;65:199–202. [PubMed] [Google Scholar]
- 11.Farina C, Boiron P, Goglio A, et al. Human nocardiosis in northern Italy from 1982 to 1992. Northern Italy collaborative group on Nocardiosis. Scand J Infect Dis. 1995;27:23–7. [DOI] [PubMed]
- 12.Usami M, Ohata A, Horiuchi T, Nagasawa K, Wakabayashi T, Tanaka S. Positive (1→3)-beta-D-glucan in blood components and release of (1→3)-beta-D-glucan from depth-type membrane filters for blood processing. Transfusion. 2002;42:1189–1195. doi: 10.1046/j.1537-2995.2002.00162.x. [DOI] [PubMed] [Google Scholar]
- 13.Mennink-Kersten MA, Warris A, Verweij PE. 1, 3-β-D-glucan in patients receiving intravenous amoxicillin-clavulanic acid. N Engl J Med. 2006;354:2834–2835. doi: 10.1056/NEJMc053340. [DOI] [PubMed] [Google Scholar]
- 14.Ogawa M, Hori H, Niiguchi S, Azuma E, Komada Y. False-positive plasma (13)-beta-D-glucan test following immunoglobulin product replacement in an adult bone marrow recipient. Int J Hematol. 2004;80:97–98. doi: 10.1532/IJH97.04030. [DOI] [PubMed] [Google Scholar]
- 15.Mennink-Kersten MA, Verweij PE. Non-culture-based diagnostics for opportunistic fungi. Infect Dis Clin N Am. 2006;20:711–727. doi: 10.1016/j.idc.2006.06.009. [DOI] [PubMed] [Google Scholar]
- 16.Mennink-Kersten MA, Ruegebrink D, Verweij PE. Pseudomonas Aeruginosa as a cause of 1,3-β-D-glucan assay reactivity. CID. 2008;46:1930–1931. doi: 10.1086/588563. [DOI] [PubMed] [Google Scholar]
- 17.Metan G, Agkus C, Nedret Koc A, Elmali F, Finkelman MA. Does ampicillin-sulbactam cause false positivity of (1,3)-beta-D-glucan assay? A prospective evaluation of 15 patients without invasive fungal infections. Mycoses. 2012;55:366–371. doi: 10.1111/j.1439-0507.2011.02131.x. [DOI] [PubMed] [Google Scholar]
- 18.Marty FM, Lowry CM, Lempitski SJ, Kubiak DW, Finkelman MA, Baden LR. Reactivity of (1→3)-β-D-glucan assay with commonly used intravenous antimicrobials. Antimicrob Agents Chemother. 2006;50:3450–3453. doi: 10.1128/AAC.00658-06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Severo CB, Oliveria Fde M, Cunha L, Cantarelli V, Severo LC. Disseminated nocardiosis due to Nocardia farcinica: diagnosis by thyroid abscess culture. Rev Inst Med Trop Sao Paulo. 2005;47:355–358. doi: 10.1590/S0036-46652005000600009. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All available data is presented in the main paper.